
Analgesic Effect of Butorphanol during Castration in Donkeys under Total Intravenous Anaesthesia


 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matthews, N.S.; Taylor, T.S.; Hartsfield, S.M. Anaesthesia of donkeys and mules. Equine Vet. Educ. 1997, 9, 198–202. [Google Scholar] [CrossRef]
- Mendoza, F.J.; Perez-Ecija, A.; Toribio, R.E. Clinical Pharmacology in Donkeys and Mules. Vet. Clin. N. Am. Equine Pract. 2019, 35, 589–606. [Google Scholar] [CrossRef]
- Matthews, N.; van Loon, J.P.A.M. Anesthesia, sedation, and pain management of donkeys and mules. Vet. Clin. N. Am Equine Pract. 2019, 35, 515–527. [Google Scholar] [CrossRef]
- Fielding, D. The number and distribution of equine in the world. In Donkeys, Mules and Horses in the Tropical Agricoltural Devel-opment; Colloquium Proceedings; Fielding, D., Pearson, R.A., Eds.; Edinburgh School of Agriculture and Centre of Tropical Veterinary Medicine, University of Edinburgh: Edinburgh, UK, 1991; pp. 62–66. [Google Scholar]
- Sgorbini, M.; Bonelli, F.; Rota, A.; Baragli, P.; Marchetti, V.; Corazza, M. Hematology and clinical chemistry in Amiata don-key foals from birth to 2 months of age. J. Equine Vet. Sci. 2013, 33, 35–39. [Google Scholar] [CrossRef]
- Ali, A.B.; Matoock, M.; Fouad, M.A.; Heleski, C.R. Are mules or donkeys better adapted for Egyptian brick kiln work? (Until we can change the kilns). J. Vet. Behav. 2015, 10, 158–165. [Google Scholar] [CrossRef]
- De Rose, P.; Cannas, E.; Cantiello, P.R. Donkey-assisted rehabilitation program for children: A pilot study. Ann. Dell’Istituto Super. Sanità 2011, 47, 391–396. [Google Scholar]
- Borioni, N.; Marinaro, P.; Celestini, S.; Del Sole, F.; Magro, R.; Zoppi, D.; Mattei, F.; Armi, V.D.; Mazzarella, F.; Cesario, A.; et al. Effect of equestrian therapy and onotherapy in physical and psycho-social performances of adults with intellectual disability: A preliminary study of evaluation tools based on the ICF classification. Disabil. Rehabil. 2011, 34, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Lizarraga, I.; Sumano, H.; Brumbaugh, G.W. Pharmacological and pharmacokinetic differences between donkeys and horses. Equine Vet. Educ. 2010, 16, 102–112. [Google Scholar] [CrossRef]
- Grosenbaugh, D.A.; Reinemeyer, C.R.; Figueiredo, M.D. Pharmacology and therapeutics in donkeys. Equine Vet. Educ. 2011, 23, 523–530. [Google Scholar] [CrossRef]
- Matthews, N.S.; Peck, K.E.; Mealey, K.L.; Taylor, T.S.; Ray, A.C. Pharmacokinetics and cardiopulmonary effects of guaifenesin in donkeys. J. Vet. Pharmacol. Ter. 1997, 20, 442–446. [Google Scholar] [CrossRef]
- Jordan, W.J. Surgery. In The professional Handbook of the Donkeys; Svendsen, E.D., Ed.; The Donkey Sanctuary: Devon, UK, 1986; pp. 101–119. [Google Scholar]
- Joubert, K.; Briggs, P.; Gerber, D.; Gottschalk, R. The sedative and analgesic effects of detomidine-butorphanol and detomidine alone in donkeys. J. S. Afr. Vet. Assoc. 1999, 70, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Daunt, D.A. Detomidine in equine sedation and analgesia. Compend. Contin. Educ. 1994, 15, 1405–1411. [Google Scholar]
- Yamashita, K.; Tsubakishita, S.; Futaoka, S.; Ueda, I.; Hamaguchi, H.; Seno, T.; Katoh, S.; Izumiawa, Y.; Kotani, T.; Miur, W.W. Cardiovascular effect of medetomidine, detomidine and xylazine in horses. J. Vet. Med. Sci. 2000, 62, 1025–1032. [Google Scholar] [CrossRef] [Green Version]
