

Concurrence of Adenomyoepithelioma of the Breast and Gastrointestinal Stromal Tumor of the Stomach: A Case Report and Review of the Literature

Abstract
:1. Introduction
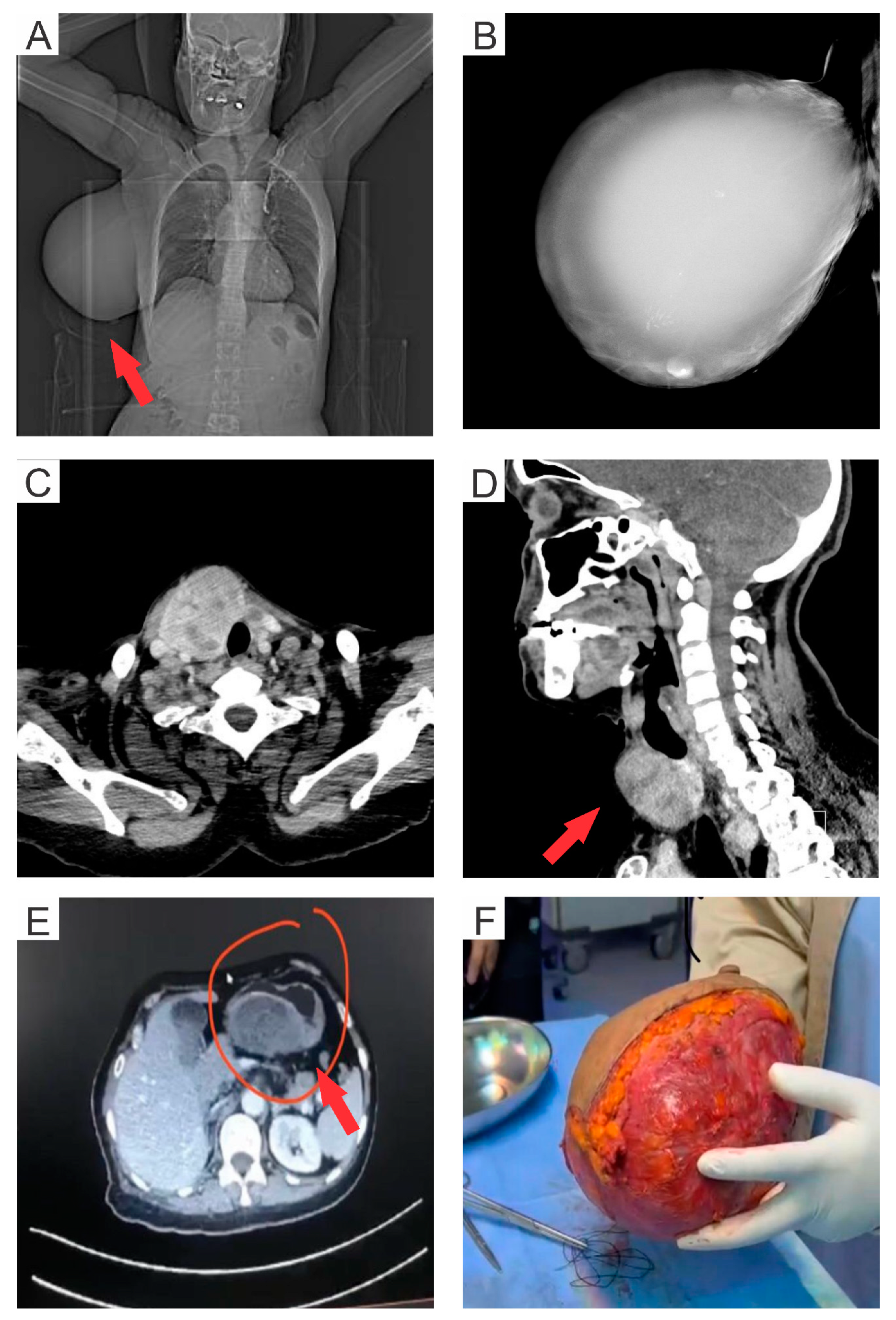
2. Case Presentation
Histology and Immunohistochemistry
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamperl, H. The myothelia (myoepithelial cells). Normal state; regressive changes; hyperplasia; tumors. Curr. Top. Pathol. 1970, 53, 161–220. [Google Scholar]
- Tavassoli, F.A. Myoepithelial lesions of the breast. Myoepitheliosis, adenomyoepithelioma, and myoepithelial carcinoma. Am. J. Surg. Pathol. 1991, 15, 554–568. [Google Scholar] [CrossRef] [PubMed]
- Tan, P.H.; Ellis, I.; Allison, K.; Brogi, E.; Fox, S.B.; Lakhani, S.; Lazar, A.J.; Morris, E.A.; Sahin, A.; Salgado, R.; et al. The 2019 World Health Organization classification of tumours of the breast. Histopathology 2020, 77, 181–185. [Google Scholar] [CrossRef]
- Yuan, Z.; Qu, X.; Zhang, Z.T.; Jiang, W.G. Lessons From Managing the Breast Malignant Adenomyoepithelioma and the Discussion on Treatment Strategy. World J. Oncol. 2017, 8, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Ito, R.; Ota, D.; Ando, S.; Mori, M.; Fukuuchi, A. A case of adenomyoepithelioma with myoepithelial carcinoma of the breast. Clin. Case Rep. 2019, 7, 930–934. [Google Scholar] [CrossRef]
- Kamei, M.; Daa, T.; Miyawaki, M.; Suehiro, S.; Sugio, K. Adenomyoepithelioma of the breast coexisting with ductal carcinoma in situ: A case report and review of the literature. Surg. Case Rep. 2015, 1, 81. [Google Scholar] [CrossRef]
- Kuroda, N.; Fujishima, N.; Ohara, M.; Hirouchi, T.; Mizuno, K.; Hayashi, Y.; Lee, G.H. Coexistent adenomyoepithelioma and invasive ductal carcinoma of the breast: Presentation as separate tumors. Med. Mol. Morphol. 2008, 41, 238–242. [Google Scholar] [CrossRef]
- Han, J.S.; Peng, Y. Multicentric adenomyoepithelioma of the breast with atypia and associated ductal carcinoma in situ. Breast J. 2010, 16, 547–549. [Google Scholar] [CrossRef] [PubMed]
- Warrier, S.; Hwang, S.; Ghaly, M.; Matthews, A. Adenomyoepithelioma with ductal carcinoma in situ: A case report and review of the literature. Case Rep. Surg. 2013, 2013, 521417. [Google Scholar] [CrossRef]
