
Dexmedetomidine Has Differential Effects on the Contractility of Equine Jejunal Smooth Muscle Layers In Vitro
 , and
, and 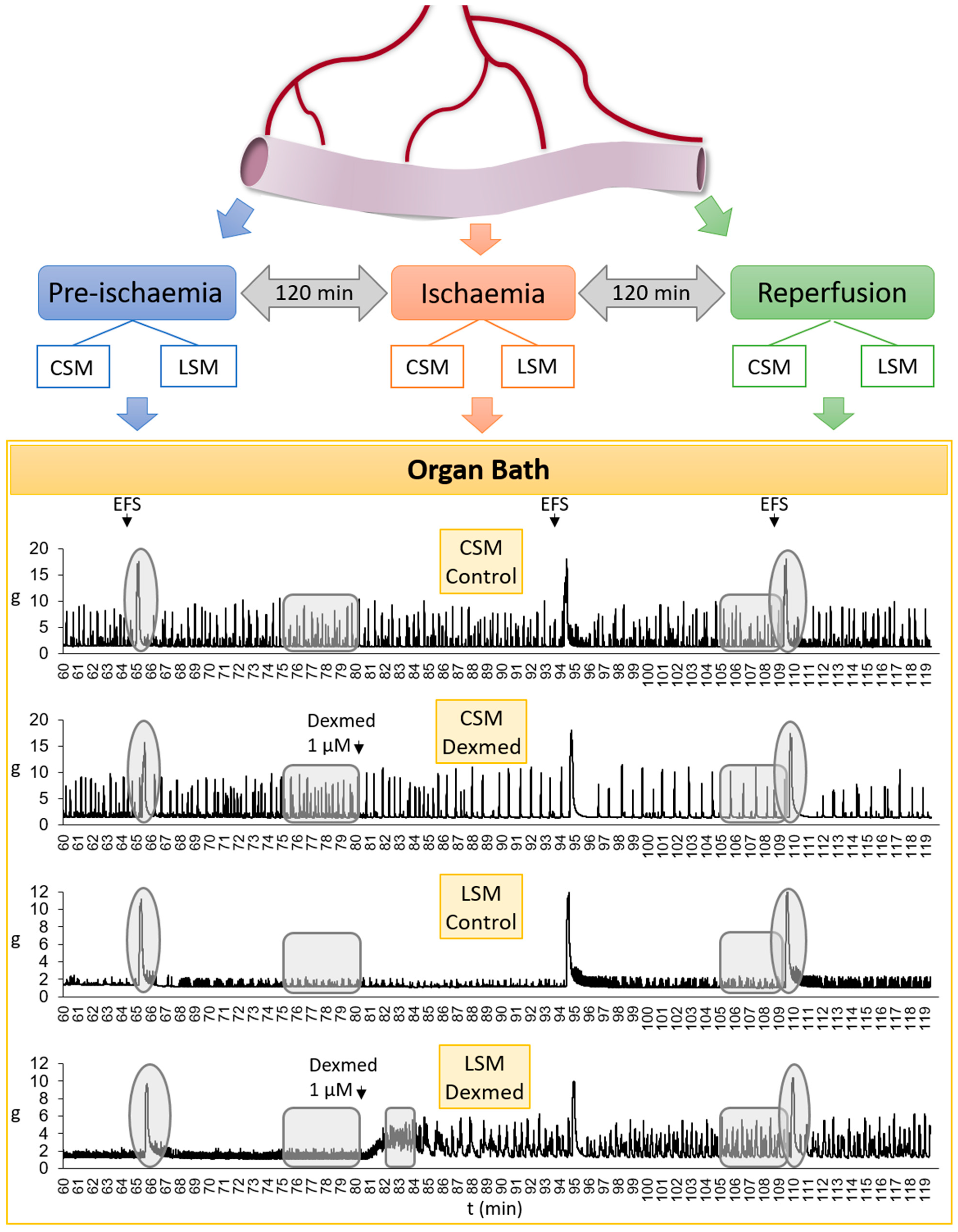{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Surgical Procedure
2.3. Organ Bath
2.3.1. In Vitro Experiment—Day 1
2.3.2. In Vitro Experiment—Day 2
2.4. Data Analysis
3. Results
3.1. Ischaemia Model
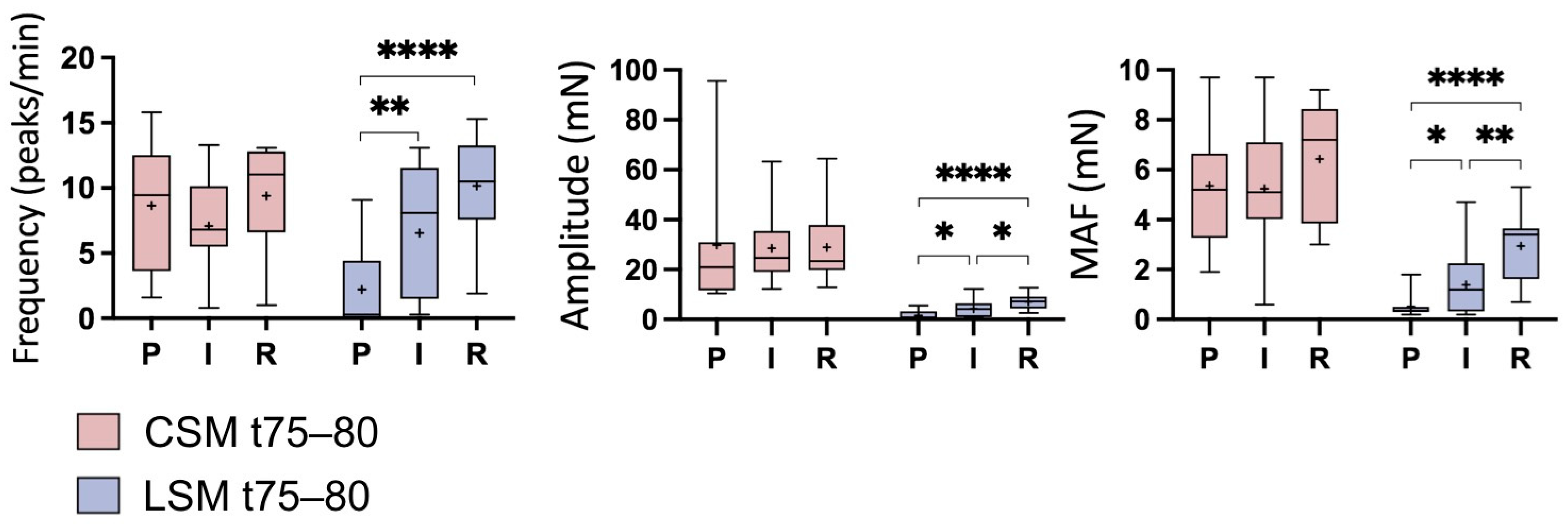
3.2. Basal Contractile Activity
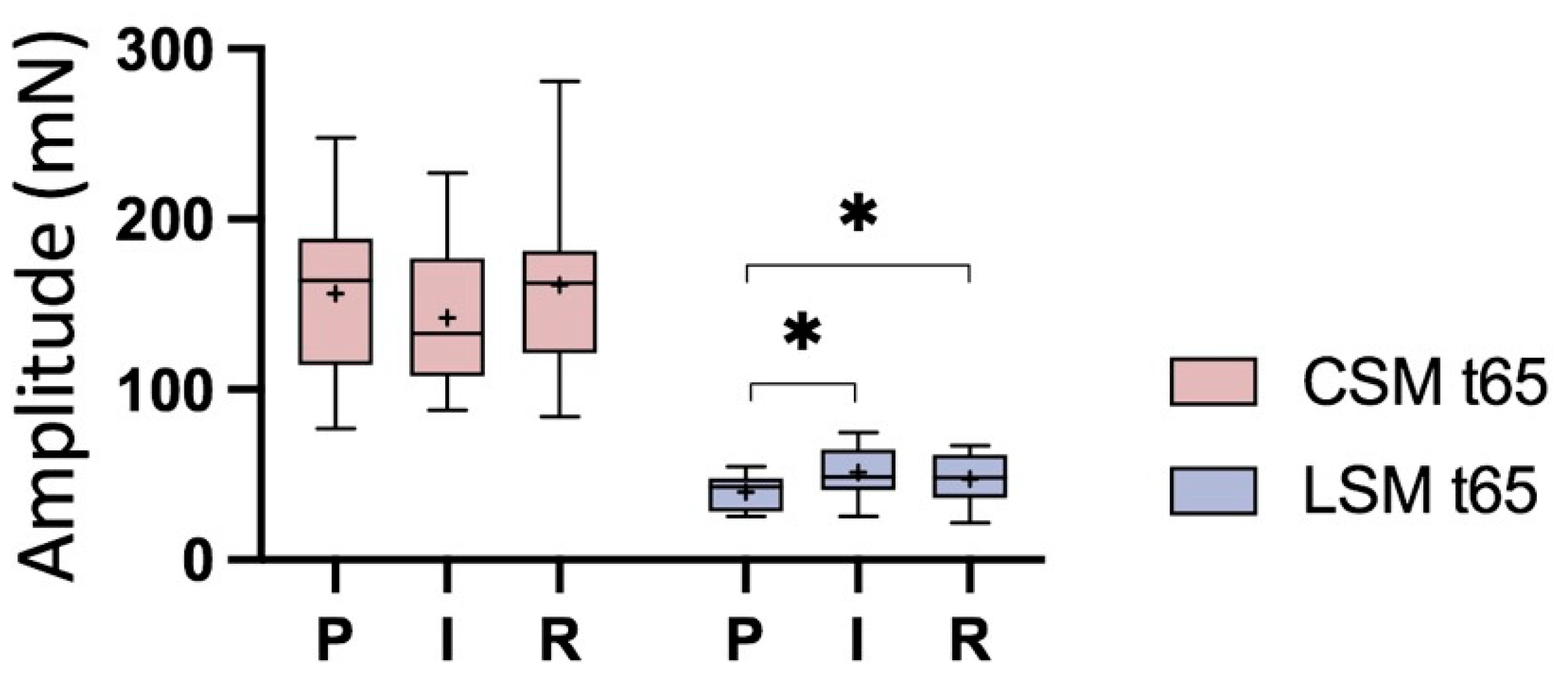
3.2.1. Ischaemia Phases
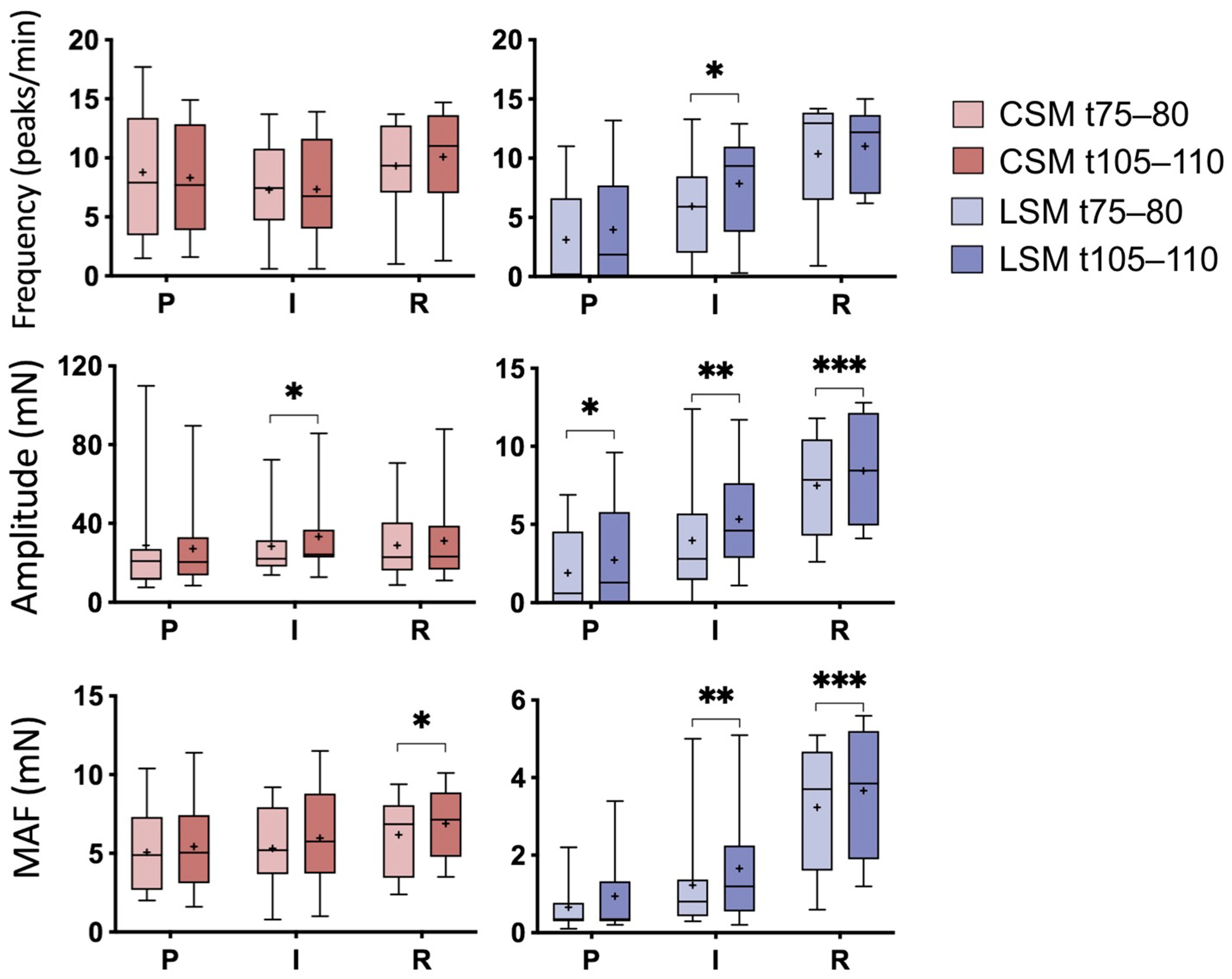
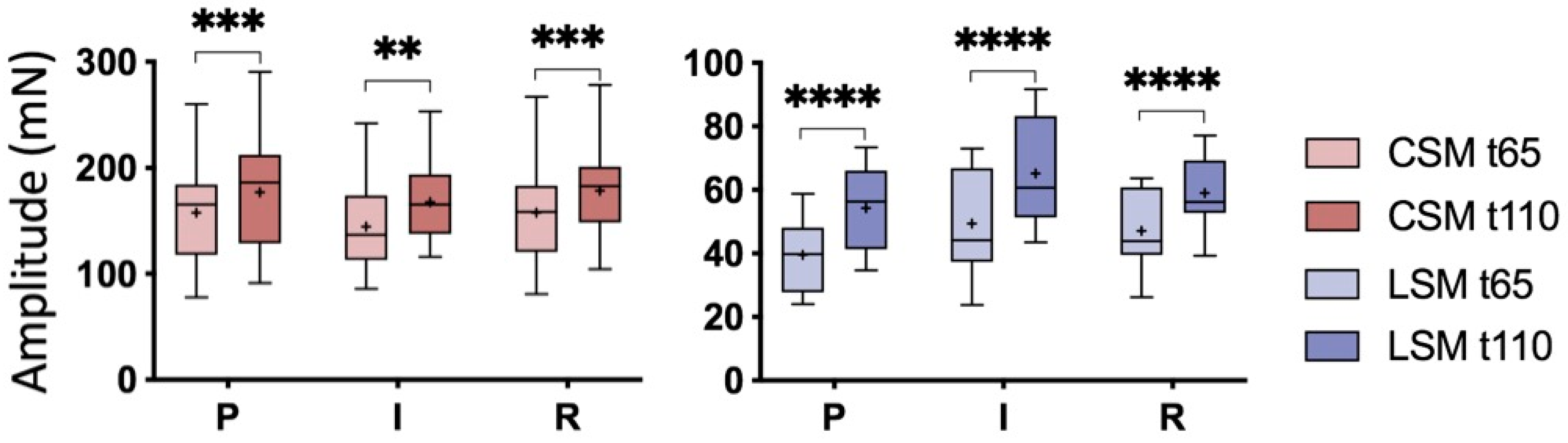
3.2.2. Development over Time without the Addition of Dexmed
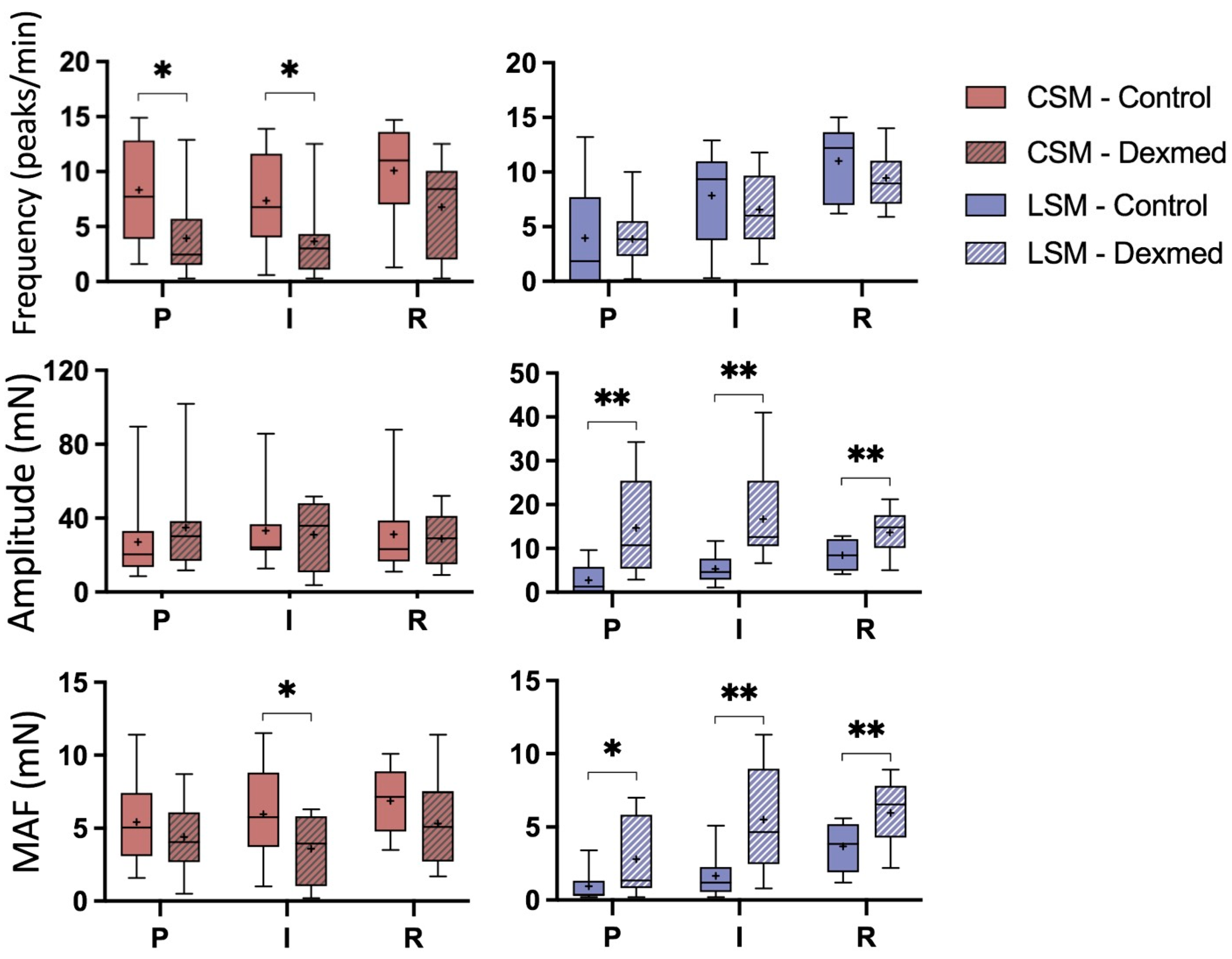
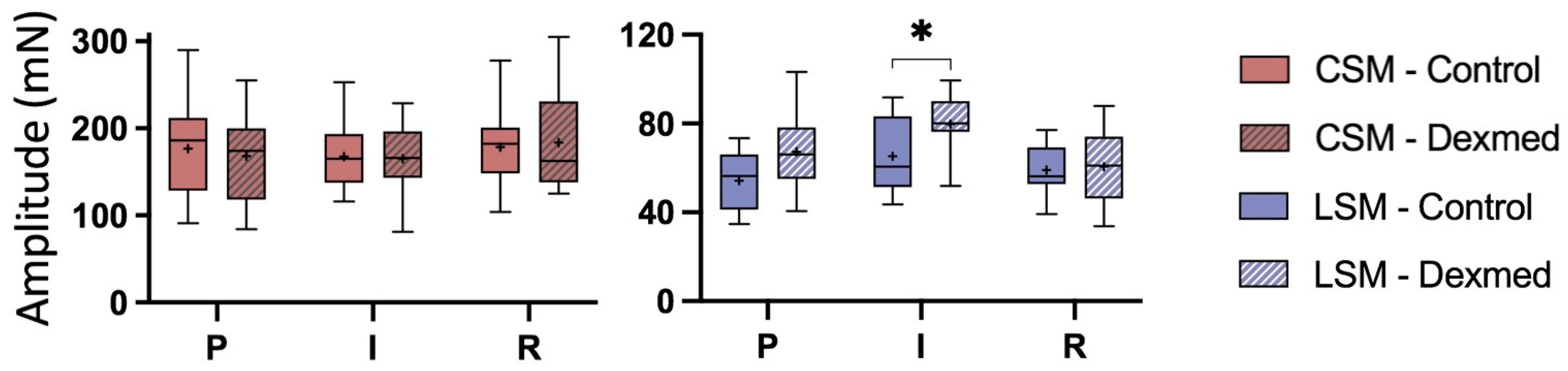
3.2.3. Effect of Dexmedetomidine Addition
3.3. Electrical Field Stimulation
3.3.1. Ischaemia Phases
3.3.2. Development over Time without the Addition of Dexmed
3.3.3. Effect of Dexmedetomidine Addition
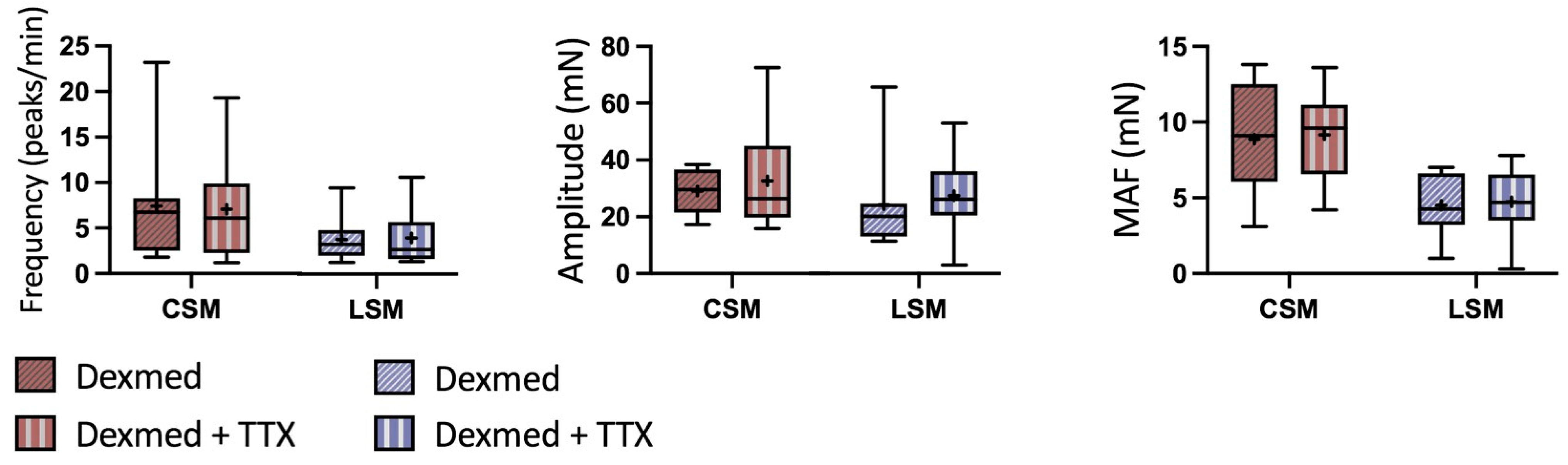
3.4. Day 2 of the In Vitro Experiment—Dexmedetomidine with and without TTX
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holcombe, S.J.; Rodriguez, K.M.; Haupt, J.L.; Campbell, J.O.; Chaney, K.P.; Sparks, H.D.; Hauptman, J.G. Prevalence of and risk factors for postoperative ileus after small intestinal surgery in two hundred and thirty-three horses. Vet. Surg. 2009, 38, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Mair, T.; Smith, L. Survival and complication rates in 300 horses undergoing surgical treatment of colic. Part 2: Short-term complications. Equine Vet. J. 2005, 37, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Boorman, S.; Stefanovski, D.; Southwood, L.L. Clinical findings associated with development of postoperative reflux and short-term survival after small intestinal surgery in geriatric and mature nongeriatric horses. Vet. Surg. 2019, 48, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Little, D.; Tomlinson, J.E.; Blikslager, A.T. Post operative neutrophilic inflammation in equine small intestine after manipulation and ischaemia. Equine Vet. J. 2005, 37, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Lisowski, Z.M.; Pirie, R.S.; Blikslager, A.T.; Lefebvre, D.; Hume, D.A.; Hudson, N.P.H. An update on equine post-operative ileus: Definitions, pathophysiology and management. Equine Vet. J. 2018, 50, 292–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boscan, P.; Van Hoogmoed, L.M.; Farver, T.B.; Snyder, J.R. Evaluation of the effects of the opioid agonist morphine on gastrointestinal tract function in horses. Am. J. Vet. Res. 2006, 67, 992–997. [Google Scholar] [CrossRef]
