
Procalcitonin as an Endogenous Biomarker for Mastitis in Cows

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Samples
2.2.1. Milk: Preparation for PCT Measurement, Somatic Cell Count, and Bacteriology
2.2.2. Blood: Preparation for PCT Measurement, Hematology, and Clinical Chemistry
2.3. Detection of PCT by Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Statistics
3. Results
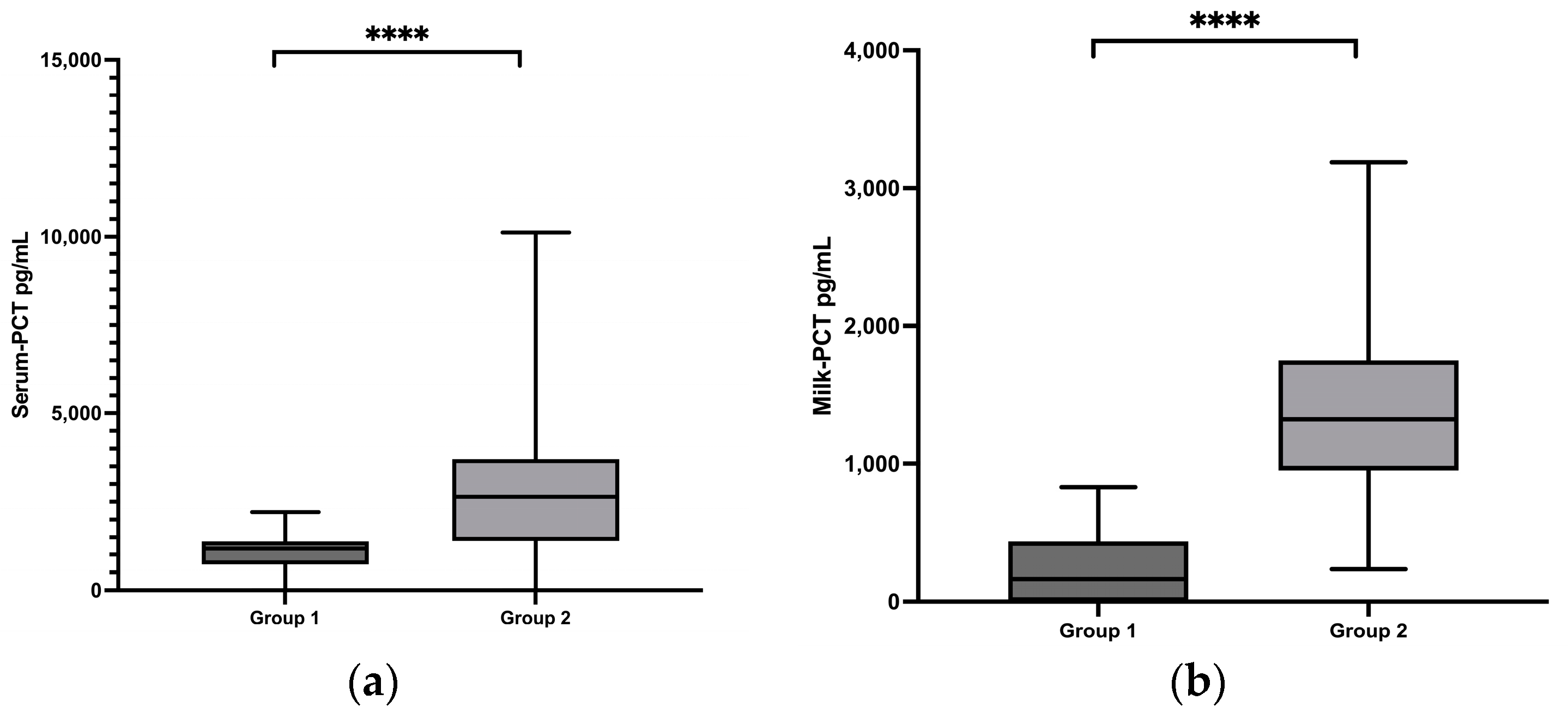
3.1. Comparison of PCT Concentrations in Healthy Cows vs. Cows with Clinical Mastitis
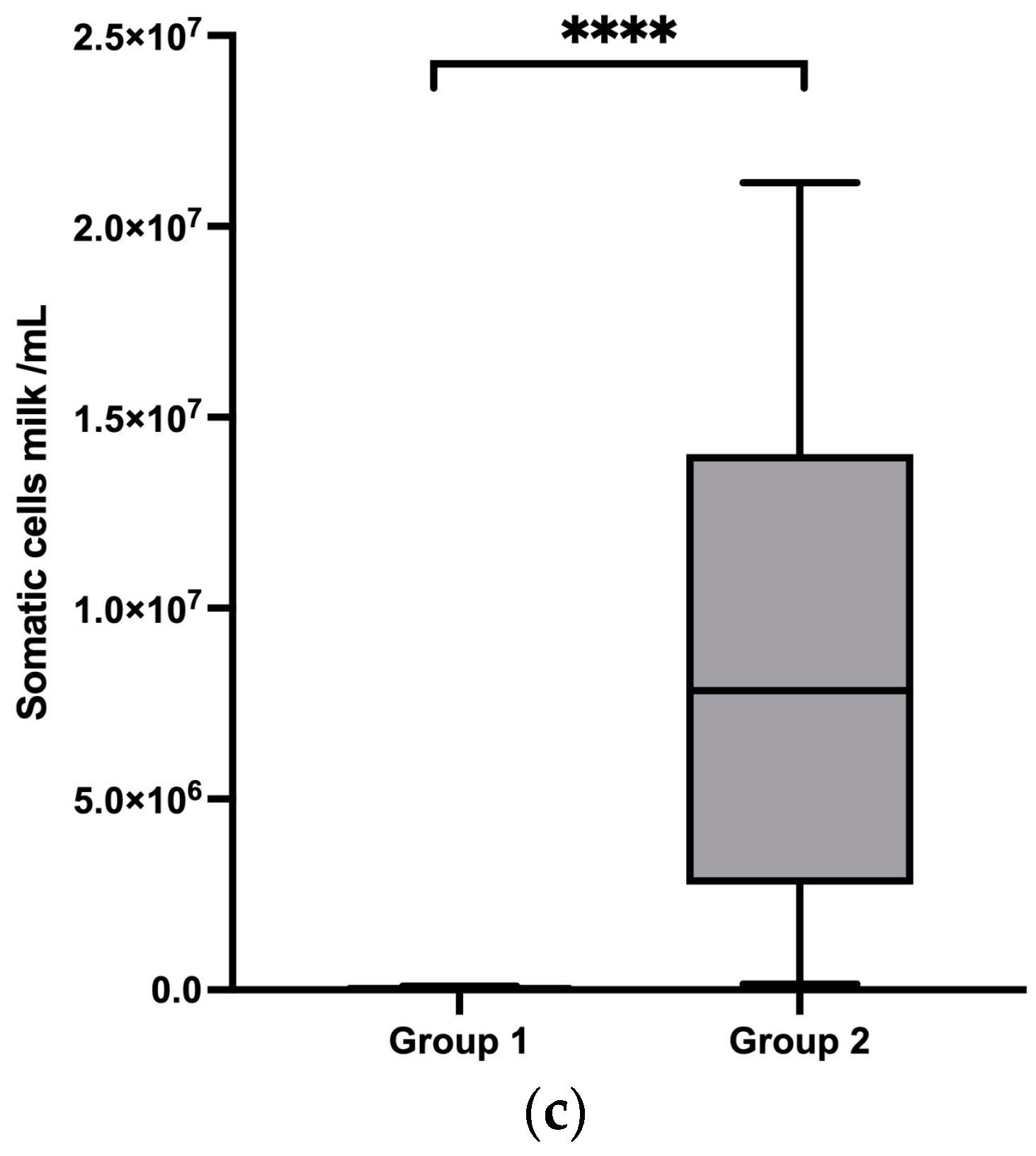
3.2. Comparison of PCT Concentrations between Healthy Cows and Cows with Subclinical Mastitis
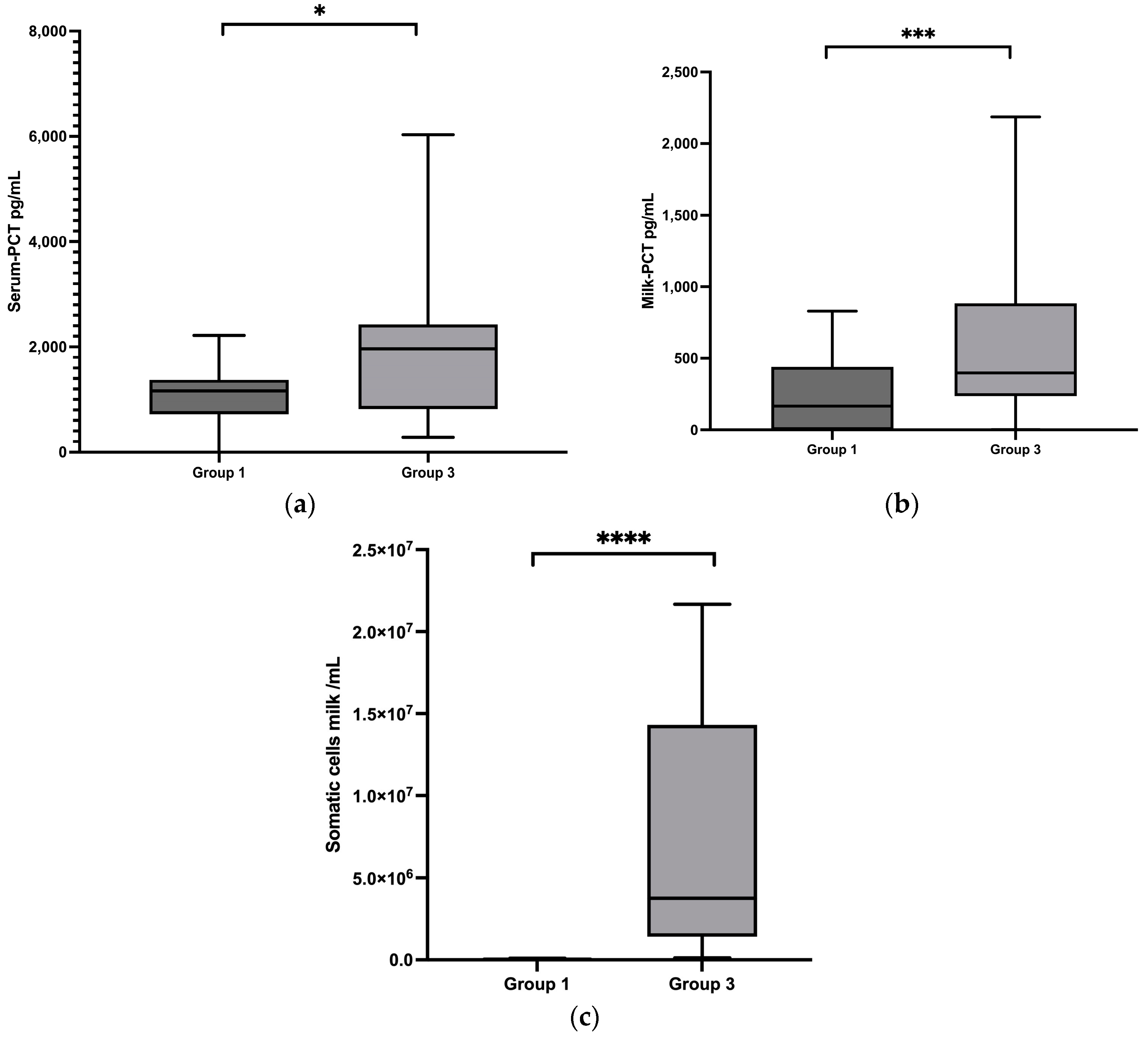
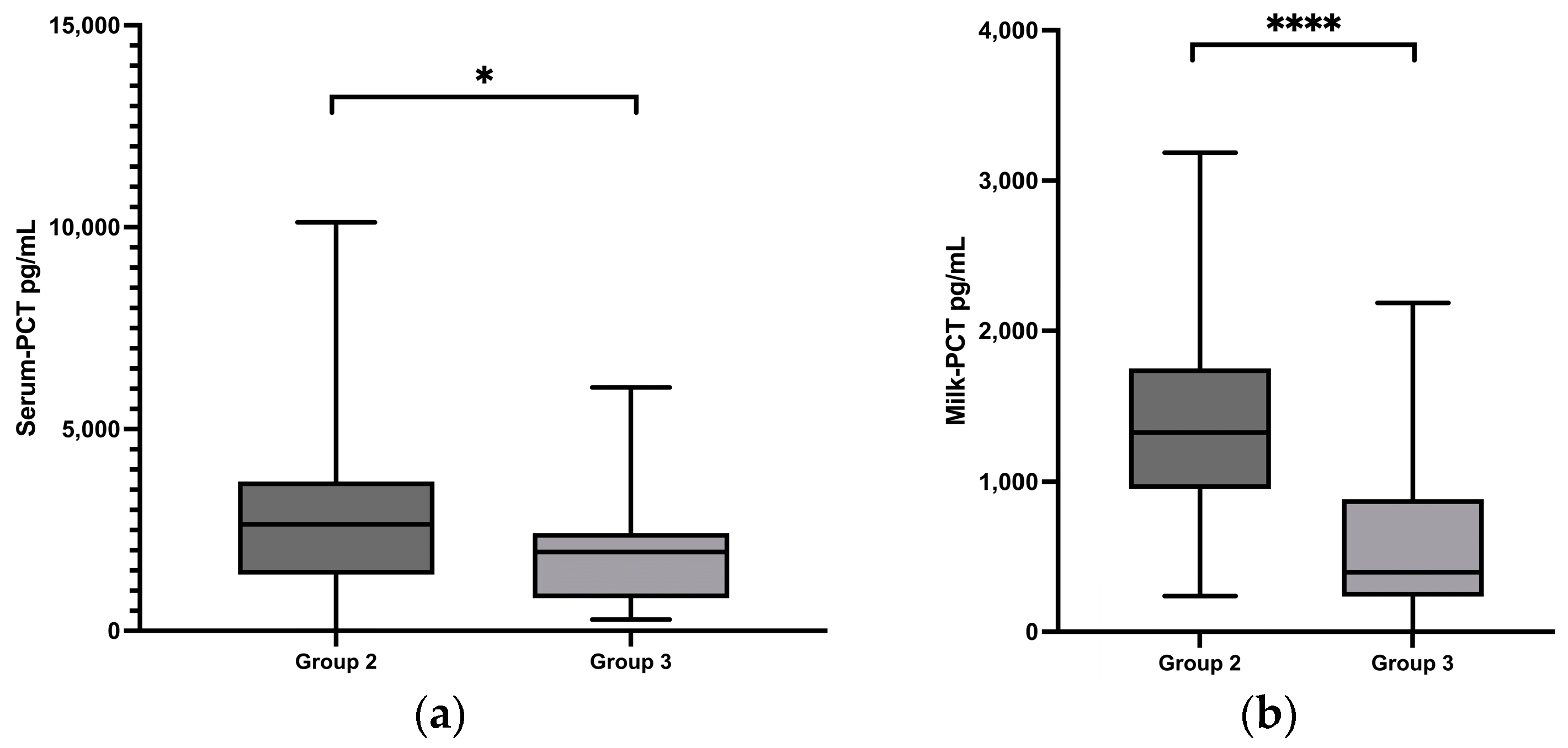
3.3. Comparison of PCT Concentrations between Cows with Clinical Mastitis and Cows with Subclinical Mastitis
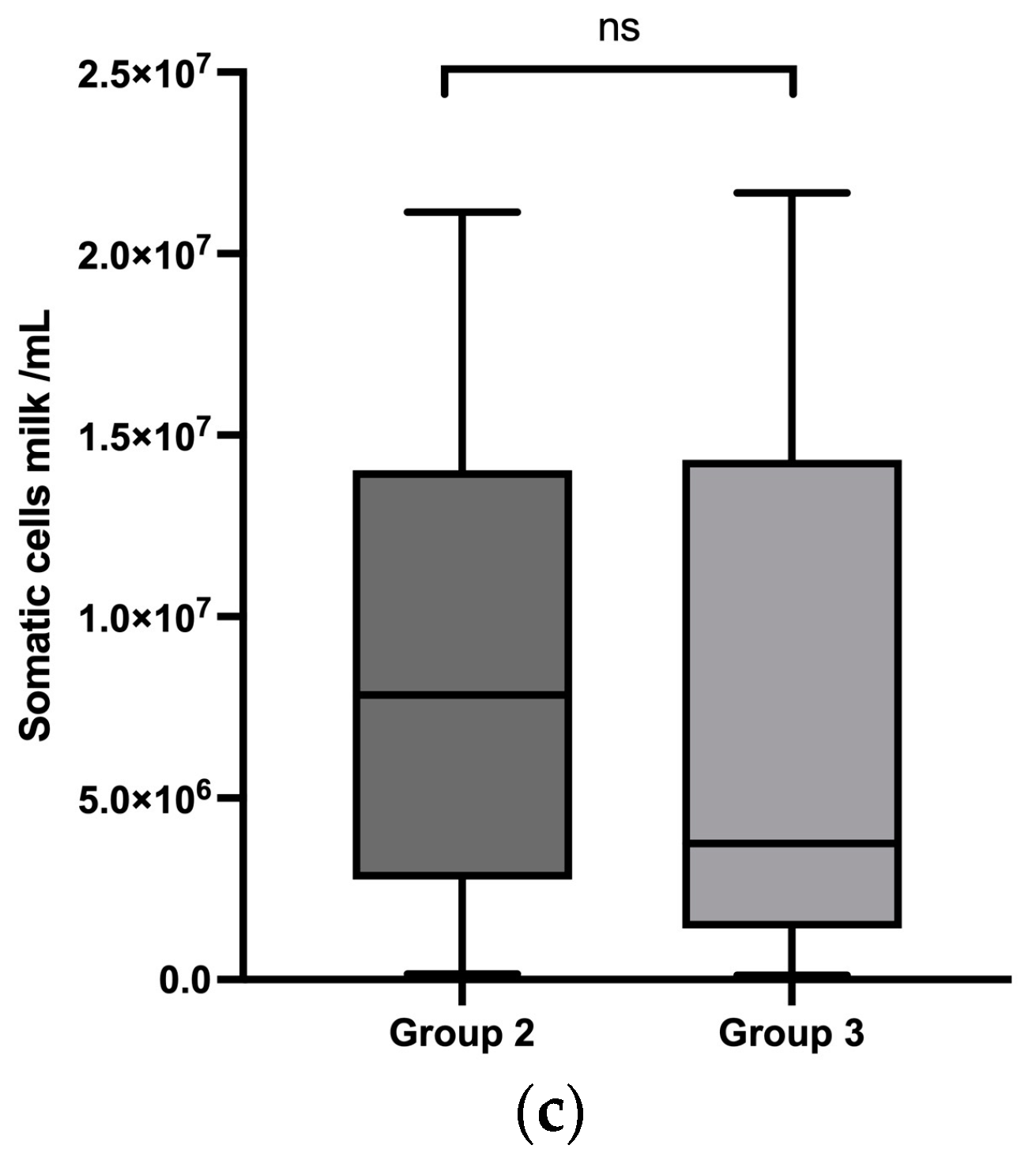
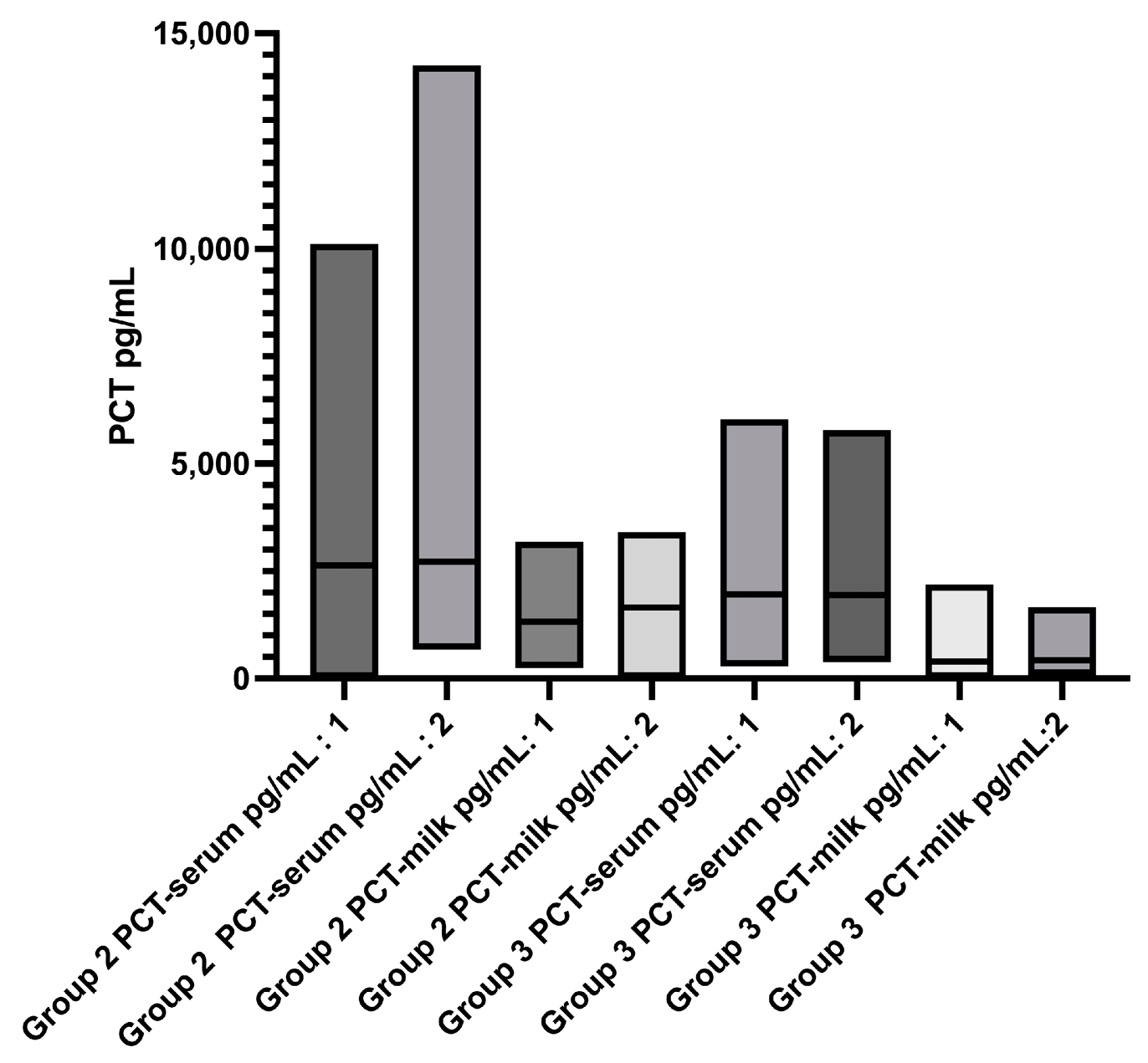
3.4. Comparison of Cells and PCT in Groups 2 and 3 between the Initial Examination and a Re-Examination after 12 Days
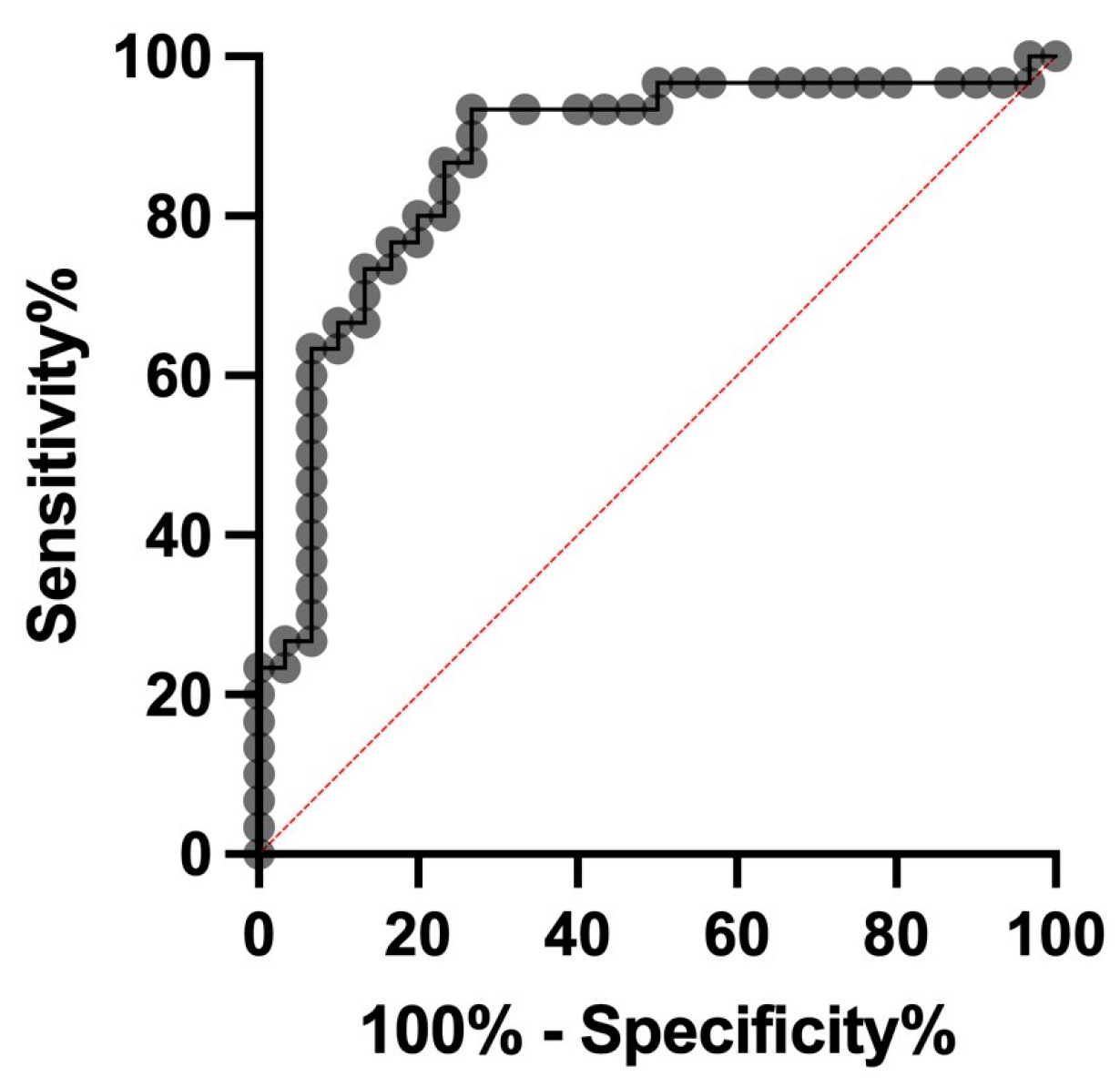
3.5. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mierzchała-Pasierb, M.; Lipińska-Gediga, M. Sepsis diagnosis and monitoring—Procalcitonin as standard, but what next? Anaesthesiol. Intensive Ther. 2019, 51, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Velissaris, D.; Zareifopoulos, N.; Lagadinou, M.; Platanaki, C.; Tsiotsios, K.; Stavridis, E.L.; Kasartzian, D.I.; Pierrakos, C.; Karamouzos, V. Procalcitonin and sepsis in the Emergency Department: An update. