This section proposes research hypotheses based on the Theory of Planned Behavior and related studies, and constructs a theoretical model. In addition, it analyzes the reliability of the scale questionnaire using the SPSS26.0 software (SPSS26.0 is a professional statistical analysis software released by IBM in USA in 2019), tests the convergent validity and differential validity of the scale questionnaire using AMOS24.0 software (Amos24.0 is a structural equation modeling software released by IBM in USA), conducts a descriptive statistical analysis of the factors, and constructs a structural equation model of the factors affecting women’s fertility intentions. This section reveals the factors influencing women’s fertility intentions from a quantitative perspective and analyzes their influence paths.
4.4.1. Research Hypothesis and Construction of Theoretical Model
In 1985, Ajzen added perceived behavioral control variables to the original rational behavior framework, thus forming the Theory of Planned Behavior (TPB).The TPB aims to explain human behavior rather than just predict it, and it considers that behavioral attitudes, subjective norms, and perceived behavioral control are the three prerequisites for determining behavioral intentions and behavior. The behavioral attitude refers to an individual’s positive or negative value judgment of behavior. The subjective norm refers to the social pressure individuals feel due to a particular behavior. The perceived behavioral control refers to an individual’s perception of the difficulty level of an operating behavior. Based on this, the subjective attitudes toward fertility, perceptions of family and friends’ attitudes, external social norms, and cost constraints determine the behavioral attitudes, normative beliefs, and perceived behavioral control of fertility.
Since its initial introduction, the Theory of Planned Behavior has been widely used in various industries, such as healthcare, leisure activities, travel, environmental behaviors, employment choices, shopping consumption, online activities, and online services. The predictive and explanatory power of the three variables in the model, behavior attitudes, subjective norms and perceived behavioral control, in relation to behavioral intentions has been empirically demonstrated in several studies. Ajzen et al. [
19] analyzed college students’ willingness to engage in outdoor activities, and found that behavior attitude, subjective norms, and perceived behavior control all positively influenced behavior willingness, among which perceived behavior control had the greatest influence, while subjective norms had the least influence. Liao et al. [
20] conducted a study of virtual banks, and found that the effect of subjective norms on use intention was not significant. Therefore, it is reasonable to construct a structural equation model of women’s fertility intentions based on TPB. However, the existing studies show that the three variables have different impacts on behavioral intentions, among which the influence of subjective norms is small, and is the weak link in the model [
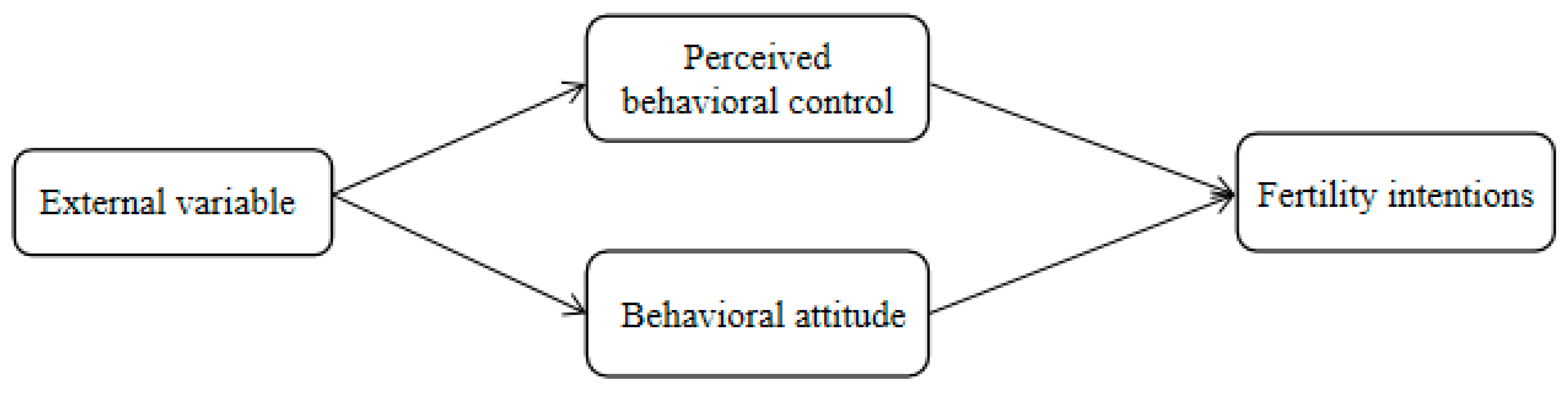
21]. Therefore, this paper introduces external variables, and selects perceived behavioral control and behavioral attitudes as determinants of fertility intentions; we propose research hypotheses H1 and H2 to construct a conceptual model, as shown in
Figure 3.