- Tokura, M.; Omi, Y.; Noguchi, E.; Yamamoto, T.; Kamio, T.; Okamoto, T. Two Cases of Malignant Adenomyoepithelioma of the Breast. Nihon Rinsho Geka Gakkai Zasshi (J. Jpn. Surg. Assoc.) 2018, 79, 294–301. [Google Scholar] [CrossRef]
- Gahlot, G.P.; Alam, A.; Takkar, P.; Jain, N.K.; Pothina, S.H.; Sharma, M. Breast adenomyoepithelioma with ductal carcinoma in situ: An unusual entity. Indian J. Case Rep. 2021, 7, 114–117. [Google Scholar] [CrossRef]
- AlQurashi, M.; Abdel Hadi, M.; Binammar, A.A.; Al Muhanna, A.; Kussaibi, H.; Al Shammary, E. Adenomyoepithelioma of the Breast: A Report of 3 Cases. Am. J. Case Rep. 2022, 23, e936070. [Google Scholar] [CrossRef] [PubMed]
- Karthikeyan, M.; Kolandasamy, C.; Naganath Babu, O.L. Malignant Gastrointestinal Stromal Tumor of Rectum: A Case Report and Review of Literature. Surg. J. (N. Y.) 2022, 8, e60–e64. [Google Scholar] [CrossRef] [PubMed]
- Miettinen, M.; Sarlomo-Rikala, M.; Lasota, J. Gastrointestinal stromal tumors: Recent advances in understanding of their biology. Hum. Pathol. 1999, 30, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Pidhorecky, I.; Cheney, R.T.; Kraybill, W.G.; Gibbs, J.F. Gastrointestinal stromal tumors: Current diagnosis, biologic behavior, and management. Ann. Surg. Oncol. 2000, 7, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Nishida, T.; Blay, J.Y.; Hirota, S.; Kitagawa, Y.; Kang, Y.K. The standard diagnosis, treatment, and follow-up of gastrointestinal stromal tumors based on guidelines. Gastric Cancer 2016, 19, 3–14. [Google Scholar] [CrossRef]
- Hegyi, L.; Thway, K.; Newton, R.; Osin, P.; Nerurkar, A.; Hayes, A.J.; Fisher, C. Malignant myoepithelioma arising in adenomyoepithelioma of the breast and coincident multiple gastrointestinal stromal tumours in a patient with neurofibromatosis type 1. J. Clin. Pathol. 2009, 62, 653–655. [Google Scholar] [CrossRef]
- Parikh, P.; Jameel, Z.; Falcon, S.; Rosa, M.; Kiluk, J.; Hoover, S.; Soliman, H.; Ataya, D. Adenomyoepithelioma of the breast: Case series and literature review. Clin. Imaging 2021, 75, 157–164. [Google Scholar] [CrossRef]
- Ortega, J.M.G.; Cuevas, Z.C.L.; Soto, M.G.; Valdés, M.D.; Parets, D.L.N.; Acosta, A.F. Adenomyoepithelioma of the breast. A case presentation. Rev. Méd. Electrón. 2019, 41, 733–740. [Google Scholar]
