
The Potential of Bemegride as an Activation Agent in Electroencephalography in Dogs

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Anesthetic Procedure
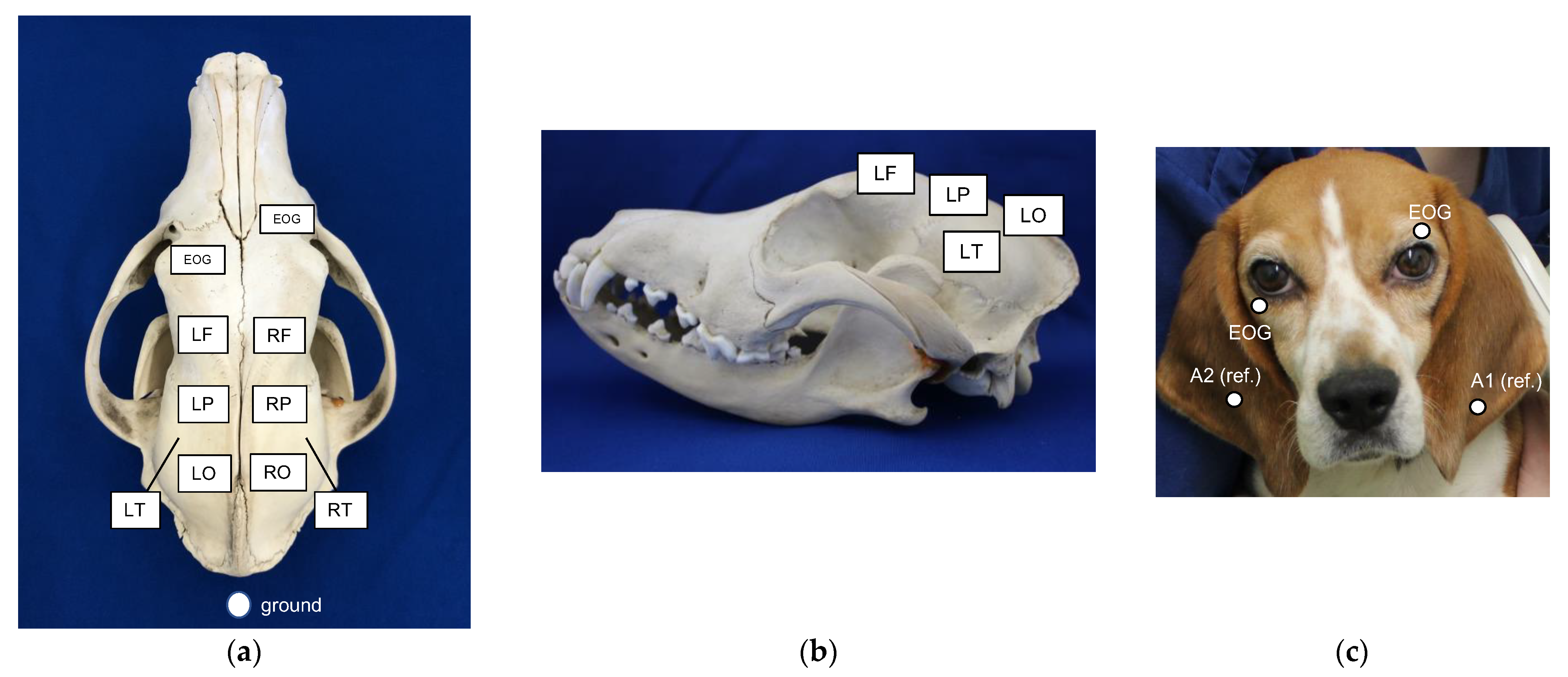
2.3. EEG
2.4. Procedure
2.5. Analyses
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kearsle-Fleet, L.; O’Neill, D.G.; Volk, H.A.; Church, D.B.; Brodbelt, D.C. Prevalence and risk factors for canine epilepsy of unkown origin in the UK. Vet. Rec. 2013, 172, 338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heske, L.; Nodtvedt, A.; Jaderlund, K.; Berendt, M.; Egenvall, A. A cohort study of epilepsy among 665,000 insured dogs: Incidence, mortality and survival after diagnosis. Vet. J. 2014, 202, 471–476. [Google Scholar] [CrossRef] [PubMed]
- De Risio, L.; Bhatti, S.; Muñana, K.; Penderis, J.; Stein, V.; Tipold, A.; Berendt, M.; Farqhuar, R.; Fischer, A.; Long, S.; et al. International veterinary epilepsy task force consensus proposal: Diagnostic approach to epilepsy in dogs. BMC Vet. Res. 2015, 11, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, F.M.K. Electroencephalography. In A Practical Guide to Seizure Disorders in Dogs and Cats; De Risio, L., Muñana, K., Eds.; Edra Publishing: Palm Beach, FL, USA, 2022; pp. 153–181. [Google Scholar]
- Tatum, W.O.; Rubboli, G.; Kaplan, P.W.; Mirsatari, S.M.; Gloss, D.; Caboclo, L.O.; Drislane, F.W.; Koutroumanidis, M.; Schomer, D.L.; Beniczky, S.; et al. Clinical utility of EEG in diagnosing and monitoring epilepsy in adults. Clin. Neurophysiol. 2018, 129, 1056–1082. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, F.; Sica, R. Canine electroencephalographic recording technique: Findings in normal and epileptic dogs. Clin. Neurophylol. 2004, 115, 477–487. [Google Scholar] [CrossRef]
- Brauer, C.; Kästner, S.B.R.; Schenk, H.C.; Tünsmeyer, J.; Tipold, A. Electroencephalographic recordings in dogs: Prevention of muscle artifacts and evaluation of two activation techniques in healthy individuals. Res. Vet. Sci. 2011, 90, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Brauer, C.; Kästner, S.B.R.; Schenk, H.C.; Tünsmeyer, J.; Tipold, A. Electroencephalographic recordings in dogs suffering from idiopathic and symptomatic epilepsy: Diagnostic value of interictal short time EEG protocols supplemented by two activation techniques. Vet. J. 2012, 193, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Wrzosek, M.; Ives, J.R.; Karczewski, M.; Dziadkowiak, E.; Gruszka, E. The relationship between epileptiform discharges and background activity in the visual analysis of electroencephalographic examinations in dogs with seizures of different etiologies. Vet. J. 2017, 222, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Utsugi, S.; Saito, M.; Sato, T.; Kunimi, M. Relationship between interictal epileptiform discharges under medetomidine sedation and clinical seizures in canine idiopathic epilepsy. Vet. Rec. 2020, 187, 67. [Google Scholar] [CrossRef] [PubMed]
