
Keep Moving to Retain the Healthy Self: The Influence of Physical Exercise in Health Anxiety among Chinese Menopausal Women


Abstract
:1. Introduction
2. Literature Review and Hypothesis Development
2.1. The Concept of Variables
2.1.1. Physical Exercise
2.1.2. Health Anxiety
2.1.3. Interpersonal Competence
2.1.4. Emotional Intelligence
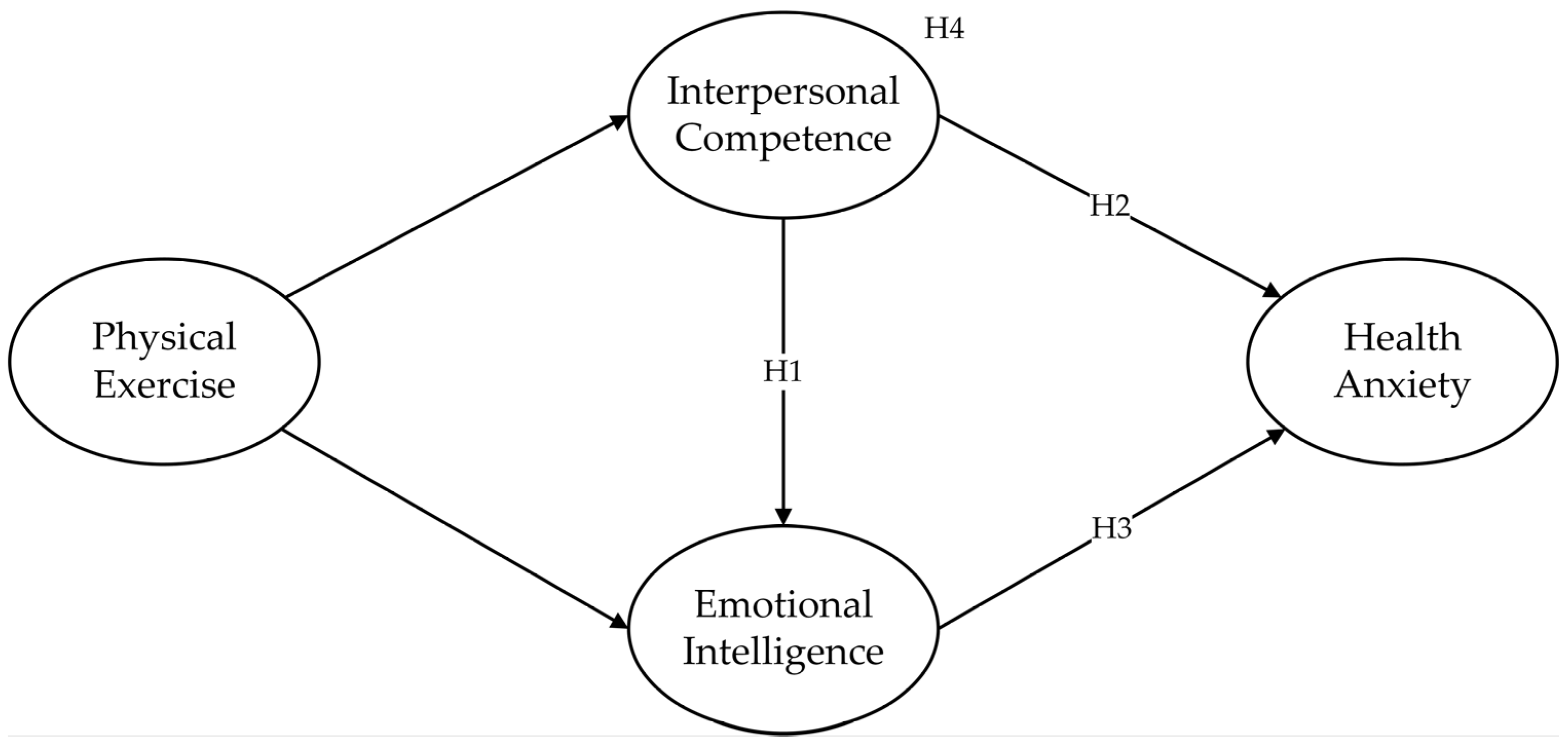
2.2. Hypotheses
2.2.1. Interpersonal Competence, Emotional Intelligence, and Health Anxiety
2.2.2. The Mediating Effects
3. Methodology
3.1. Participants and Procedure
3.2. Instruments
3.3. Data Analysis
4. Results
4.1. Assessment of the Measurement Model Reliability and Validity
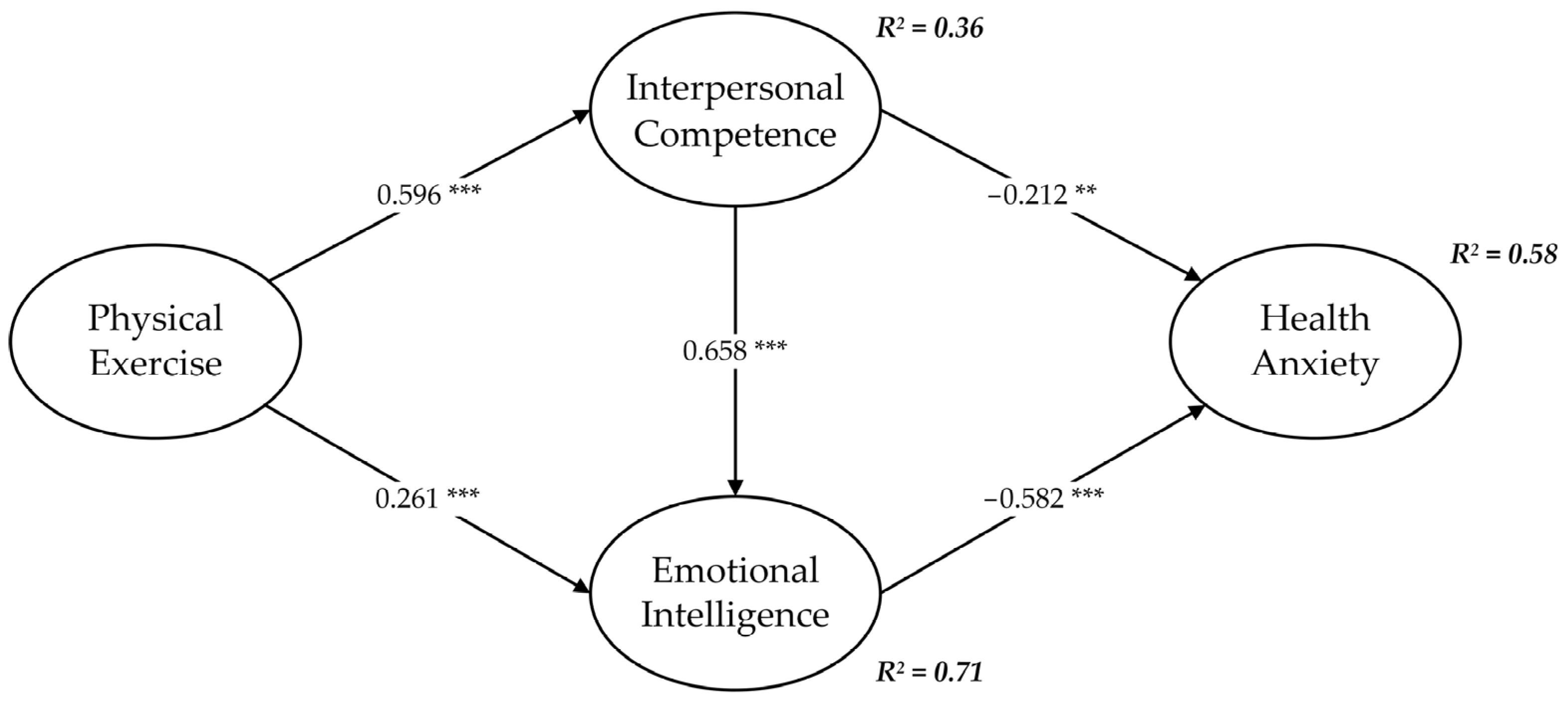
4.2. Hypothesis Testing Results
5. Discussion
5.1. Theoretical Contribution
5.2. Practical Implications
5.3. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sagsöz, N.; Oguztürk, Ö.; Bayram, M.; Kamacı, M. Anxiety and depression before and after the menopause. Arch. Gynecol. Obstet. 2001, 264, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Avis, N.E.; Stellato, R.; Crawford, S.; Bromberger, J.; Ganz, P.; Cain, V.; Kagawa-Singer, M. Is there a menopausal syndrome? Menopausal status and symptoms across racial/ethnic groups. Soc. Sci. Med. 2001, 52, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Mulhall, S.; Andel, R.; Anstey, K.J. Variation in symptoms of depression and anxiety in midlife women by menopausal status. Maturitas 2018, 108, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.W.; Sammel, M.D.; Lin, H.; Nelson, D.B. Associations of hormones and menopausal status with depressed mood in women with no history of depression. Arch. Gen. Psychiatry 2006, 63, 375–382. [Google Scholar] [CrossRef]
- Sowers, M.R.; La Pietra, M.T. Menopause: Its epidemiology and potential association with chronic diseases. Epidemiol. Rev. 1995, 17, 287–302. [Google Scholar] [CrossRef]
- Anderson, E.; Shivakumar, G. Effects of exercise and physical activity on anxiety. Front. Psychiatry 2013, 4, 27. [Google Scholar] [CrossRef]
- Ströhle, A. Physical activity, exercise, depression and anxiety disorders. J. Neural. Transm. 2009, 116, 777–784. [Google Scholar] [CrossRef]
- Kandola, A.; Vancampfort, D.; Herring, M.; Rebar, A.; Hallgren, M.; Firth, J.; Stubbs, B. Moving to beat anxiety: Epidemiology and therapeutic issues with physical activity for anxiety. Curr. Psychiatry Rep. 2018, 20, 63. [Google Scholar] [CrossRef]
