
Equine Melanocytic Tumors: A Narrative Review

Abstract
:Simple Summary
Abstract
1. Introduction
2. Etiology
3. Classification
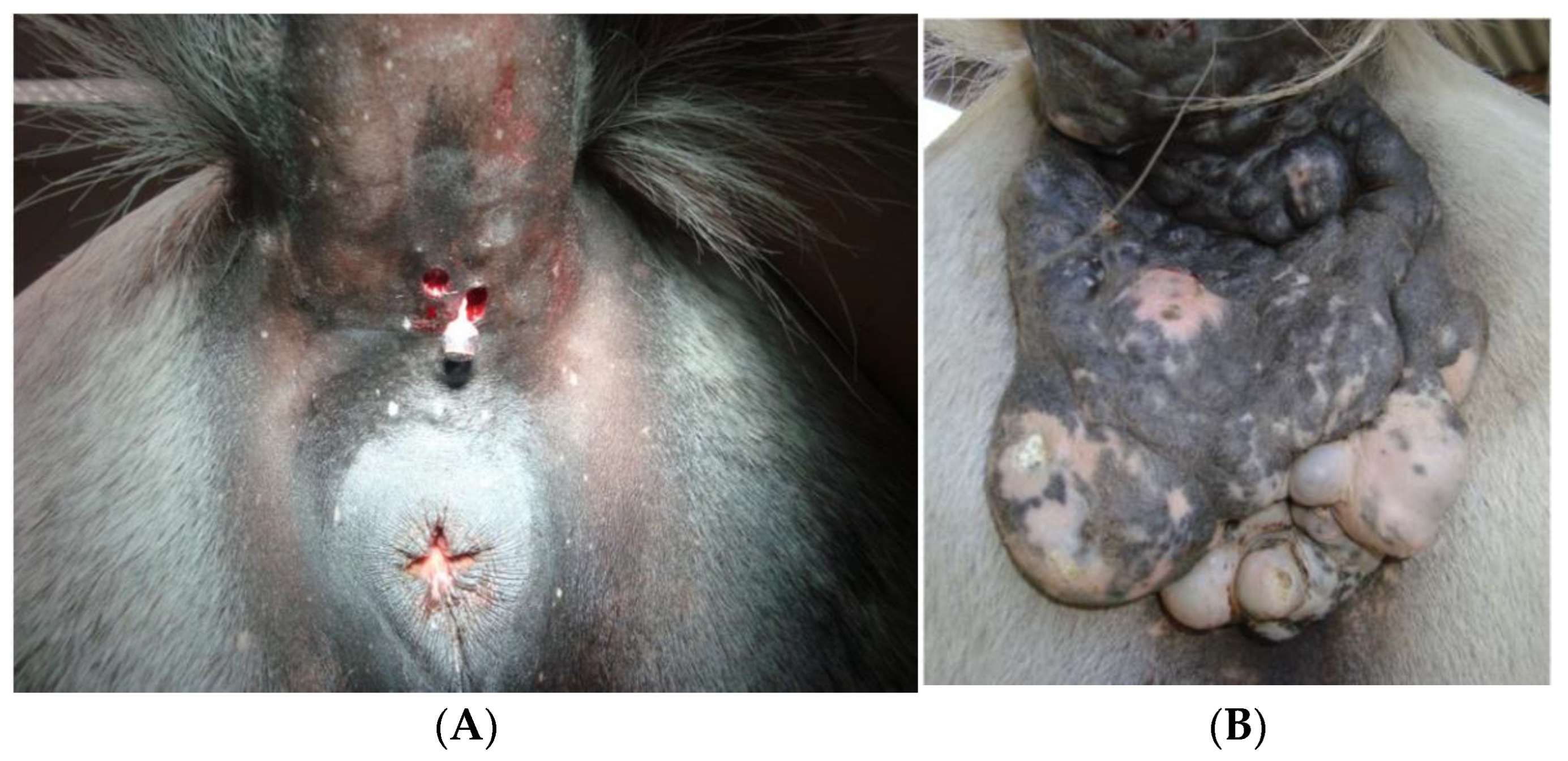
4. Clinical Features
5. Diagnosis
5.1. Clinical Diagnostic Procedures
5.2. Laboratorial Diagnostic Procedures
5.2.1. Hematology and Biochemistry
5.2.2. Histopathology
Melanocytic Naevus
Intradermal Common Melanocytic Naevus
Cellular Blue Naevus
Combined Cellular Blue Naevus
Dermal Melanoma and Dermal Melanomatosis
Anaplastic Malignant Melanoma
5.2.3. Immunohistochemistry
6. Differential Diagnosis
7. Management
7.1. Surgical Treatment
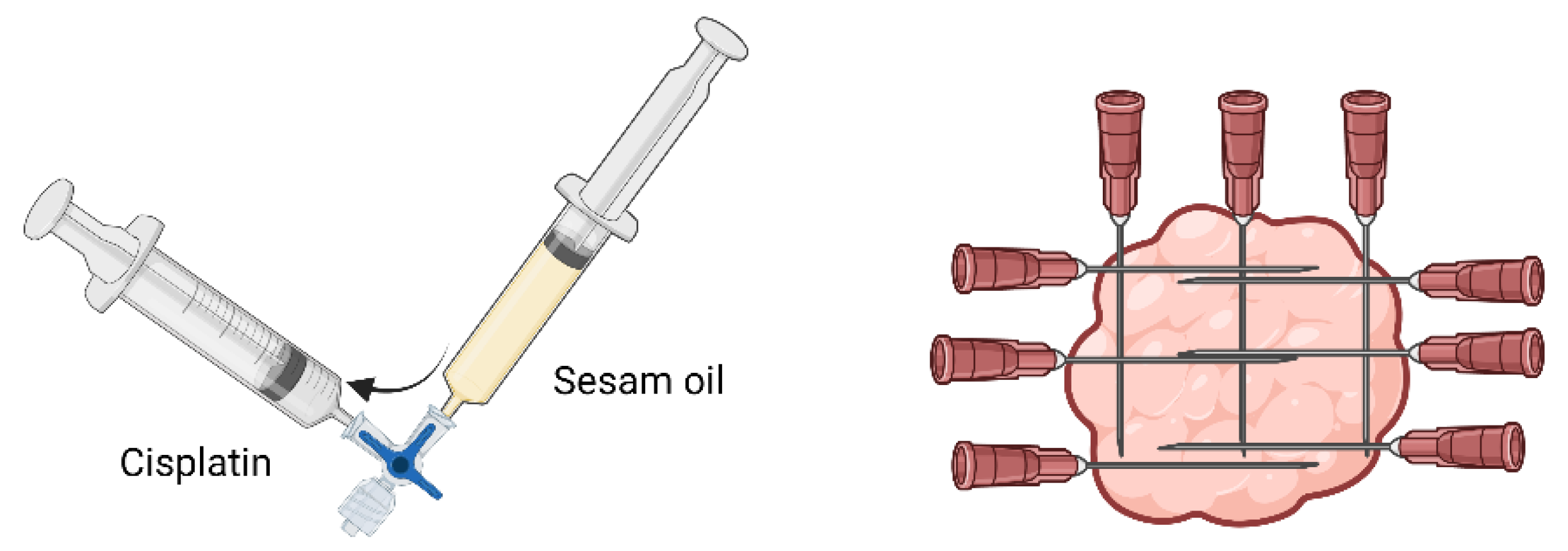
7.2. Chemotherapy
7.3. Adjunctive Therapies
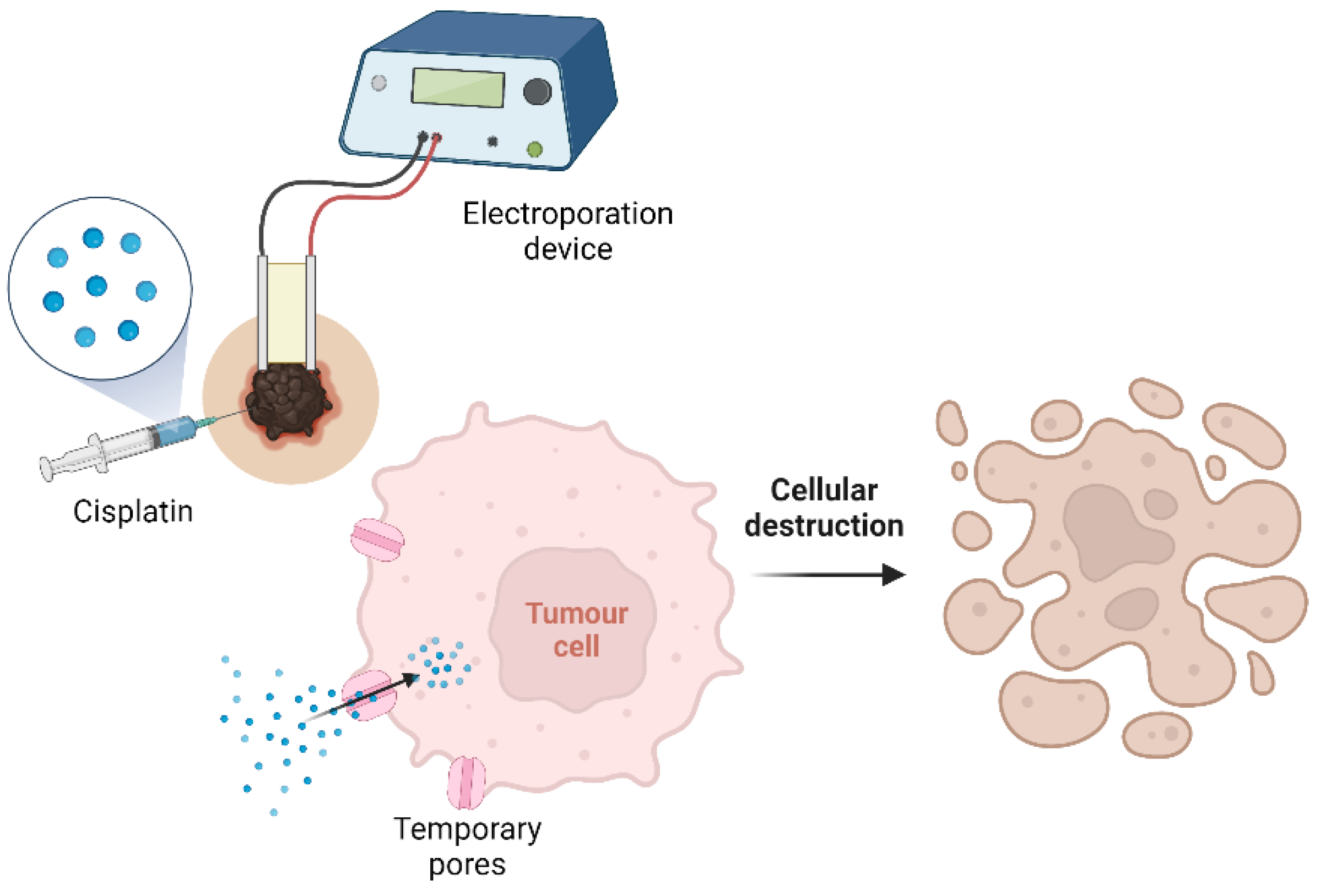
7.4. Calcium Electroporation
7.5. Irreversible Electroporation
7.6. Oral Therapies
7.7. Topical Therapy
7.8. Radiotherapy
7.9. Immunotherapy
Bacterial Products Injection
7.10. Proteasome Inhibition
8. Immunohistochemistry: A Way to New Therapies
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, S.H.; Goldschmidt, M.H.; Mcmanus, P.M. A Comparative Review of Melanocytic Neoplasms. Vet. Pathol. 2002, 39, 651–678. [Google Scholar] [CrossRef]
- Knottenbelt, D.C.; Patterson-Kane, J.C.; Snalune, K.L. Melanocytic Neoplasms. In Clinical Equine Oncology; Elsevier: Amsterdam, The Netherlands, 2015; pp. 237–246. ISBN 978-0-7020-4266-9. [Google Scholar]
- Valentine, B.A. Equine Melanocytic Tumors: A Retrospective Study of 53 Horses (1988 to 1991). J. Vet. Intern. Med. 1995, 95, 291–297. [Google Scholar] [CrossRef]
- Rodríguez, F.; Forga, J.; Herráez, P.; Andrada, M.; Fernández, A. Metastatic Melanoma Causing Spinal Cord Compression in a Horse. Vet. Rec. 1998, 142, 248–249. [Google Scholar] [CrossRef]
- Johnson, P. Dermatologic Tumours. Vet. Clin. N. Am. Equine Pract. 1998, 14, 625–659. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.C.; Lembcke, L.M. Equine Melanocytic Tumors. Vet. Clin. N. Am. Equine Pract. 2013, 29, 673–687. [Google Scholar] [CrossRef]
- MacKay, R.J. Treatment Options for Melanoma of Gray Horses. Vet. Clin. N. Am. Equine Pract. 2019, 35, 311–325. [Google Scholar] [CrossRef]
- Agar, N.; Young, A.R. Melanogenesis: A Photoprotective Response to DNA Damage? Mutat. Res. Fundam. Mol. Mech. Mutagen. 2005, 571, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Curik, I.; Druml, T.; Seltenhammer, M.; Sundström, E.; Pielberg, G.R.; Andersson, L.; Sölkner, J. Complex Inheritance of Melanoma and Pigmentation of Coat and Skin in Grey Horses. PLoS Genet. 2013, 9, e1003248. [Google Scholar] [CrossRef] [Green Version]
- Seltenhammer, M.H.; Simhofer, H.; Scherzer, S.; Zechner, P.; Curik, I.; Sölkner, J.; Brandt, S.M.; Jansen, B.; Pehamberger, H.; Eisenmenger, E. Equine Melanoma in a Population of 296 Grey Lipizzaner Horses. Equine Vet. J. 2003, 35, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Guerrero, M.J.; Solé, M.; Azor, P.J.; Sölkner, J.; Valera, M. Genetic and Environmental Risk Factors for Vitiligo and Melanoma in Pura Raza Español Horses. Equine Vet. J. 2019, 51, 606–611. [Google Scholar] [CrossRef]
- Rieder, S.; Stricker, C.; Joerg, H.; Dummer, R.; Stranzinger, G. A Comparative Genetic Approach for the Investigation of Ageing Grey Horse Melanoma. J. Anim. Breed. Genet. 2000, 117, 73–82. [Google Scholar] [CrossRef]
