
Reactivation of a Hospital-Based Therapy Dog Visitation Program during the COVID-19 Pandemic


Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Barriers to Program Reactivation
1.2. Animal Welfare during Reactivation
1.3. Purpose of Current Study
2. Materials and Methods
2.1. Therapy Dog/Handler Teams
Handler and Therapy Dog Characteristics
2.2. Measures
2.2.1. Participant Role
2.2.2. Observed Gender
2.2.3. Total Visit Time
2.2.4. Time Spent in Volunteer Services (VS)
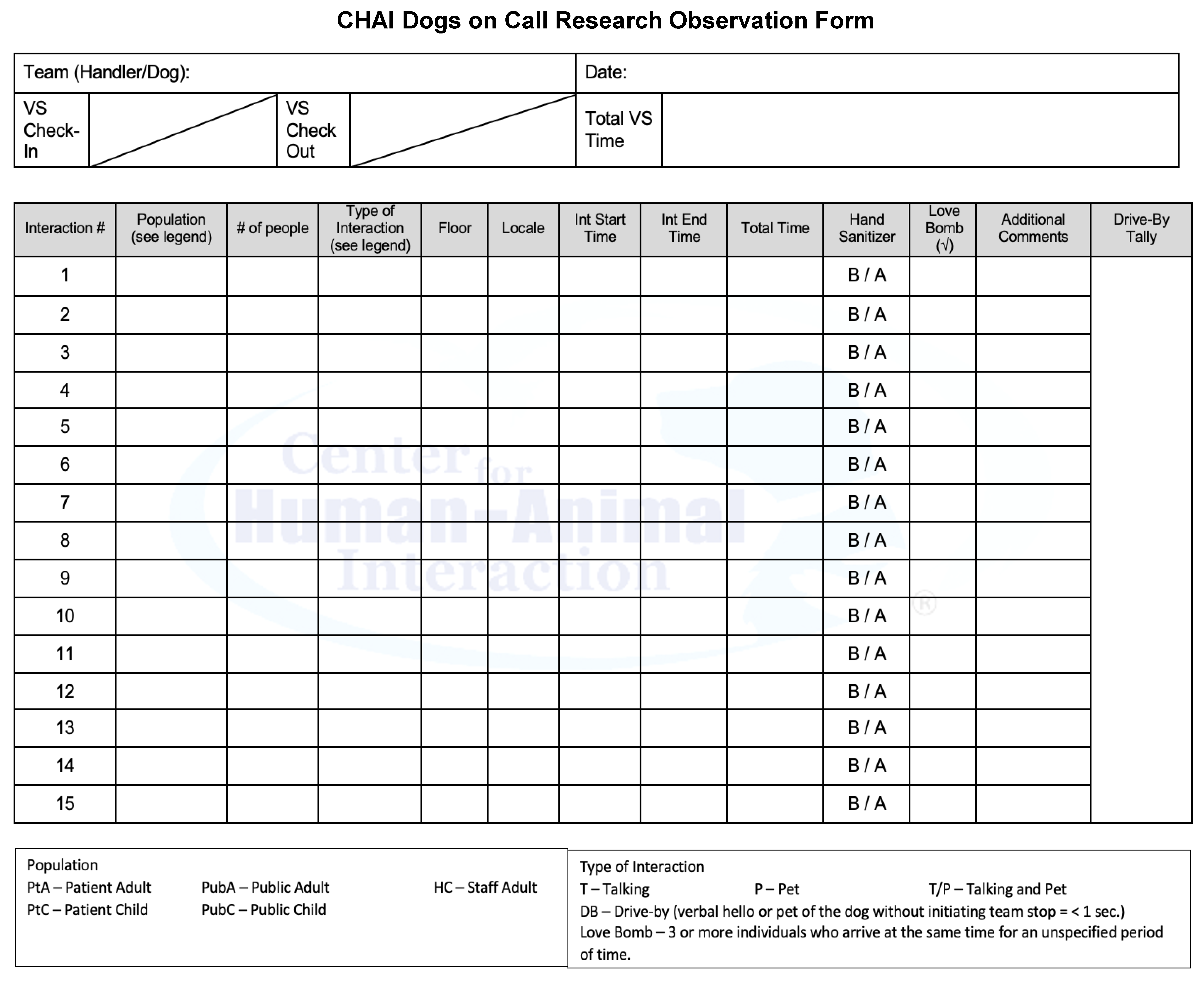
2.2.5. Interaction Characteristics
2.2.6. “Love Bombing”
2.2.7. Floor
2.2.8. Location
2.2.9. Hand Sanitizer Use
2.2.10. “Drive-Bys”
2.3. Procedure
2.3.1. Data Collection
2.3.2. Study Design
2.3.3. Data Analysis