- Wang, H.; Zheng, X.; Liu, Y.; Xu, Z.; Yang, J. Alleviating doctors’ emotional exhaustion through sports involvement during the COVID-19 pandemic: The mediating roles of regulatory emotional self-efficacy and perceived stress. Int. J. Environ. Res. Public Health 2022, 19, 11776. [Google Scholar] [CrossRef]
- State Council. National Fitness Program (2021–2025). 2021. Available online: http://www.gov.cn/zhengce/content/2021-08/03/content_5629218.htm (accessed on 3 August 2021).
- Saqib, Z.A.; Dai, J.; Menhas, R.; Mahmood, S.; Karim, M.; Sang, X.; Weng, Y. Physical activity is a medicine for non-communicable diseases: A survey study regarding the perception of physical activity impact on health wellbeing. Risk Manag. Healthc. Policy 2020, 13, 2949–2962. [Google Scholar] [CrossRef]
- Wang, K.; Wang, X. Providing sports venues on mainland China: Implications for promoting leisure-time physical activity and national fitness policies. Int. J. Environ. Res. Public Health 2020, 17, 5136. [Google Scholar] [CrossRef]
- Burnside, C.; Dollar, D. Aid, policies, and growth. Am. Econ. Rev. 2000, 90, 847–868. [Google Scholar] [CrossRef]
- Wang, H.; Jiaxuan, L.; Aweewan, M.; Jiafu, S. Linking perceived policy effectiveness and proenvironmental behavior: The influence of attitude, implementation intention, and Knowledge. Int. J. Environ. Res. Public Health 2021, 18, 2910. [Google Scholar] [CrossRef]
- Bromberger, J.T.; Kravitz, H.M.; Chang, Y.; Randolph, J.F., Jr.; Avis, N.E.; Gold, E.B.; Matthews, K.A. Does risk for anxiety increase during the menopausal transition? Study of women’s health across the nation. Menopause 2013, 20, 488–495. [Google Scholar] [CrossRef]
- Jia, R.-X.; Liang, J.-H.; Xu, Y.; Wang, Y.-Q. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: A meta-analysis. BMC Geriatr. 2019, 19, 181. [Google Scholar] [CrossRef]
- Hagger, M.S. Habit and physical activity: Theoretical advances, practical implications, and agenda for future research. Psychol. Sport Exerc. 2019, 42, 118–129. [Google Scholar] [CrossRef]
- Wang, X.; Song, G.; Wan, X. Measuring “nudgeability”: Development of a scale on susceptibility to physical activity nudges among college students. Behav. Sci. 2022, 12, 318. [Google Scholar] [CrossRef]
- Jungmann, S.M.; Witthöft, M. Health anxiety, cyberchondria, and coping in the current COVID-19 pandemic: Which factors are related to coronavirus anxiety? J. Anxiety Disord. 2020, 73, 102239. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Simbar, M.; Nazarpour, S.; Alavi Majd, H.; Dodel Andarvar, K.; Jafari Torkamani, Z.; Alsadat Rahnemaei, F. Is body image a predictor of women’s depression and anxiety in postmenopausal women? BMC Psychiatry 2020, 20, 202. [Google Scholar] [CrossRef]