- Sundström, E.; Komisarczuk, A.Z.; Jiang, L.; Golovko, A.; Navratilova, P.; Rinkwitz, S.; Becker, T.S.; Andersson, L. Identification of a Melanocyte-Specific, Microphthalmia-Associated Transcription Factor-Dependent Regulatory Element in the Intronic Duplication Causing Hair Greying and Melanoma in Horses. Pigment Cell Melanoma Res. 2012, 25, 28–36. [Google Scholar] [CrossRef]
- Rosengren Pielberg, G.; Golovko, A.; Sundström, E.; Curik, I.; Lennartsson, J.; Seltenhammer, M.H.; Druml, T.; Binns, M.; Fitzsimmons, C.; Lindgren, G.; et al. A Cis-Acting Regulatory Mutation Causes Premature Hair Graying and Susceptibility to Melanoma in the Horse. Nat. Genet. 2008, 40, 1004–1009. [Google Scholar] [CrossRef]
- Lindgren, G.; Naboulsi, R.; Frey, R.; Solé, M. Genetics of Skin Disease in Horses. Vet. Clin. N. Am. Equine Pract. 2020, 36, 323–339. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, R.B.C.; Rendahl, A.K.; Anderson, S.M.; Mickelson, J.R.; Sigler, D.; Buchanan, B.R.; Coleman, R.J.; Mccue, M.E. Coat Color Genotypes and Risk and Severity of Melanoma in Gray Quarter Horses. J. Vet. Intern. Med. 2013, 27, 1201–1208. [Google Scholar] [CrossRef]
- Nowacka-Woszuk, J.; Mackowski, M.; Stefaniuk-Szmukier, M.; Cieslak, J. The Equine Graying with Age Mutation of the STX17 Gene: A Copy Number Study Using Droplet Digital PCR Reveals a New Pattern. Anim. Genet. 2021, 52, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Smalley, K.S.M. A pivotal role for ERK in the oncogenic behaviour of malignant melanoma? Int. J. Cancer 2003, 104, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Campagne, C.; Sundström, E.; Sousa, P.; Imran, S.; Seltenhammer, M.; Pielberg, G.; Olsson, M.J.; Egidy, G.; Andersson, L.; et al. Constitutive Activation of the ERK Pathway in Melanoma and Skin Melanocytes in Grey Horses. BMC Cancer 2014, 14, 857. [Google Scholar] [CrossRef] [Green Version]
- Druml, T.; Brem, G.; Horna, M.; Ricard, A.; Grilz-Seger, G. DPF3, A Putative Candidate Gene For Melanoma Etiopathogenesis in Gray Horses. J. Equine Vet. Sci. 2022, 108, 103797. [Google Scholar] [CrossRef]
- Wong, K.; van der Weyden, L.; Schott, C.R.; Foote, A.; Constantino-Casas, F.; Smith, S.; Dobson, J.M.; Murchison, E.P.; Wu, H.; Yeh, I.; et al. Cross-Species Genomic Landscape Comparison of Human Mucosal Melanoma with Canine Oral and Equine Melanoma. Nat. Commun. 2019, 10, 353. [Google Scholar] [CrossRef]
- Kanellis, V.G. The Potential Role of Sensors in Equine Melanoma Prevention. Equine Vet. Educ. 2020, 32, 631–632. [Google Scholar] [CrossRef]
- Knottenbelt, D.C.; Patterson-Kane, J.C.; Snalune, K.L. Pathological Methods in Equine Oncology. In Clinical Equine Oncology; Elsevier: Amsterdam, The Netherlands, 2015; pp. 108–117. ISBN 978-0-7020-4266-9. [Google Scholar]
- Moore, J.S.; Shaw, C.; Shaw, E.; Buechner-Maxwell, V.; Scarratt, W.K.; Crisman, M.; Furr, M.; Robertson, J. Melanoma in Horses: Current Perspectives. Equine Vet. Educ. 2013, 25, 144–151. [Google Scholar] [CrossRef]
- Macgillivray, K.C.; Sweeney, R.W.; del Piero, F. Metastatic Melanoma in Horses. J. Vet. Intern. Med. 2002, 16, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Patterson-Kane, J.C.; Sanchez, L.C.; Uhl, E.W.; Edens, L.M. Disseminated Metastatic Intramedullary Melanoma in an Aged Grey Horse. J. Comp. Pathol. 2001, 125, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Cavalleri, J.M.V.; Mählmann, K.; Steinig, P.; Feige, K. Aetiology, Clinical Presentation and Current Treatment Options of Equine Malignant Melanoma—A Review of the Literature. Pferdeheilkunde 2014, 30, 455–460. [Google Scholar] [CrossRef] [Green Version]
