
Towards Eradication of PPR: Disease Status, Economic Cost and Perception of Veterinarians in Karnataka, India
 ,
,  , , ,
, , ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
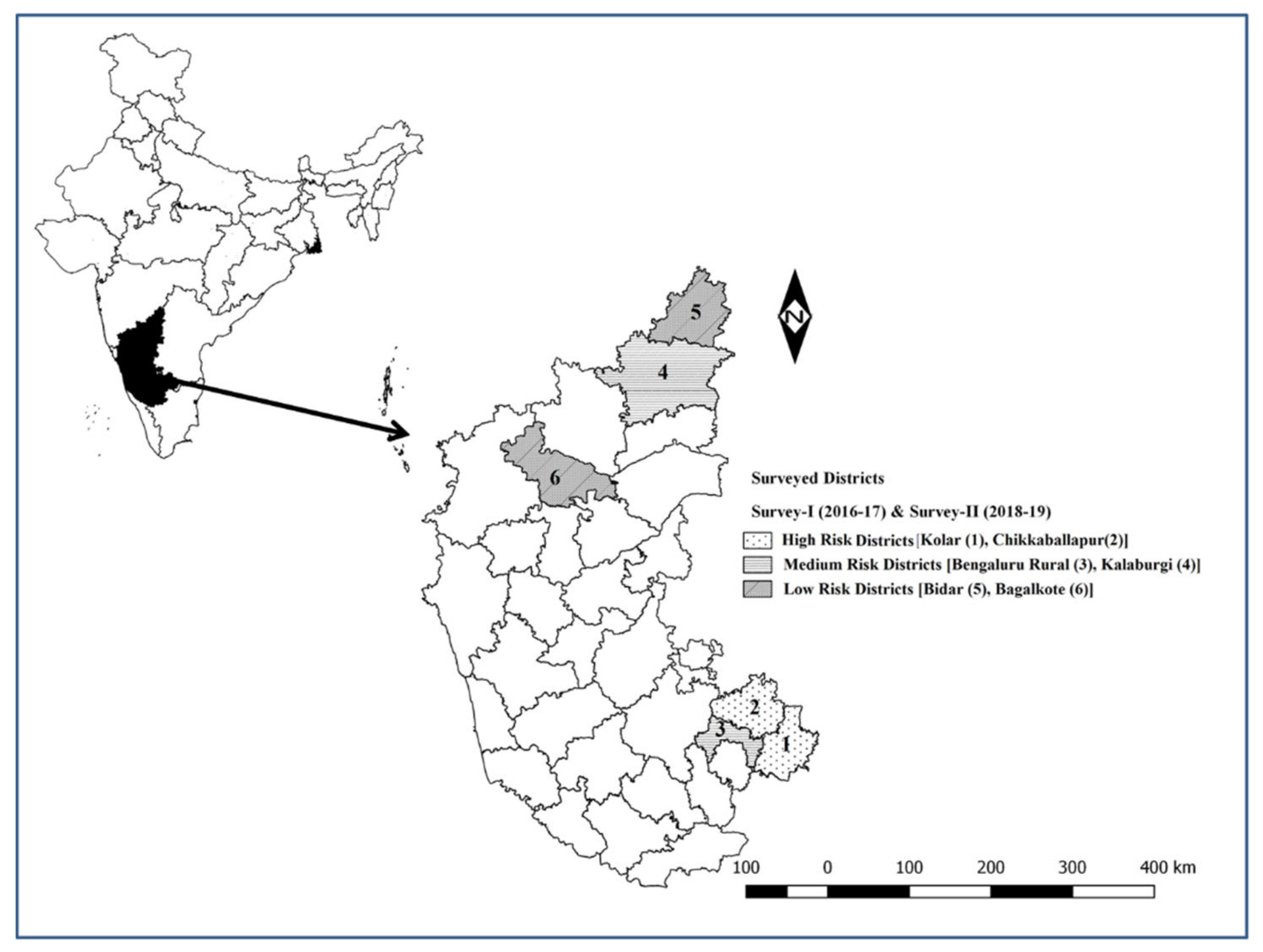
2.1. Study Area
2.2. Sampling Procedure
2.3. Sample Size
2.4. Data Collection and Identification of PPR-Affected Flocks
2.5. Estimation of the Flock-Level Economic Cost of PPR
2.6. Estimation of the Financial Viability of Vaccination
2.6.1. Vaccination Period
2.6.2. Vaccination Coverage and Plans
2.6.3. Population Projection
2.6.4. Incidence Interpolation
2.6.5. Benefit Stream
2.6.6. Vaccination Cost Stream
2.6.7. Financial Assessment of PPR Vaccination
2.7. Perspectives of Veterinary Officers on PPR-CP
2.8. Statistical Analysis
3. Results
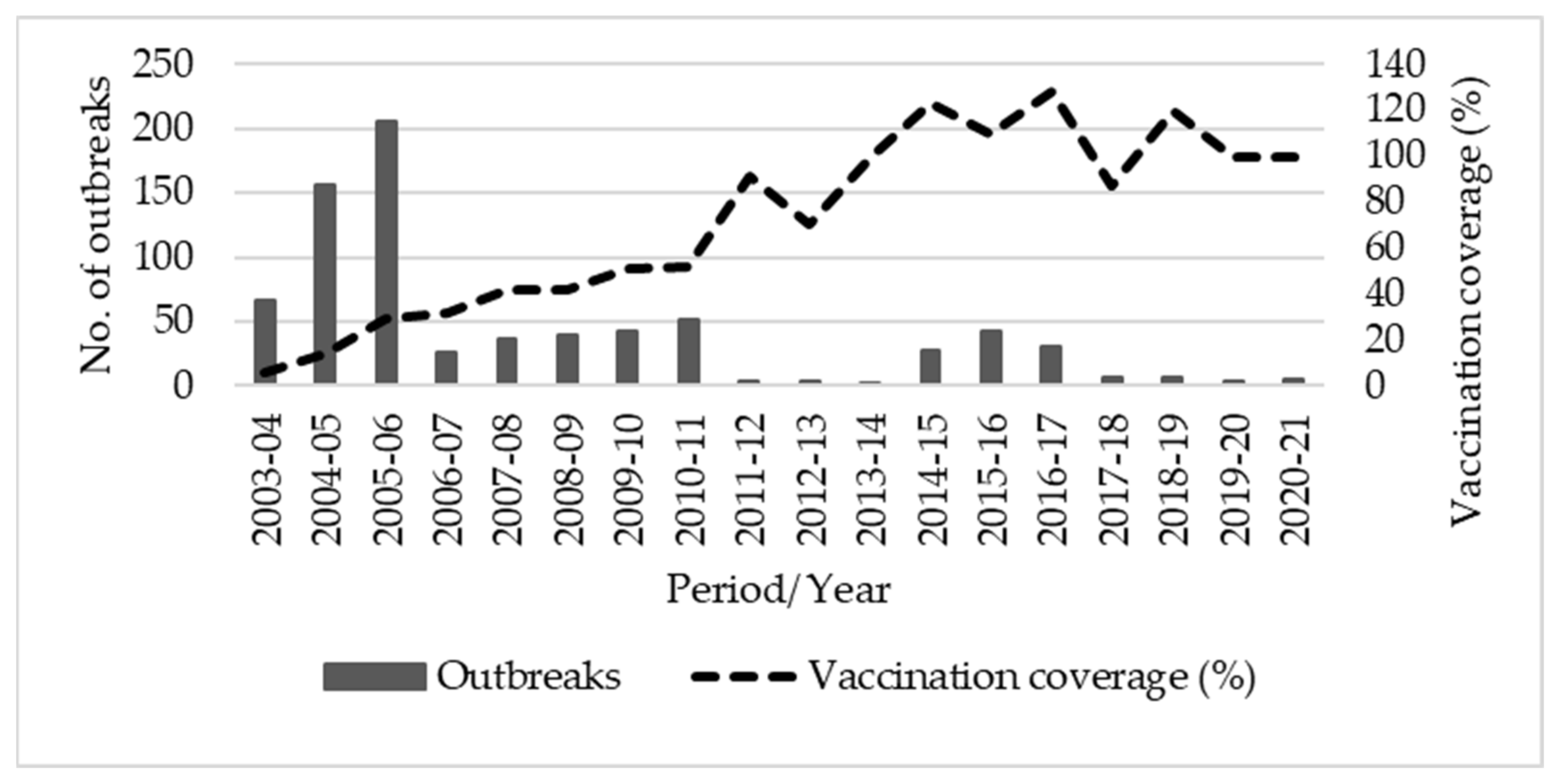
