

Neutrophil Gelatinase-Associated Lipocalin in Synovial Fluid from Horses with and without Septic Arthritis
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Horses
3.2. Samples and Synovial Structures
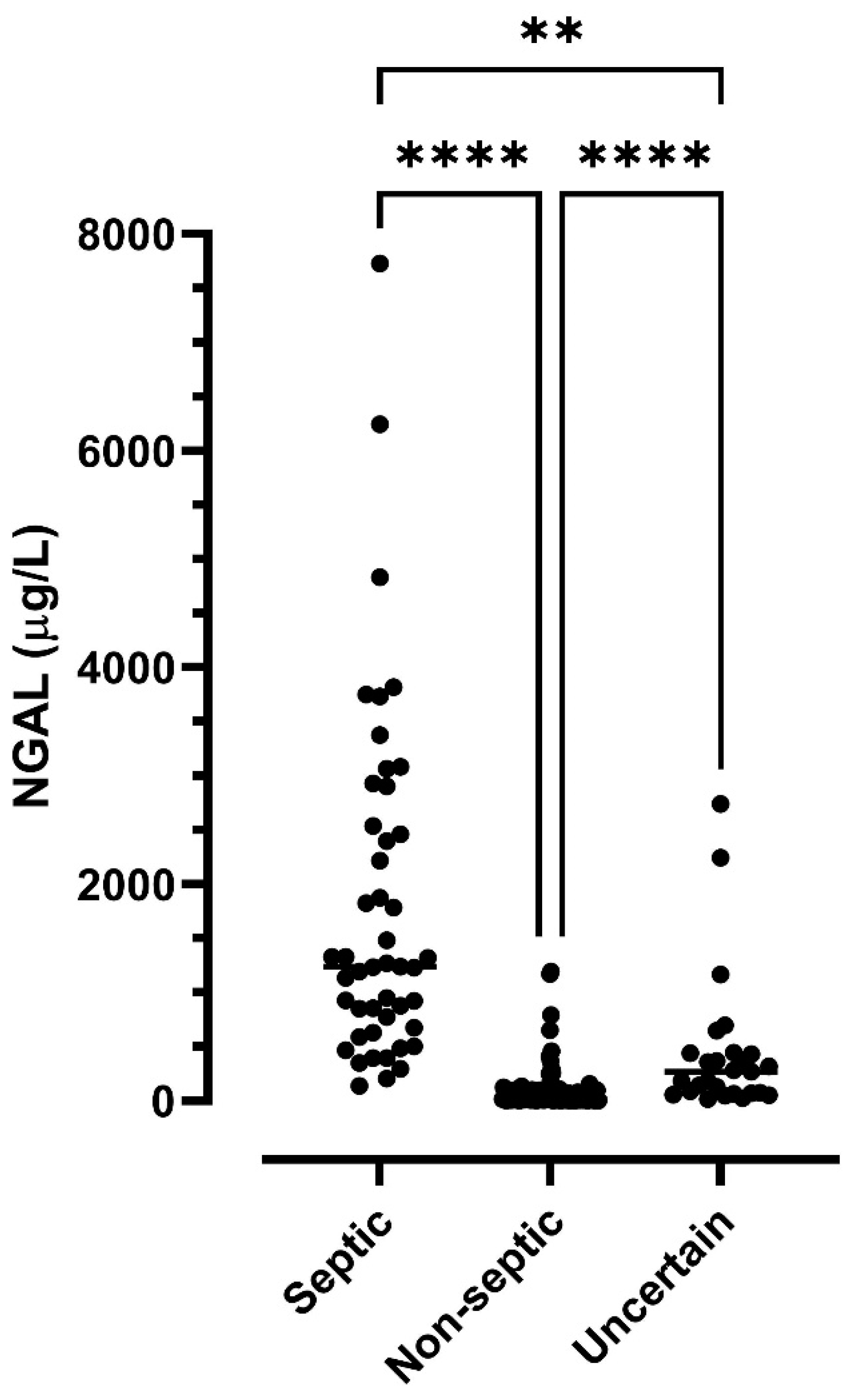
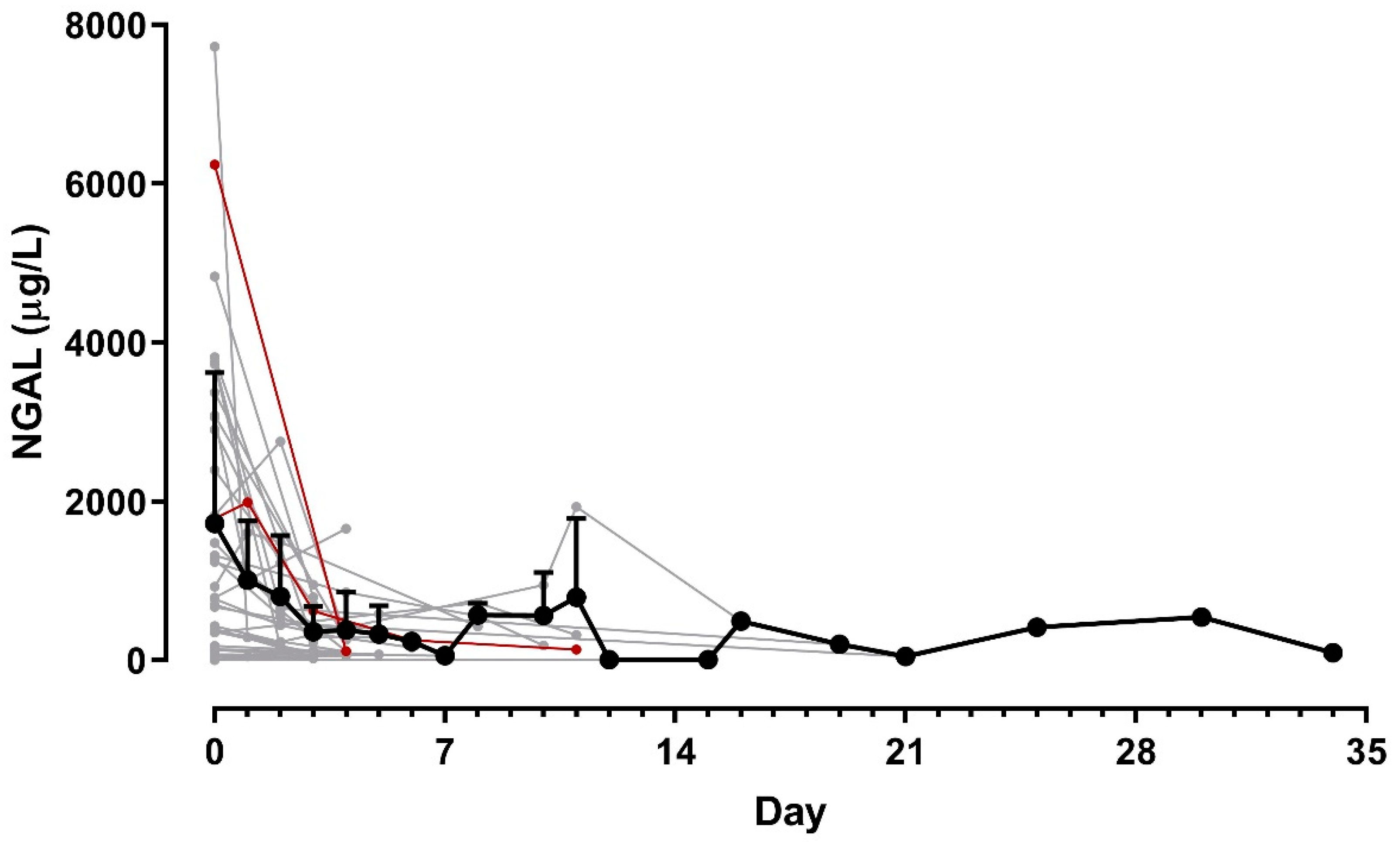
3.3. NGAL Concentrations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vos, N.J.; Ducharme, N.G. Analysis of factors influencing prognosis in foals with septic arthritis. Ir. Vet. J. 2008, 61, 102–106. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Martinez, L.M.; Elmas, C.R.; Black, B.; Monteith, G. Clinical use of antimicrobial regional limb perfusion in horses: 174 cases (1999–2009). J. Am. Vet. Med. Assoc. 2012, 241, 1650–1658. [Google Scholar] [CrossRef] [Green Version]
- Lindegaard, C.; van Galen, G.; Aarsvold, S.; Berg, L.; Verwilghen, D. Haematogenous septic arthritis, physitis and osteomyelitis in foals: A tutorial review on pathogenesis, diagnosis, treatment and prognosis. Part 2. Eq. Vet. Edu 2022, 34, 37–48. [Google Scholar] [CrossRef]
- Glass, K.; Watts, A.E. Septic arthritis, physitis, and osteomyelitis in foals. Vet. Clin. N. Am. Equine Pract. 2017, 33, 299–314. [Google Scholar] [CrossRef] [PubMed]
- Lindegaard, C.; van Galen, G.; Aarsvold, S.; Berg, L.C.; Verwilghen, D. Haematogenous septic arthritis, physitis and osteomyelitis in foals: A tutorial review on pathogenesis, diagnosis, treatment and prognosis. Part 1. Eq. Vet. Edu. 2021, 33, 659–672. [Google Scholar] [CrossRef]
- Ludwig, E.K.; van Harreveld, P.D. Equine wounds over synovial structures. Vet. Clin. N. Am. Equine Pract. 2018, 34, 575–590. [Google Scholar] [CrossRef]
- Gilbertie, J.M.; Schnabel, L.V.; Stefanovski, D.; Kelly, D.J.; Jacob, M.E.; Schaer, T.P. Gram-negative multi-drug resistant bacteria influence survival to discharge for horses with septic synovial structures: 206 Cases (2010–2015). Vet. Microbiol. 2018, 226, 64–73. [Google Scholar] [CrossRef]
- Firth, E.C. Current concepts of infectious polyarthritis in foals. Equine Vet. J. 1983, 15, 5–9. [Google Scholar] [CrossRef]
- Jacobsen, S.; Thomsen, M.H.; Nanni, S. Concentrations of serum amyloid A in serum and synovial fluid from healthy horses and horses with joint disease. Am. J. Vet. Res. 2006, 67, 1738–1742. [Google Scholar] [CrossRef]
