
From Keratoma to Anaplastic Malignant Melanoma in a Horse’s Hoof
 ,
,  , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
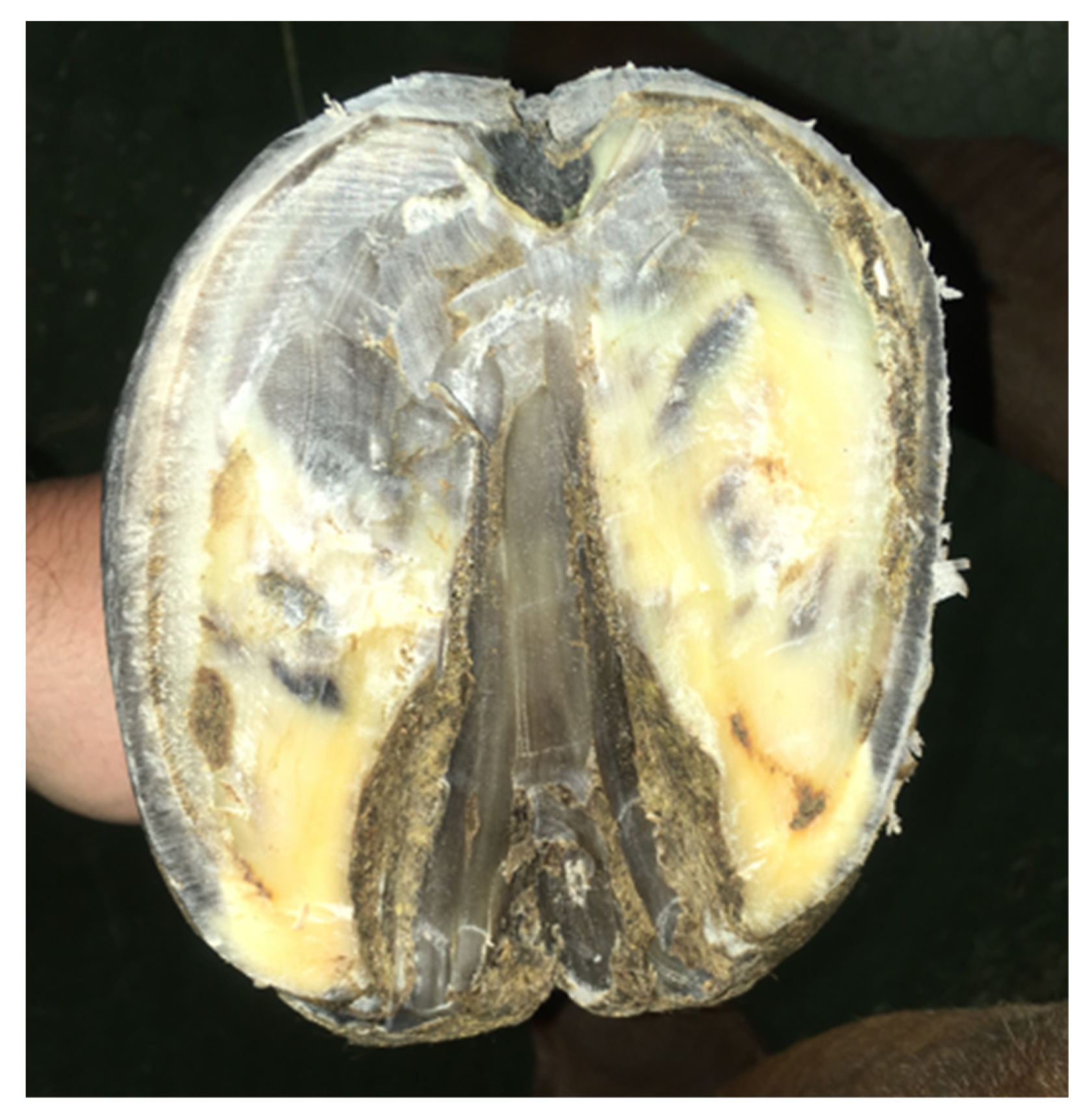
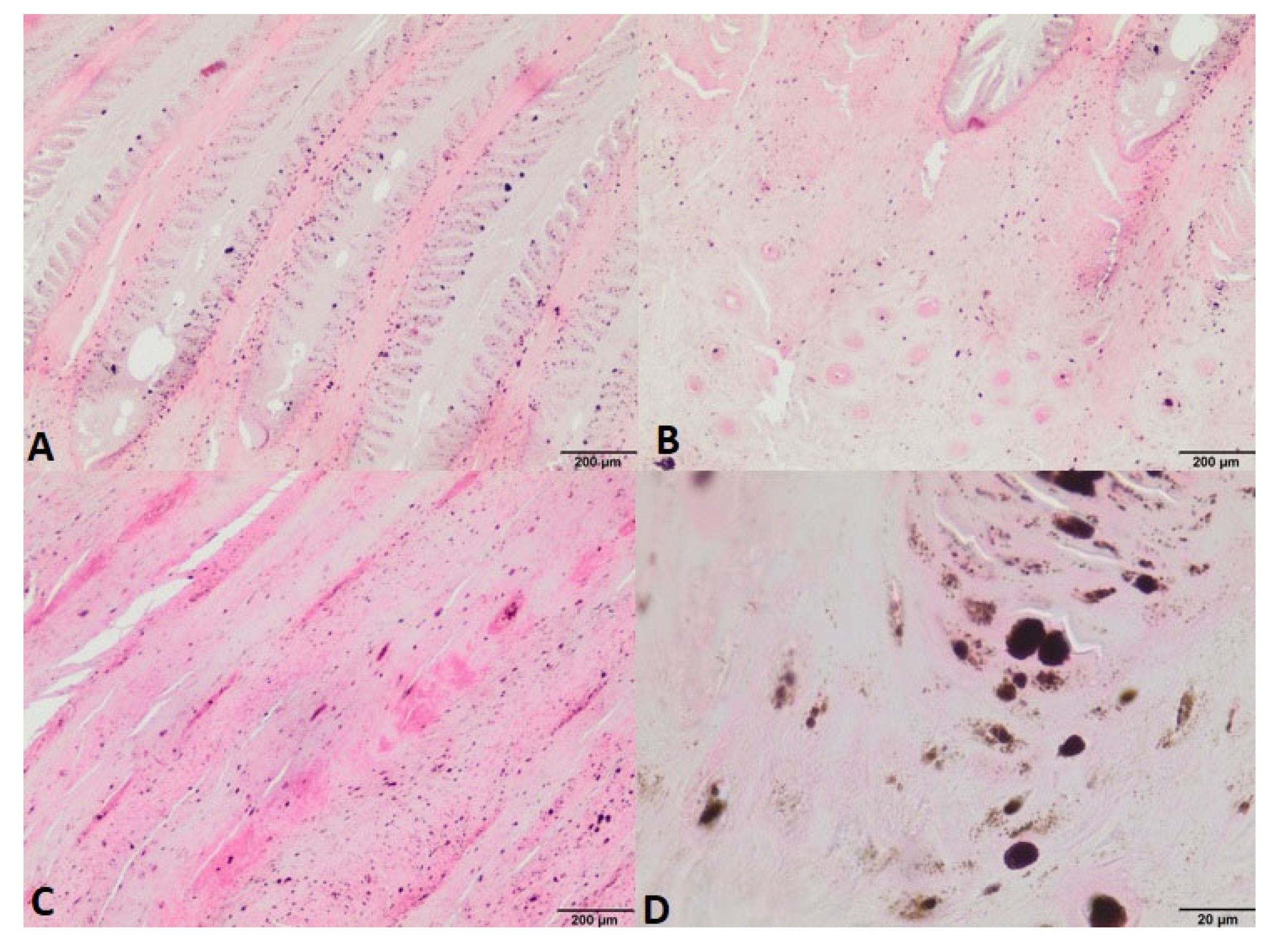
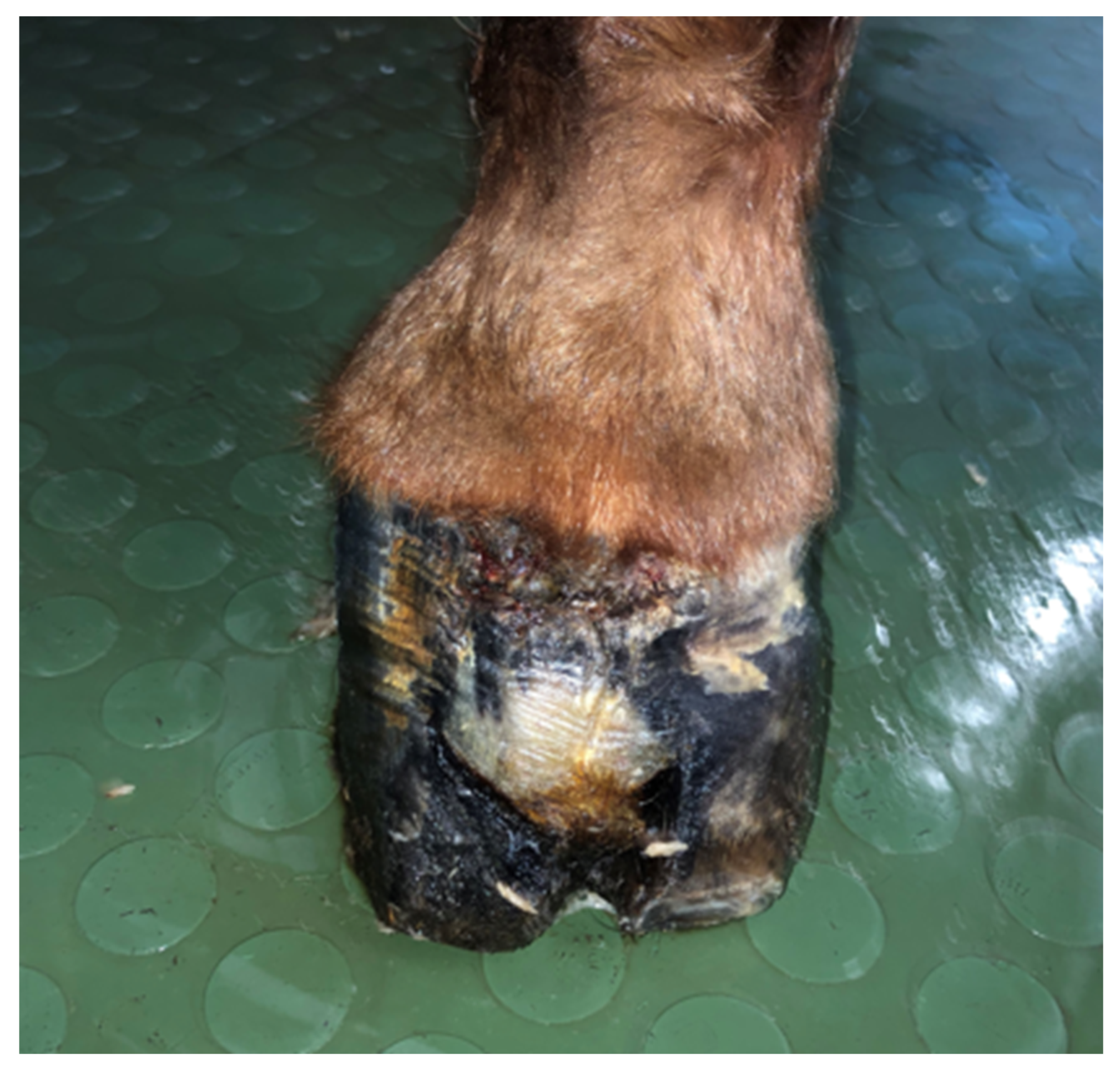
Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valentine, B.A. Equine melanocytic tumors: A retrospective study of 53 horses (1988 to 1991). J. Vet. Intern. Med. 1995, 9, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.C.; Lembcke, L.M. Equine Melanocytic Tumors. Vet. Clin. N. Am.-Equine Pract. 2013, 29, 673–687. [Google Scholar] [CrossRef]
- Kay, G.; McNeil, P.; Knottenbelt, D.; Tligui, N. Locally Invasive Melanoma in the Internal Laminae of the Hoof of a Bay Mule. Equine Veter-Educ. 2020, 32, 66–70. [Google Scholar] [CrossRef]
- Moore, J.S.; Shaw, C.; Shaw, E.; Buechner-Maxwell, V.; Scarratt, W.K.; Crisman, M.; Furr, M.; Robertson, J. Melanoma in Horses: Current Perspectives. Equine Veter-Educ. 2013, 25, 144–151. [Google Scholar] [CrossRef]
- Redding, W.R.; O’Grady, S.E. Nonseptic Diseases Associated with the Hoof Complex. Keratoma, White Line Disease, Canker, and Neoplasia. Vet. Clin. N. Am.-Equine Pract. 2012, 28, 407–421. [Google Scholar] [CrossRef]
- Osborne, C.; Elce, Y.A.; Meehan, L.; Davern, A.J.; Lescun, T.B. Neoplasia within the Equine Foot: A Retrospective Case Series of Four Horses. Equine Vet. Educ. 2022, 34, e431–e437. [Google Scholar] [CrossRef]