3.1. Reported Outbreaks and PPR Vaccination Coverage
3.2. Socio-Economic Characteristics of Sheep- and Goat-Rearing Farmers
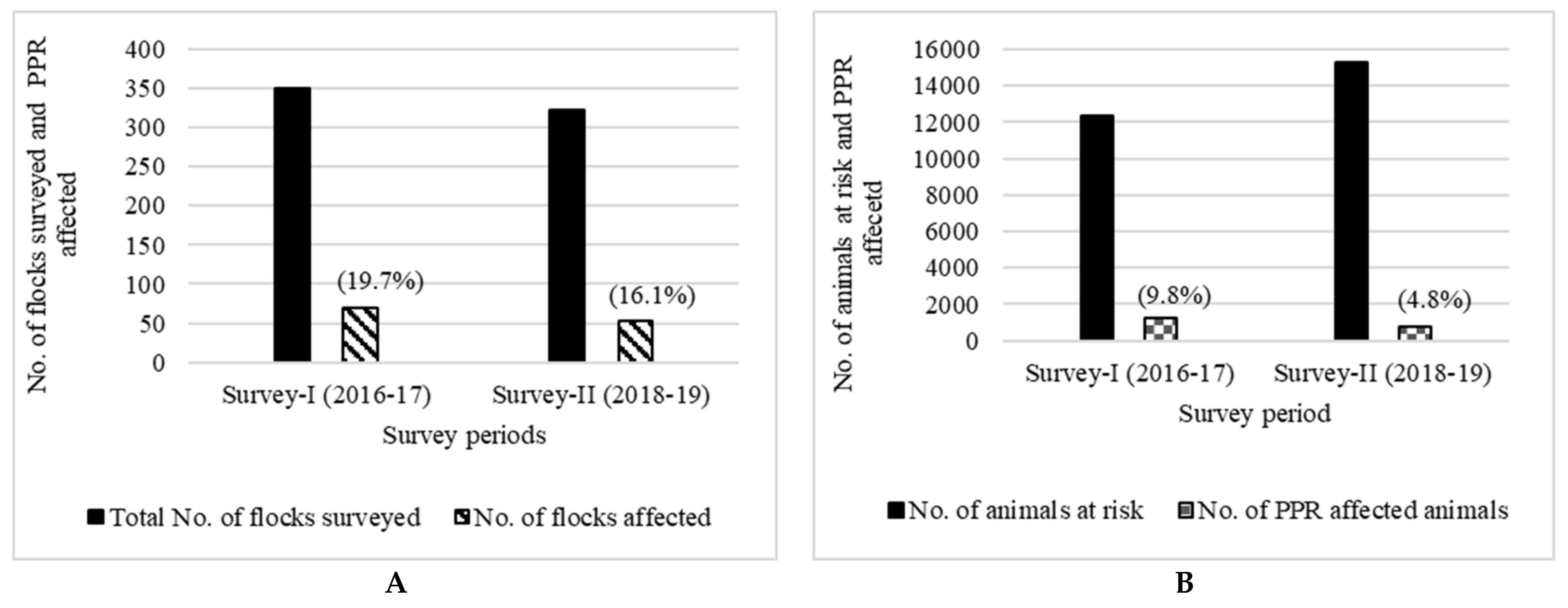
3.3. PPR Incidence in the Surveyed Flocks
3.4. Distribution of Incidence, Mortality and Case Fatality Rate (CFR)
3.5. Estimated Loss of PPR
3.6. Financial Viability of PPR Vaccination
3.7. Perspective of Field Veterinarians on PPR-CP
3.7.1. Planning and Rollout of PPR-CP
3.7.2. Performance of Functional Components of PPR-CP
3.7.3. Opinions of the Veterinarians on Improving the Implementation of PPR-CP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, R.P.; Saravanan, P.; Sreenivasa, B.P.; Singh, R.K.; Bandyopadhyay, S.K. Prevalence and distribution of Peste des petits ruminants virus infection in small ruminants in India. Rev. Sci. Tech. Off. Int. Epiz. 2004, 23, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Balamurugan, V.; Vinod Kumar, K.; Dheeraj, R.; Kurli, R.; Suresh, K.P.; Govindaraj, G.; Shome, B.R.; Roy, P. Temporal and Spatial Epidemiological Analysis of Peste des Petits Ruminants Outbreaks from the Past 25 Years in Sheep and Goats and Its Control in India. Viruses 2021, 13, 480. [Google Scholar] [CrossRef] [PubMed]
- Hegde, R.; Gomes, A.R.; Muniyellappa, H.K.; Byregowda, S.M.; Giridhar, P.; Renukaprasad, C. A short note on Peste des petits ruminants in Karnataka. Rev. Sci. Tech. Off. Int. Epiz. 2009, 28, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- OIE; FAO. Manual on Global Strategy for the Control and Eradication of Pesti des Petits Ruminants. 2015. Available online: http://www.fao.org/3/a-i4460e.pdf (accessed on 25 November 2022).