- Smit, Y.; Marais, H.J.; Thompson, P.N.; Mahne, A.T.; Goddard, A. Clinical findings, synovial fluid cytology and growth factor concentrations after intra-articular use of a platelet-rich product in horses with osteoarthritis. J. S. Afr. Vet. Assoc. 2019, 90, e1–e9. [Google Scholar] [CrossRef]
- Sanchez-Teran, A.F.; Bracamonte, J.L.; Hendrick, S.; Burguess, H.J.; Duke-Novakovski, T.; Schott, M.; Hoff, B.; Rubio-Martinez, L.M. Effect of arthroscopic lavage on systemic and synovial fluid serum amyloid A in healthy horses. Vet. Surg. 2016, 45, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Adler, D.M.T.; Serteyn, D.; Franck, T.; Jorgensen, E.; Christophersen, M.T.; Denwood, M.; Verwilghen, D.R. Effects of intra-articular administration of lidocaine, mepivacaine, and the preservative methyl parahydroxybenzoate on synovial fluid biomarkers of horses. Am. J. Vet. Res. 2020, 81, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Abella, V.; Scotece, M.; Conde, J.; Gomez, R.; Lois, A.; Pino, J.; Gomez-Reino, J.J.; Lago, F.; Mobasheri, A.; Gualillo, O. The potential of lipocalin-2/NGAL as biomarker for inflammatory and metabolic diseases. Biomarkers 2015, 20, 565–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flo, T.H.; Smith, K.D.; Sato, S.; Rodriguez, D.J.; Holmes, M.A.; Strong, R.K.; Akira, S.; Aderem, A. Lipocalin 2 mediates an innate immune response to bacterial infection by sequestrating iron. Nature 2004, 432, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Bao, G.; Clifton, M.; Hoette, T.M.; Mori, K.; Deng, S.X.; Qiu, A.; Viltard, M.; Williams, D.; Paragas, N.; Leete, T.; et al. Iron traffics in circulation bound to a siderocalin (Ngal)-catechol complex. Nat. Chem. Biol. 2010, 6, 602–609. [Google Scholar] [CrossRef]
- Goetz, D.H.; Holmes, M.A.; Borregaard, N.; Bluhm, M.E.; Raymond, K.N.; Strong, R.K. The neutrophil lipocalin NGAL is a bacteriostatic agent that interferes with siderophore-mediated iron acquisition. Mol. Cell 2002, 10, 1033–1043. [Google Scholar] [CrossRef]
- Bjorkqvist, M.; Kallman, J.; Fjaertoft, G.; Xu, S.; Venge, P.; Schollin, J. Human neutrophil lipocalin: Normal levels and use as a marker for invasive infection in the newborn. Acta Paediatr. 2004, 93, 534–539. [Google Scholar] [CrossRef]