3. Results
3.1. Handler and Dog Characteristics
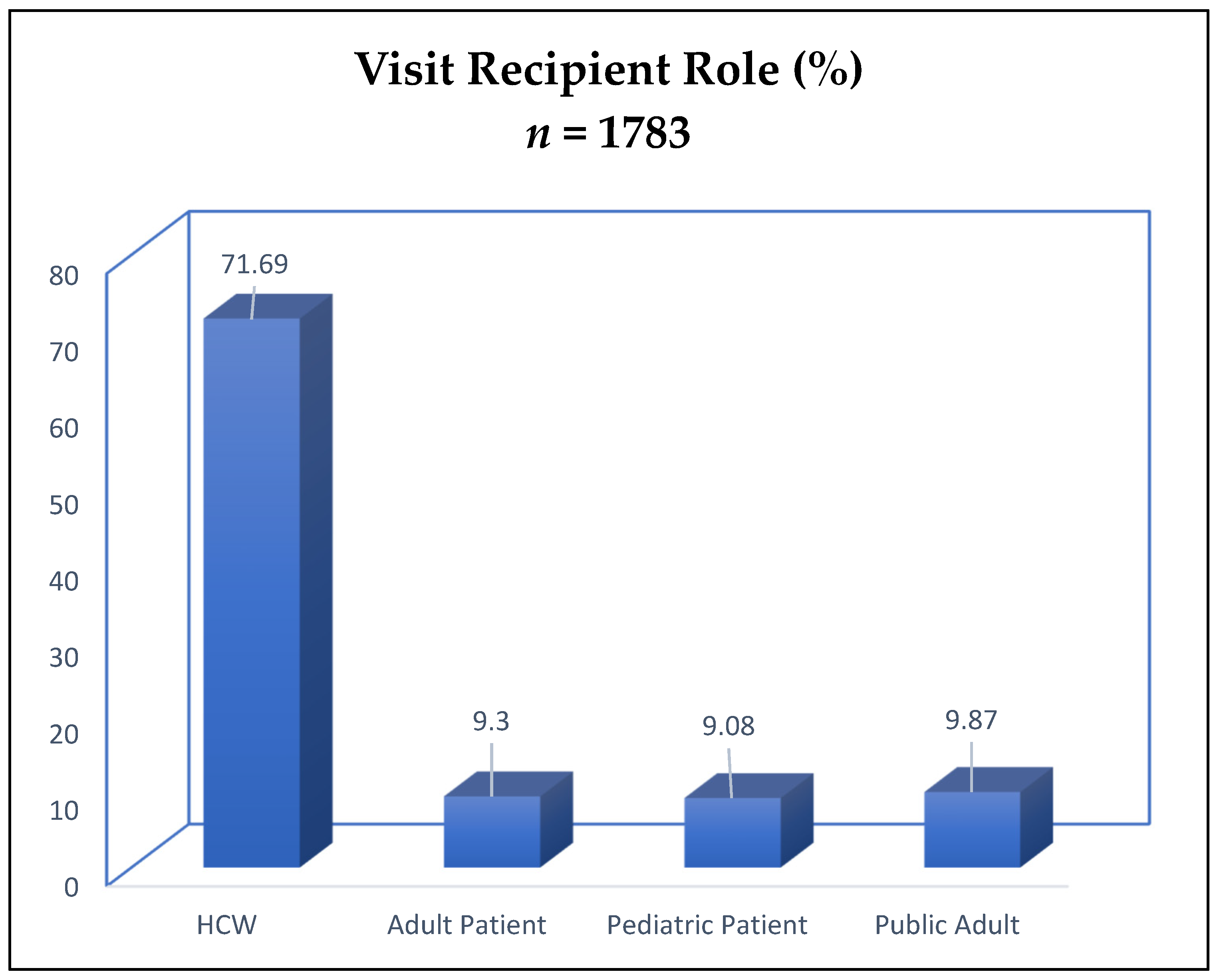
3.2. Participant Role and Observed Gender
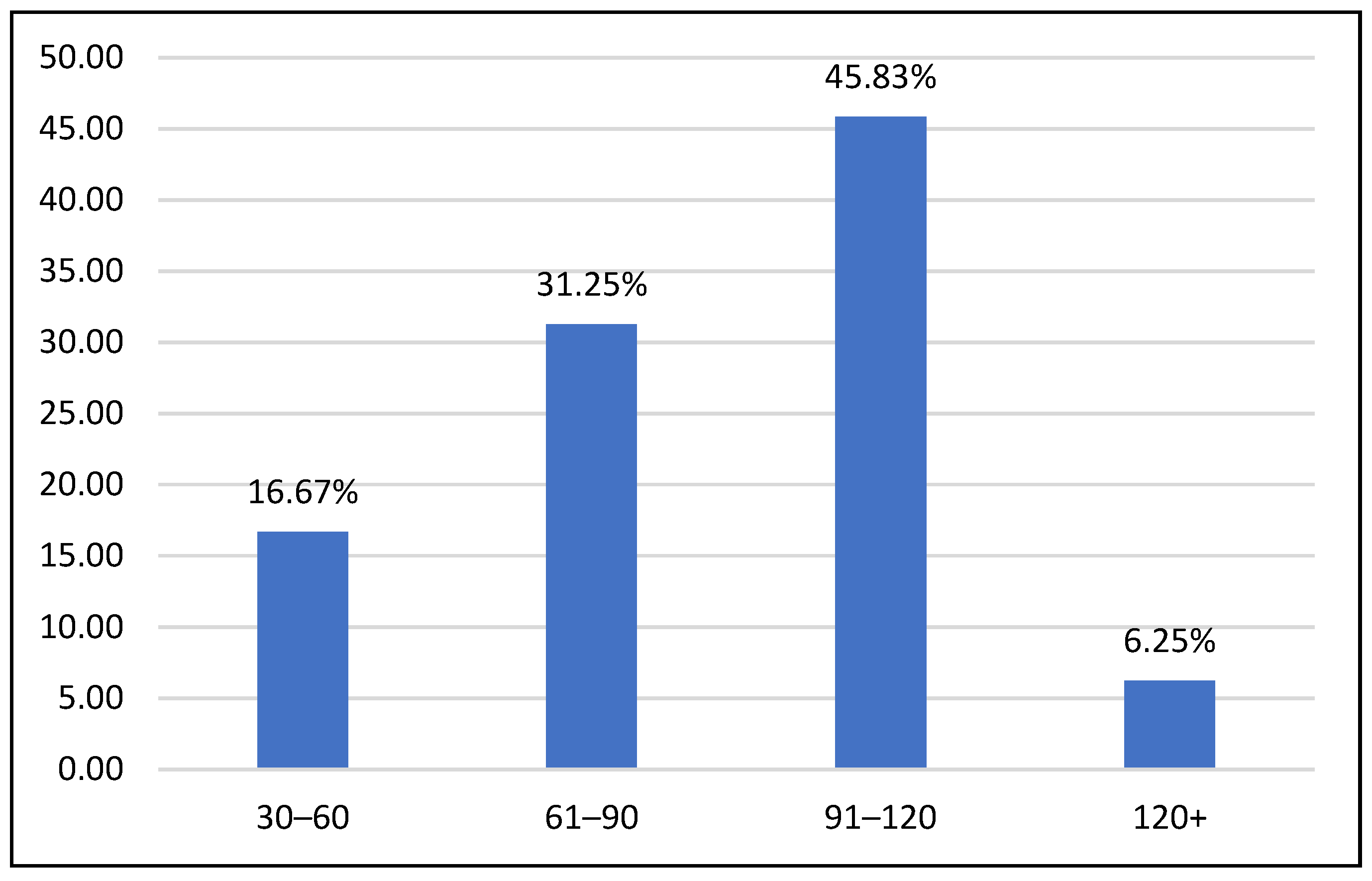
3.3. Total Visit Time
3.4. Interaction Characteristics
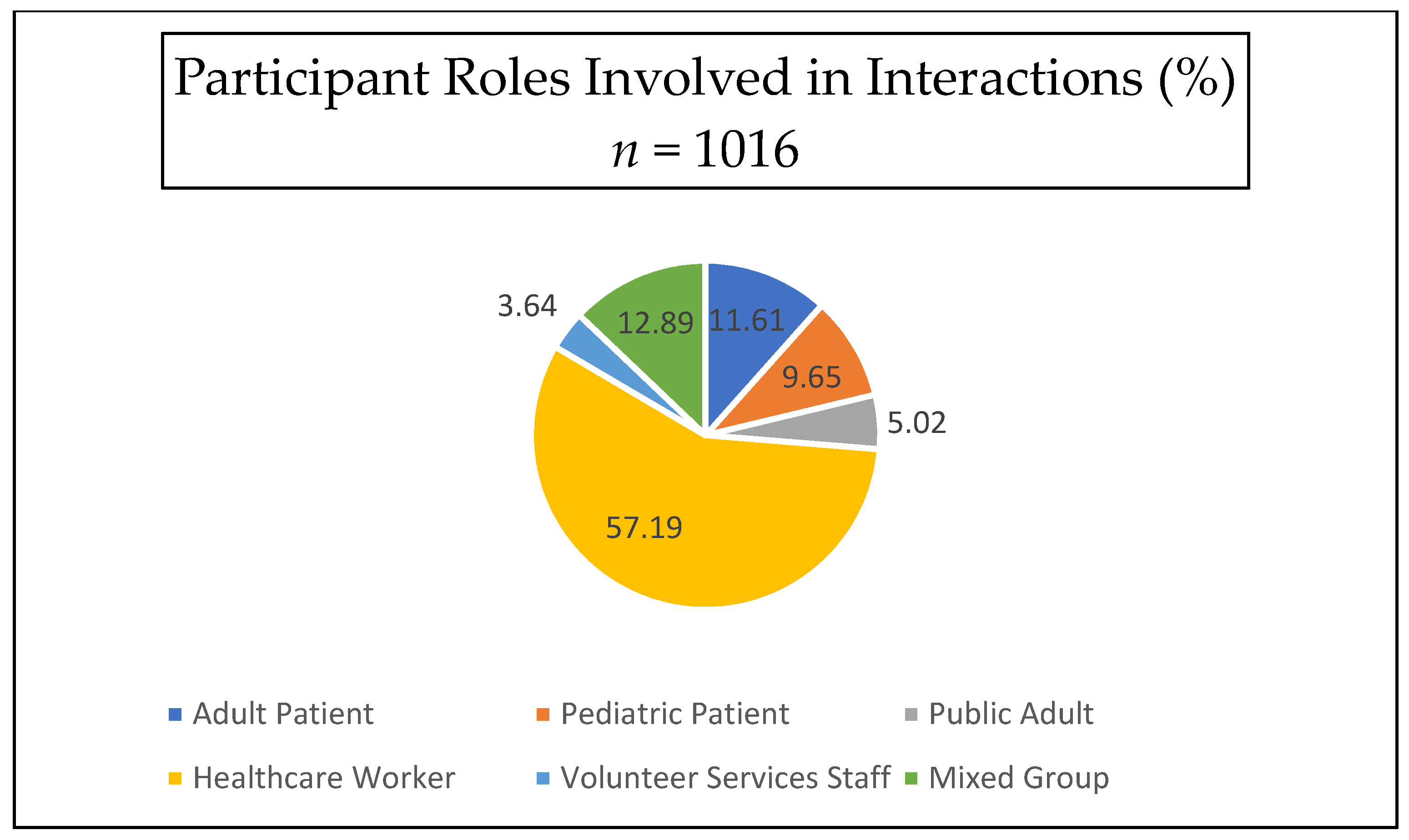
3.4.1. Interaction Type
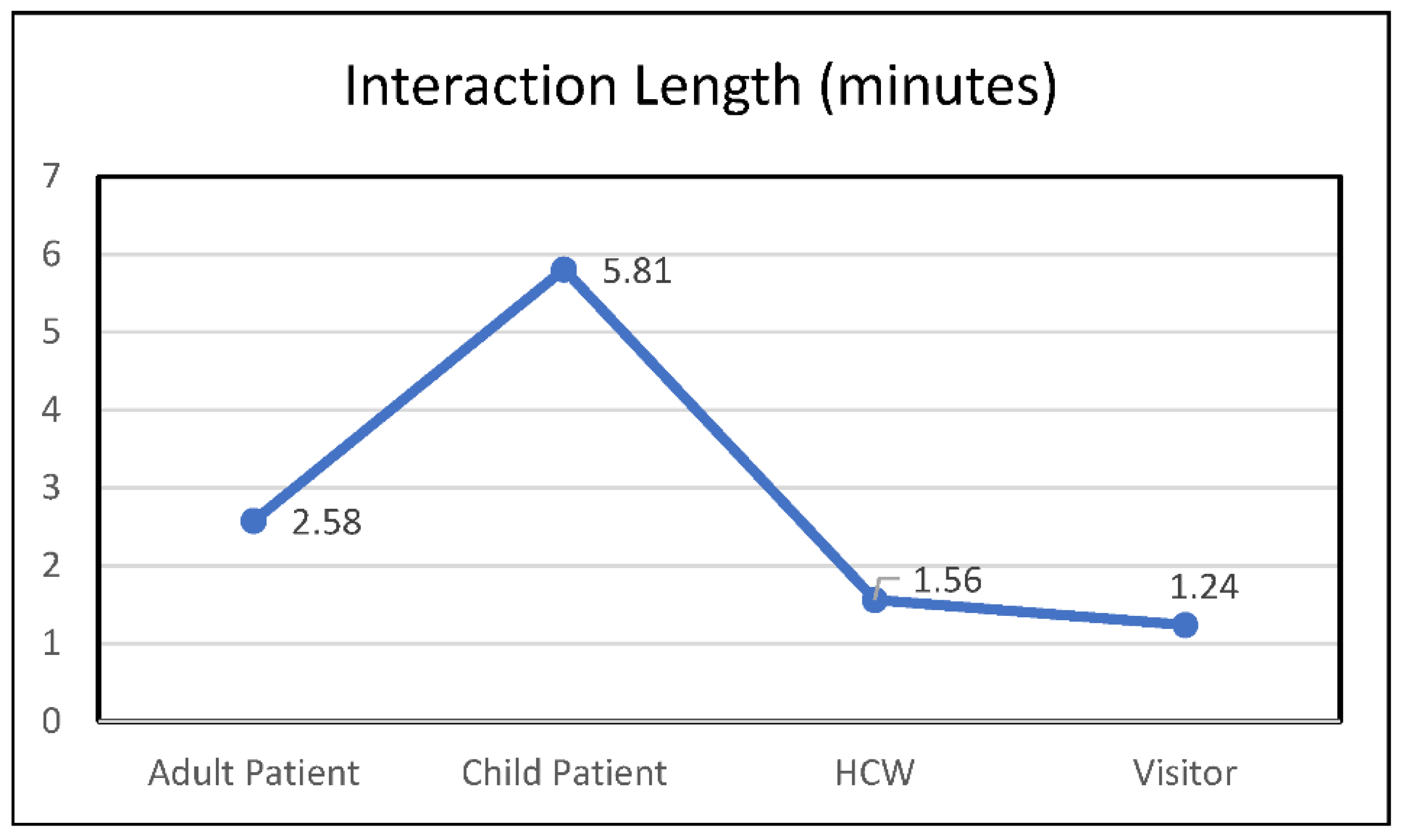
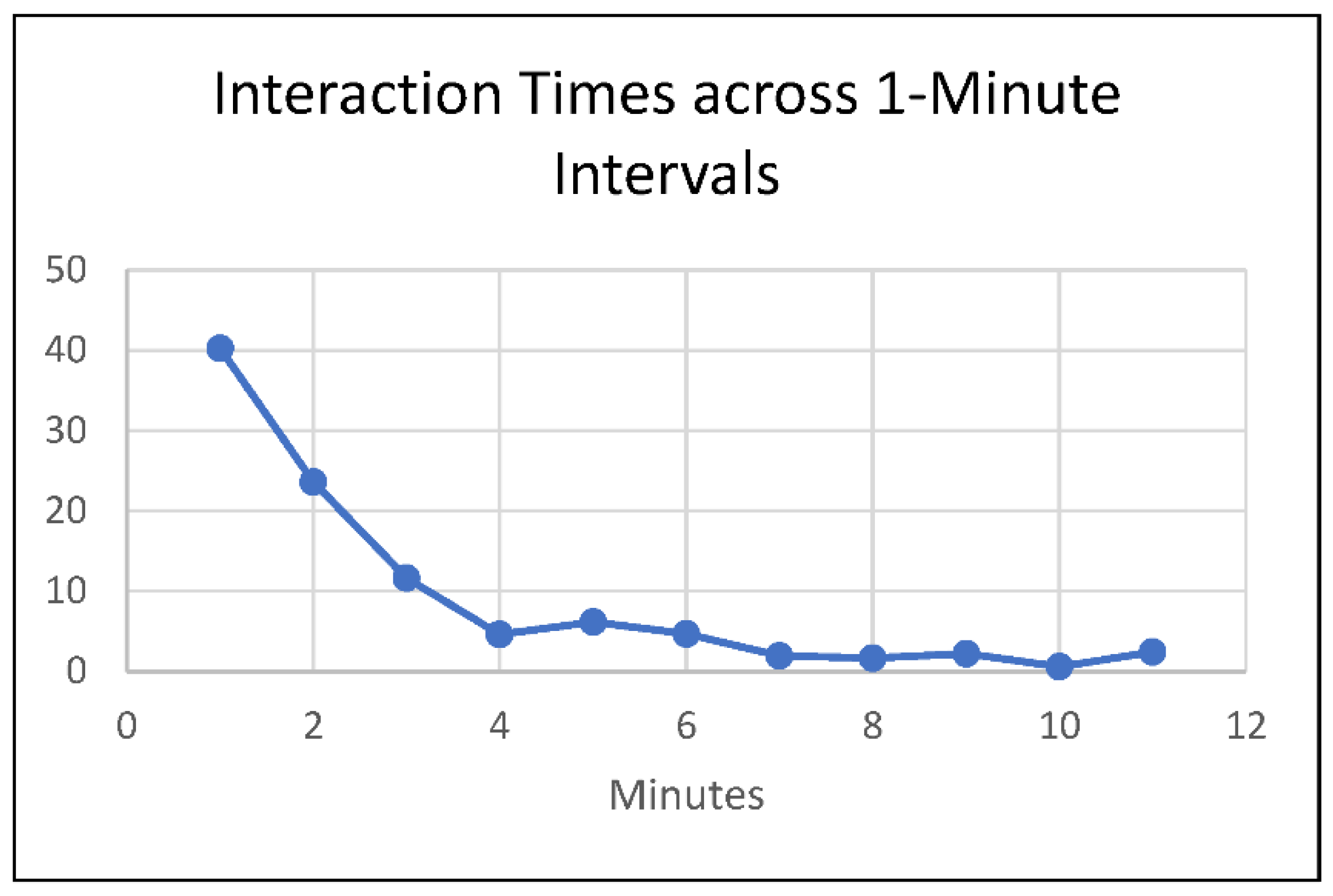
3.4.2. Interaction Time
3.4.3. Number of People per Interaction
3.5. Love Bombing
3.6. Floors
3.7. Location
3.8. Hand Sanitizer Use
3.9. Drive-Bys
4. Discussion
4.1. Program Impact on Visit Recipients
4.2. Strategies for Maintaining Human and Animal Welfare
4.3. Challenges during Program Reactivation
4.4. Visit Recipient Characteristics