- Del Sueldo, M.; Martell-Claros, N.; Abad-Cardiel, M.; Zilberman, J.M.; Marchegiani, R.; Fernández-Pérez, C. Health perception in menopausal women. Int. J. Women’s Health 2018, 10, 655. [Google Scholar] [CrossRef] [PubMed]
- Santoro, N.; Epperson, C.N.; Mathews, S.B. Menopausal symptoms and their management. Endocrinol. Metab. Clin. 2015, 44, 497–515. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, K.; Sahin, S.; Guler, D.S.; Unsal, A.; Akdemir, N. Depression, anxiety, and fear of death in postmenopausal women. Menopause 2020, 27, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Englefield, E.; Black, S.A.; Copsey, J.A.; Knight, A.T. Interpersonal competencies define effective conservation leadership. Biol. Conserv. 2019, 235, 18–26. [Google Scholar] [CrossRef]
- Theelen, H.; Van den Beemt, A.; den Brok, P. Classroom simulations in teacher education to support preservice teachers’ interpersonal competence: A systematic literature review. Comput. Educ. 2019, 129, 14–26. [Google Scholar] [CrossRef]
- Kotsou, I.; Mikolajczak, M.; Heeren, A.; Grégoire, J.; Leys, C. Improving emotional intelligence: A systematic review of existing work and future challenges. Emot. Rev. 2019, 11, 151–165. [Google Scholar] [CrossRef]
- Bar-On, R. Emotional and social intelligence: Insights from the Emotional Quotient Inventory. In The Handbook of Emotional Intelligence: Theory, Development, Assessment, and Application at Home, School, and in the Workplace; Jossey-Bass: San Francisco, CA, USA, 2000; pp. 363–388. [Google Scholar]
- Law, K.S.; Wong, C.-S.; Song, L.J. The construct and criterion validity of emotional intelligence and its potential utility for management studies. J. Appl. Psychol. 2004, 89, 483–496. [Google Scholar] [CrossRef]
- Parker, J.D.; Summerfeldt, L.J.; Walmsley, C.; O’Byrne, R.; Dave, H.P.; Crane, A.G. Trait emotional intelligence and interpersonal relationships: Results from a 15-year longitudinal study. Pers. Individ. Differ. 2021, 169, 110013. [Google Scholar] [CrossRef]
- Oh, E.-J. Mediating effect of communication ability on relationships among self-awareness, empathy, emotional intelligence and interpersonal competence of nursing students. J. Digit. Converg. 2021, 19, 549–560. [Google Scholar] [CrossRef]
- Baudry, A.-S.; Lelorain, S.; Mahieuxe, M.; Christophe, V. Impact of emotional competence on supportive care needs, anxiety and depression symptoms of cancer patients: A multiple mediation model. Support. Care Cancer 2018, 26, 223–230. [Google Scholar] [CrossRef]