- Schöniger, S.; Summers, B.A. Equine Skin Tumours in 20 Horses Resembling Three Variants of Human Melanocytic Naevi. Vet. Dermatol. 2009, 20, 165–173. [Google Scholar] [CrossRef]
- Poore, L.A.; Rest, J.R.; Knottenbelt, D.C. The Clinical Presentation of a Mid-Tail Melanocytoma with Sudden Malignant Transformation in a Bay Irish Draught Gelding. Equine Vet. Educ. 2013, 25, 134–138. [Google Scholar] [CrossRef]
- Sullins, K.E. Melanocytic Tumours in Horses. Equine Vet. Educ. 2020, 32, 624–630. [Google Scholar] [CrossRef]
- Valentine, B.A.; Calderwood Mays, M.B.; Cheramie, H.S. Anaplastic Malignant Melanoma of the Tail in Non-Grey Horses. Equine Vet. Educ. 2014, 26, 156–158. [Google Scholar] [CrossRef]
- Knottenbelt, D.C.; Patterson-Kane, J.C.; Snalune, K.L. Tumours of the Skin. In Clinical Equine Oncology; Elsevier: Amsterdam, The Netherlands, 2015; pp. 544–584. ISBN 978-0-7020-4266-9. [Google Scholar]
- Albanese, V.; Newton, J.C.; Waguespack, R.W. Malignant Melanoma of the Third Eyelid in a Horse. Equine Vet. Educ. 2015, 27, e15–e19. [Google Scholar] [CrossRef]
- Caston, S.S.; Fales-Williams, A. Primary Malignant Melanoma in the Oesophagus of a Foal. Equine Vet. Educ. 2010, 22, 387–390. [Google Scholar] [CrossRef]
- Strauss, R.A.; Allbaugh, R.A.; Haynes, J.; Ben-Shlomo, G. Primary Corneal Malignant Melanoma in a Horse. Equine Vet. Educ. 2019, 31, 403–409. [Google Scholar] [CrossRef]
- Tyler, R.J.; Fox, R.I. Nasopharyngeal Malignant Amelanotic Melanoma in a Gelding Age 9 Years. Equine Vet. Educ. 2003, 15, 19–26. [Google Scholar] [CrossRef]
- Stefanik, E.; Górski, K.; Turek, B.; Drewnowska-Szczepakowska, O.; Kliczkowska-Klarowicz, K.; Stefanik, A. From Keratoma to Anaplastic Malignant Melanoma in a Horse’s Hoof. Animals 2022, 12, 3090. [Google Scholar] [CrossRef] [PubMed]
- Knottenbelt, D.C.; Patterson-Kane, J.C.; Snalune, K.L. Principles of Diagnosis. In Clinical Equine Oncology; Elsevier: Amsterdam, The Netherlands, 2015; pp. 85–107. ISBN 978-0-7020-4266-9. [Google Scholar]
- Valentine, B.A. The Spectrum of Equine Melanocytic Tumours. Equine Vet. Educ. 2003, 15, 24. [Google Scholar] [CrossRef]
- Burden, K. Melanomas and Their Effect on the Grey Horse. Young Sci. J. 2011, 4, 75. [Google Scholar] [CrossRef] [Green Version]
- Conrado, F.O.; Iapoce, N.; Batista-Linhares, M.; Lopez, S.; Matthews, M.H.; McKinney, C.A.; Rothacker, C. Circulating Melanin-Containing Cells and Neutrophils with Phagocytized Melanin Granules in a Horse with Disseminated Melanoma. Vet. Clin. Pathol. 2020, 49, 624–631. [Google Scholar] [CrossRef]
- Tesena, P.; Kingkaw, A.; Vongsangnak, W.; Pitikarn, S.; Phaonakrop, N.; Roytrakul, S.; Kovitvadhi, A. Preliminary Study: Proteomic Profiling Uncovers Potential Proteins for Biomonitoring Equine Melanocytic Neoplasm. Animals 2021, 11, 1913. [Google Scholar] [CrossRef]
- Pellerin, L.; Carrié, L.; Dufau, C.; Nieto, L.; Ségui, B.; Levade, T.; Riond, J.; Andrieu-Abadie, N. Lipid Metabolic Reprogramming: Role in Melanoma Progression and Therapeutic Perspectives. Cancers 2020, 12, 3147. [Google Scholar] [CrossRef]
- Ramos-Vara, J.A.; Kiupel, M.; Baszier, T.; Bliven, L.; Brodersen, B.; Chelack, B.; Czub, S.; del Piero, F.; Dial, S.; Ehrhart, E.J.; et al. Suggested Guidelines for Immunohistochemical Techniques in Veterinary Diagnostic Laboratories. J. Vet. Diagn. Investig. 2008, 20, 393–413. [Google Scholar] [CrossRef]
- Ramos-Vara, J.A. Technical Aspects of Immunohistochemistry. Vet. Pathol. 2005, 42, 405–426. [Google Scholar] [CrossRef]