- Górski, K.; Berezowski, A.; Turek, B.; Rakowska, A. Keratoma-Rare Cause of Lameness in Horses. Życie Weter. 2017, 92, 282. [Google Scholar]
- Sprayberry, K.A.; Robinson, E.N. Robinson’s Current Therapy in Equine Medicine, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Christman, C. Multiple Keratomas in an Equine Foot. Can. Vet. J. 2008, 49, 904–906. [Google Scholar]
- Berry, C.R.; O’Brien, T.R.; Pool, R.R. Squamous Cell Carcinoma of the Hoof Wall in a Stallion. J. Am. Vet. Med. Assoc. 1991, 199, 90–92. [Google Scholar] [PubMed]
- Spugnini, E.P.; Bolaffio, C.; Scacco, L.; Baldi, A. Isolated Limb Perfusion Electrochemotherapy for the Treatment of an Advanced Squamous Cell Carcinoma of the Hoof in a Mare. Open Vet. J. 2017, 7, 192–196. [Google Scholar] [CrossRef]
- Kunze, D.J.; Monticello, T.M.; Jakob, T.P.; Crane, S. Malignant melanoma of the coronary band in a horse. J. Am. Veter-Med. Assoc. 1986, 188, 297–298. [Google Scholar]
- Honnas, C.M.; Liskey, C.C.; Meagher, D.M.; Brown, D.; Luck, E.E. Malignant melanoma in the foot of a horse. J. Am. Veter-Med. Assoc. 1990, 197, 756–758. [Google Scholar]
- Brounts, S.H.; Adams, S.B.; Vemireddi, V.; Holland, C.H. A Malignant Glomus Tumour in the Foot of a Horse. Equine Vet. Educ. 2008, 20, 24–27. [Google Scholar] [CrossRef]
- Ritmeester, A.M.; Denicola, D.B.; Blevins, W.E.; Christian, J.A. Primary Intraosseous Mast Cell Tumour of the Third Phalanx in a Quarter Horse. Equine Vet. J. 1997, 29, 151–152. [Google Scholar] [CrossRef]