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, F.; Meucci, V.; Tognetti, R.; Bonelli, F.; Sgorbini, M.; Lubas, G.; Pretti, C.; Intorre, L. Procalcitonin Detection in Veterinary Species: Investigation of Commercial ELISA Kits. Animals 2020, 10, 1511. [Google Scholar] [CrossRef] [PubMed]
- Akyüz, E.; Gökce, G. Neopterin, procalcitonin, clinical biochemistry, and hematology in calves with neonatal sepsis. Trop. Anim. Health Prod. 2021, 53, 354. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, F.; Meucci, V.; Divers, T.J.; Boccardo, A.; Pravettoni, D.; Meylan, M.; Belloli, A.G.; Sgorbini, M. Plasma procalcitonin concentration in healthy calves and those with septic systemic inflammatory response syndrome. Vet. J. 2018, 234, 61–65. [Google Scholar] [CrossRef]
- Ercan, N.; Tuzcu, N.; Başbug, O.; Tuzcu, M.; Alim, A. Diagnostic value of serum procalcitonin, neopterin, and gamma interferon in neonatal calves with septicemic colibacillosis. J. Vet. Diagn. Investig. 2016, 28, 180–183. [Google Scholar] [CrossRef] [Green Version]
- Kirbas, A.; Kandemir, F.M.; Celebi, D.; Hanedan, B.; Timurkan, M.O. The use of inflammatory markers as a diagnostic and prognostic approach in neonatal calves with septicaemia. Acta Vet. Hun. 2019, 67, 360–376. [Google Scholar] [CrossRef]