- Ramos-Vara, J.A.; Frank, C.B.; DuSold, D.; Miller, M.A. Immunohistochemical Expression of Melanocytic Antigen PNL2, Melan A, S100, and PGP 9.5 in Equine Melanocytic Neoplasms. Vet. Pathol. 2014, 51, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seltenhammer, M.H.; Heere-Ress, E.; Brandt, S.; Druml, T.; Jansen, B.; Pehamberger, H.; Niebauer, G.W. Comparative Histopathology of Grey-Horse-Melanoma and Human Malignant Melanoma. Pigment Cell Res. 2004, 17, 674–681. [Google Scholar] [CrossRef]
- Erin, M.B.; Kimberly, M.N.; Deanna, M.W. Schaefer Neoplasia and Tumour Biology. In Pathologic Basis of Veterinary Disease; Zachary, J.F., Ed.; Elsevier: St. Louis, MO, USA, 2022; pp. 341–394. [Google Scholar]
- Goldschmidt, M.H.; Goldschmidt, K.H. Epithelial and Melanocytic Tumors of the Skin. In Tumors in Domestic Animals; Meuten, D.J., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2017. [Google Scholar]
- Ohsie, S.J.; Sarantopoulos, G.P.; Cochran, A.J.; Binder, S.W. Immunohistochemical Characteristics of Melanoma. J. Cutan. Pathol. 2008, 35, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Campagne, C.; Julé, S.; Bernex, F.; Estrada, M.; Aubin-Houzelstein, G.; Panthier, J.-J.; Egidy, G. RACK1, a Clue to the Diagnosis of Cutaneous Melanomas in Horses. BMC Vet. Res. 2012, 8, 95. [Google Scholar] [CrossRef] [Green Version]
- Lilyquist, J.; White, K.A.M.; Lee, R.J.; Philips, G.K.; Hughes, C.R.; Torres, S.M. Quantitative Analysis of Immunohistochemistry in Melanoma Tumors. Medicine 2017, 96, e6432. [Google Scholar] [CrossRef] [PubMed]
- Tamzali, Y.; Kemp-Symonds, J. Principles of Oncological Therapy. In Clinical Equine Oncology; Elsevier: Amsterdam, The Netherlands, 2015; pp. 118–197. ISBN 978-0-7020-4266-9. [Google Scholar]
- Va Metcalfe, L.; O’brien, P.J.; Papakonstantinou, S.; Cahalan, S.D.; Mcallister, H.; Duggan, V.E. Malignant Melanoma in a Grey Horse: Case Presentation and Review of Equine Melanoma Treatment Options. Ir. Vet. J. 2013, 66, 22. [Google Scholar] [CrossRef] [Green Version]
- Groom, L.M.; Sullins, K.E. Surgical Excision of Large Melanocytic Tumours in Grey Horses: 38 Cases (2001–2013). Equine Vet. Educ. 2018, 30, 438–443. [Google Scholar] [CrossRef]
- Deleon, M.; Iowa State University (Digital Repository). Cutaneous Melanoma: A Comparative Study Between Gray Horses, Canines, and Humans. 2021. Available online: https://dr.lib.iastate.edu/home (accessed on 11 July 2022).
- Palmer, S.E. Treatment of Common Cutaneous Tumors Using the Carbon Dioxide Laser. Clin. Tech. Equine Pract. 2002, 1, 43–50. [Google Scholar] [CrossRef]
- McCauley, C.T.; Hawkins, J.F.; Adams, S.B.; Fessler, J.F. Use of a Carbon Dioxide Laser for Surgical Management of Cutaneous Massesin Horses: 32 Cases (1993–2000). JAVMA 2002, 220, 1192–1197. [Google Scholar] [CrossRef]
- Hewes, C.A.; Kenneth, E. Use of Cisplatin-Containing Biodegradable Beads for Treatment of Cutaneous Neoplasia in Equidae: 59 Cases (2000–2004). JAVMA 2006, 229, 1617–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Théon, A.P.; Wilson, W.D.; Magdesian, K.G.; Pusterla, N.; Snyder, J.R.G.L.D. Long-Term Outcome Associated with Intratumoral Chemotherapy with Cisplatin for Cutaneous Tumors in Equidae: 573 Cases (1995–2004). JAVMA 2007, 230, 1506–1513. [Google Scholar] [CrossRef]
- Scacco, L.; Bolaffio, C.; Romano, A.; Fanciulli, M.; Baldi, A.; Spugnini, E.P. Adjuvant Electrochemotherapy Increases Local Control in a Recurring Equine Anal Melanoma. J. Equine Vet. Sci. 2013, 33, 637–639. [Google Scholar] [CrossRef]