- MacEvilly, D.; Brosnan, G. Adapting an emotional regulation and social communication skills group programme to teletherapy, in response to the COVID-19 pandemic. Ir. J. Psychol. Med. 2020, 39, 423–428. [Google Scholar] [CrossRef]
- Domitrovich, C.E.; Durlak, J.A.; Staley, K.C.; Weissberg, R.P. Social-emotional competence: An essential factor for promoting positive adjustment and reducing risk in school children. Child. Dev. 2017, 88, 408–416. [Google Scholar] [CrossRef]
- Suarez-García, I.; Alejos, B.; Pérez-Elías, M.-J.; Iribarren, J.-A.; Hernando, A.; Ramírez, M.; Tasias, M.; Pascual, M.; Jarrin, I.; Hernando, V. How do women living with HIV experience menopause? Menopausal symptoms, anxiety and depression according to reproductive age in a multicenter cohort. BMC Women’s Health 2021, 21, 223. [Google Scholar] [CrossRef]
- Luna, P.; Guerrero, J.; Cejudo, J. Improving adolescents’ subjective well-being, trait emotional intelligence and social anxiety through a programme based on the sport education model. Int. J. Environ. Res. Public Health 2019, 16, 1821. [Google Scholar] [CrossRef]
- Zhoc, K.C.; Chung, T.S.; King, R.B. Emotional intelligence (EI) and self-directed learning: Examining their relation and contribution to better student learning outcomes in higher education. Br. Educ. Res. J. 2018, 44, 982–1004. [Google Scholar] [CrossRef]
- Metts, A.V.; LeBeau, R.T.; Craske, M.G.; Himle, J.A. Perceived interpersonal competence as a predictor of clinical outcomes in a randomized controlled trial for social anxiety and employment. Cogn. Behav. Ther. 2022, 52, 146–162. [Google Scholar] [CrossRef]
- Rask, C.U.; Munkholm, A.; Clemmensen, L.; Rimvall, M.K.; Ørnbøl, E.; Jeppesen, P.; Skovgaard, A.M. Health anxiety in preadolescence-associated health problems, healthcare expenditure, and continuity in childhood. J. Abnorm. Child Psychol. 2016, 44, 823–832. [Google Scholar] [CrossRef]
- Malkoç, A.; Aslan Gördesli, M.; Arslan, R.; Çekici, F.; Aydın Sünbül, Z. The relationship between interpersonal emotion regulation and interpersonal competence controlled for emotion dysregulation. Int. J. Higher Educ. 2019, 8, 69–76. [Google Scholar] [CrossRef]
- Bell, S.L.; Audrey, S.; Gunnell, D.; Cooper, A.; Campbell, R. The relationship between physical activity, mental wellbeing and symptoms of mental health disorder in adolescents: A cohort study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 138. [Google Scholar] [CrossRef]
- Gordon, J.L.; Sander, B.; Eisenlohr-Moul, T.A.; Tottenham, L.S. Mood sensitivity to estradiol predicts depressive symptoms in the menopause transition. Psychol. Med. 2021, 51, 1733–1741. [Google Scholar] [CrossRef]