Hypothesis 1 (H1). Perceived behavioral control has a significant positive effect on fertility intentions.
Hypothesis 2 (H2). Behavioral attitude has a significant positive effect on fertility intentions.
For the selection of external variables, this paper selected economic support, policy support, public support, family support and perceived risk as external variables for the following reasons.
Section 2 mentions that economy, employment, health, and epidemic prevention policies impact women’s fertility intentions in the epidemic context. This section unifies issues such as health factors as a variable of perceived risk. Some variables that are usually studied in demographic analyses can be used as “external” variables in social psychological research [
22]. TPB distinguishes two types of external variables: First, personal background factors, including income, education, and the number of born children while deciding to have children, which may influence fertility intentions by affecting attitudes, subjective norms, and perceived behavioral control. Second, aspects of the environment, such as institutions that provide support for childcare or working parents, are described as actual controls, or actual enablers and constraints. Several studies have been conducted by national and international scholars on the external variables (namely, behavioral attitudes and perceived behavioral controls). Billari [
23] showed that socioeconomic factors influenced attitudes, while economic factors and mental health influenced behavioral control. Lin et al. [
24] confirmed that shared spousal responsibility and paternal care support can also enhance the control beliefs and behavioral attitudes of the population at the optimal age to conceive a child, especially women of childbearing age, and promote the formation of intentions to have another child. Zhou [
25] showed that the social norms and pressures of having more children made gender discrimination in the labor market increase rather than decrease, and intensified the negative beliefs of professional women in control. Klobas [
26] performed a comparative analysis of European and Asian countries, and found that young women in countries with higher levels of family- and child-friendly policy support were more likely to identify themselves with the ability to overcome fertility barriers, and their desire to give birth was higher. Yan and Zhang [
27] argued that fertility policy significantly influences women’s fertility behavior through the mediator of fertility intentions. Tian [
28] found via a survey of women of childbearing age in Shanghai that increasing investment in public childcare, improving the accessibility of public childcare, and providing high-quality social care support for infants and toddlers aged 0–3 years would effectively increase willingness to have children again.