- Maeda, H.; Yokoi, S.; Nakazawa, M.; Koneri, K.; Imamura, Y.; Yamaguchi, A. Adenomyoepithelial adenosis associated with breast cancer: A case report and review of the literature. Springerplus 2013, 2, 50. [Google Scholar] [CrossRef]
- Khurana, A.; Jalpota, Y. Myoepithelial carcinoma arising in an adenomyoepithelioma of the breast: A case report of a rare entity. Indian J. Pathol. Microbiol. 2010, 53, 310–312. [Google Scholar] [CrossRef]
- Chen, F.; Wu, H.; Liu, Y.; Lv, M.; Zhong, J. Adenomyoepithelioma of the breast with prominent cystic changes: A case report. BMC Womens Health 2021, 21, 284. [Google Scholar] [CrossRef] [PubMed]
- Amano, Y.; Sakaguchi-Tamba, M.; Sasaki, Y.; Oshiro, H.; Fukushima, N.; Fujita, T.; Masuda, S.; Niki, T. Adenomyoepithelioma with a human epidermal growth factor receptor 2-fluorescence in situ hybridization-confirmed ductal carcinoma in situ component: A case report and review of the literature. Medicine (Baltimore) 2020, 99, e22665. [Google Scholar] [CrossRef]
- Laforga, J.B.; Aranda, F.I.; Sevilla, F. Adenomyoepithelioma of the breast: Report of two cases with prominent cystic changes and intranuclear inclusions. Diagn. Cytopathol. 1998, 19, 55–58. [Google Scholar] [CrossRef]
- Akrida, I.; Mulita, F. The clinical significance of HER2 expression in DCIS. Med. Oncol. 2022, 40, 16. [Google Scholar] [CrossRef] [PubMed]
- Moro, K.; Sakata, E.; Nakahara, A.; Hashidate, H.; Gabriel, E.; Makino, H. Malignant adenomyoepithelioma of the breast. Surg. Case Rep. 2020, 6, 118. [Google Scholar] [CrossRef]
- Lee, S.; Oh, S.Y.; Kim, S.H.; Lee, J.H.; Kim, D.C.; Cho, S.H.; Lee, M.; Kim, H.J. Malignant Adenomyoepithelioma of the Breast and Responsiveness to Eribulin. J. Breast Cancer 2015, 18, 400–403. [Google Scholar] [CrossRef]
- Parab, T.M.; DeRogatis, M.J.; Boaz, A.M.; Grasso, S.A.; Issack, P.S.; Duarte, D.A.; Urayeneza, O.; Vahdat, S.; Qiao, J.H.; Hinika, G.S. Gastrointestinal stromal tumors: A comprehensive review. J. Gastrointest. Oncol. 2019, 10, 144–154. [Google Scholar] [CrossRef]
- Kazuma, S.M.E.; Chirengendure, B.; Musonda, P.; Musowoya, J.; Ngoma, R.; Kaela, B.; Luyando, S.; Mundia, K. Review of Management of Gastrointestinal Stromal Tumor in Low-Resource Centers. Eur. J. Clin. Med. 2021, 2, 5–9. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Age | Ethnicity | Tumor Characteristics | Management |