- El-Deeb, W.; Elsohaby, I.; Fayez, M.; Mkrtchyan, H.V.; El-Etriby, D.; ElGioushy, M. Use of procalcitonin, neopterin, haptoglobin, serum amyloid A and proinflammatory cytokines in diagnosis and prognosis of bovine respiratory disease in feedlot calves under field conditions. Acta Trop. 2020, 204, 105336. [Google Scholar] [CrossRef]
- El-Deeb, W.; Fayez, M.; Alhumam, N.; Elsohaby, I.; Quadri, S.A.; Mkrtchyan, H. The effect of staphylococcal mastitis including resistant strains on serum procalcitonin, neopterin, acute phase response and stress biomarkers in Holstein dairy cows. PeerJ 2021, 9, e11511. [Google Scholar] [CrossRef]
- Bonelli, F.; Madrigali, A.; Sgorbini, M.; Meucci, V.; Battaglia, F.; Guélat-Brechbuehl, M.; Sala, G.; Meylan, M. Case—Control study: Evaluation of plasma procalcitonin concentration as an indicator of inflammation in healthy and sick cows. Res. Vet. Sci. 2023, 155, 56–61. [Google Scholar] [CrossRef]
- López-Martínez, M.J.; Franco-Martínez, L.; Martínez-Subiela, S.; Cerón, J.J. Biomarkers of sepsis in pigs, horses and cattle: From acute phase proteins to procalcitonin. Anim. Health Res. Rev. 2022, 23, 82–99. [Google Scholar] [CrossRef]