- Fjaertoft, G.; Foucard, T.; Xu, S.; Venge, P. Human neutrophil lipocalin (HNL) as a diagnostic tool in children with acute infections: A study of the kinetics. Acta Paediatr. 2005, 94, 661–666. [Google Scholar] [CrossRef]
- Xu, S.Y.; Pauksen, K.; Venge, P. Serum measurements of human neutrophil lipocalin (HNL) discriminate between acute bacterial and viral infections. Scand. J. Clin. Lab. Investig. 1995, 55, 125–131. [Google Scholar] [CrossRef]
- Frydendal, C.; Nielsen, K.B.; Berg, L.C.; van Galen, G.; Adler, D.M.T.; Andreassen, S.M.; Jacobsen, S. Influence of clinical and experimental intra-articular inflammation on neutrophil gelatinase-associated lipocalin concentrations in horses. Vet. Surg. 2021, 50, 641–649. [Google Scholar] [CrossRef]
- Winther, M.F.; Haugaard, S.L.; Pihl, T.H.; Jacobsen, S. Concentrations of neutrophil gelatinase-associated lipocalin are increased in serum and peritoneal fluid from horses with inflammatory abdominal disease and non-strangulating intestinal infarctions. Equine Vet. J. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Van Galen, G.; Jacobsen, S.; Vinther, A.M.; Laurberg, M.B.; Tvermose, E.; Broe-Brøndum, R.; Theisen, L.P.; Berg, L. NGAL: A new biomarker in the horse for renal injury and inflammation. In Proceedings of the 11th Annual European College of Equine Internal Medicine Congress, Ghent, Belgium, 9–10 November 2018; Volume 33, pp. 1549–1550. [Google Scholar]
- Vergara, A.; Fernandez-Pittol, M.J.; Munoz-Mahamud, E.; Morata, L.; Bosch, J.; Vila, J.; Soriano, A.; Casals-Pascual, C. Evaluation of lipocalin-2 as a biomarker of periprosthetic joint infection. J. Arthroplasty 2019, 34, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Deirmengian, C.; Kardos, K.; Kilmartin, P.; Cameron, A.; Schiller, K.; Parvizi, J. Diagnosing periprosthetic joint infection: Has the era of the biomarker arrived? Clin. Orthop. Relat. Res. 2014, 472, 3254–3262. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Li, X.; Ni, M.; Fu, J.; Xu, C.; Chai, W.; Chen, J.Y. What is the performance of novel synovial biomarkers for detecting periprosthetic joint infection in the presence of inflammatory joint disease? Bone Joint J. 2021, 103-B, 32–38. [Google Scholar] [CrossRef]