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Chahraoui, K.; Laurent, A.; Bioy, A.; Quenot, J.P. Psychological experience of patients 3 months after a stay in the intensive care unit: A descriptive and qualitative study. J. Crit. Care 2015, 30, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Eakin, M.N.; Patel, Y.; Mendez-Tellez, P.; Dinglas, V.D.; Needham, D.M.; Turnbull, A.E. Patients’ outcomes after acute respiratory failure: A qualitative study with the PROMIS framework. Am. J. Crit. Care 2017, 26, 456–465. [Google Scholar] [CrossRef]
- Hosey, M.M.; Jaskulski, J.; Wegener, S.T.; Chlan, L.L.; Needham, D.M. Animal-assisted intervention in the ICU: A tool for humanization. Crit. Care 2018, 22, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, S.B.; Gee, N.R. Canine-Assisted Interventions in Hospitals: Best Practices for Maximizing Human and Canine Safety. Front. Vet. Sci. 2021, 8, 615–730. [Google Scholar] [CrossRef]
- Perkins, A. The benefits of pet therapy. Nurs. Made Incred. Easy 2020, 18, 5–8. [Google Scholar] [CrossRef]
- Carey, B.; Dell, C.A.; Stempien, J.; Tupper, S.; Rohr, B.; Carr, E.; Cruz, M.; Acoose, S.; Butt, P.; Broberg, L.; et al. Outcomes of a controlled trial with visiting therapy dog teams on pain in adults in an emergency department. PLoS ONE 2022, 17, e0262599. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.; Shykoff, B.E.; Izzo, J.L. Pet ownership, but not ACE inhibitor therapy, blunts home blood pressure responses to mental stress. Hypertension 2001, 38, 815–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiloh, S.; Sorek, G.; Terkel, J. Reduction of state-anxiety by petting animals in a controlled laboratory experiment. Anxiety Stress Coping 2003, 16, 387–395. [Google Scholar] [CrossRef]
- Barker, S.B.; Dawson, K.S. The effects of animal-assisted therapy on anxiety ratings of hospitalized psychiatric patients. Psychiatr Serv. 1998, 49, 797–801. [Google Scholar] [CrossRef]
- McCullough, A.; Ruehrdanz, A.; Jenkins, M.A. HABRI Central Briefs: The Use of Dogs in Hospital Settings. Available online: https://habricentral.org/resources/54871/download/hc_brief_dogsinhospitals20160115Access.pdf. (accessed on 4 June 2022).