- Shaila, M.S.; Purushothaman, V.; Bhavasar, D.; Venugopal, K.; Venkatesan, R.A. Peste des petits ruminants in India. Vet. Rec. 1989, 125, 602. [Google Scholar]
- Balamurugan, V.; Hemadri, D.; Gajendragad, M.R.; Singh, R.K.; Rahman, H. Diagnosis and control of Peste des Petits Ruminants: A comprehensive review. Virus Dis. 2014, 25, 39–56. [Google Scholar] [CrossRef] [Green Version]
- Muthuchelvan, D.; Rajak, K.K.; Ramakrishnan, M.A.; Choudhary, D.; Bhadouriya, S.; Saravanan, P.; Pandey, A.B.; Singh, R.K. Peste-Des-Petits-Ruminants: An Indian Perspective. Adv. Anim. Vet. Sci. 2015, 3, 422–429. [Google Scholar] [CrossRef] [Green Version]
- Parida, S.; Muniraju, M.; Mahapatra, M.; Muthuchelvan, D.; Buczkowski, H.; Banyard, A.C. Peste des petitis ruminants. Vet. Microbiol. 2015, 181, 90–106. [Google Scholar] [CrossRef] [Green Version]
- Thombare, N.N.; Sinha, M.K. Economic implications of Peste des petits ruminants (PPR) disease in sheep and goats: A sample analysis of district Pune, Maharashtra, Agril. Econ. Res. Rev. 2009, 22, 319–322. [Google Scholar] [CrossRef]
- Govindaraj, G.; Balamurugan, V.; Rahman, H. Estimation of economic loss of PPR in sheep and goats in India: An annual incidence based analysis. Br. J. Virol. 2016, 3, 77–85. [Google Scholar] [CrossRef]
- Singh, B.; Bardhan, D.; Verma, M.R.; Shiv Prasad; Sinha, D.K. Estimation of economic losses due to Peste de Petits ruminants in small ruminants in India. Vet. World 2014, 7, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Bardhan, D.; Kumar, S.; Anandsekaran, G.; Chaudhury, J.K.; Meraj, M.; Singh, R.K.; Verma, M.R.; Kumar, D.; Kumar, P.T.N.; Ahmed, S.L.; et al. The economic impact of Peste des Petits Ruminants in India. Rev. Sci. Tech. Off. Int. Epiz. 2017, 36, 245–263. [Google Scholar] [CrossRef] [Green Version]
- Saravanan, P.; Balamurugan, V.; Sen, A.; Sreenivasa, B.P.; Singh, R.P.; Bandyopadhyay, S.K.; Singh, R.K. Long term immune response of goats to a vero cell adapted live attenuated homologous PPR vaccine. Indian Vet. J. 2010, 87, 1–3. [Google Scholar]
- Sreenivasa, B.P.; Dhar, P.; Singh, R.P.; Bandyopadhyay, S.K. Evaluation of an indigenously developed homologous live attenuated cell culture vaccine against Peste-des-petits-ruminants infection of small ruminants. In Proceedings of the XX Annual Conference of Indian Association of Veterinary Microbiologists, Immunologists and Specialists in Infectious Diseases (IAVMI), Pantnagar, Uttaranchal, India, 14–16 October 2000; p. 84. [Google Scholar]
- Balamurugan, V.; Govindaraj, G.; Rahman, H. Planning, implementation of Peste des Petits Ruminants Control Programme and strategies adopted for disease control in India. Br. J. Virol. 2016, 3, 53–62. [Google Scholar] [CrossRef]
- Govindaraj, G.; Goutam, R.; Mohanty, B.S.; Balamurugan, V.; Pandey, A.K.; Sharma, V.; Patel, A.; Mehra, M.; Pandey, S.K.; Parimal, R. Evaluation of effectiveness of Mass Vaccination Campaign against Peste des petits ruminants in Chhattisgarh state, India. Transbound Emerg. Dis. 2019, 66, 1349–1359. [Google Scholar] [CrossRef]
- Cochran, W.G. Sampling Techniques, 3rd ed.; John Wiley and Sons Inc.: New York, NY, USA, 1977; p. 225. [Google Scholar]
- Balamurugan, V.; Govindaraj, G.; SowjanyaKumari, S.; Nagalingam, M.; Tapase, J.; Manjunathareddy, G.B.; Rahman, H. Scorecard method for assessing the severity of Peste des Petits Ruminants in sheep and goats. Virus Dis. 2019, 30, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Limon, G.; Gamawa, A.A.; Ahmed, A.I.; Lyons, N.A.; Beard, P.M. Epidemiological Characteristics and Economic Impact of Lumpy Skin Disease, Sheep pox and Goat Pox Among Subsistence Farmers in Northeast Nigeria. Vet. Sci. 2020, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Data.Govt. Available online: https://data.gov.in/resource/all-india-consumer-price-index-ruralurban-upto-december-2018 (accessed on 12 October 2019).