- Zimmer, C.; McDonough, M.H.; Hewson, J.; Toohey, A.; Din, C.; Crocker, P.R.; Bennett, E.V. Experiences with Social Participation in group physical activity programs for older adults. J. Sport Exerc. Psychol. 2021, 43, 335–344. [Google Scholar] [CrossRef]
- Owari, Y.; Miyatake, N.; Kataoka, H. Relationship between social participation, physical activity and psychological distress in apparently healthy elderly people: A pilot study. Acta Med. Okayama 2018, 72, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Berli, C.; Bolger, N.; Shrout, P.E.; Stadler, G.; Scholz, U. Interpersonal processes of couples’ daily support for goal pursuit: The example of physical activity. Pers. Soc. Psychol. Bull. 2018, 44, 332–344. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Zhang, L.; Teo, K. Social use of fitness apps and physical activity knowledge: The roles of information elaboration and interpersonal communication. J. Broadcast. Electron. Media 2021, 65, 549–574. [Google Scholar] [CrossRef]
- Malchrowicz-Mośko, E.; Poczta, J. Running as a form of therapy socio-psychological functions of mass running events for men and women. Int. J. Environ. Res. Public Health 2018, 15, 2262. [Google Scholar] [CrossRef] [PubMed]
- Waaso, P.; Gofton, N.; Zuhl, M. The effect of self-selected exercise workloads on perceived enjoyment and self-efficacy in sedentary adults. Behav. Sci. 2022, 12, 224. [Google Scholar] [CrossRef]
- Adamczyk, K.; Segrin, C. The mediating role of romantic desolation and dating anxiety in the association between interpersonal competence and life satisfaction among polish young adults. J. Adult Dev. 2016, 23, 1–10. [Google Scholar] [CrossRef]
- Zhao, J.; Xiang, Y.; Zhang, W.; Dong, X.; Zhao, J.; Li, Q. Childhood maltreatment affects depression and anxiety: The mediating role of emotional intelligence. Int. J. Ment. Health Addict. 2021, 19, 2021–2030. [Google Scholar] [CrossRef]
- Di Stasio, M.; Rinaldi, C.; Sciaraffa, J.; Cheong, C. The relationship between indirect aggression and loneliness for emerging adults: What does interpersonal competence have to do with wellbeing? Alberta J. Educ. Res. 2020, 66, 1–16. [Google Scholar] [CrossRef]
- Lanciano, T.; Curci, A.; Kafetsios, K.; Elia, L.; Zammuner, V.L. Attachment and dysfunctional rumination: The mediating role of Emotional Intelligence abilities. Pers. Individ. Differ. 2012, 53, 753–758. [Google Scholar] [CrossRef]