- Cohen, N.D.; Lester, G.D.; Sanchez, L.C.; Merritt, A.M.; Roussel, A.J. Evaluation of risk factors associated with development of postoperative ileus in horses. J. Am. Vet. Med. Assoc. 2004, 225, 1070–1078. [Google Scholar] [CrossRef]
- Hopster-Iversen, C.C.; Hopster, K.; Staszyk, C.; Rohn, K.; Freeman, D.E.; Rötting, A.K. Effects of experimental mechanical manipulations on local inflammation in the jejunum of horses. Am. J. Vet. Res. 2014, 75, 385–391. [Google Scholar] [CrossRef]
- Adams, S.; Lamar, C.; Masty, J. Motility of the distal portion of the jejunum and pelvic flexure in ponies: Effects of six drugs. Am. J. Vet. Res. 1984, 45, 795–799. [Google Scholar]
- Merritt, A.; Campbell-Thompson, M.; Lowrey, S. Effect of xylazine treatment on equine proximal gastrointestinal tract myoelectrical activity. Am. J. Vet. Res. 1989, 50, 945–949. [Google Scholar]
- Merritt, A.; Burrow, J.; Hartless, C. Effect of xylazine, detomidine, and a combination of xylazine and butorphanol on equine duodenal motility. Am. J. Vet. Res. 1998, 59, 619–623. [Google Scholar] [PubMed]
- Lester, G.; Merritt, A.; Neuwirth, L.; Vetro-Widenhouse, T.; Steible, C.; Rice, B. Effect of alpha 2-adrenergic, cholinergic, and nonsteroidal anti-inflammatory drugs on myoelectric activity of ileum, cecum, and right ventral colon and on cecal emptying of radiolabeled markers in clinically normal ponies. Am. J. Vet. Res. 1998, 59, 320–327. [Google Scholar] [PubMed]
- Elfenbein, J.R.; Sanchez, L.C.; Robertson, S.A.; Cole, C.A.; Sams, R. Effect of detomidine on visceral and somatic nociception and duodenal motility in conscious adult horses. Vet. Anaesth. Analg. 2009, 36, 162–172. [Google Scholar] [CrossRef]
- de Vries, A.; Pakkanen, S.A.; Raekallio, M.R.; Ekiri, A.; Scheinin, M.; Taylor, P.M.; Vainio, O.M. Clinical effects and pharmacokinetic variables of romifidine and the peripheral α2-adrenoceptor antagonist MK-467 in horses. Vet. Anaesth. Analg. 2016, 43, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Vainionpää, M.H.; Raekallio, M.R.; Pakkanen, S.A.; Ranta-Panula, V.; Rinne, V.M.; Scheinin, M.; Vainio, O.M. Plasma drug concentrations and clinical effects of a peripheral alpha-2-adrenoceptor antagonist, MK-467, in horses sedated with detomidine. Vet. Anaesth. Analg. 