- Awase, M.; Gangwar, L.S.; Patil, A.K.; Goyal, G.; Omprakash. Assessment of economic losses due to Peste des Petits Ruminants (PPR) disease in goats in Indore Division of Madhya Pradesh. Livest. Res. Int. 2013, 1, 61–63. [Google Scholar]
- Jones, B.A.; Rich, K.M.; Mariner, J.C.; Anderson, J.; Jeggo, M.; Thevasagayam, S.; Cai, Y.; Peters, A.R.; Roeder, P. The Economic Impact of Eradicating Peste des Petits Ruminants: A Benefit-Cost Analysis. PLoS ONE 2016, 11, e0149982. [Google Scholar] [CrossRef] [Green Version]
- Gittinger, J.P. Economic Analysis of Agricultural Projects; Unnumbered series; no. UNN 76; World Bank: Washington, DC, USA, 1985. [Google Scholar]
- Bardhan, D.; Singh, R.P.; Sanjay, K.; Anandasekaran, G.; Meraj, M. Impact of vaccine against Peste-des-Petits Ruminants (PPR) in India: An analysis using economic surplus model. Indian J. Anim. Sci. 2017, 87, 1176–1184. [Google Scholar]
- Stem, C. An economic analysis of the prevention of peste des petits ruminants in Nigerien goats. Prev. Vet. Med. 1993, 16, 141–150. [Google Scholar] [CrossRef]
- Singh, R.K.; Balamurugan, V.; Bhanuprakash, V.; Sen, A.; Saranavan, P.; Yadav, M.P. Possible control and eradication of peste des petits ruminants from India: Technical aspects. Vet. Ital. 2009, 45, 449–462. [Google Scholar] [PubMed]
- Alimi, Y.A.; Adamu, A.M.; Akinbobola, J.S.; Wunti, M.Z.; Mohammed, K. Perspective of animal health workers in Nigeria to global eradication of Pest des Petits Ruminants (PPR). Skoto J. Vet. Sci. 2018, 16, 72–75. [Google Scholar] [CrossRef]
- Channappagouda, B.; Sasidhar, P.V.K. Assessment of Veterinary Health Care Infrastructure Availability in Karnataka. Indian Res. J. Ext. Edu. 2017, 46–49. [Google Scholar]
- Modisane, B.M. Field Services: Eradication and control of animal diseases. Onderstepoort J. Vet. Res. 2009, 76, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Rathod, P.; Chander, M.; Bangar, Y. Livestock vaccination in India: An analysis of theory and practice among multiple stakeholders. Rev. Sci. Tech. Off. Int. Epiz. 2016, 35, 729–739. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Particulars | Unit | Survey I (2016–2017) | Survey II (2018–2019) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Districts | Pooled | Districts | Pooled | ||||||
| Kolar | Bangalore Rural | Bagalkote | Chikkaballapur | Kalaburagi | Bidar | ||||
| No. of farms/flocks surveyed | No. | 200 | 90 | 60 | 350 | 205 | 44 | 74 | 323 |
| Age of the farmers (Average) | Years | 50 | 51 | 44 | 49 | 48 | 45 | 43 | 46 |
| Family size (Median) | No. | 6 | 5 | 8 | 6 | 5 | 6 | 5 | 5 |
| Education | |||||||||
| Illiterate | No. | 101 (51.0) | 29 (32.2) | 39 (65.0) | 205 (58.6) | 141 (38.1) | 37 (84.1) | 60 (81.1) | 238 (73.7) |
| Primary | No. | 40 (19.8) | 9 (10.0) | 7 (11.7) | 39 (11.1) | 22 (29.3) | 4 (9.1) | 5 (6.8) | 31 (9.6) |