- Hatai, H.; Hatazoe, T.; Seo, H.; Tozaki, T.; Ishikawa, S.; Miyoshi, N.; Misumi, K.; Hobo, S. Primary Sinonasal Malignant Melanoma with Systemic Metastasis in a Non-Gray Horse. J. Vet. Diagn. Investig. 2021, 33, 379–383. [Google Scholar] [CrossRef]
- McFadyean, J. Equine Melanomatosis. J. Comp. Pathol. Ther. 1933, 46, 186–204. [Google Scholar] [CrossRef]
- Kato, T.; Suetake, T.; Sugiyama, Y.; Tabata, N.; Tagami, H. Epidemiology and Prognosis of Subungual Melanoma in 34 Japanese Patients. Br. J. Dermatol. 1996, 134, 383–387. [Google Scholar] [CrossRef]
- Haneke, E. Ungual Melanoma-Controversies in Diagnosis and Treatment. Dermatol. Ther. 2012, 25, 510–524. [Google Scholar] [CrossRef]
- Blessing, K.; Kernohan, N.M.; Park, K.G.M. Subungual Malignant Melanoma: Clinicopathological Features of 100 Cases Subungual Malignant Melanoma: Clinicopathologicat Features of 100 Cases. Histopathology 1991, 19, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.R.; Arbache, S.T.; Quaresma, M.V.; Nico, M.M.S.; Gabbi, T.V.B. Nail Apparatus Melanoma: Experience of 10 Years in a Single Institution. Ski. Appendage Disord. 2018, 5, 20–26. [Google Scholar] [CrossRef]