- Jaggy, A.; Bernardini, M. Idiopathic epilepsy in 125 dogs: A long-term study. Clinical and electroencephalographic findings. J. Small Anim. Prac. 1998, 39, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Berendt, M.; Hogenhaven, H.; Flagstad, A.; Dam, M. Electroencephalography in dogs with epilepsy: Similarities between human and canine findings. Acta Neuro Scand. 1999, 99, 276–283. [Google Scholar] [CrossRef]
- Jeserevies, J.; Viitmaa, R.; Cizinauskas, S.; Sainio, K.; Jokinen, T.S.; Snellman, M.; Bellino, C.; Bergamasco, L. Electroencephalography findings in healthy and Finnish Spitz dogs with epilepsy: Visual and background quantitative analysis. J. Vet. Intern. Med. 2007, 21, 1299–1306. [Google Scholar] [CrossRef]
- Hughes, J.R. The significance of the interictal spike discharge: A review. J. Clin. Neurophysiol. 1989, 6, 207–226. [Google Scholar] [CrossRef] [PubMed]
- Holliday, T.A.; Cunningham, J.G.; Gutnick, M.J. Comparative clinical and electroencephalographic studies of canine epilepsy. Epilepsia 1970, 11, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Goiz-Marquez, G.; Caballero, S.; Solis, H.; Rodriguez, C.; Sumano, H. Electroencephalographic evaluation of gold wire implants inserted in acupuncture points in dogs with epileptic seizures. Res. Vet. Sci. 2009, 86, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Katagai, H.; Yasui-Fukunori, N.; Kaneko, S. Bemegride lengthens seizure duration during electric convulsive therapy in a schizophrenic patient with increased seizure threshold. J. ECT 2009, 25, 61–63. [Google Scholar] [CrossRef]
- Fröscher, W.; Bülau, P. EEG activation with bemegride in epilepsy diagnosis. 1: Literature review. EEG EMG Elektroenzephalogr. Elektromyogr. Verwandte Geb. 1984, 15, 75–81. [Google Scholar]
- Bingle, J. Bemegride as an activator in electroencephalography. Br. Med. J. 1958, 5076, 923–926. [Google Scholar] [CrossRef]
- Fujita, C.; Karasawa, A.; Endo, S.; Kawajiri, T.; Hasegwa, K.; Takagi, K.; Okuda, Y.; Ohara, K.; Ishikawa, S.; Ishii, S. The critical study on the EEG-activating effects of megimide. Clin. Psychiat. 1960, 2, 533–539. [Google Scholar]
- Rokukawa, J.; Hayakawa, T.; Nakatani, S.; Iwata, Y.; Kobayashi, K. Characteristics of metrazol and megimide for activation of seizure discharges. Brain Nerve 1976, 7, 671–675. [Google Scholar]
- Rodin, E.A.; Rutledge, L.T.; Calhoun, H.D. Megimide and metrazol: A comparison of their convulsant properties in man and cat. Electroencephalogr. Clin. Neurophysiol. 1958, 4, 719–723. [Google Scholar] [CrossRef] [Green Version]
- Rokukawa, J.; Iwata, Y.; Kobayashi, K.; Oku, K. Experimental study of the megimied induced seizure with special reference to the comparison with the metrazol induced siezure. Brain Nerve 1976, 6, 559–563. [Google Scholar]
- Hasegawa, D.; Mizoguchi, S.; Kuwabara, T.; Hamamoto, Y.; Ogawa, F.; Matsuki, N.; Uchida, K.; Fujita, M. Electroencephalographic features of familial spontaneous epileptic cats. Epilepsy Res. 2014, 108, 1018–1025. [Google Scholar] [CrossRef]