2013, 40, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Zullian, C.; Menozzi, A.; Pozzoli, C.; Poli, E.; Bertini, S. Effects of α2-adrenergic drugs on small intestinal motility in the horse: An in vitro study. Vet. J. 2011, 187, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Tapio, H.; Raekallio, M.R.; Mykkänen, A.; Männikkö, S.; Scheinin, M.; Bennett, R.C.; Vainio, O. Effects of vatinoxan on cardiorespiratory function and gastrointestinal motility during constant-rate medetomidine infusion in standing horses. Equine Vet. J. 2019, 51, 646–652. [Google Scholar] [CrossRef] [Green Version]
- Rezende, M.; Grimsrud, K.N.; Stanley, S.D.; Steffey, E.; Mama, K. Pharmacokinetics and pharmacodynamics of intravenous dexmedetomidine in the horse. J. Vet. Pharmacol. Ther. 2015, 38, 15–23. [Google Scholar] [CrossRef]
- Bettschart-Wolfensberger, R.; Freeman, S.; Bowen, I.; Aliabadi, F.; Weller, R.; Huhtinen, M.; Clarke, K. Cardiopulmonary effects and pharmacokinetics of iv dexmedetomidine in ponies. Equine Vet. J. 2005, 37, 60–64. [Google Scholar] [CrossRef]
- Bettschart-Wolfensberger, R.; Clarke, K.W.; Vainio, O.; Aliabadi, F.; Demuth, D. Pharmacokinetics of medetomidine in ponies and elaboration of a medetomidine infusion regime which provides a constant level of sedation. Res. Vet. Sci. 1999, 67, 41–46. [Google Scholar] [CrossRef]
- Abass, M.; Ibrahim, H.; Salci, H.; Hamed, M.A. Evaluation of the effect of different sedative doses of dexmedetomidine on the intestinal motility in clinically healthy donkeys (Equus asinus). BMC Vet. Res. 2022, 18, 274. [Google Scholar] [CrossRef] [PubMed]
- Memis, D.; Dokmeci, D.; Karamanlioglu, B.; Turan, A.; Ture, M. A comparison of the effect on gastric emptying of propofol or dexmedetomidine in critically ill patients. Crit. Care 2005, 9, P374. [Google Scholar] [CrossRef]
- Chen, C.; Huang, P.; Lai, L.; Luo, C.; Ge, M.; Hei, Z.; Zhu, Q.; Zhou, S. Dexmedetomidine improves gastrointestinal motility after laparoscopic resection of colorectal cancer: A randomized clinical trial. Medicine 2016, 95, e4295. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.Z.; Lu, Z.F.; Lv, X.Q.; Guo, Y.P.; Cui, X.G. Epidural Co-Administration of Dexmedetomidine and Levobupivacaine Improves the Gastrointestinal Motility Function after Colonic Resection in Comparison to Co-Administration of Morphine and Levobupivacaine. PLoS ONE 2016, 11, e0146215. [Google Scholar] [CrossRef] [Green Version]