- Goodrich, L.R.; Semevolos, S.A. How to Prepare and Inject Cisplatin in Oily Emulsion to Treat Equine Sarcoids and Squamous Cell Carcinomas. In Proceedings of the Annual Convention of the AAEP, San Antonio, TX, USA, 26–29 November 2000; pp. 173–175. [Google Scholar]
- Bienert-Zeit, A.; Nordemann, E.; von Borstel, M.; Wohlsein, P.; Iseringhausen, M.; Hellige, M.; Rötting, A. Unilateral Exophthalmos in a Horse-Diagnosis, Management and Outcome. Pferdeheilkunde 2014, 30, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Spugnini, E.P.; d’Alterio, G.L.; Dotsinsky, I.; Mudrov, T.; Dragonetti, E.; Murace, R.; Citro, G.; Baldi, A. Electrochemotherapy for the Treatment of Multiple Melanomas in a Horse. J. Equine Vet. Sci. 2011, 31, 430–433. [Google Scholar] [CrossRef]
- Spugnini, E.P.; Scacco, L.; Bolaffio, C.; Baldi, A. Electrochemotherapy for the Treatment of Cutaneous Solid Tumors in Equids: A Retrospective Study. Open Vet. J. 2021, 11, 385–389. [Google Scholar] [CrossRef]
- Stauffer, P.R. Evolving Technology for Thermal Therapy of Cancer. J. Hyperth. 2005, 21, 731–744. [Google Scholar] [CrossRef]
- Plaschke, C.C.; Gehl, J.; Johannesen, H.H.; Fischer, B.M.; Kjaer, A.; Lomholt, A.F.; Wessel, I. Calcium Electroporation for Recurrent Head and Neck Cancer: A Clinical Phase I Study. Laryngoscope Investig. Otolaryngol. 2019, 4, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frandsen, S.K.; Gehl, J.; Tramm, T.; Thoefner, M.S. Calcium Electroporation of Equine Sarcoids. Animals 2020, 10, 517. [Google Scholar] [CrossRef] [Green Version]
- Galant, L.; Delverdier, M.; Lucas, M.N.; Raymond-Letron, I.; Teissie, J.; Tamzali, Y. Calcium Electroporation: The Bioelectrochemical Treatment of Spontaneous Equine Skin Tumors Results in a Local Necrosis. Bioelectrochemistry 2019, 129, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Byron, C.R.; DeWitt, M.R.; Latouche, E.L.; Davalos, R.v.; Robertson, J.L. Treatment of Infiltrative Superficial Tumors in Awake Standing Horses Using Novel High-Frequency Pulsed Electrical Fields. Front. Vet. Sci. 2019, 6, 265. [Google Scholar] [CrossRef] [Green Version]
- Laus, F.; Cerquetella, M.; Paggi, E.; Ippedico, G.; Argentieri, M.; Castellano, G.; Spaterna, A.; Tesei, B. Evaluation of Cimetidine as a Therapy for Dermal Melanomatosis in Grey Horse. Isr. J. Vet. Med. 2010, 65, 48–52. [Google Scholar]
- Enwerem, N.M.; Okogun, J.I.; Wambebe, C.O.; Okorie, D.A.; Akah, P.A. Anthelmintic Activity of the Stem Bark Extracts of Berlina Grandiflora and One of Its Active Principles, Betulinic Acid. Phytomedicine 2001, 8, 112–114. [Google Scholar] [CrossRef]
- Oliveira Costa, J.F.; Barbosa-Filho, J.M.; de Azevedo Maia, G.L.; Guimarães, E.T.; Meira, C.S.; Ribeiro-Dos-Santos, R.; Pontes De Carvalho, L.C.; Soares, M.B.P. Potent Anti-Inflammatory Activity of Betulinic Acid Treatment in a Model of Lethal Endotoxemia. Int. Immunopharmacol. 2014, 23, 469–474. [Google Scholar] [CrossRef] [Green Version]
- Liebscher, G.; Vanchangiri, K.; Mueller, T.; Feige, K.; Cavalleri, J.M.V.; Paschke, R. In Vitro Anticancer Activity of Betulinic Acid and Derivatives Thereof on Equine Melanoma Cell Lines from Grey Horses and Invivo Safety Assessment of the Compound NVX-207 in Two Horses. Chem. Biol. Interact. 2016, 246, 20–29. [Google Scholar] [CrossRef]