- Jensen, C.L.; Bibbo, J.; Rodriguez, K.E.; O’Haire, M.E. The effects of facility dogs on burnout, job-related well-being, and mental health in paediatric hospital professionals. J. Clin. Nurs. 2021, 30, 1429–1441. [Google Scholar] [CrossRef]
- Graystone, R. Prevent compassion fatigue and burnout with a magnet culture. J. Nurs. Adm. 2019, 49, 231–233. [Google Scholar] [CrossRef] [PubMed]
- Bragard, I.; Dupuis, G.; Fleet, R. Quality of work life, burnout, and stress in emergency department physicians: A qualitative review. Eur. J. Emerg. Med. 2015, 22, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Takayesu, J.K.; Ramoska, E.A.; Clark, T.R.; Hansoti, B.; Dougherty, J.; Freeman, W.; Weaver, K.R.; Chang, Y.; Gross, E. Factors associated with burnout during emergency medicine residency. Acad. Emerg. Med. 2014, 21, 1031–1035. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch. Intern. Med. 2012, 172, 1377–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cross, L.A. Compassion fatigue in palliative care nursing: A concept analysis. J. Hosp. Palliat. Nurs. 2019, 21, 21–28. [Google Scholar] [CrossRef]
- Feinstein, R.E.; Kotara, S.; Jones, B.; Shanor, D.; Nemeroff, C.B. A health care workers mental health crisis line in the age of COVID-19. Depress. Anxiety 2020, 37, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. The effects of social support on sleep quality of medical staff treating patients with Coronavirus Disease 2019 (COVID-19) in January and February 2020 in China. Med. Sci. Monit. 2020, 26, e923549-1–e923549-8. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The mental health impact of the COVID-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Mortier, P.; Vilagut, G.; Ferrer, M.; Serra, C.; Molina, J.D.; Lopez-Fresnena, N.; Puig, T.; Pelayo-Teran, J.M.; Pijoan, J.I.; Emparanza, J.I.; et al. Thirty-day suicidal thoughts and behaviors among hospital workers during the first wave of the spain COVID-19 outbreak. Depress. Anxiety 2021, 38, 528–544. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Jahan, I.; Ullah, I.; Griffiths, M.D.; Mamun, M.A. Covid-19 suicide and its causative factors among the healthcare professionals: Case study evidence from press reports. Perspect. Psychiatr. Care 2021, 57, 1707–1711. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.; Xiz, G.; Pang, P.; Wu, B.; Jiang, W.; Li, Y.T.; Wang, M.; Ling, Q.; Chang, X.; Wang, J.; et al. COVID-19 epidemic peer support and crisis intervention via social media. Community Ment. Health J. 2020, 56, 786–792. [Google Scholar] [CrossRef]
- Yuan, K.; Gong, Y.M.; Liu, L.; Sun, Y.K.; Tian, S.S.; Wang, Y.J.; Zhong, Y.; Zhang, A.Y.; Su, S.Z.; Liu, X.X.; et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: A meta-analysis and systematic review. Mol. Psychiatry 2021, 26, 4982–4998. [Google Scholar] [CrossRef] [PubMed]
- Barker, S.B.; Knisely, J.S.; McCain, N.L.; Best, A.M. Measuring stress and immune response in healthcare professionals following interaction with a therapy dog: Pilot study. Psychol. Rep. 2005, 96, 713–729. [Google Scholar] [CrossRef] [PubMed]
- Kline, J.A.; Van Ryzin, K.; Davis, J.C.; Parra, J.A.; Todd, M.L.; Shaw, L.L.; Haggard, B.R.; Fisher, M.A.; Petit, K.L.; Beck, A.M. Randomized trial of therapy Dogs Versus deliberative Coloring (Art therapy) to reduce stress in emergency Medicine Providers. Acad. Emerg. Med. 2020, 27, 266–275. [Google Scholar] [CrossRef]
- Acquadro Maran, D.; Capitanelli, I.; Cortese, C.G.; Ilesanmi, O.S.; Gianino, M.M.; Chirico, F. Animal-Assisted Intervention and Health Care Workers’ Psychological Health: A Systematic Review of the Literature. Animals 2022, 12, 383. [Google Scholar] [CrossRef]
- Dell, C.; Williamson, L.; McKenzie, H.; Carey, B.; Cruz, M.; Gibson, M.; Pavelich, A. A commentary about lessons learned: Transitioning a therapy dog program online during the COVID-19 pandemic. Animals 2021, 11, 914. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Animals and COVID-19. 5 October 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/animals.html (accessed on 5 June 2022).