- Shivaji, P.; Agrawal, S.; Kumar, A.; Bahadur, A. Evaluation of lignocaine, dexmedetomidine, lignocaine-dexmedetomidine infusion on pain and quality of recovery for robotic abdominal hysterectomy: A prospective randomized controlled trial. Braz. J. Anesthesiol. 2022, 72, 593–598. [Google Scholar] [CrossRef]
- Rekatsina, M.; Theodosopoulou, P.; Staikou, C. Effects of Intravenous Dexmedetomidine Versus Lidocaine on Postoperative Pain, Analgesic Consumption and Functional Recovery After Abdominal Gynecological Surgery: A Randomized Placebo-controlled Double Blind Study. Pain Physician 2021, 24, E997–E1006. [Google Scholar] [PubMed]
- Wu, Y.; Cai, Z.; Liu, L.; Wang, J.; Li, Y.; Kang, Y.; An, N. Impact of intravenous dexmedetomidine on gastrointestinal function recovery after laparoscopic hysteromyomectomy: A randomized clinical trial. Sci. Rep. 2022, 12, 1–9. [Google Scholar] [CrossRef]
- Xiang, H.; Hu, B.; Li, Z.; Li, J. Dexmedetomidine controls systemic cytokine levels through the cholinergic anti-inflammatory pathway. Inflammation 2014, 37, 1763–1770. [Google Scholar] [CrossRef]
- Sun, Y.; Gao, Q.; Wu, N.; Li, S.D.; Yao, J.X.; Fan, W.J. Protective effects of dexmedetomidine on intestinal ischemia-reperfusion injury. Exp. Ther. Med. 2015, 10, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Li, Y.; Tian, S.; Wang, H.; Wu, H.; Zhang, A.; Gao, C. Anti-inflammatory effects of perioperative dexmedetomidine administered as an adjunct to general anesthesia: A meta-analysis. Sci. Rep. 2015, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wang, Y.; Chang, H.; Cheng, B.; Miao, J.; Li, S.; Hu, H.; Huang, L.; Wang, Q. Inhibitory Effects of Dexmedetomidine and Propofol on Gastrointestinal Tract Motility Involving Impaired Enteric Glia Ca(2+) Response in Mice. Neurochem. Res. 2021, 46, 1410–1422. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Li, S.; Li, Y.; Hu, H.; Cheng, B.; Miao, J.; Gao, H.; Ma, H.; Gao, Y.; Wang, Q. Effect of sedation with dexmedetomidine or propofol on gastrointestinal motility in lipopolysaccharide-induced endotoxemic mice. BMC Anesthesiol. 2020, 20, 227. [Google Scholar] [CrossRef] [PubMed]
- Herbert, M.K.; Roth-Goldbrunner, S.; Holzer, P.; Roewer, N. Clonidine and dexmedetomidine potently inhibit peristalsis in the Guinea pig ileum in vitro. Anesthesiology 2002, 97, 1491–1499. [Google Scholar] [CrossRef]