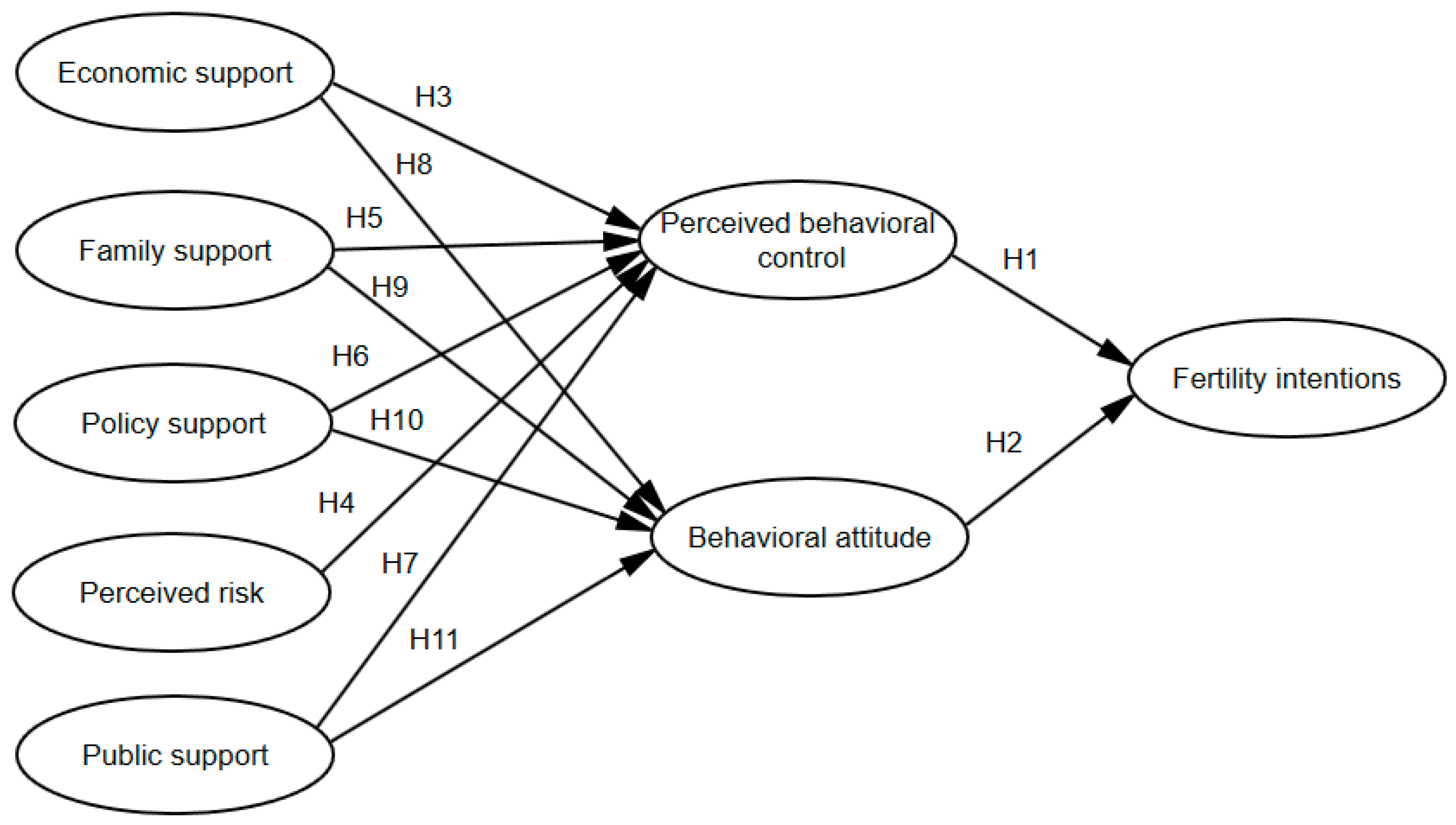
Therefore, research hypotheses H3-H11 are proposed, and a theoretical model of the fertility intentions of women of childbearing age is constructed, as shown in
Figure 4.
Hypothesis 3 (H3). Economic support has a significant positive effect on perceived behavioral control.
Hypothesis 4 (H4). Perceived risk has a significant negative effect on perceived behavioral control.
Hypothesis 5 (H5). Family support has a significant positive effect on perceived behavioral control.
Hypothesis 6 (H6). Policy support has a significant positive effect on perceived behavioral control.
Hypothesis 7 (H7). Public support has a significant positive effect on perceived behavioral control.
Hypothesis 8 (H8). Economic support has a significant positive effect on behavioral attitudes.
Hypothesis 9 (H9). Family support has a significant positive effect on behavioral attitudes.
Hypothesis 10 (H10). Policy support has a significant positive effect on behavioral attitudes.
Hypothesis 11 (H11). Public support has a significant positive effect on behavioral attitudes.