- Dalanezi, F.M.; Joaquim, S.F.; Guimarães, F.F.; Guerra, S.T.; Lopes, B.C.; Schmidt, E.M.S.; Cerri, R.L.A.; Langoni, H. Influence of pathogens causing clinical mastitis on reproductive variables of dairy cows. J. Dairy Sci. 2020, 103, 3648–3655. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Jaccard-Stolz, D.; Bingisser, R.; Gencay, M.M.; Huber, P.R.; Tamm, M.; Müller, B. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: Cluster-randomised, single-blinded intervention trial. Lancet 2004, 363, 600–607. [Google Scholar] [CrossRef]
- Teuber, M. Veterinary use and antibiotic resistance. Curr. Opin. Microbiol. 2001, 4, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Bassim, C.W.; Redman, R.S.; DeNucci, D.J.; Becker, K.L.; Nylén, E.S. Salivary procalcitonin and periodontitis in diabetes. J. Dent. Res. 2008, 87, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, J.A.; Elster, E.A.; Andersen, R.C.; Nylén, E.; Brown, T.S.; Rose, M.W.; Stojadinovic, A.; Becker, K.L.; McGuigan, F.X. Correlation of procalcitonin and cytokine expression with dehiscence of wartime extremity wounds. J. Bone Jt. Surg. 2008, 90, 580–588. [Google Scholar] [CrossRef]
- Struck, J.; de Almeida, P.; Bergmann, A.; Morgenthaler, N.G. High concentrations of procalcitonin but not mature calcitonin in normal human milk. Horm. Metab. Res. 2002, 34, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Deb, R.; Kumar, A.; Chakraborty, S.; Verma, A.K.; Tiwari, R.; Dhama, K.; Singh, U.; Kumar, S. Trends in diagnosis and control of bovine mastitis: A review. Pak. J. Biol. Sci. 2013, 16, 1653–1661. [Google Scholar] [CrossRef] [Green Version]