- Aydin, C.; Bagcivan, I.; Gursoy, S.; Altun, A.; Topcu, O.; Koyuncu, A. Altered spontaneous contractions of the ileum by anesthetic agents in rats exposed to peritonitis. World J. Gastroenterol. 2009, 15, 1620–1624. [Google Scholar] [CrossRef] [PubMed]
- Iirola, T.; Vilo, S.; Aantaa, R.; Wendelin-Saarenhovi, M.; Neuvonen, P.; Scheinin, M.; Olkkola, K. Dexmedetomidine inhibits gastric emptying and oro-caecal transit in healthy volunteers. Br. J. Anaesth. 2011, 106, 522–527. [Google Scholar] [CrossRef] [Green Version]
- Malone, E.D.; Brown, D.R.; Trent, A.M.; Turner, T.A. Influence of adrenergic and cholinergic mediators on the equine jejunum in vitro. Am. J. Vet. Res. 1996, 57, 884–890. [Google Scholar] [PubMed]
- Guschlbauer, M.; Hoppe, S.; Geburek, F.; Feige, K.; Huber, K. In vitro effects of lidocaine on the contractility of equine jejunal smooth muscle challenged by ischaemia-reperfusion injury. Equine Vet. J. 2010, 42, 53–58. [Google Scholar] [CrossRef]
- Malone, E.D.; Kannan, M.S. Effects of intestinal ischemia on in vitro activity of adjacent jejunum in samples obtained from ponies. Am. J. Vet. Res. 2001, 62, 1973–1978. [Google Scholar] [CrossRef]
- Parlar, A.; Arslan, S.O. Resveratrol normalizes the deterioration of smooth muscle contractility after intestinal ischemia and reperfusion in rats associated with an antioxidative effect and modulating tumor necrosis factor alpha activity. Ann. Vasc. Surg. 2019, 61, 416–426. [Google Scholar] [CrossRef]
- Angeles-López, G.E.; González-Trujano, M.E.; Déciga-Campos, M.; Ventura-Martínez, R. Neuroprotective evaluation of Tilia americana and Annona diversifolia in the neuronal damage induced by intestinal ischemia. Neurochem. Res. 2013, 38, 1632–1640. [Google Scholar] [CrossRef]
- Kurahashi, M.; Kito, Y.; Hara, M.; Takeyama, H.; Sanders, K.M.; Hashitani, H. Norepinephrine Has Dual Effects on Human Colonic Contractions Through Distinct Subtypes of Alpha 1 Adrenoceptors. Cell. Mol. Gastroenterol. Hepatol. 2020, 10, 658–671.e651. [Google Scholar] [CrossRef] [PubMed]
- Larauche, M.; Kiank, C.; Tache, Y. Corticotropin releasing factor signaling in colon and ileum: Regulation by stress and pathophysiological implications. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2009, 60 (Suppl. S7), 33–46. [Google Scholar]