- Weber, L.A.; Meißner, J.; Delarocque, J.; Kalbitz, J.; Feige, K.; Kietzmann, M.; Michaelis, A.; Paschke, R.; Michael, J.; Pratscher, B.; et al. Betulinic Acid Shows Anticancer Activity against Equine Melanoma Cells and Permeates Isolated Equine Skin in Vitro. BMC Vet. Res. 2020, 16, 44. [Google Scholar] [CrossRef]
- Weber, L.A.; Puff, C.; Kalbitz, J.; Kietzmann, M.; Feige, K.; Bosse, K.; Rohn, K.; Cavalleri, J.M.V. Concentration Profiles and Safety of Topically Applied Betulinic Acid and NVX-207 in Eight Healthy Horses—A Randomized, Blinded, Placebo-Controlled, Crossover Pilot Study. J. Vet. Pharmacol. Ther. 2020, 44, 47–57. [Google Scholar] [CrossRef]
- Weber, L.A.; Delarocque, J.; Feige, K.; Kietzmann, M.; Kalbitz, J.; Meißner, J.; Paschke, R.; Cavalleri, J.M.V. Effects of Topically Applied Betulinic Acid and Nvx-207 on Melanocytic Tumors in 18 Horses. Animals 2021, 11, 3250. [Google Scholar] [CrossRef] [PubMed]
- Henson, F.M.D.; Dobson, J.M. Use of Radiation Therapy in the Treatment of Equine Neoplasia. Equine Vet. Educ. 2004, 16, 315–318. [Google Scholar] [CrossRef]
- Bradley, W.M.; Schilpp, D.; Khatibzadeh, S.M. Electronic Brachytherapy Used for the Successful Treatment of Three Different Types of Equine Tumours. Equine Vet. Educ. 2017, 29, 293–298. [Google Scholar] [CrossRef]
- Saulez, M.N.; Voigt, A.; Steyl, C.A.; van Wilpe, E.; Kotzen, J.; Daniels, F. Use of Ir 192 Interstitial Brachytherapy for an Equine Malignant Dermal Schwannoma. J. S. Afr. Vet. Assoc. 2009, 80, 264–269. [Google Scholar] [CrossRef]
- Müller, J.M.V.; Feige, K.; Wunderlin, P.; Hödl, A.; Meli, M.L.; Seltenhammer, M.; Grest, P.; Nicolson, L.; Schelling, C.; Heinzerling, L.M. Double-Blind Placebo-Controlled Study with Interleukin-18 and Interleukin-12-Encoding Plasmid DNA Shows Antitumor Effect in Metastatic Melanoma in Gray Horses. J. Immunother. 2011, 34, 58–64. [Google Scholar] [CrossRef] [Green Version]
- Heinzerling, L.M.; Feige, K.; Rieder, S.; Akens, M.K.; Dummer, R.; Stranzinger, G.; Moelling, K. Tumor Regression Induced by Intratumoral Injection of DNA Coding for Human Interleukin 12 into Melanoma Metastases in Gray Horses. J. Mol. Med. 2001, 78, 692–702. [Google Scholar] [CrossRef]
- Kim, K.W.; Lee, S.J.; Kim, W.Y.; Seo, J.H.; Lee, H.Y. How Can We Treat Cancer Disease Not Cancer Cells? Cancer Res. Treat. 2017, 49, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Lembcke, L.M.; Kania, S.A.; Blackford, J.T.; Trent, D.J.; Odoi, A.; Grosenbaugh, D.A.; Fraser, D.G.; Leard, T.; Phillips, J.C. Development of Immunologic Assays to Measure Response in Horses Vaccinated with Xenogeneic Plasmid DNA Encoding Human Tyrosinase. J. Equine Vet. Sci. 2012, 32, 607–615. [Google Scholar] [CrossRef]
- Phillips, J.C.; Blackford, J.T.; Lembcke, L.M.; Grosenbaugh, D.A.; Leard, A.T. Evaluation of Needle-Free Injection Devices for Intramuscular Vaccination in Horses. J. Equine Vet. Sci. 2011, 31, 738–743. [Google Scholar] [CrossRef]
- Phillips, J.C.; Lembcke, L.M.; Noltenius, C.E.; Newman, S.J.; Blackford, J.T.; Grosenbaugh, D.A.; Leard, A.T. Evaluation of Tyrosinase Expression in Melanomas. AJVR 2012, 73, 273–278. [Google Scholar] [CrossRef]
- Lembcke Perez Prieto, L.M. Safety and Immunoreactivity of a Xenogeneic DNA Plasmid Vaccine Expressing Human Tyrosinase in Tumor-Bearing Horses. Ph.D. Thesis, University of Tennessee, Knoxville, TN, USA, 2013. [Google Scholar]
- Mählmann, K.; Feige, K.; Juhls, C.; Endmann, A.; Schuberth, H.J.; Oswald, D.; Hellige, M.; Doherr, M.; Cavalleri, J.M.V. Local and Systemic Effect of Transfection-Reagent Formulated DNA Vectors on Equine Melanoma. BMC Vet. Res. 2015, 11, 107. [Google Scholar] [CrossRef] [Green Version]