- Kobayashi, M.; Oono, S.; Kadono, H. Research about epilepsy in dogs: Activation of abnormal EEG activity by bemegride. J. Vet. Med. 1977, 4, 223–227. [Google Scholar]
- Booth, N.H. Stimulants. In Veterinary Pharmacology and Therapeutics, 5th ed.; Booth, N.H., McDonald, L.E., Eds.; Iowa State University Press: Ames, IA, USA, 1982; p. 348. [Google Scholar]
- Gershon, S.; Shaw, F.H. Effect of bemegride on barbiturate overdosage in humans. Br. Med. J. 1957, 5060, 1509–1514. [Google Scholar] [CrossRef] [PubMed]
- Johanson, J.O.; Järbe, T.U. Diazepam as a discriminative cue: Its antagonism by bemegride. Eur. J. Pharmacol. 1975, 2, 372–375. [Google Scholar] [CrossRef]
- Luders, H.O.; Engel, J., Jr.; Munari, C. General principles. In Surgical Treatment of the Epilepsies, 2nd ed.; Engel, J., Jr., Ed.; Raven Press: New York, NY, USA, 1993; pp. 137–159. [Google Scholar]
- Hasegawa, D. Diagnostic techniques to detect the epileptogenic zone: Pathophysiological and presurgical analysis of epilepsy in dogs and cats. Vet. J. 2016, 215, 64–75. [Google Scholar] [CrossRef] [Green Version]
- Nakai, S.; Saito, S.; Watanabe, S.; Fukai, H. The use of megimide as an activator in electroencephalography. Brain Nerve 1959, 11, 487–494. [Google Scholar]
- Cerda-Gonzalez, S.; Packer, R.A.; Garosi, L.; Lowrie, M.; Mandigers, P.J.J.; O’Brien, D.P.; Volk, H.A. International veterinary canine dyskinesia task force ECVN consensus statement: Terminology and classification. J. Vet. Intern. Med. 2021, 35, 1218–1230. [Google Scholar] [CrossRef]
- Yu, Y.; Hasegawa, D.; Kanazono, S.; Saito, M. Clinical characterization of epileptic seizures in Pomeranians with idiopathic epilepsy or epilepsy of unknown cause. J. Vet. Intern. Med. 2022, 1–10, Online ahead of print. [Google Scholar] [CrossRef]
- Tanaka, S.; Oda, Y.; Ryokai, M.; Uda, T.; Kunihiro, N.; Kuki, I.; Okutani, R. The effect of sevoflurane on electroencephalographic spike activity in pediatric patients with epilepsy. Paediatr Anaesth. 2017, 4, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Iijima, T.; Nakamura, Z.; Iwao, Y.; Sankawa, H. The epileptogenic properties of the volatile anesthetics sevoflurane and isoflurane in patients with epilepsy. Anesth Analg. 2000, 91, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Kunimi, M.; Saito, M.; Fujita, Y.; Mutou, M. Comparation of scalp electroencephalogram between spontaneous epileptic dogs and normal dogs. In Proceedings of the 31st Congress of Japanese Society of Veterinary Neurology, Tokyo, Japan, 14 December 2008; Japanese Society of Veterinary Neurology: Tokyo, Japan, 2008. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dog | Age (Months) | Body Weight (kg) | Sex | Diagnosis | Seizure Frequency (per 3 Months) | Medication |
|---|---|---|---|---|---|---|
| Epilepsy group | ||||||
| Pekinese (Dog 1) | 25 | 3 | Female | IE (Tier I) | 2 | KBr |