- Behzadnia, B.; Adachi, P.J.; Deci, E.L.; Mohammadzadeh, H. Associations between students’ perceptions of physical education teachers’ interpersonal styles and students’ wellness, knowledge, performance, and intentions to persist at physical activity: A self-determination theory approach. Psychol. Sport Exerc. 2018, 39, 10–19. [Google Scholar] [CrossRef]
- Eys, M.; Bruner, M.W.; Martin, L.J. The dynamic group environment in sport and exercise. Psychol. Sport Exerc. 2019, 42, 40–47. [Google Scholar] [CrossRef]
- Herbert, C.; Gilg, V.; Sander, M.; Kobel, S.; Jerg, A.; Steinacker, J. Preventing mental health, well-being and physical activity during the corona pandemic—Recommendations from psychology and sports medicine. Dtsch. Z. Sportmed. 2020, 71, 249–256. [Google Scholar] [CrossRef]
- Giulia, V.; Giulia, S.; Paola, F. Emotional intelligence, empathy and alexithymia: A cross-sectional survey on emotional competence in a group of nursing students. Acta Biomed. 2019, 90, 32–43. [Google Scholar] [CrossRef]
- Shukla, A.; Srivastava, R. Examining the effect of emotional intelligence on socio-demographic variable and job stress among retail employees. Cogent Bus. Manag. 2016, 3, 1201905. [Google Scholar] [CrossRef]
- Andersen, L.G.; Groenvold, M.; Jørgensen, T.; Aadahl, M. Construct validity of a revised Physical Activity Scale and testing by cognitive interviewing. Scand. J. Public Health 2010, 38, 707–714. [Google Scholar] [CrossRef]
- Buhrmester, D.; Furman, W.; Wittenberg, M.T.; Reis, H.T. Five domains of interpersonal competence in peer relationships. J. Pers. Soc. Psychol. 1988, 55, 991–1008. [Google Scholar] [CrossRef]
- Abramowitz, J.S.; Deacon, B.J.; Valentiner, D.P. The short health anxiety inventory: Psychometric properties and construct validity in a non-clinical sample. Cognit. Ther. Res. 2007, 31, 871–883. [Google Scholar] [CrossRef]
- Wang, H.; Mangmeechai, A. Understanding the gap between environmental intention and pro-environmental behavior towards the waste sorting and management policy of China. Int. J. Environ. Res. Public Health 2021, 18, 757. [Google Scholar] [CrossRef]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Mossholder, K.W.; Bennett, N.; Kemery, E.R.; Wesolowski, M.A. Relationships between bases of power and work reactions: The mediational role of procedural justice. J. Manag. 1998, 24, 533–552. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Bollen, K.A.; Stine, R. Direct and indirect effects: Classical and bootstrap estimates of variability. Sociol. Methodol. 1990, 20, 115–140. [Google Scholar] [CrossRef]