- Finocchiaro, L.M.E.; Riveros, M.D.; Glikin, G.C. Cytokine-Enhanced Vaccine and Suicide Gene Therapy as Adjuvant Treatments of Metastatic Melanoma in a Horse. Vet. Rec. 2009, 164, 278–279. [Google Scholar] [CrossRef]
- Cavalleri, J.-M.v.; Mählmann, K.; Schuberth, H.-J.; Feige, K. Prospect for Immunological Therapies of the Equine Malignant Melanoma. Pferdeheilkunde 2015, 31, 448–460. [Google Scholar] [CrossRef] [Green Version]
- Nejman, D.; Livyatan, I.; Fuks, G.; Gavert, N.; Zwang, Y.; Geller, L.T.; Rotter-Maskowitz, A.; Weiser, R.; Mallel, G.; Gigi, E.; et al. The Human Tumor Microbiome Is Composed of Tumor Type-Specific Intracellular Bacteria. Science 2020, 368, 973–980. [Google Scholar] [CrossRef]
- Kalaora, S.; Nagler, A.; Nejman, D.; Alon, M.; Barbolin, C.; Barnea, E.; Ketelaars, S.L.C.; Cheng, K.; Vervier, K.; Shental, N.; et al. Identification of Bacteria-Derived HLA-Bound Peptides in Melanoma. Nature 2021, 592, 138–143. [Google Scholar] [CrossRef]
- Carroll, C.S.E.; Andrew, E.R.; Malik, L.; Elliott, K.F.; Brennan, M.; Meyer, J.; Hintze, A.; Almonte, A.A.; Lappin, C.; Macpherson, P.; et al. Simple and Effective Bacterial-Based Intratumoral Cancer Immunotherapy. J. Immunother. Cancer 2021, 9, e002688. [Google Scholar] [CrossRef]
- Sidor-Kaczmarek, J.; Cichorek, M.; Spodnik, J.H.; Wójcik, S.; Moryś, J. Proteasome Inhibitors against Amelanotic Melanoma. Cell Biol. Toxicol. 2017, 33, 557–573. [Google Scholar] [CrossRef] [Green Version]
- Selimovic, D.; Porzig, B.B.O.W.; El-Khattouti, A.; Badura, H.E.; Ahmad, M.; Ghanjati, F.; Santourlidis, S.; Haikel, Y.; Hassan, M. Bortezomib/Proteasome Inhibitor Triggers Both Apoptosis and Autophagy-Dependent Pathways in Melanoma Cells. Cell. Signal. 2013, 25, 308–318. [Google Scholar] [CrossRef]
- Lichtenstein, F.; Iqbal, A.; de Lima Will, S.E.A.; Bosch, R.V.; DeOcesano-Pereira, C.; Goldfeder, M.B.; Chammas, R.; Trufen, C.E.M.; Morais, K.L.P.; de Souza, J.G.; et al. Modulation of Stress and Immune Response by Amblyomin-X Results in Tumor Cell Death in a Horse Melanoma Model. Sci. Rep. 2020, 10, 6388. [Google Scholar] [CrossRef] [Green Version]
- Batista, I.F.C.; Chudzinski-Tavassi, A.M.; Faria, F.; Simons, S.M.; Barros-Batestti, D.M.; Labruna, M.B.; Leão, L.I.; Ho, P.L.; Junqueira-de-Azevedo, I.L.M. Expressed Sequence Tags (ESTs) from the Salivary Glands of the Tick Amblyomma Cajennense (Acari: Ixodidae). Toxicon 2008, 51, 823–834. [Google Scholar] [CrossRef]
- Willingham, S.B.; Volkmer, J.P.; Gentles, A.J.; Sahoo, D.; Dalerba, P.; Mitra, S.S.; Wang, J.; Contreras-Trujillo, H.; Martin, R.; Cohen, J.D.; et al. The CD47-Signal Regulatory Protein Alpha (SIRPa) Interaction Is a Therapeutic Target for Human Solid Tumors. Proc. Natl. Acad. Sci. USA 2012, 109, 6662–6667. [Google Scholar] [CrossRef] [Green Version]
- Caston, S.S.; Cooper, E.E.; Chandramani-Shivalingappa, P.; Sponseller, B.A.; Hostetter, J.M.; Sun, Y. CD47 Expression in Cryopreserved Equine Cutaneous Masses and Normal Skin. J. Vet. Diagn. Investig. 2016, 28, 408–413. [Google Scholar] [CrossRef] [Green Version]
- Freeman, G.J.; Long, A.J.; Iwai, Y.; Bourque, K.; Chernova, T.; Nishimura, H.; Fitz, L.J.; Malenkovich, N.; Okazaki, T.; Byrne, M.C.; et al. Engagement of the PD-1 Immunoinhibitory Receptor by a Novel B7 Family Member Leads to Negative Regulation of Lymphocyte Activation. J. Exp. Med. 2000, 192, 1027–1034. [Google Scholar] [CrossRef] [Green Version]