- Swinkels, J.M.; Hilkens, A.; Zoche-Golob, V.; Kromker, V.; Buddiger, M.; Jansen, J.; Lam, T.J. Social influences on the duration of antibiotic treatment of clinical mastitis in dairy cows. J. Dairy Sci. 2015, 98, 2369–2380. [Google Scholar] [CrossRef] [Green Version]
- Meucci, V.; Orsetti, C.; Sgorbini, M.; Battaglia, F.; Cresci, M.; Bonelli, F. Can Procalcitonin Be Dosed in Bovine Milk Using a Commercial ELISA Kit? Animals 2022, 12, 289. [Google Scholar] [CrossRef]
- Assicot, M.; Gendrel, D.; Carsin, H.; Raymond, J.; Guilbaud, J.; Bohuon, C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet 1993, 341, 515–518. [Google Scholar] [CrossRef]
- Schneider, H.G.; Lam, Q.T. Procalcitonin for the clinical laboratory: A review. Pathology 2007, 39, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Barton, A.K.; Pelli, A.; Rieger, M.; Gehlen, H. Procalcitonin as a biomarker in equine chronic pneumopathies. BMC Vet. Res. 2016, 12, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meisner, M. Pathobiochemistry and clinical use of procalcitonin. Clin. Chim. Acta 2002, 323, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Long, W.; Yan, L.; Zhang, Y.; Xie, J.; Lu, G.; Yang, C. Procalcitonin guided antibiotic therapy of