4.4.3. Reliability and Validity Test
(1) Reliability analysis
The reliability analysis, also called the reliability test, measures and tests the reliability and stability of the questionnaire. Cronbach’s alpha (α), which is commonly used in academia, is adopted to analyze the intrinsic reliability of the scale. Generally speaking, the closer the alpha value is to 1, the better the reliability of the questionnaire. When α is greater than 0.8, the reliability of the questionnaire is high. When α is 0.7–0.8, the reliability of the questionnaire is good. When α is 0.6–0.7, the reliability of the questionnaire is acceptable. When α is less than 0.6, some problems exist in the design or structure of the questionnaire, which should be revised.
The results of the reliability test of each variable in the questionnaire, performed by SPSS 26.0, are shown in
Table 5. As can be seen from
Table 5, the α coefficient of each variable is greater than 0.7, and the α coefficient of the total questionnaire reached 0.932, indicating that the questionnaire is internally consistent and stable.
(2) Validity analysis
(1) Convergence validity analysis
Convergence validity analysis is carried out by analyzing the factor loadings of each dimension. In this paper, the convergence validity of the questionnaire is determined by three indicators: standardized loading coefficient (Std.), average variance extracted (AVE), and combined reliability (CR). The questionnaire scale has convergence validity when Std. > 0.5, AVE > 0.5 and CR > 0.7. As can be seen from
Table 6, the Std. values of all dimensions are greater than 0.6, which is higher than the standard value (0.5). Meanwhile, the AVE values are higher than 0.5 and the CR values are greater than 0.7, indicating that the questionnaire has good combined reliability and validity, i.e., the scale has good internal consistency and convergent validity.
(2) Distinguishing validity analysis
Distinguishing validity analysis is used to estimate the difference in the degree of correlation between a measure and different internal and external structural variables by comparing the internal correlation of the measure within a structural variable with the external correlation of each structural variable, and thus determining the distinguishing validity of the variable. If the square root of the AVE of a variable is greater than the correlation coefficient of that variable with other variables, then the distinguishing validity of that variable is good. As can be seen from
Table 7, the AVE square roots of each variable (main diagonal part) are greater than the correlation coefficients of that variable and other variables, which indicates that all dimensions of the formal questionnaire have met the criteria of distinguishing validity and passed the test, and this questionnaire can thus construct structural equation models.
4.4.5. Construction of Structural Equation Model
(1) Evaluation of the overall fitness of the structural equation model
Structural equation modeling (SEM) is an empirical analysis technique used to find the relationship between variables and verify whether the theoretical model and hypotheses are reasonable. Based on the research hypothesis and the theoretical model constructed in the previous paper, AMOS24.0 software is used to construct a structural equation model of the factors influencing women’s fertility intentions. The relative chi-square (CMIN/DF), comparative fit index (CFI), Tucker–Lewis Index (TLI), and root mean square of the error of approximation (RMSEA) are used as fitted indicators to test the fitness of the structural model. As can be seen from
Table 9, the CMIN/DF value is 1.744, which is less than 3. The values of CFI, IFI, and TLI are 0.942, 0.943, and 0.934, respectively, all of which are greater than 0.9. The RMSEA value is 0.05, which is less than 0.08, i.e., all the fitted indicators are within the recommended values, indicating that the structural equation model fits better, and the theoretical model constructed in this paper is acceptable.
