2.1. Hypothesis Development
Technological advancement in the medical field provided safety measures and cures for prevalent diseases. Diseases such as COVID-19 emerge and severely impact the health of people and workers. Any disease or pandemic greatly impacts people’s lives and economic conditions [
22,
23]. Kaye et al. enumerated the elective procedures of safety protocols and measures that were efficacious in reducing the dominance of COVID-19 anxiety among hospital workers [
24,
25,
26]. The pandemic impacted the global financial situation, by raising the inflation level of almost all commodities. The increase in anxiety levels during COVID-19 disrupted everyday lives of people. The WHO positively introduced safety protocols comprising the use of various aspects of dressings, masks, distancing, and precautionary medication for health and hospital workers.
Yim et al. analyzed the strategies of maintaining safety measures and prerequisites in the hospitals during the COVID-19 pandemic to eliminate anxiety [
27]. The COVID-19 safety protocols were found to have a positive effect on people, specifically hospital workers, because they could save many lives. These safety protocols were initially organized when COVID-19 emerged in China. However, the anxiety levels were enhanced due to the closure of businesses and the need to maintain distance. This enhancement negatively influenced hospital workers’ mental health, because they could not meet with their loved ones. Even though the hospital workers were restrained, a ban was imposed on movements from the hospitals. Therefore, the hospital workers faced tremendous anxiety and depression that disrupted their everyday lives and their relationships with their family members.
Siegel et al. examined the symptoms of stress, emotions, sensitivity, and anxiety during COVID-19 to determine the mental health problems [
28]. COVID-19 anxiety increased among hospital workers, and many of their family members suffered from depression and anxiety. The pandemic negatively impacted the life and health of hospital workers, and many suffered from other diseases. Safety protocols had a positive role in reducing anxiety, but the fear of disease was too prominent to eliminate all the gaps that could reduce the anxiety levels. Thus, the hypothesis derived from the above discussion is as follows:
H1: COVID-19 safety protocols significantly influence COVID-19 anxiety.
Every individual in the world experiences anxiety at some point, whether it pertains to life or professionalism [
29]. Anxiety is a feeling individuals encounter in performing tasks in their lives. Improper availability of time also leads to anxiety. Some people have anxiety due to diseases or the diseases of their loved ones. Mohanty et al. investigated the attitudes associated with COVID-19 anxiety that intentionally impacted the mental health of hospital workers where precautionary measures were not adopted [
30]. Mattila et al. enumerated the associated factors of COVID-19 anxiety that dominantly prevailed among hospital workers and influenced their mental health [
31]. The diseases were less infectious than the fear. These immediate effects were compromised by some international news that sudden death due to COVID-19 was unstoppable and a patient would not have time after receiving a positive result.
The predictors of mental health help in understanding the reasons for psychological anxiety among health workers. Caycho-Rodríguez et al. discussed the predictors of mental health that primarily affected hospital workers and increased the levels of COVID-19 anxiety [
32]. Most types of COVID-19 anxiety are unpredictable. Some people experience anxiety due to their illness, and others experience anxiety as a result of the illness of their loved ones. Munyenyembe and Chen assessed quantitative COVID-19 anxiety strategies among health workers in controlling mental health [
33]. These negative impacts were the primary cause of COVID-19 anxiety that subsequently increased and disturbed hospital workers’ mental health.
The emotions of hospital workers were deadened during the first wave of COVID-19 in China, and people’s experiences were too punitive. Mittal et al. reported that during the waves of COVID-19, humanity faced a massive loss of mental strength that essentially indicated its future impact on hospital staff and workers [
34]. The hospital staff felt increasing levels of anxiety concerning patients, and many patients also died due to the same anxiety. This phenomenon diverted attention to other hospital workers who adopted preventive measures. Thus, the hypothesis derived from the above discussion is as follows:
H2: COVID-19 anxiety significantly influences mental health.
Anxiety is a dangerous element of human life that may cause additional damage to the organs of the human body. When people feel anxious for specific reasons, some body organs stop working, leading to dangerous health situations. Different aspects, such as exercise and artificial working, have highlighted the negativity of anxiety and unveiled the factors that could remove anxiety. Mohlman et al. explored COVID-19 inventories that were important in measuring the anxieties linked with the illness and mental health of hospital staff and workers [
35]. The human mind entertains hopes and situations which, when positively interpreted, can eliminate anxiety. COVID-19 is a dangerous disease that occurred in 2019 and impacted the whole world with depression and anxiety [
36]. Hagan et al. analyzed the mandate of vaccines as a safety measure and protocol during COVID-19 among hospital workers in a social justice policy [
37]. Anxiety affected the mental health and safety protocols, and clarifying it could safely manage the implications of safety protocols and stabilize mental health.