| High school | No. | 40 (19.8) | 37 (41.1) | 12 (20.0) | 80 (22.9) | 32 (32.7) | 2 (4.6) | 5 (6.8) | 39 (12.1) |
| College and above | No. | 19 (9.4) | 15 (16.7) | 2 (3.3) | 26 (7.4) | 10 (0) | 1 (2.3) | 4 (5.4) | 15 (4.6) |
| Land holdings | |||||||||
| Landless | No. | 51 (25.5) | 14 (15.5) | 18 (30.0) | 81 (23.1) | 32 (15.6) | 27 (61.4) | 45 (60.8) | 104 (32.2) |
| Small (< 5 Acre) | No. | 140 (70.0) | 68 (75.6) | 21 (35.0) | 229 (65.4) | 124 (60.5) | 13 (29.6) | 24 (32.4) | 161 (49.9) |
| Medium (5 to 10 Acre) | No. | 8 (4.0) | 6 (6.7) | 15 (25.0) | 30 (8.6) | 41 (20) | 3 (6.8) | 4 (5.4) | 48 (14.9) |
| Large (> 10 Acre) | No. | 1 (0.5) | 2 (2.2) | 6 (10.0) | 10 (2.9) | 8 (3.9) | 1 (2.3) | 1 (1.4) | 10 (3.1) |
| Income levels (USD) | |||||||||
| < 715 | No. | 78 (39.0) | 34 (37.8) | 10 (16.7) | 122 (34.9) | 51 (24.9) | 0 (0) | 17 (22.9) | 68 (21.1) |
| 715–1429 | No. | 73 (36.5) | 36 (40.0) | 34 (56.7) | 141 (40.3) | 135 (65.9) | 9 (20.5) | 26 (35.1) | 170 (52.6) |
| 1429–2858 | No. | 33 (16.5) | 15 (16.7) | 16 (26.7) | 64 (18.3) | 18 (8.8) | 15 (34.1) | 15 (20.3) | 48 (14.9) |
| > 2958 | No. | 18 (9.0) | 5 (5.6) | 0 (0.0) | 23 (6.6) | 1 (0.5) | 20 (45.5) | 16 (21.6) | 37 (11.5) |
| Total No. of sheep and goats in surveyed farms/flocks | No. | 4070 | 1970 | 6297 | 12,337 | 7765 | 2649 | 4897 | 15,311 |
| Average No. of sheep and goats per farm/flock | No. | 27 | 22 | 108 | 40 | 38 | 60 | 66 | 55 |
| Total No. of sheep and goats sold per year | No. | 1706 | 599 | 1843 | 4148 | 1825 | 1033 | 1371 | 4229 |
| Average No. of sheep and goats sold per year per farm/flock | No. | 9 | 7 | 31 | 12 | 9 | 23 | 19 | 17 |
| Groups | Category | No. of Surveyed Animals/Animals at Risk | No. of Affected Animals/ Incidence (Morbidity) | No. of Death Cases (Mortality) | CFR (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2016–2017 | 2018–2019 | 2016–2017 | 2018–2019 | z-Value |z| | 2016–2017 | 2018–2019 | z-Value |z| | 2016–2017 | 2018–2019 | ||
| Animal/species Type | Sheep | 10,006 | 9794 | 1036 (10.4) | 279 (2.8) | 21.20 *** | 455 (4.5) | 207 (2.1) | 9.52 *** | 43.9 | 74.2 |
| Goats | 2331 | 5517 | 169 (7.3) | 460 (8.3) | 1.62 NS | 81 (3.5) | 388 (7) | 6.07 *** | 47.9 | 84.3 | |
| Total | 12,337 | 15,311 | 1205(9.8) | 739 (4.8) | 15.97 *** | 536 (4.3) | 595 (3.9) | 1.91 * | 44.5 | 80.5 | |
| Sheep | |||||||||||
| Age-wise | <6 months | 2112 | 2812 | 336 (15.9) | 137 (4.9) | 13.01 *** | 204 (9.7) | 113 (4) | 7.98 *** | 60.7 | 82.5 |
| 6–12 months | 947 | 3426 | 108 (11.4) | 102 (3) | 10.73 *** | 30 (3.2) | 69 (2) | 2.11 * | 27.8 | 67.6 | |
| >1 year | 6947 | 3556 | 592 (8.5) | 40 (1.1) | 15.08 *** | 221 (3.2) | 25 (0.7) | 7.94 *** | 37.3 | 62.5 | |
| Sex-wise | Male | 2029 | 3939 | 328 (16.2) | 134 (3.4) | 17.47 *** | 153 (7.5) | 99 (2.5) | 9.14 *** | 46.6 | 73.9 |
| Female | 7977 | 5855 | 708 (8.9) | 145 (2.5) | 15.45 *** | 302 (3.8) | 108 (1.8) | 6.65 *** | 42.7 | 74.5 | |