| Miniature Dachshund (Dog 2) | 48 | 3.8 | Female | IE (Tier III, necropsy) | 4 | PB, KBr |
| Beagle (Dog 3) | 109 | 12 | Female | IE (Tier I *, necropsy) | 0.5 | None |
| Beagle (Dog 4) | 49 | 49 | Male | IE (Tier I) | 0.25 | None |
| Control group | ||||||
| Beagle (Dog 5) | 60 | 10.45 | Male | |||
| Beagle (Dog 6) | 25 | 9.3 | Female | |||
| Beagle (Dog 7) | 26 | 10.3 | Male | |||
| Beagle (Dog 8) | 60 | 10 | Male |
| Dog | Seizure Type/Semiology | Laterality |
|---|---|---|
| Dog 1 | Focal motor/facial twitching, then repeated jerking head movements, which rapidly progressed to generalized tonic clonic movements | No laterality |
| Dog 2 | Focal motor/facial twitching that rapidly progressed to generalized tonic clonic movements | No laterality |
| Dog 3 | Focal motor/head shaking, followed by clonic movements of the jaw, which rapidly progressed to generalized tonic movements | No laterality |
| Dog 4 | Focal motor/facial twitching that rapidly progressed to generalized tonic clonic movements | No laterality |
| Dog | Region of the Irritative Zone | |
|---|---|---|
| Epilepsy group | Baseline | Activation |
| Dog 1 | Right frontal | Right frontal |
| Dog 2 | Left parietal | Left parietal |
| Dog 3 | None | Left parietal |
| Dog 4 | Left parietal | Left parietal |
| Control group | ||
| Dog 5 | None | None |
| Dog 6 | None | Left parietal |
| Dog 7 | None | None |
| Dog 8 | None | Left parietal |
| Dog | Epileptiform Discharges | |
|---|---|---|
| Epilepsy group | Baseline | Activation |
| Dog 1 | Sharp wave | Spike, sharp wave |
| Dog 2 | Spike | Spike |
| Dog 3 | None | Sharp wave |
| Dog 4 | Sharp wave | Spike, rhythmic spikes |
| Control group | ||
| Dog 5 | None | None |
| Dog 6 | None | Spike |
| Dog 7 | None | None |
| Dog 8 | None | Spike |
| Dog | ED Frequency (per Minute) | p-Value | |
|---|---|---|---|
| Epilepsy group | Baseline | Activation | |
| Dog 1 | 0.2 | 1.6 | |
| Dog 2 | 4.4 | 18.0 | |
| Dog 3 | 0.0 | 1.0 | |
| Dog 4 | 0.1 | 0.4 | |
| 0.125 | |||
| Control group | |||
| Dog 5 | 0.0 | 0.0 | |
| Dog 6 | 0.0 | 0.2 | |
| Dog 7 | 0.0 | 0.0 | |
| Dog 8 | 0.0 | 0.4 | |
| 0.500 | |||
| Dog | Sevoflurane Concentration (%) |
|---|---|
| Epilepsy group | |
| Dog 1 | 3.0 |
| Dog 2 | 3.0 |
| Dog 3 | 3.0 |
| Dog 4 | 3.5 |
| Control group | |
| Dog 5 | 3.5 |
| Dog 6 | 3.0 |
| Dog 7 | 3.5 |
| Dog 8 | 3.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirashima, J.; Saito, M.; Yokomori, M. The Potential of Bemegride as an Activation Agent in Electroencephalography in Dogs. Animals 2022, 12, 3210. https://doi.org/10.3390/ani12223210
Hirashima J, Saito M, Yokomori M. The Potential of Bemegride as an Activation Agent in Electroencephalography in Dogs. Animals. 2022; 12(22):3210. https://doi.org/10.3390/ani12223210
Chicago/Turabian StyleHirashima, Junya, Miyoko Saito, and Minoru Yokomori. 2022. "The Potential of Bemegride as an Activation Agent in Electroencephalography in Dogs" Animals 12, no. 22: 3210. https://doi.org/10.3390/ani12223210