(2) Test results of the research hypothesis
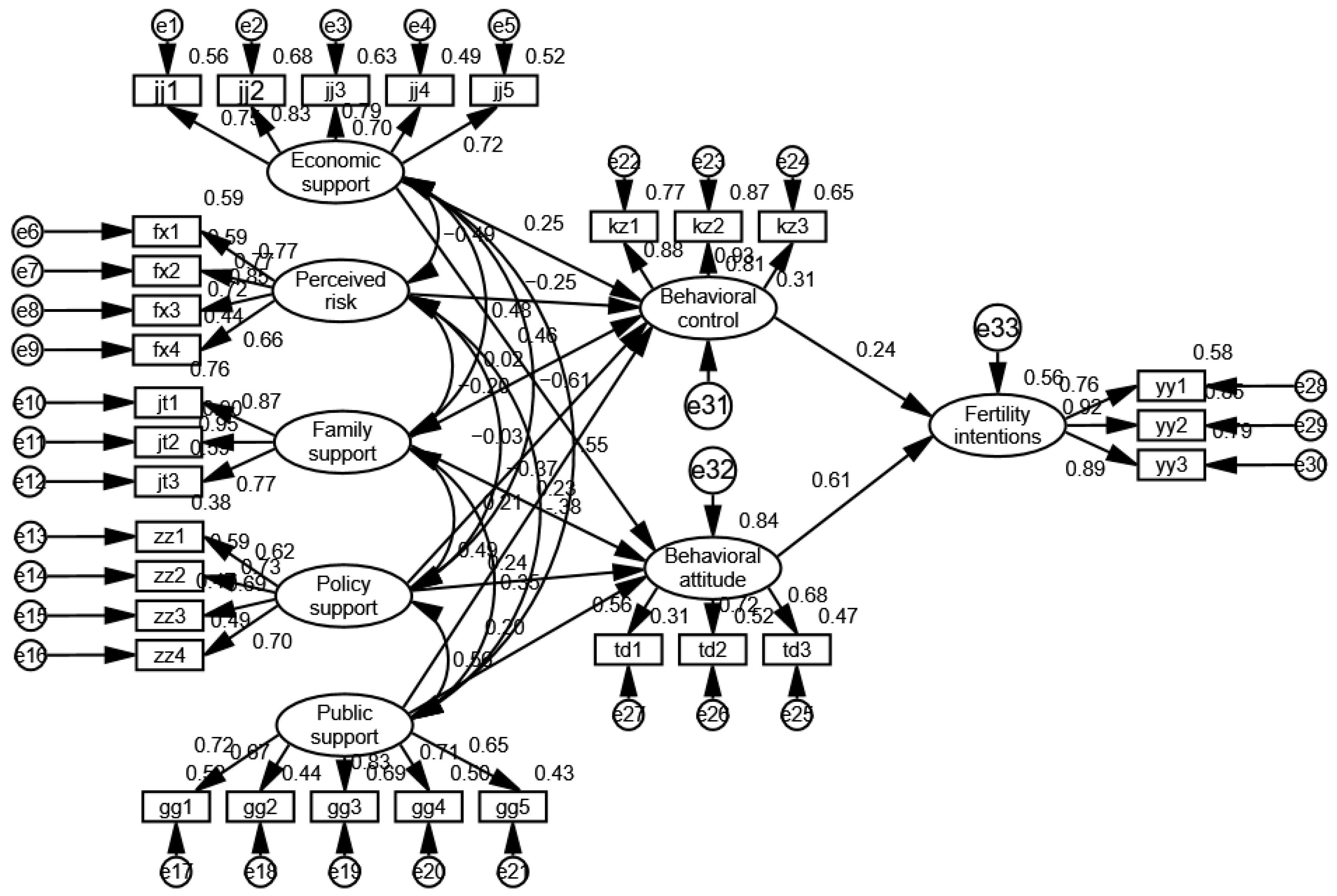
The results of the structural equation model of “factors influencing women’s fertility intentions”, the model relationships and standardized path coefficient estimates among the latent variables, as well as the hypothesis tests, are shown in
Figure 5 and
Table 10. As can be seen from
Figure 5, the path coefficients of the observed variables and their latent variables in each dimension are mostly above 0.6, which indicates that the measured items of each variable are quite supportive.
As shown in
Table 10, in terms of fertility intentions, the
p values of perceived behavioral control and behavioral attitude related to fertility intentions are less than 0.001, and the standardized estimates are positive, indicating that perceived behavioral control and behavioral attitude have a significant positive effect on fertility intentions, so the original hypotheses H1 and H2 are accepted. The standardized path coefficient of behavioral attitude affecting fertility intentions is 0.611, which is significantly greater than the standardized path coefficient of perceived behavioral control (0.236), indicating that behavioral attitudes have a greater effect on fertility intentions.