- Ozcan, H.; Savci, H.; Canik, M.; Ayan, M.; Bas, C.F. Comparison of the relationship between menopausal symptoms and loneliness and anger. Perspect. Psychiatr. Care 2022, 58, 1900–1906. [Google Scholar] [CrossRef]
- Keating, N.L.; Cleary, P.D.; Rossi, A.S.; Zaslavsky, A.M.; Ayanian, J.Z. Use of hormone replacement therapy by postmenopausal women in the United States. Ann. Intern. Med. 1999, 130, 545–553. [Google Scholar] [CrossRef]
- Hinchliff, S.; Gott, M. Perceptions of well-being in sexual ill health: What role does age play? J. Health Psychol. 2004, 9, 649–660. [Google Scholar] [CrossRef]
- Ubago-Jiménez, J.L.; González-Valero, G.; Puertas-Molero, P.; García-Martínez, I. Development of emotional intelligence through physical activity and sport practice. A systematic review. Behav. Sci. 2019, 9, 44. [Google Scholar] [CrossRef]
- Li, L.; Meng, J. Network effects on physical activity through interpersonal vs. masspersonal communication with the core and acquaintance networks. Comput. Hum. Behav. 2023, 141, 107594. [Google Scholar] [CrossRef]
- Prins, R.G.; Oenema, A.; van der Horst, K.; Brug, J. Objective and perceived availability of physical activity opportunities: Differences in associations with physical activity behavior among urban adolescents. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 70. [Google Scholar] [CrossRef]
- Niven, A.; Baker, G.; Almeida, E.C.; Fawkner, S.G.; Jepson, R.; Manner, J.; Morton, S.; Nightingale, G.; Sivaramakrishnan, D.; Fitzsimons, C. “Are we working (too) comfortably?”: Understanding the nature of and factors associated with sedentary behaviour when working in the home environment. Occup. Health Sci. 2022, 1–18. [Google Scholar] [CrossRef]
- Waldman, E.G.; Cahn, N.R.; Crawford, B.J. Contextualizing menopause in the law. Harv. J. Law Gend. 2022, 45, 1–62. [Google Scholar]
- Brin, D.J. The use of rituals in grieving for a miscarriage or stillbirth. In From Menarche to Menopause: The Female Body in Feminist Therapy, 1st ed.; Routledge: New York, NY, USA, 2014; pp. 123–132. [Google Scholar]



{kind=link}
{kind=link}
| Profiles | Survey (%) |
|---|---|
| Age | |
| 40–45 | 32.1 |
| 46–50 | 54.7 |
| 51–55 | 13.2 |
| Menopausal status | |
| Late reproductive stage | 56.7 |
| Menopausal transition | 27.3 |
| Postmenopausal | 16.0 |
| Marital status | |
| Married | 87.3 |
| Single (i.e., unmarried, divorced, or widowed) | 12.7 |
| Education level | |
| Below high school | 33.4 |
| High school/vocational school | 61.1 |
| College and above | 5.5 |
| Employment status | |
| Employed | 63.1 |
| Unemployed | 36.9 |
| Income | |