| Goats | |||||||||||
| Age-wise | <6 months | 633 | 1476 | 43 (6.8) | 234 (15.9) | 5.65 *** | 28 (4.4) | 217 (14.7) | 6.75 *** | 65.1 | 92.7 |
| 6–12 months | 267 | 1830 | 9 (3.4) | 139 (7.6) | 2.52 * | 5 (1.9) | 104 (5.7) | 2.62 *** | 55.6 | 74.8 | |
| >1 year | 1431 | 2211 | 117 (8.2) | 87 (3.9) | 5.43 *** | 48 (3.4) | 67 (3) | 0.54 NS | 41 | 77 | |
| Sex-wise | Male | 631 | 2182 | 61 (9.7) | 227 (10.4) | 0.53 NS | 30 (4.8) | 192 (8.8) | 3.32 *** | 49.2 | 84.6 |
| Female | 1700 | 3335 | 108 (6.4) | 233 (7) | 0.45 NS | 51 (3) | 196 (5.9) | 4.47 *** | 47.2 | 84.1 | |
| Sheep + Goats | |||||||||||
| Age-wise | < 6 months | 2745 | 4288 | 379 (13.8) | 371 (8.7) | 6.83 *** | 232 (8.5) | 330 (7.7) | 1.14 NS | 61.2 | 88.9 |
| 6–12 months | 1214 | 5256 | 117 (9.6) | 241 (4.6) | 6.94 *** | 35 (2.9) | 173 (3.3) | 0.73 NS | 29.9 | 71.8 | |
| > 1 year | 8378 | 5767 | 709 (8.5) | 127 (2.2) | 15.51 *** | 269 (3.2) | 92 (1.6) | 5.99 *** | 37.9 | 72.4 | |
| Sex-wise | Male | 2660 | 6121 | 389 (14.6) | 361 (5.9) | 13.44 *** | 183 (6.9) | 291 (4.8) | 4.05 *** | 47 | 80.6 |
| Female | 9677 | 9190 | 816 (8.4) | 378 (4.1) | 13.26 *** | 353 (3.6) | 304 (3.3) | 1.27 NS | 43.3 | 80.4 | |
| Parameters | Sheep | Goats | Pooled (Sheep + Goats) | |||
|---|---|---|---|---|---|---|
| 2016–2017 | 2018–2019 | 2016–2017 | 2018–2019 | 2016–2017 | 2018–2019 | |
| Loss due to reduction in body weight (USD) | 4.2 (0.4, 1.7–12.5) | 4.3 (0.5, 2.9–7.3) | 3.9 (0.4, 3.9–7.6) | 4.0 (0.4, 2.0–7.4) | 4 (0.4, 1.7–12.5) | 4.2 (0.4, 2.0–7.4) |
| Mortality loss (USD) | 49.1 (2.4, 25.8–91.9) | 56.4 (2.6, 34.3–128.6) | 51.2 (2.5, 34.7–99.6) | 56.5 (2.5, 42.9–120.0) | 50.2 (2.5, 30.1–99.6) | 56.5 (2.6, 34.3–128.6) |
| Distress sale loss (USD) | 43.3 (1.9, 26.1–76.5) | 0 (0, 0–0) | 38.3 (1.5, 15.3–68.9) | 84.9 (3.7, 35.7–101.8) | 40.8 (1.7, 19.6–76.5) | 84.9 (13.7, 35.7–101.8) |
| Treatment cost (USD) | 1.6 (0, 0.3–9.2) | 2.6 (0.07, 0.9–7.3) | 1.6 (0, 0.3–9.2) | 2.6 (0.07, 0.9–7.3) | 1.6 (0, 0.3–9.2) | 2.6 (0.07, 0.9–7.3) |
| Opportunity cost of labour (USD) | 1.8 (0.1, 0.2–4) | 2.4 (0.05, 0.4–8.3) | 1.8 (0.1, 0.2–4) | 2.4 (0.05, 0.4–8.3) | 1.8 (0.1, 0.2–4) | 2.4 (0.05, 0.4–8.3) |
| Statements | Disagree | Neutral/Undecided | Agree |
|---|---|---|---|
| The PPR vaccination programme has been well planned in your jurisdiction. | 4 (6.5, 0.3–12.6) | 0 (0, 0–0) | 58 (93.5, 87.4–99.7) |
| Proper coordination exists between various functionaries. | 1 (1.6, −1.5–4.7) | 12 (19.4, 9.5–29.2) | 49 (79, 68.9–89.2) |
| Funding delays hindered the implementation of PPR-CP. | 20 (32.3, 20.6–43.9) | 26 (41.9, 29.7–54.2) | 16 (25.8, 14.9–36.7) |
| Weak support from local authority such as the Panchayat was experienced. | 20 (32.3, 20.6–43.9) | 16 (25.8, 14.9–36.7) | 26 (41.9, 29.7–54.2) |
| The vaccination programme was acceptable for farmers | 1 (1.6, −1.5–4.7) | 10 (16.1, 7–25.3) | 51 (82.3, 72.7–91.8) |