In terms of perceived behavioral control, the p values of economic support and public support in relation to perceived behavioral control are 0.006 and 0.007, respectively, both of which are less than 0.05, and the standardized estimates are greater than 0, indicating that economic support and public support have a significant positive effect on perceived behavioral control, so the original hypotheses H3 and H7 are accepted. The p values of perceived risk related to perceived behavioral control are less than 0.001 and the standardized estimates are less than 0, indicating that perceived risk has a significant negative effect on perceived behavior control, so the original hypothesis H4 is accepted. Hypothesis H5 is not tested, indicating family support has no significant effect on perceived behavioral control, because most of the respondents have college and above degrees, and are more likely to have the ability to overcome fertility barriers. In addition, the positive effect of family support on perceived behavioral control may be offset by the negative effect of perceived risk. When p > 0.05, hypothesis H6 is not tested, indicating that there is no significant impact of policy support on perceived behavioral control because the questionnaire focuses on measures of fertility policy awareness and promotion.
In terms of behavioral attitudes, the p values of economic support, family support, policy support, and public support in relation to behavioral attitudes are all less than 0.05, and the standardized path coefficients are all greater than 0, indicating that economic support, family support, policy support, and public support have a significant positive effect on behavioral attitudes; therefore, the original hypotheses H8, H9, H10, and H11 are tested. The standardized path coefficient (0.463) is the largest, indicating that the economy has the greatest influence on behavioral attitudes.
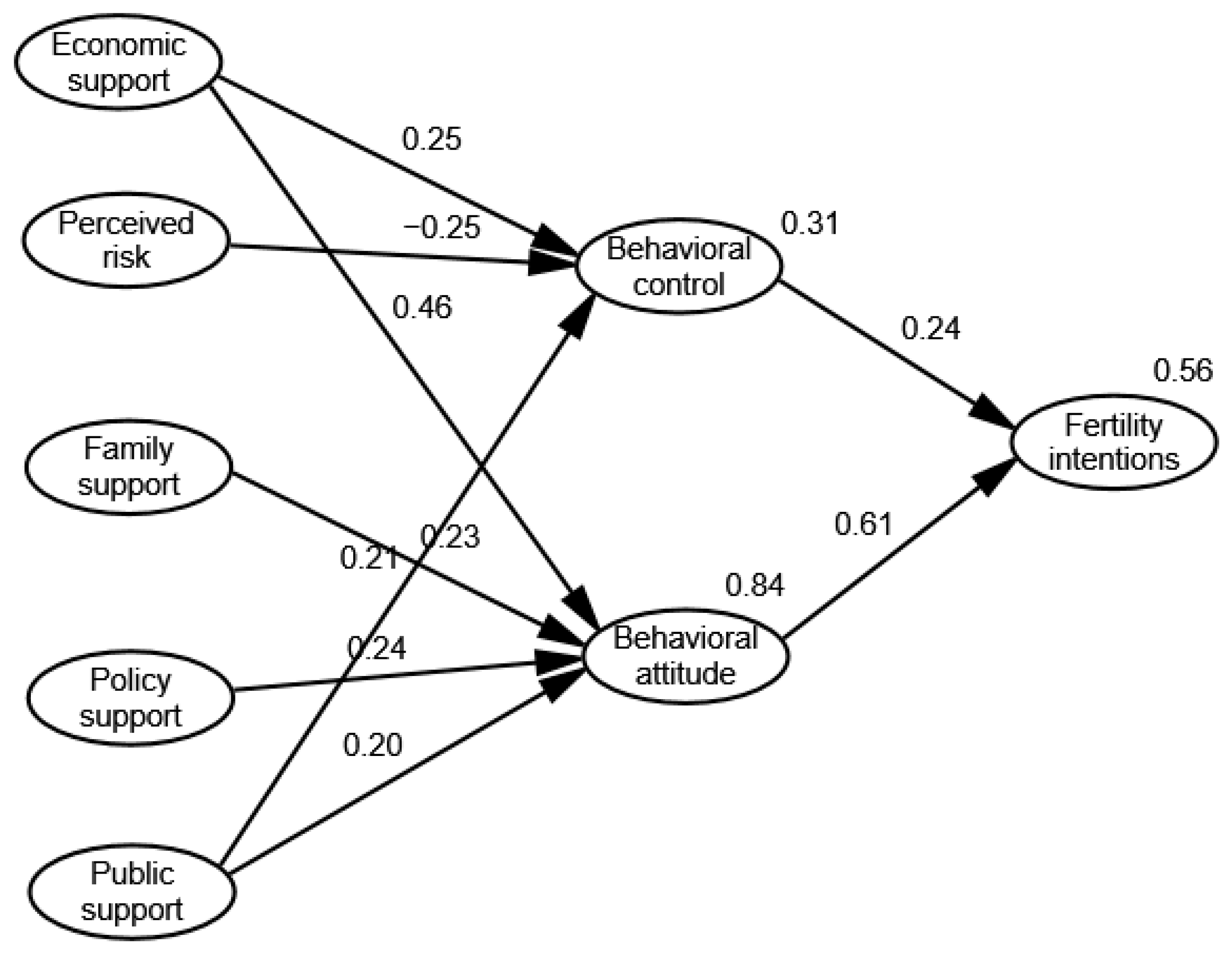
4.4.6. Empirical Explanation
Based on the Theory of Planned Behavior, this paper constructs a structural equation model of the factors influencing women’s fertility intentions, and obtains the theoretical model shown in
Figure 6.