COVID-19 anxiety is one of the core elements that resulted in imbalance in the work–life balance of healthcare workers, and caused a lack of focus on professional obligations. It also affected the relationship between mental health of hospital workers and COVID-19 safety protocols. Karatepe et al. narrated the relationship between COVID-19 anxiety, stress, and mental health problems that could be addressed with proper safety protocols [
38]. People with solid psychological foundations controlled their anxiety levels by adapting safety protocols. Meanwhile, people with less solid psychological abilities could not control their anxiety by mediating between safety protocols and mental health.
Masjoudi et al. investigated the relationship among the elements COVID-19 anxiety, fear, and stress that favored self-care and helped in recovering from mental health disturbance [
39]. Muscular disorders prevailed due to the massive levels of anxiety. Uzunova et al. assessed the management and presentation of COVID-19 anxiety among hospital workers and individuals that significantly helped them recover from adverse mental health [
40]. Panic attacks were on the rise due to the obsessional behaviors of patients and hospital workers in response to COVID-19. These behaviors played a negative role in increasing the levels of COVID-19 anxiety that disrupted the mental health of many hospital workers. Good and controlled COVID-19 anxiety could improve the application of safety protocols in a mediating way to save mental health. Thus, the hypothesis derived from the above discussion is as follows:
H3: COVID-19 anxiety significantly mediates the relationship between COVID-19 safety protocols and mental health.
Safety protocols and anxiety during COVID-19 are interlinked with each other. Safety protocols play a vital role in the removal of COVID-19 anxiety. These safety protocols were established during the start of COVID-19 to restrain the effects of COVID-19 on unaffected people. Sakız and Aftab investigated the importance of psychological resilience and its dominant characteristics in adopting COVID-19 safety protocols for to control COVID-19 anxiety [
41]. The COVID-19 safety protocols provided feasible measures for people and hospital workers. These feasible safety measures involved various curative medications and items of clothing that helped hospital workers protect themselves from the infection.
Sharpley et al. asserted the effects of psychological resilience on the interactions between COVID-19 safety protocols and mental health counseling in hospital workers [
42]. Psychological resilience is crucial in COVID-19 anxiety and COVID-19 safety protocols. People with psychological resilience are eminently able in dealing with elements of anxiety. Hospital workers exhibiting psychological springiness are better able to deal with diseases. Carrnar rated the elements of protective glasses, masks, and social distancing COVID-19 safety protocols as important in decreasing anxiety through psychological resilience [
43].
Psychological resilience is essential regarding COVID-19 due to the impact of fear of it on health. Psychological resilience in hospital workers gave them the capability and ability to behave effectively and the mental process for speedy recovery and promotion of personal abilities [
44]. Arslan et al. discussed the effects of psychological resilience on the relationship between anxiety elements and the implications of safety protocols [
45] and found its moderating impact on COVID-19 safety protocols and COVID-19 anxiety.
Brown et al. indicated psychological resilience was essential in performing safety protocols to combat COVID-19 anxiety [
46]. All the harmful elements of this type of anxiety are effectively managed by inserting safety protocols moderated by psychological resilience. Managing the emotions and impulses of hospital workers is important because of their vital role in eliminating anxiety among patients. Effective management can be achieved by adopting safety protocols to appease COVID-19 anxiety, moderated by psychological resilience. Thus, the hypothesis derived from the above discussion is as follows:
H4: Psychological resilience significantly moderates between COVID-19 safety protocols and COVID-19 anxiety.
2.2. Data and Empirical Method
The article examined the impact of COVID-19 safety protocols on COVID-19 anxiety and its impact on the mental health of hospital workers. It also analyzed the moderating impact of psychological resilience regarding COVID-19 safety protocols and COVID-19 anxiety among hospital/health workers in China.
The employees of the designated treatment institutions for patients with COVID-19 in Chongqing China were the respondents.
There were two ways to distribute the questionnaire. First, the researchers directly distributed the questionnaire to the designated medical institutions for COVID-19. Second, the researchers mailed the questionnaire to worker at the designated medical institutions, who assisted the researchers in organizing colleagues to complete the questionnaire. After filling in the questionnaire, the respondent returned it to the author. Both methods were used. Before the questionnaire was issued, the subjects were informed of the important impact of the questionnaire on the research results, and the subjects were required to fill in the questionnaire carefully. At the same time, a small gift was given to each subject to arouse their attention. The author answered any questions concerning the questionnaire as soon as possible. Due to medical workers being extremely busy, the researchers sent 645 questionnaires and received 370 responses, representing around a 57.36 percent response rate. The specifics of the questionnaire are provided in
Appendix A.