- Mostafa, M.B.; Farag, K.A.; Zomor, E.; Bashandy, M.M. The Sedative and Analgesic Effects of Detomidine (Domosedan) in Donkeys. J. Vet. Med. Ser. A 1995, 42, 351–356. [Google Scholar] [CrossRef]
- El-Maghraby, H.M.; Atta, A.H. Sedative and analgesic effects of detomidine with and without butorphanol in donkey. Assiut. Vet. Med. J. 1997, 37, 201–211. [Google Scholar]
- Lavoie, J.P.; Phan, S.T.; Blais, D. Effects of a combination of detomidine and butorphanol on respiratory function in horses with or without chronic obstructive pulmonary disease. Am. J. Vet. Res. 1996, 57, 705–709. [Google Scholar]
- Robertson, J.T.; Muir, W.W. A new analgesic drug combination in the horse. Am. J. Vet. Res. 1983, 44, 1667–1669. [Google Scholar]
- Taylor, P.M.; Browning, A.P.; Harris, C.P. Detomidine-butorphanol sedation in equine clinical practice. Vet. Rec. 1988, 123, 388–390. [Google Scholar] [CrossRef]
- Clarke, K.W.; Taylor, P.M. Detomidine: A new sedative for horses. Equine Vet. J. 1986, 18, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Clarke, K.W.; Paton, B.S. Combined use of detomidine with opiates in the horse. Equine Vet. J. 1988, 20, 331–334. [Google Scholar] [CrossRef]
- England, G.W.; Clarke, K.W. Apha2 adrenoreceptor agonists in the horse—A review. Br. Vet. J. 1996, 152, 641–657. [Google Scholar] [CrossRef]
- Kalpravidh, M.; Lumb, W.V.; Wright, M.; Heath, R.B. Effects of butorphanol, flunixin, levorphanol, morphine and xylazine in ponies. Am. J. Vet. Res. 1984, 45, 217–223. [Google Scholar]
- Coelho, C.M.M.; Moreno, J.C.D.; da Goulart, D.S.; Caetano, L.B.; Soares, L.K.; Coutinho, G.H.; Alves, G.E.S.; da Silva, A.F. Evaluation of cardiorespiratory and biochemical effects of ketamin–propofol and guaiphenesin-ketamine-xylazine anaesthesia in donkeys (Equus asinus). Vet. Anaesth. Analg. 2014, 41, 602–612. [Google Scholar] [CrossRef]
- Taylor, P.M.; Luna, S.P.L.; Sear, J.W.; Wheeler, M.J. Total intravenous anaesthesia in ponies using detomidine ketamine ad guaiphenesin: Pharmacokinetics, cardiopulmonary and endocrine effects. Res. Vet. Sci. 1996, 59, 17–23. [Google Scholar] [CrossRef]
- Bettschart-Wolfensberger, R.; Taylor, P.M.; Sear, J.W.; Bloomfield, M.R.; Rentsch, K.; Dawlin, S. Physiological effects of anaesthesia induced and maintained by intravenous administration of a climazolam-ketamine combination in ponies premedicated with acepromazine and xylazine. Am. J. Vet. Res. 1996, 57, 1472–1477. [Google Scholar]
- Taylor, P.M.; Kirby, J.J.; Shrimpton, D.J.; Johnson, J.B. Cardiovascular effects of surgical castration during anaesthesia main-tained with halothane or infusion of detomidine, ketamine and guaifenesin in ponies. Equine Vet. J. 1998, 30, 304–309. [Google Scholar] [CrossRef]
- Muir, W.W.; Lerche, P.; Robertson, J.T.; Hubbel, J.A.; Beard, W.; Miller, T.; Badgley, B.; Bothwell, V. Comparison of four drugs combinations for total intravenous anaesthesia of horses undergoing surgical removal of abdominal testis. J. Am. Vet. Med. Ass. 2000, 217, 869–873. [Google Scholar]