- Mallesh, S.; Schneider, R.; Schneiker, B.; Lysson, M.; Efferz, P.; Lin, E.; de Jonge, W.J.; Wehner, S. Sympathetic Denervation Alters the Inflammatory Response of Resident Muscularis Macrophages upon Surgical Trauma and Ameliorates Postoperative Ileus in Mice. Int. J. Mol. Sci. 2021, 22, 6872. [Google Scholar] [CrossRef]
- Murray, A.; Pearson, G.; Cottrell, D. In vitro response to noradrenaline of small intestine taken from normal and grass sickness-affected horses. Vet. Res. Commun. 1997, 21, 571–585. [Google Scholar] [CrossRef]
- Liu, L.; Coupar, I.M. Characterisation of pre-and post-synaptic α-adrenoceptors in modulation of the rat ileum longitudinal and circular muscle activities. Naunyn-Schmiedeberg’s Arch. Pharmacol. 1997, 356, 248–256. [Google Scholar] [CrossRef]
- Sarna, S.K. Gastrointestinal longitudinal muscle contractions. Am. J. Physiol. -Gastrointest. Liver Physiol. 1993, 265, G156–G164. [Google Scholar] [CrossRef] [PubMed]
- Traserra, S.; Villarte, S.; Traini, C.; Palacin, S.; Vergara, P.; Vannucchi, M.G.; Jimenez, M. The asymmetric innervation of the circular and longitudinal muscle of the mouse colon differently modulates myogenic slow phasic contractions. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2020, 32, e13778. [Google Scholar] [CrossRef]
- Menozzi, A.; Pozzoli, C.; Poli, E.; Dacasto, M.; Giantin, M.; Lopparelli, R.; Passeri, B.; Zullian, C.; Gobbetti, T.; Bertini, S. Effects of nonselective and selective cyclooxygenase inhibitors on small intestinal motility in the horse. Res. Vet. Sci. 2009, 86, 129–135. [Google Scholar] [CrossRef]
- Re, G.; Badino, P.; Odore, R.; Galaverna, D.; Girardi, C. Characterization of α-adrenoceptor subtypes in smooth muscle of equine ileum. Am. J. Vet. Res. 2001, 62, 1370–1374. [Google Scholar] [CrossRef]
- Ali, A.; Cheng, H.Y.; Ting, K.N.; Wilson, V.G. Rilmenidine reveals differences in the pharmacological characteristics of prejunctional alpha2-adrenoceptors in the guinea-pig, rat and pig. Br. J. Pharmacol. 1998, 125, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Hudson, N.; Mayhew, I.; Pearson, G. In vitro microelectrode study of the electrical properties of smooth muscle in equine ileum. Vet. Rec. 2001, 149, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.Y.; Choi, S.; Yeum, C.H.; Chang, I.Y.; Park, C.K.; Kim, M.Y.; Kong, I.D.; So, I.; Kim, K.W.; You, H.J. Noradrenaline inhibits pacemaker currents through stimulation of β1-adrenoceptors in cultured interstitial cells of Cajal from murine small intestine. Br. J. Pharmacol. 