- Iwai, Y.; Terawaki, S.; Honjo, T. PD-1 Blockade Inhibits Hematogenous Spread of Poorly Immunogenic Tumor Cells by Enhanced Recruitment of Effector T Cells. Int. Immunol. 2005, 17, 133–144. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.M.; Hwu, W.-J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and Activity of Anti–PD-L1 Antibody in Patients with Advanced Cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [Green Version]
- Ganbaatar, O.; Konnai Id, S.; Okagawa Id, T.; Nojima, Y.; Maekawa, N.; Minato, E.; Kobayashi, A.; Ando, R.; Sasaki, N.; Miyakoshi, D.; et al. PD-L1 Expression in Equine Malignant Melanoma and Functional Effects of PD-L1 Blockade. PLoS ONE 2020, 15, e0234218. [Google Scholar] [CrossRef]
- Taketo, M.M. Review Cyclooxygenase-2 Inhibitors in Tumorigenesis (Part I). J. Natl. Cancer Inst. 1998, 90, 1529–1536. [Google Scholar] [CrossRef] [Green Version]
- Thamm, D.H.; Ehrhart Iii, E.J.; Charles, J.B.; Elce, Y.A. Brief communications and case reports Cyclooxygenase-2 Expression in Equine Tumors. Vet. Pathol. 2008, 45, 825–828. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Stage | Number of Masses | Diameter | Growth Pattern | Dissemination |
|---|---|---|---|---|
| 1 | Single | <2 cm | Slow (same size for months to years) | Absent |
| 2 | Multiple | <2 cm | Slow (same size for months to years) | Absent |
| 3 | Multiple | <4 cm | Slow (25% increase in size in months or years) | Present |
| 4 | Multiple | >4 cm | Rapid (25% increase in size in weeks or months) | Present |
| Tumor Type | Coat Color | Age | Clinical Features | Biological Behavior | Anatomical Localization |
|---|---|---|---|---|---|
| Naevus | Grey and non-grey horses | Young horses (5–6 yo) | Single masses | Benign | Neck, trunk, limbs and face |
| Dermal melanoma | Grey horses | Young horses (6–7 yo) Geriatric | Single or multiple spherical isolated masses | Benign or malignant | Ventral tail, perianal region, external genitalia, lips, eyelids |
| Dermal melanomatosis | Grey horses | Geriatric (>15 yo) | Multiple and coalescent masses | Benign or malignant | Ventral tail, perianal region, external genitalia, lips, eyelids |
| Anaplastic malignant melanoma | Grey horses | Geriatric (>15 yo) | Rare, but with fast growth to multiple and coalescent masses; Heterogeneous color (pink-grey) | Malignant and very aggressive, with high capacity for dissemination; death within months | Unspecified |
| Treatments | ||||||||
|---|---|---|---|---|---|---|---|---|
| Surgery | Chemotherapy | Electroporation | Oral | Topic | Radiotherapy | Immunotherapy | Bacterial products | Proteasome inhibition |
| Traditional surgery Cryosurgery Laser surgery | Cisplatine Adjunctive therapies: Electrochemotherapy Hyperthermia | With calcium Irreversible | Cimetidine | Betulinic acid | Teletherapy Brachytherapy Eletronic brachytherapy | Intratumoral Systemic | Amblyomin X | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pimenta, J.; Prada, J.; Cotovio, M. Equine Melanocytic Tumors: A Narrative Review. Animals 2023, 13, 247. https://doi.org/10.3390/ani13020247
Pimenta J, Prada J, Cotovio M. Equine Melanocytic Tumors: A Narrative Review. Animals. 2023; 13(2):247. https://doi.org/10.3390/ani13020247
Chicago/Turabian StylePimenta, José, Justina Prada, and Mário Cotovio. 2023. "Equine Melanocytic Tumors: A Narrative Review" Animals 13, no. 2: 247. https://doi.org/10.3390/ani13020247