- Bert, F.; Gualano, M.R.; Camussi, E.; Pieve, G.; Voglino, G.; Siliquini, R. Animal Assisted Intervention: A systematic review of benefits and risks. Eur. J. Integr. Med. 2016, 8, 695–706. [Google Scholar] [CrossRef] [Green Version]
- Chur-Hansen, A.; McArthur, M.; Winefield, H.; Hanieh, E.; Hazel, S. Animal-assisted interventions in children’s hospitals: A critical review of the literature. Anthrozoös 2014, 27, 5–18. [Google Scholar] [CrossRef]
- American Veterinary Medical Association. Animal Assisted Interventions: Guidelines. Available online: https://www.avma.org/resources-tools/avma-policies/animal-assisted-interventions-guidelines (accessed on 5 June 2022).
- Murthy, R.; Bearman, G.; Brown, S.; Bryant, K.; Chinn, R.; Hewlett, A.; Glenn George, B.; Goldstein, E.J.C.; Holzmann-Pazgal, G.; Rupp, M.E.; et al. Animals in healthcare facilities: Recommendations to minimize potential risks. Infect. Control. Hosp. Epidemiol. 2015, 36, 495–516. [Google Scholar] [CrossRef] [Green Version]
- Agresti, A. Categorical Data Analysis, 2nd ed.; Wiley: New York, NY, USA, 2002; p. 81. [Google Scholar]
- Viswanathan, R.; Myers, M.F.; Fanous, A.H. Support groups and individual mental health care via video conferencing for frontline clinicians during the COVID-19 pandemic. Psychosom. J. Consult. Liaison Psychiatry 2020, 61, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.; Cervoni, C.; Lochner, M.; Marangio, J.; Stanley, C.; Marriott, S. Supporting health care workers during the COVID-19 pandemic: Mental health support initiatives and lessons learned from an academic medical center. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S168–S170. [Google Scholar] [CrossRef] [PubMed]
- Landa-Ramírez, E.; Domínguez-Vieyra, N.A.; Hernández-Nuñez, M.E.; Díaz-Vásquez, L.P.; Santana-García, I.A. Psychological support during COVID-19 death notifications: Clinical experiences from a hospital in Mexico. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 518–520. [Google Scholar] [CrossRef] [PubMed]
- Putrino, D.; Ripp, J.; Herrera, J.E.; Cortes, M.; Kellner, C.; Rizk, D.; Dams-O’Connor, K. Multisensory, nature-inspired recharge rooms yield short-term reductions in perceived stress among frontline healthcare workers. Front. Psychol 2020, 11, 560833. [Google Scholar] [CrossRef] [PubMed]
- Nepps, P.; Stewart, C.N.; Bruckno, S.R. Animal-Assisted Activity: Effects of a Complementary Intervention Program on Psychological and Physiological Variables. J. Evid. Based Complementary Altern. Med. 2014, 19, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Gagnon, J.; Bouchard, F.; Landry, M.; Belles-Isles, M.; Fortier, M.; Fillion, L. Implementing a hospital-based animal therapy program for children with cancer: A descriptive study. Can. Oncol. Nurs. J. 2004, 14, 217–222. [Google Scholar] [CrossRef]
- Abate, S.V.; Zucconi, M.; Boxer, B.A. Impact of canine-assisted ambulation on hospitalized chronic heart failure patients’ ambulation outcomes and satisfaction: A pilot study. J. Cardiovasc. Nurs. 2011, 26, 224–230. [Google Scholar] [CrossRef]
- Centers for Disease Control. Weekly Counts of Deaths by Age Group. Available online: https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm (accessed on 5 May 2022).
- Pet Partners. Pet Partners Brief Information. Available online: https://petpartners.org/wp-content/uploads/2019/12/PP_Info-General-Information-w-terms.pdf (accessed on 7 May 2022).