2004, 141, 670–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colucci, R.; Blandizzi, C.; Carignani, D.; Placanica, G.; Lazzeri, G.; Del Tacca, M. Effects of imidazoline derivatives on cholinergic motility in guinea-pig ileum: Involvement of presynaptic alpha2-adrenoceptors or imidazoline receptors? Naunyn-Schmiedeberg’s Arch. Pharmacol. 1998, 357, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Hieble, J.P.; Ruffolo Jr, R.R. Possible structural and functional relationships between imidazoline receptors and α2-adrenoceptors. Ann. N. Y. Acad. Sci. 1995, 763, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Colucci, R.; Blandizzi, C.; Carignani, D.; Lazzeri, G.; Natale, G.; Crema, F.; Del Tacca, M. Determination on functional basis of presynaptic alpha 2-adrenoceptor subtypes in guinea-pig duodenum. Neurosci. Lett. 1996, 210, 29–32. [Google Scholar] [CrossRef]
- Scheibner, J.; Trendelenburg, A.U.; Hein, L.; Starke, K.; Blandizzi, C. Alpha 2-adrenoceptors in the enteric nervous system: A study in alpha 2A-adrenoceptor-deficient mice. Br. J. Pharmacol. 2002, 135, 697–704. [Google Scholar] [CrossRef] [Green Version]
- König, K.S.; Verhaar, N.; Hopster, K.; Pfarrer, C.; Neudeck, S.; Rohn, K.; Kästner, S.B. Ischaemic preconditioning and pharmacological preconditioning with dexmedetomidine in an equine model of small intestinal ischaemia-reperfusion. PLoS ONE 2020, 15, e0224720. [Google Scholar] [CrossRef]
- VanderBroek, A.R.; Engiles, J.B.; Kästner, S.B.R.; Kopp, V.; Verhaar, N.; Hopster, K. Protective effects of dexmedetomidine on small intestinal ischaemia-reperfusion injury in horses. Equine Vet. J. 2021, 53, 569–578. [Google Scholar] [CrossRef]
- Hector, R.C.; Rezende, M.L.; Nelson, B.B.; Monnet, E. Cardiopulmonary function and intestinal blood flow in anaesthetised, experimentally endotoxaemic horses given a constant rate infusion of dexmedetomidine. Equine Vet. J. 2022, 54, 820–828. [Google Scholar] [CrossRef]
- Hernández, G.; Tapia, P.; Alegría, L.; Soto, D.; Luengo, C.; Gomez, J.; Jarufe, N.; Achurra, P.; Rebolledo, R.; Bruhn, A. Effects of dexmedetomidine and esmolol on systemic hemodynamics and exogenous lactate clearance in early experimental septic shock. Crit. Care 2016, 20, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Wittenberg-Voges, L.; Kastner, S.B.; Raekallio, M.; Vainio, O.M.; Rohn, K.; Hopster, K. Effect of dexmedetomidine and xylazine followed by MK-467 on gastrointestinal microperfusion in anaesthetized horses. Vet. Anaesth. Analg. 