acute exacerbations of asthma: A randomized controlled trial. BMC Infect. Dis. 2013, 13, 596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christ-Crain, M.; Stolz, D.; Bingisser, R.; Müller, C.; Miedinger, D.; Huber, P.R.; Zimmerli, W.; Harbarth, S.; Tamm, M.; Müller, B. Procalcitonin guidance of antibiotic therapy in community-acquired pneumonia: A randomized trial. Am. J. Respir. Crit. Care Med. 2006, 174, 84–93. [Google Scholar] [CrossRef] [Green Version]
- Barlow, J. Mastitis therapy and antimicrobial susceptibility: A multispecies review with a focus on antibiotic treatment of mastitis in dairy cattle. J. Mammary Gland Biol. Neoplasia 2011, 16, 383–407. [Google Scholar] [CrossRef]
- Roy, J.P.; Keefe, G. Systematic review: What is the best antibiotic treatment for Staphylococcus aureus intramammary infection of lactating cows in North America? Vet. Clin. N. Am. Food Anim. Pract. 2012, 28, 39–50. [Google Scholar] [CrossRef]
- Preas, H.L., 2nd; Nylén, E.S.; Snider, R.H.; Becker, K.L.; White, J.C.; Agosti, J.M.; Suffredini, A.F. Effects of anti-inflammatory agents on serum levels of calcitonin precursors during human experimental endotoxemia. J. Infect. Dis. 2011, 184, 373–376. [Google Scholar] [CrossRef]