| Creating awareness about PPR and vaccination for farmers and other functionaries through mass media is effective in its implementation. | 1 (1.6, −1.5–4.7) | 4 (6.5, 0.3–12.6) | 57 (91.9, 85.2–98.7) |
| Statements | Disagree | Neutral/Undecided | Agree |
|---|---|---|---|
| Timely availability of vaccines | 4 (6.5, 0.3–12.6) | 7 (11.3, 3.4–19.2) | 51 (82.3, 72.7–91.8) |
| Supply of sufficient quantity of vaccines and quality of vaccination materials (syringes, gloves, etc.) | 6 (9.7, 2.3–17) | 5 (8.1, 1.3–14.8) | 51 (82.3, 72.7–91.8) |
| Able to cover the targeted population within the stipulated time | 9 (14.5, 5.7–23.3) | 8 (12.9, 4.6–21.2) | 45 (72.6, 61.5–83.7) |
| Appropriate training was imparted to the vaccination team to vaccinate animals at the farmer’s doorstep | 10 (16.1, 7–25.3) | 9 (14.5, 5.7–23.3) | 43 (69.4, 57.9–80.8) |
| Storage and cold-chain facilities were good | 6 (9.7, 2.3–17) | 3 (4.8, −0.5–10.2) | 53 (85.5, 76.7–94.3) |
| Veterinarians were able to manage the reported outbreaks in time | 1 (1.6, −1.5–4.7) | 8 (12.9, 4.6–21.2) | 53 (85.5, 76.7–94.3) |
| Statements | Yes | No |
|---|---|---|
| Training should be supplied to veterinarians and para-veterinary workers on the vaccine’s efficacy and effectiveness | 52(83.9, 74.7–93.0) | 10(16.1, 6.9–25.3) |
| Provision of funds for mobility, contingencies, etc., is key for success | 48(77.4, 67.0–87.8) | 14(22.6, 12.2–32.9) |
| Involving various local authorities in vaccination will strengthen the programme | 45(72.6, 61.5–83.7) | 17(27.4, 16.3–38.5) |
| Organising farmer-awareness meetings is one way to make the programme better | 57(91.9, 85.2–98.7) | 5(8.1, 1.3–14.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Govindaraj, G.N.; Balamurugan, V.; Reddy, G.B.M.; Yogisharadhya, R.; Reddy, T.S.; Naveenkumar, G.S.; Kumar, K.V.; Chaithra, H.R.; Bi, A.Z.; Parida, S.; et al. Towards Eradication of PPR: Disease Status, Economic Cost and Perception of Veterinarians in Karnataka, India. Animals 2023, 13, 778. https://doi.org/10.3390/ani13050778
Govindaraj GN, Balamurugan V, Reddy GBM, Yogisharadhya R, Reddy TS, Naveenkumar GS, Kumar KV, Chaithra HR, Bi AZ, Parida S, et al. Towards Eradication of PPR: Disease Status, Economic Cost and Perception of Veterinarians in Karnataka, India. Animals. 2023; 13(5):778. https://doi.org/10.3390/ani13050778
Chicago/Turabian StyleGovindaraj, Gurrappa Naidu, Vinayagamurthy Balamurugan, Gundalahalli Bayyappa Manjunatha Reddy, Revanaiah Yogisharadhya, Timmareddy Sreenivasa Reddy, Gajalavarahalli Subbanna Naveenkumar, Kirubakaran Vinod Kumar, Hosahalli Rajanna Chaithra, Afrin Zainab Bi, Satya Parida, and et al. 2023. "Towards Eradication of PPR: Disease Status, Economic Cost and Perception of Veterinarians in Karnataka, India" Animals 13, no. 5: 778. https://doi.org/10.3390/ani13050778