2018, 45, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Risberg, A.; Spadavecchia, C.; Ranheim, B.; Krontveit, R.; Haga, H.A. Antinociceptive effects of three escalating dexmedetomidine and lignocaine constant rate infusions in conscious horses. Vet. J. 2014, 202, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Melville, J.; Macagno, E.; Christensen, J. Longitudinal contractions in the duodenum: Their fluid-mechanical function. Am. J. Physiol. -Leg. Content 1975, 228, 1887–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafik, A.; Shafik, A.A.; Ahmed, I. Role of the longitudinal smooth muscle coat in the ileal motile activity: Evidence of ileo–ileal inhibitory reflex. J. Gastroenterol. Hepatol. 2002, 17, 1267–1271. [Google Scholar] [CrossRef] [PubMed]
- Tappenbeck, K.; Hoppe, S.; Hopster, K.; Kietzmann, M.; Feige, K.; Huber, K. Lidocaine and structure-related mexiletine induce similar contractility-enhancing effects in ischaemia-reperfusion injured equine intestinal smooth muscle in vitro. Vet. J. 2013, 196, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Grages, A.M.; Verhaar, N.; Pfarrer, C.; Breves, G.; Burmester, M.; Neudeck, S.; Kästner, S. Low Flow versus No Flow: Ischaemia Reperfusion Injury Following Different Experimental Models in the Equine Small Intestine. Animals 2022, 12, 2158. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verhaar, N.; Hoppe, S.; Grages, A.M.; Hansen, K.; Neudeck, S.; Kästner, S.; Mazzuoli-Weber, G. Dexmedetomidine Has Differential Effects on the Contractility of Equine Jejunal Smooth Muscle Layers In Vitro. Animals 2023, 13, 1021. https://doi.org/10.3390/ani13061021
Verhaar N, Hoppe S, Grages AM, Hansen K, Neudeck S, Kästner S, Mazzuoli-Weber G. Dexmedetomidine Has Differential Effects on the Contractility of Equine Jejunal Smooth Muscle Layers In Vitro. Animals. 2023; 13(6):1021. https://doi.org/10.3390/ani13061021
Chicago/Turabian StyleVerhaar, Nicole, Susanne Hoppe, Anna Marei Grages, Kathrin Hansen, Stephan Neudeck, Sabine Kästner, and Gemma Mazzuoli-Weber. 2023. "Dexmedetomidine Has Differential Effects on the Contractility of Equine Jejunal Smooth Muscle Layers In Vitro" Animals 13, no. 6: 1021. https://doi.org/10.3390/ani13061021