- Dijkman, C.; Thomas, A.R.; Koenraadt, K.L.M.; Ermens, A.A.M.; van Geenen, R.C.I. Synovial neutrophilic gelatinase-associated lipocalin in the diagnosis of periprosthetic joint infection after total knee arthroplasty. Arch. Orthop. Trauma Surg. 2020, 140, 941–947. [Google Scholar] [CrossRef]
- Jacobsen, S.; Berg, L.C.; Tvermose, E.; Laurberg, M.B.; van Galen, G. Validation of an ELISA for detection of neutrophil gelatinase-associated lipocalin (NGAL) in equine serum. Vet. Clin. Pathol. 2018, 47, 603–607. [Google Scholar] [CrossRef]
- Haralambus, R.; Florczyk, A.; Sigl, E.; Gultekin, S.; Vogl, C.; Brandt, S.; Schnierer, M.; Gamerith, C.; Jenner, F. Detection of synovial sepsis in horses using enzymes as biomarkers. Equine Vet. J. 2022, 54, 513–522. [Google Scholar] [CrossRef]
- Stack, J.D.; Cousty, M.; Steele, E.; Handel, I.; Lechartier, A.; Vinardell, T.; David, F. Comparison of serum amyloid A measurements in equine synovial fluid with routine diagnostic methods to detect synovial infection in a clinical environment. Front. Vet. Sci. 2019, 6, 325. [Google Scholar] [CrossRef]
- Liu, H.; Yu, Y.; Niu, Y. Utility of Human Neutrophil Lipocalin as a Diagnosing Biomarker of Prosthetic Joint Infection: A Clinical Pilot Study. Infect. Drug Resist. 2022, 15, 2393–2400. [Google Scholar] [CrossRef]
- Venge, P. Human neutrophil lipocalin (HNL) as a biomarker of acute infections. Ups. J. Med. Sci. 2018, 123, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Laurberg, M.B.; Jacobsen, S.; Berg, L.C.; Laursen, S.H.; Karlsson, E.; Sånge, E.A.; Ticehurst, C.; van Galen, G. Estimation of prevalence of acute kidney injury (AKI) in hospitalized neonatal foals based on a multimodal approach including serumneutrophil gelatinase-associated lipocalin (NGAL) concentrations upon admission. In In Proceedings of the 13th Annual European College of Equine Internal Medicine Congress, Online, 20 November 2020; Volume 35, pp. 1181–1182. [Google Scholar]
- Siwinska, N.; Zak, A.; Paslawska, U. Evaluation of serum and urine neutrophil gelatinase-associated lipocalin and cystatin C as biomarkers of acute kidney injury in horses. J. Vet. Res. 2021, 65, 245–252. [Google Scholar] [CrossRef]