|---|---|---|---|---|---|
| Naoto Kuroda et al. [7] | 2008 | 66 | Japanese | Coexistence of benign AME with DCIS | Partial mastectomy |
| Jeong S. Han and Yan Peng [8] | 2010 | 55 | ND | Coexistence of benign AME with DCIS | Total mastectomy |
| Sanjay Warrier et al. [9] | 2013 | 55 | Australian | Coexistence of benign AME with DCIS | Adjuvant radiotherapy and mastectomy with reconstruction |
| Hiroyuki Maeda et al. [20] | 2013 | 35 | Japanese | Coexistence of benign AME with DCIS | Adjuvant endocrine therapy and mastectomy |
| Mirei Kamei et al. [6] | 2015 | 71 | Japanese | Coexistence of benign AME with DCIS | Mastectomy |
| Momoko Tokura et al. [10] | 2018 | 68 | Japanese | Coexistence of benign AME with DCIS | Partial mastectomy |
| Gaurav P. Gahlot et al. [11] | 2021 | 51 | Indian | Coexistence of benign AME with DCIS | Modified radical mastectomy |
| Mariam AlQurashi et al. [12] | 2022 | 49 | Saudi | Coexistence of benign AME with DCIS | Mastectomy |
| Hegyi L. et al. [17] | 2015 | 41 | Caucasian | Malignant myoepithelioma of the breast and GIST of the small bowel developed in patient with neurofibromatosis type 1 (NF-1) | Right simple mastectomy with excision of the pectoral fascia and GIST excised by limited resection |
| Present study | 2023 | 56 | Saudi | Coexistence of benign AME with DCIS and spindle cell-type GIST | Adjuvant therapy with total gastrectomy and mastectomy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Althoubaity, F.; Wazira, L.A.; Ahmad, H.M.Y.; Aljuhani, R.T. Concurrence of Adenomyoepithelioma of the Breast and Gastrointestinal Stromal Tumor of the Stomach: A Case Report and Review of the Literature. Med. Sci. 2023, 11, 57. https://doi.org/10.3390/medsci11030057
Althoubaity F, Wazira LA, Ahmad HMY, Aljuhani RT. Concurrence of Adenomyoepithelioma of the Breast and Gastrointestinal Stromal Tumor of the Stomach: A Case Report and Review of the Literature. Medical Sciences. 2023; 11(3):57. https://doi.org/10.3390/medsci11030057
Chicago/Turabian StyleAlthoubaity, Fatma, Lamar A. Wazira, Hanin M. Y. Ahmad, and Reyof T. Aljuhani. 2023. "Concurrence of Adenomyoepithelioma of the Breast and Gastrointestinal Stromal Tumor of the Stomach: A Case Report and Review of the Literature" Medical Sciences 11, no. 3: 57. https://doi.org/10.3390/medsci11030057