- Fogsgaard, K.K.; Lovendahl, P.; Bennedsgaard, T.W.; Ostergaard, S. Changes in milk yield, lactate dehydrogenase, milking frequency, and interquarter yield ratio persist for up to 8 weeks after antibiotic treatment of mastitis. J. Dairy Sci. 2015, 98, 7686–7698. [Google Scholar] [CrossRef] [Green Version]
- Monneret, G.; Laroche, B.; Bienvenu, J. Procalcitonin is not produced by circulating blood cells. Infection 1999, 27, 34–35. [Google Scholar] [CrossRef] [PubMed]
- Müller, B.; Becker, K.L. Procalcitonin: How a hormone became a marker and mediator of sepsis. Swiss Med. Wkly. 2001, 131, 595–602. [Google Scholar] [PubMed]
- Krömker, V. Euterkrankheiten. In Kurzes Lehrbuch Milchkunde und Milchhygiene; Krömker, V., Bruckmaier, R.M., Eds.; Parey: Stuttgart, Germany, 2007; pp. 47–74. [Google Scholar]
- Oliveira, L.; Hulland, C.; Ruegg, P.L. Characterization of clinical mastitis occurring in cows on 50 large dairy herds in Wisconsin. J. Dairy Sci. 2013, 96, 7538–7549. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.L.; Snider, R.; Nylén, E.S. Procalcitonin in sepsis and systemic inflammation: A harmful biomarker and a therapeutic target. Br. J. Pharmacol. 2010, 159, 253–264. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cows with Clinical Mastitis | Cows with Subclinical Mastitis | Healthy Control Cows T1 | |||
|---|---|---|---|---|---|
| T1 | T2 | T1 | T2 | ||
| Internal body Temperature (°C) | 39.3 (38.3 to 40.8) | 38.7 (38.1 to 41.1) | 38.4 (37.6 to 38.9) | 38.6 (37.8 to 38.9) | 38.3 (37.3 to 38.9) |