Overall, economic support and public support have a significant positive effect on perceived behavioral control. Economic support significantly impacts perceived behavioral control and public support negatively impacts perceived behavioral control, while family support and policy support do not have significant impacts on it. Economic support, family support, policy support, and public support have a significant positive effect on behavioral attitudes, in which economic support has the largest effect, followed by economic support, family support, policy support, and public support. Perceived behavioral control and behavioral attitude impact fertility intentions positively, in which behavioral attitude has the larger effect. The results are shown as follows.
(1) The role of economic support in perceived behavioral control
The standardized path coefficient of economic support affecting perceived behavioral control is 0.249, which means that if economic support increases by one standard deviation, perceived behavioral control will increase by 0.249 standard deviations. It can be seen from
Figure 5 that the standardized path coefficient jj2 in the observed variables is the largest, at 0.83, indicating that increasing income has the greatest impact on perceived behavioral control, can greatly improve the confidence of women of childbearing age in reproductive behavior and their birth ability, and thus promote their fertility willingness. This conclusion is consistent with previous studies. For example, Karabchuk [
29] pointed out that work and income instability were important drivers of declining birth rates.
(2) The role of perceived risk in perceived behavioral control
The standardized path coefficient of perceived risk affecting perceived behavioral control is −0.251, which means that if perceived risk increases by one unit, perceived behavioral control will be reduced by 0.251 units. Perceived risk during the epidemic contains many elements; for example, Liu et al. [
30] pointed out that insufficient access to activities that fulfill fundamental needs would cause mental health issues. The perceived risks defined in this paper include the health risks, unemployment risks and psychological risks caused by the epidemic. The existence of these risks reduces women’s confidence in childbirth, and thus has a negative effect on women’s fertility intention.