The questionnaire consisted of the following four parts: basic information of the respondents, views on COVID-19 Safety Protocols, COVID-19 Anxiety status, and Mental Health status and Psychological Resilience. The demographic characteristics of the respondents included sex, age, education, professional title and years of service. The demographic information of the respondents is given in
Table 1.
The other three parts of the questionnaires had a five-point Likert scale from one for strongly disagree to five for strongly agree. The items were adopted from past studies. COVID-19 safety protocols had eight items, extracted from Taylor et al. [
47], COVID-19 anxiety had five items, taken from Lee [
48], mental health also had five items, taken from Berwick et al. [
49], and psychological resilience had twelve items, extracted from Scrivner et al. [
50]. The measurements and sources are given in
Table 2.
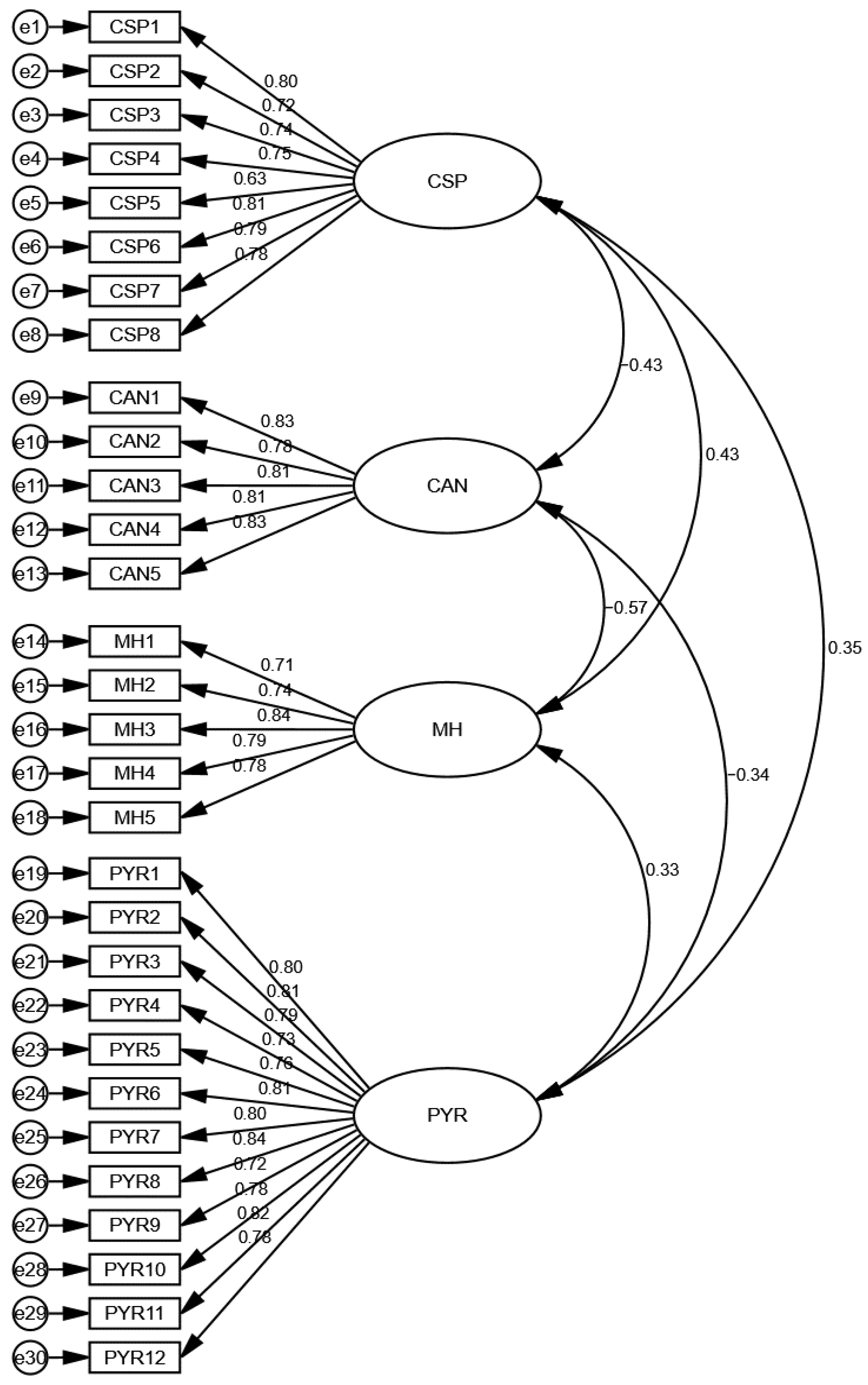
To test the pre-specified hypothesis, SEM was used for analysis, and the statistical software AMOS was used. The article applied AMOS to test the hypotheses and associations among variables. AMOS is an effective statistical tool for dealing with large and small sample sizes. In addition, it is also an effective tool that deals with complex models. It checks the reliability of the items and variables using measurement model assessment. The items’ reliability is checked using convergent validity tests like factor loadings, Alpha, and average variance extracted (AVE). The factor loadings and AVE values should be more than 0.50, while Alpha values should be more than 0.70. In addition, variables’ reliability was examined using a discriminant validity test like Fornell–Larcker, and the criteria were that the first value of the column should be larger than the other values in the same column [
51].