| Somatic cells/mL (n = measurable samples) | 7,842,000 (n = 14) (155,000 to 21,142,000) | 701,000 (n = 28) (56,000 to 21,628,000) | 3,753,000 (n = 30) (117,000 to 21,673,000) | 1,206,000 (n = 29) (101,000 to 23,305,000) | 47,000 (n = 28) (7000 to 100,000) |
| Leukocytes (103/µL) | 6.9 (n = 24) (0.4 to 13) | 9.0 (n = 30) (0.2 to 27.5) | 8.7 (n = 29) (5.4 to 17.9) | 7.6 (n = 29) (3.5 to 11.4) | 7.3 (n = 27) (4.7 to 10.0) |
| Bacteria (main pathogens) | Streptococcus uberis (n = 12), Escherichia coli (n = 6) | Streptococcus uberis (n = 7), Escherichia coli (n = 7) | Streptococcus uberis (n = 11), Staphylococcus aureus (n = 7), Streptococcus dysgalactiae (n = 5) | Streptococcus uberis (n = 5) Staphylococcus aureus (n = 7), Streptococcus dysgalactiae (n = 3), Escherichia coli (n = 2) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neumann, S.; Siegert, S.; Fischer, A. Procalcitonin as an Endogenous Biomarker for Mastitis in Cows. Animals 2023, 13, 2204. https://doi.org/10.3390/ani13132204
Neumann S, Siegert S, Fischer A. Procalcitonin as an Endogenous Biomarker for Mastitis in Cows. Animals. 2023; 13(13):2204. https://doi.org/10.3390/ani13132204
Chicago/Turabian StyleNeumann, Stephan, Stephan Siegert, and Anneke Fischer. 2023. "Procalcitonin as an Endogenous Biomarker for Mastitis in Cows" Animals 13, no. 13: 2204. https://doi.org/10.3390/ani13132204