- Haneda, S.; Nagaoka, K.; Nambo, Y.; Kikuchi, M.; Nakano, Y.; Li, J.; Matsui, M.; Miyake, Y.I.; Imakawa, K. Expression of uterine lipocalin 2 and its receptor during early- to mid-pregnancy period in mares. J. Reprod. Dev. 2017, 63, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marth, C.D.; Firestone, S.M.; Glenton, L.Y.; Browning, G.F.; Young, N.D.; Krekeler, N. Oestrous cycle-dependent equine uterine immune response to induced infectious endometritis. Vet. Res. 2016, 47, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marth, C.D.; Firestone, S.M.; Hanlon, D.; Glenton, L.Y.; Browning, G.F.; Young, N.D.; Krekeler, N. Innate immune genes in persistent mating-induced endometritis in horses. Reprod. Fertil. Dev. 2018, 30, 533–545. [Google Scholar] [CrossRef]
- Marth, C.D.; Young, N.D.; Glenton, L.Y.; Noden, D.M.; Browning, G.F.; Krekeler, N. Deep sequencing of the uterine immune response to bacteria during the equine oestrous cycle. BMC Genomics 2015, 16, 934. [Google Scholar] [CrossRef] [Green Version]
- Hayes, M.A.; Quinn, B.A.; Keirstead, N.D.; Katavolos, P.; Waelchli, R.O.; Betteridge, K.J. Proteins associated with the early intrauterine equine conceptus. Reprod. Domest. Anim. 2008, 43, 232–237. [Google Scholar] [CrossRef]
- Gupta, K.; Shukla, M.; Cowland, J.B.; Malemud, C.J.; Haqqi, T.M. Neutrophil gelatinase-associated lipocalin is expressed in osteoarthritis and forms a complex with matrix metalloproteinase 9. Arthritis Rheum. 2007, 56, 3326–3335. [Google Scholar] [CrossRef]
- Katano, M.; Okamoto, K.; Arito, M.; Kawakami, Y.; Kurokawa, M.S.; Suematsu, N.; Shimada, S.; Nakamura, H.; Xiang, Y.; Masuko, K.; et al. Implication of granulocyte-macrophage colony-stimulating factor induced neutrophil gelatinase-associated lipocalin in pathogenesis of rheumatoid arthritis revealed by proteome analysis. Arthritis Res. Ther. 2009, 11, R3. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Synovial Structure | Number and Percentage of Samples | Classification |
|---|---|---|
| Tarsometatarsal joint | 1 (0.6%) | Septic = 0 |
| Non-septic = 1 | ||
| Uncertain = 0 | ||
| Carpal and tarsal sheaths | 2 (1.1%) | Septic = 0 |
| Non-septic = 2 | ||
| Uncertain = 0 | ||
| Extensor tendon sheaths (common digital extensor, extensor carpi radialis) | 2 (1.1%) | Septic = 1 |
| Non-septic = 1 | ||
| Uncertain = 0 | ||
| Scapulohumeral joint | 2 (1.1%) | Septic = 1 |
| Non-septic = 1 | ||
| Uncertain = 0 | ||
| Navicular bursa | 2 (1.1%) | Septic = 0 |
| Non-septic = 2 | ||
| Uncertain = 0 | ||
| Calcaneal bursa | 3 (1.7%) | Septic = 2 |