Moreover, good model fitness was also checked using the Tucker–Lewis index (TLI). The criteria for this test were that the value should be higher than 0.90. The model was also checked with the comparative fit index (CFI), and the criteria for the test was that the value should be higher than 0.90. Root mean square error of approximation (RMSEA) was applied and the criteria for the test was that the value should not be higher than 0.10 [
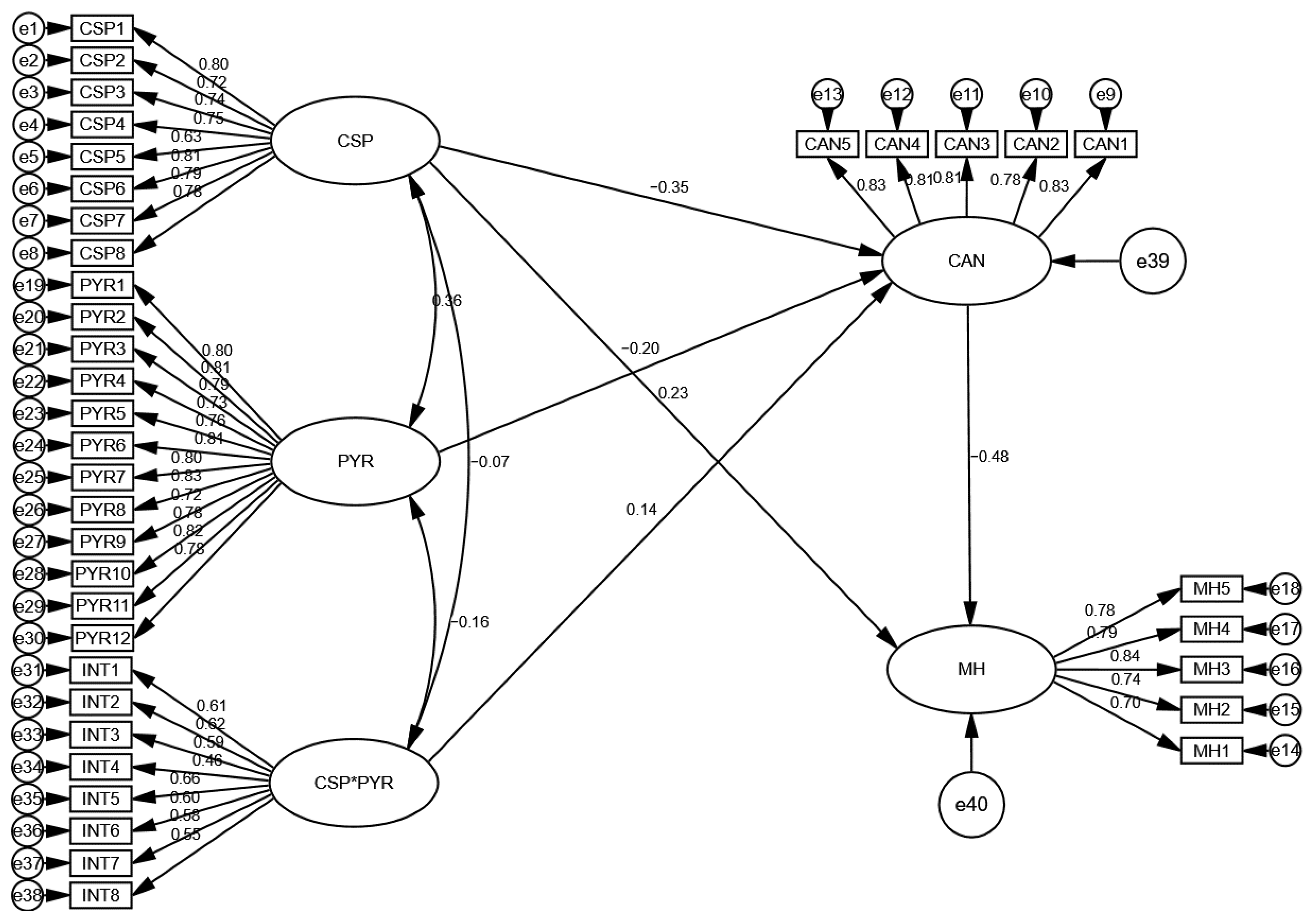
52]. Finally, the association among the variables was been examined using structural model assessment, and t-values and