(3) The role of family support in perceived behavioral control
Family support includes three parts: support from family members, family members’ situation, and family living environment. Perceived behavioral control is the degree to which individuals perceive their fertility behaviors to be controlled. Individuals consider the ability, resources, and opportunities they have to give birth, as well as the health status of the couple, job opportunities, economic situation, and the possibility that a babysitter can help them take care of the child. When there are more relevant resources and opportunities, the perceived behavioral control and fertility intentions are stronger. For example, Lin et al. [
24] confirmed that family support impacts perceived behavioral controlpositively. However, family support has no significant effect on perceived behavioral control when constructing a structural equation model, because the questionnaire in this paper was released during the period when the more infectious COVID variant strain Omicron was taking hold.
During this period, respondents perceived more risks, such as health and unemployment risks. We suggest in
Section 2 that the epidemic impacts women’s employment and health, while it is verified in
Section 4.4.5 that perceived risk has a significant negative effect on perceived behavioral control, and the positive effect of family support on perceived behavioral control may be offset by the negative effect of perceived risk on it. In other words, respondents perceive that family support is not sufficient to equip them for childbearing and parenting during the epidemic. In addition, most of the respondents in this paper have college and above degrees, and are more likely to have the ability to overcome barriers to childbirth. Liefbroer [
31] pointed out that for women, a high level of education meant a high opportunity cost of fertility, in that family and career conflicts might weaken their belief in fertility control. As such, with the development of their career, women tended to adjust their fertility intentions downward.
(4) The role of public support and policy support in perceived behavioral control
The standardized path coefficient of public support affecting perceived behavioral control is 0.211, which means that if public support increases by one unit, perceived behavioral control will increase by 0.211 units. Adequate labor rights protection and high-quality public service provision are important to easing the family–career conflicts of working women and improving their beliefs about birth control. Sound job security and social care resource support help boost the fertility intentions of women of childbearing age in China. This conclusion is the same as in the study of Tang and Li [
32], which pointed out that rural–urban migrants were more vulnerable during the pandemic due to poor public support or policy support. In addition, they have faced various discriminations caused by containment interventions [
33]. These may make childbearing even more difficult than for other populations. However, our analysis via structural equation modeling demonstrates that that policy support has no significant effect on perceived behavioral control. The reason for this is that the design of the measurement questions of the latent variable policy support refers to Yang [
34], who focuses on whether policy awareness and support have a positive effect on perceived behavioral control, instead of focusing on specific fertility support measures, such as possible effects when increasing the construction of public child care services, which only shows that support for and knowledge of policies have no significant effect on women’s perceptions of their fertility. Therefore, it is rational to believe that policy support has no significant impact on perceived behavioral control.
(5) The role of economic support, family support, policy support and public support in behavioral attitudes
The standardized path coefficient of economic support affecting behavioral attitudes is 0.463, which means if economic support increases by one unit, behavioral attitudes will increase by 0.463 units. The standardized path coefficients of family support, policy support, and public support affecting behavioral attitudes are 0.227, 0.238, and 0.200, respectively, which are significantly smaller than 0.463, indicating that the effect of economic support on behavioral attitudes is the largest. In other words, the economic recession caused by COVID-19 has reduced their expectations and happiness regarding future births, increased their insecurity, and thus reduced their willingness to have children [
35].
(6) The role of perceived behavioral control and behavioral attitudes in fertility intentions
The standardized path coefficient of perceived behavioral control affecting fertility intentions was 0.232, which means if perceived behavioral control increases by one unit, fertility intentions will increase by 0.232 units. The standardized path coefficient of behavioral attitudes affecting fertility intentions is 0.614, meaning if behavioral attitudes increase by one unit, fertility intentions will increase by 0.614 units, which is significantly greater than 0.232, indicating that behavioral attitudes have the greatest effect on fertility intentions. However, relevant studies have shown that perceived behavioral control has the greatest impact on behavioral intention [
19], which is different from this conclusion. The reason for this is that the study focuses on women of childbearing age, and most respondents have two expectations regarding the number of children. In addition, Billari et al. [
23] pointed out that in the case of intentions for a second child, the dominating variable for women is the one comprising positive attitudes towards a birth, while for men it is perceived control. Therefore, the result is reasonable.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}