| <CNY 3000 | 29.2 |
| CNY 3000–6000 | 49.5 |
| >CNY 6000 | 21.3 |
| Items | Loadings | Cα | AVE | CR |
|---|---|---|---|---|
| Physical Exercise (PE) | 0.946 | 0.856 | 0.947 | |
| PE1 | 0.939 | |||
| PE2 | 0.922 | |||
| PE3 | 0.914 | |||
| Interpersonal Competence (IC) | 0.929 | 0.769 | 0.930 | |
| IC1 | 0.815 | |||
| IC2 | 0.874 | |||
| IC3 | 0.897 | |||
| IC4 | 0.917 | |||
| Emotional Intelligence (EI) | 0.917 | 0.787 | 0.917 | |
| EI1 | 0.891 | |||
| EI2 | 0.897 | |||
| EI3 | 0.873 | |||
| Health Anxiety (HA) | 0.965 | 0.874 | 0.965 | |
| HA1 | 0.910 | |||
| HA2 | 0.931 | |||
| HA3 | 0.944 | |||
| HA4 | 0.953 |
| Construct | PE | IC | EI | HA |
|---|---|---|---|---|
| PE | (0.925) | |||
| IC | 0.559 ** | (0.877) | ||
| EI | 0.599 ** | 0.756 ** | (0.887) | |
| HA | −0.576 ** | −0.654 ** | −0.704 ** | (0.935) |
| Point Estimate | Product of Coefficients | Bootstrapping | ||||||
|---|---|---|---|---|---|---|---|---|
| Percentile 95% CI | Bias-Corrected 95% CI | Two-Tailed Significance | ||||||
| SE | Z | Lower | Upper | Lower | Upper | |||
| Direct effects | ||||||||
| PE → IC | 0.596 | 0.037 | 16.108 | 0.521 | 0.665 | 0.520 | 0.665 | 0.000 (***) |
| PE → EI | 0.261 | 0.054 | 4.833 | 0.162 | 0.374 | −0.160 | 0.371 | 0.000 (***) |
| IC → EI | 0.658 | 0.051 | 12.902 | 0.549 | 0.749 | 0.549 | 0.748 | 0.000 (***) |
| IC → HA | −0.212 | 0.067 | −3.164 | −0.340 | −0.074 | −0.341 | −0.075 | 0.004 (**) |
| EI → HA | −0.582 | 0.070 | −8.314 | −0.723 | −0.447 | −0.717 | −0.441 | 0.000 (***) |
| Indirect effects | ||||||||
| PE → HA | −0.506 | 0.039 | −12.974 | −0.583 | −0.428 | −0.582 | −0.427 | 0.000 (***) |
| Total effects | ||||||||
| PE → HA | −0.506 | 0.039 | −12.974 | −0.583 | −0.428 | −0.582 | −0.427 | 0.000 (***) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Zhang, Q.; Lin, Y.; Liu, Y.; Xu, Z.; Yang, J. Keep Moving to Retain the Healthy Self: The Influence of Physical Exercise in Health Anxiety among Chinese Menopausal Women. Behav. Sci. 2023, 13, 140. https://doi.org/10.3390/bs13020140
Wang H, Zhang Q, Lin Y, Liu Y, Xu Z, Yang J. Keep Moving to Retain the Healthy Self: The Influence of Physical Exercise in Health Anxiety among Chinese Menopausal Women. Behavioral Sciences. 2023; 13(2):140. https://doi.org/10.3390/bs13020140
Chicago/Turabian StyleWang, Huilin, Qingxing Zhang, Yapeng Lin, Yang Liu, Ziqing Xu, and Jingyu Yang. 2023. "Keep Moving to Retain the Healthy Self: The Influence of Physical Exercise in Health Anxiety among Chinese Menopausal Women" Behavioral Sciences 13, no. 2: 140. https://doi.org/10.3390/bs13020140