p-values exposed the significance of the relationships. The relationship was significant if the t-values were more prominent than 1.64 and
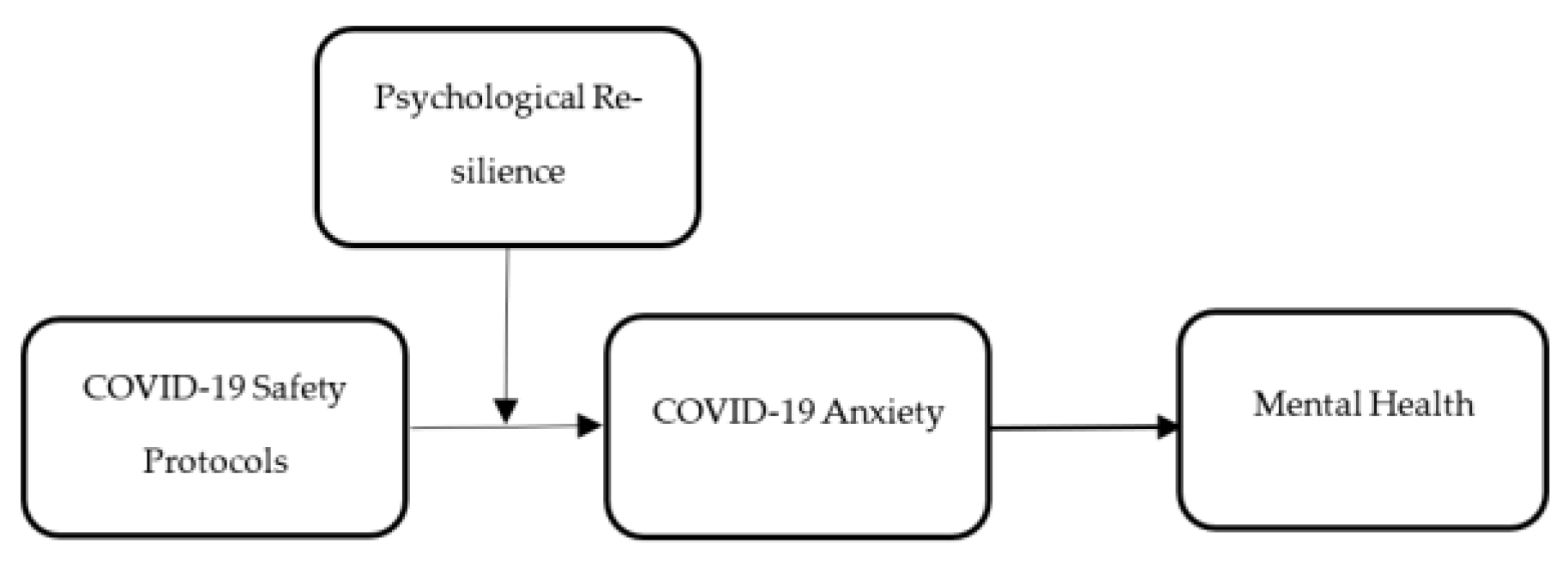
p-values were less than 0.05. Finally, the current study used the COVID-19 safety protocols (CSPs) as the independent variable, COVID-19 anxiety (CAN) as the mediating variable, mental health (MH) as the dependent variable, and psychological resilience (PYR) as the moderating variable. These constructs are given in
Figure 1.








{kind=link}
{kind=link}
{kind=link}