- Fanti, P.A.; Dika, E.; Misciali, C.; Vaccari, S.; Barisani, A.; Piraccini, B.M.; Cavrin, G.; Maibach, H.I.; Patrizi, A. Nail Apparatus Melanoma: Is Trauma a Coincidence? Is This Peculiar Tumor a Real Acral Melanoma? Cutan. Ocul. Toxicol. 2013, 32, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A. The Inflammation—Cancer Connection. FEBS J. 2018, 285, 638–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bormann, G.; Marsch, W.C.; Haerting, J.; Helmbold, P. Concomitant Traumas Influence Prognosis in Melanomas of the Nail Apparatus. Br. J. Dermatol. 2006, 155, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Stern, D.K.; Creasey, A.A.; Quijije, J.; Lebwohl, M.G. UV-A and UV-B Penetration of Normal Human Cadaveric Fingernail Plate. Arch. Derm. 2011, 147, 439–441. [Google Scholar] [CrossRef] [PubMed]













Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanik, E.; Górski, K.; Turek, B.; Drewnowska-Szczepakowska, O.; Kliczkowska-Klarowicz, K.; Stefanik, A. From Keratoma to Anaplastic Malignant Melanoma in a Horse’s Hoof. Animals 2022, 12, 3090. https://doi.org/10.3390/ani12223090
Stefanik E, Górski K, Turek B, Drewnowska-Szczepakowska O, Kliczkowska-Klarowicz K, Stefanik A. From Keratoma to Anaplastic Malignant Melanoma in a Horse’s Hoof. Animals. 2022; 12(22):3090. https://doi.org/10.3390/ani12223090
Chicago/Turabian StyleStefanik, Elżbieta, Kamil Górski, Bernard Turek, Olga Drewnowska-Szczepakowska, Katarzyna Kliczkowska-Klarowicz, and Aleksandra Stefanik. 2022. "From Keratoma to Anaplastic Malignant Melanoma in a Horse’s Hoof" Animals 12, no. 22: 3090. https://doi.org/10.3390/ani12223090