| Non-septic = 1 | ||
| Uncertain = 0 | ||
| Cubital joint | 5 (6.5%) | Septic = 3 |
| Non-septic = 1 | ||
| Uncertain = 1 | ||
| Lateral/medial femorotibial joints | 7 (2.0%) | Septic = 1 |
| Non-septic = 5 | ||
| Uncertain = 1 | ||
| Femoropatellar joint | 10 (5.6%) | Septic = 3 |
| Non-septic = 5 | ||
| Uncertain = 2 | ||
| Distal interphalangeal joint | 16 (9.0%) | Septic = 0 |
| Non-septic = 12 | ||
| Uncertain = 4 | ||
| Digital flexor tendon sheath | 24 (13.6%) | Septic = 7 |
| Non-septic = 15 | ||
| Uncertain = 2 | ||
| Carpal joints (radiocarpal and middle carpal) | 27 (15.3%) | Septic = 5 |
| Non-septic = 19 | ||
| Uncertain = 3 | ||
| Metacarpo- and metatarsophalangeal joints | 31 (17.5%) | Septic = 15 |
| Non-septic = 10 | ||
| Uncertain = 6 | ||
| Tarsocrural joint | 45 (25.4%) | Septic = 9 |
| Non-septic = 28 | ||
| Uncertain = 8 | ||
| Total | 177 (100%) | Septic = 47 |
| Non-septic = 103 | ||
| Uncertain = 27 |
| ROC Curve | Sensitivity (%) | Specificity (%) | Area under the Curve (95% Confidence Interval) | Cutoff Value (µg/L) | p-Value |
|---|---|---|---|---|---|
| Septic versus non-septic | 95.7 | 93.2 | 0.981 (0.945–0.996) | 293.6 | <0.0001 |
| Septic versus uncertain | 87.2 | 75.0 | 0.849 (0.740–0.925) | 444.6 | <0.0001 |
| Uncertain versus non-septic | 88.9 | 69.9 | 0.853 (0.781–0.909) | 52.8 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacobsen, S.; Mortensen, C.D.; Høj, E.A.; Vinther, A.M.; Berg, L.C.; Adler, D.M.T.; Verwilghen, D.; van Galen, G. Neutrophil Gelatinase-Associated Lipocalin in Synovial Fluid from Horses with and without Septic Arthritis. Animals 2023, 13, 29. https://doi.org/10.3390/ani13010029
Jacobsen S, Mortensen CD, Høj EA, Vinther AM, Berg LC, Adler DMT, Verwilghen D, van Galen G. Neutrophil Gelatinase-Associated Lipocalin in Synovial Fluid from Horses with and without Septic Arthritis. Animals. 2023; 13(1):29. https://doi.org/10.3390/ani13010029
Chicago/Turabian StyleJacobsen, Stine, Camilla Drejer Mortensen, Elisabeth Alkærsig Høj, Anne Mette Vinther, Lise Charlotte Berg, Ditte Marie Top Adler, Denis Verwilghen, and Gaby van Galen. 2023. "Neutrophil Gelatinase-Associated Lipocalin in Synovial Fluid from Horses with and without Septic Arthritis" Animals 13, no. 1: 29. https://doi.org/10.3390/ani13010029