- Smiley, R.A.; Ruttinger, C.; Oliveira, C.M.; Hudson, L.R.; Allgeyer, R.; Reneau, K.A.; Silvestre, J.H.; Alexander, M. The 2020 National Nursing Workforce Survey. J. Nurs. Regul. 2021, 12, S1–S96. [Google Scholar] [CrossRef]
- Ruiz, M.A.; Gibson, C.A.M. Emotional impact of the COVID-19 pandemic on U.S. health care workers: A gathering storm. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S153–S155. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-COVID-19 | Additions during COVID-19 | |
|---|---|---|
| Handler | Varicella (vaccine or titer) | COVID-19 vaccine |
| MMR (measles, mumps, rubella) (vaccine or titer) | COVID-19 booster | |
| Annual flu vaccine | Level 3 face mask | |
| Tuberculosis screening | Face shield or goggles | |
| Temperature measurement and respiratory symptom checklist upon hospital entry | ||
| Dog | Registration with Pet Partners or Alliance of Therapy Dogs w/Canine Good Citizen Test | Reactivation shadowing |
| Annual veterinary exam | Canine stress evaluation by program staff | |
| Vaccine or titer for: rabies, distemper, and parvovirus | Three one-hour reactivation visits for reacclimation | |
| Negative annual fecal exam | ||
| Two-hour visit limit | ||
| Visit Protocol | Hand sanitizer before/after touching dog | No entry into COVID+ (“Hot”) zones |
| Contact tracing | Remain at home if exposed to COVID-19 virus or experiencing respiratory symptoms |
| Common Areas | Areas which all persons in the hospital (staff, visitors, volunteers, etc.) are free to use (with the exception of food service areas where teams do not visit) |
| Inpatient/Inpatient Support | Floors that provide general medical care and an array of services such as respiratory therapy, trauma treatment, cardiac care, orthopedics, intensive care, etc. |
| Pediatric | Floors that specialize in the treatment of pediatric patients including the Children’s Hospital of Richmond |
| ICU | Floors that specialize in the treatment of patients with critical illness or injury |
| Volunteer Services | Volunteer service office where Dogs on Call teams sign in and out before and after hospital visits |
| Gateway | The Gateway Building serves as VCU Medical Center’s “front door” and houses some of its outpatient services. Check-in and waiting areas for surgical services are located on the 5th floor of this building |
| Emergency Department | Department that provides immediate treatment for life threatening or time-sensitive health concerns |
| Nelson Clinic | Various outpatient services such as OB/GYN & Women’s Health, Outpatient Eye Clinic, and dental care are housed here |
| West Hospital | West Hospital houses clinical, administrative, and support services for VCU Medical Center, as well as academic and administrative offices of VCU’s School of Medicine and College of Health Professions |
| Psychiatric, Palliative Care | These departments share the same floor. Psychiatry treats those suffering from mental illness. Palliative care refers to end-of-life treatment |
| Dog | Age (Years) | Sex | Breed | Height (cm) | Weight (kg) |
|---|---|---|---|---|---|
| 1 | - | Female | Labradoodle | - | - |
| 2 | 4 | Female | Golden Retriever | 71.12 | 27.22 |
| 3 | 10 | Male | Mixed Breed (Large Terrier/Wolfhound) | 78.74 | 27.22 |
| 4 | 11 | Male | English Cream Golden Retriever | 71.12 | 26.76 |
| 5 | 3 | Male | English Cream Golden Retriever | 71.12 | 29.94 |
| 6 | 9 | Female | Leonberger | 88.90 | 41.73 |
| 7 | 4 | Male | Mixed Breed (Terrier x) | 30.48 | 7.26 |
| 8 | 13 | Male | Irish Setter | 66.04 | 29.48 |
| 9 | 9 | Female | Irish Setter | 68.58 | 29.48 |
| 10 | 10 | Female | Pembroke Welsh Corgi | 38.10 | 11.34 |
| 11 | 12 | Male | Mixed Breed (Lab/Pug/Boxer) | 60.96 | 21.77 |
| 12 | 7 | Female | Golden Doodle | 76.20 | 27.22 |
| 13 | 8 | Male | Shih Tzu | 38.10 | 8.16 |
| 14 | 7 | Male | Miniature Schnauzer | 35.56 | 3.40 |
| 15 | 13 | Female | Jack Russell Terrier | 30.48 | 7.26 |
| 16 | 5 | Female | English Cream Golden Retriever | 71.12 | 29.48 |
| 17 | - | Female | Chocolate Labrador Retriever | - | - |
| 18 | 8 | Male | Standard Wire Hair Dachshund | 40.64 | 12.70 |
| 19 | 10 | Female | Maltipoo | 25.40 | 2.27 |
| 20 | 2 | Male | English Cream Golden Retriever | 91.44 | 32.66 |
| Floor | Interaction Frequency (n, %) | Pearson’s Residuals |
|---|---|---|
| Common Areas | 123, 12.64 | −3.08 * |
| Inpatient/Inpatient Support | 286, 29.39 | 9.72 * |
| Pediatric Inpatient | 235, 24.15 | 5.72 * |
| Critical Care | 254, 26.10 | 7.21 * |
| Non-emergency Outpatient | 27, 2.77 | −10.61 * |
| Emergency Department | 48, 4.93 | −8.97 * |
| Total | 973, 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Townsend, L.; Heatwole, J.K.; Gee, N.R. Reactivation of a Hospital-Based Therapy Dog Visitation Program during the COVID-19 Pandemic. Animals 2022, 12, 1842. https://doi.org/10.3390/ani12141842
Townsend L, Heatwole JK, Gee NR. Reactivation of a Hospital-Based Therapy Dog Visitation Program during the COVID-19 Pandemic. Animals. 2022; 12(14):1842. https://doi.org/10.3390/ani12141842
Chicago/Turabian StyleTownsend, Lisa, Jennifer K. Heatwole, and Nancy R. Gee. 2022. "Reactivation of a Hospital-Based Therapy Dog Visitation Program during the COVID-19 Pandemic" Animals 12, no. 14: 1842. https://doi.org/10.3390/ani12141842