- Matthews, N.S.; Taylor, T.S.; A Sullivan, J. A comparison of three combinations of injectable anesthetics in miniature donkeys. Vet. Anaesth. Analg. 2002, 29, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Emami, M.R.; Seifi, H.; Tavakoli, Z. Effects of totally intravenous thiopental anesthesia on cardiopulmonary and termoregu-latory system in donkeys. J. Appl. An. Res. 2006, 1, 13–16. [Google Scholar] [CrossRef]
- Naddaf, H.; Baiadam, A.; Rasekh, A.; Arasteh, A.; Saboza, S. Cardiopulmonary effects during anaesthesia induced and mantained with propofol in acepromazine premedicated donkey. Vet. Anaesth. Analg. 2015, 42, 83–87. [Google Scholar] [CrossRef]
- Amin, A.A.; Mohammed, M.S. Cardiopulmonary effects of detomidine-propofol and ketamine administration in the donkey. Al Anbar J. Vet. Sci. 2012, 5, 168–172. [Google Scholar]
- Lindsay, F.E.; Clayton, H.M. An anatomical and endoscopic study of the nasopharynx and larynx of the donkeys (Equus asinus). J. Anat. 1986, 144, 123–132. [Google Scholar]
- Sprayson, T.; Thiemann, A. Clinical approach to castration in the donkey. Practice 2007, 29, 526–531. [Google Scholar] [CrossRef]
- Lerche, P. Total intravenous anaesthesia in horses. Vet. Clin. N. Am. Equine Pract. 2013, 29, 123–129. [Google Scholar] [CrossRef]
- Lizarraga, I.; Castillo-Alcala, F.; Varner, K.M.; Robinson, L.S. Sedation and mechanical antinociception after intravenous administration of detomidine in donkeys: A dosage-effect study. Vet. Rec. 2015, 176, 202. [Google Scholar] [CrossRef] [PubMed]
- Hamed, M.A.; Abouelnasr, K.S.; Ibrahim, H.M.; El-Khodery, S.A. Comparative, Sedative, and Analgesic Effects of Epidural Dexmedetomidine and Xylazine in Donkeys (Equus asinus). J. Equine Vet. Sci. 2017, 59, 104–109. [Google Scholar] [CrossRef]
- Kerr, C.L.; McDonnell, W.N.; Young, S.S. A comparison of romifidine and xylazine when used with diazepam/ketamine for short duration anaesthesia in the horse. Can. Vet. J. 1996, 37, 601–609. [Google Scholar]
- Vesce, G. Ocular nystagmus during general anaesthesia in the horse. Vet. Anaesth. Analg. 1982, 10, 257–263. [Google Scholar] [CrossRef]
- Love, E.J.; Taylor, P.M.; Clark, C.; Whay, H.R.; Murrell, J. Analgesic effect of butorphanol in ponies following castration. Equine Vet. J. 2009, 41, 552–556. [Google Scholar] [CrossRef]
- Love, E.J.; Taylor, P.M.; Whay, H.R.; Murrell, J. Postcastration analgesia in ponies using buprenorphine hydrochloride. Vet. Rec. 2013, 172, 635. [Google Scholar] [CrossRef]
- Costa, E.D.; Minero, M.; Lebelt, D.; Stucke, D.; Canali, E.; Leach, M.C. Development of the Horse Grimace Scale (HGS) as a Pain Assessment Tool in Horses Undergoing Routine Castration. PLoS ONE 2014, 9, e92281. [Google Scholar] [CrossRef] [Green Version]
- Mellor, D.; Stafford, K. Acute castration and/or tailing distress and its alleviation in lambs. N. Z. Vet. J. 2000, 48, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Aengwanich, W.; Sakundech, K.; Chompoosan, C.; Tuchpramuk, P.; Boonsorn, T. Physiological changes, pain stress, oxidative stress, and total antioxidant capacity before, during, and after castration in male dogs. J. Vet. Behav. 2019, 32, 76–79. [Google Scholar] [CrossRef]
- Mogheiseh, A.; Koohi, F.; Nazifi, S.; Tabrizi, A.S.; Taheri, P.; Salavati, S. Oxidative-antioxidative status and hepatic and renal factors following melatonin administration in castrated and intact dogs. Basic Clin. Androl. 2019, 29, 14. [Google Scholar] [CrossRef]
- Abou-Khalil, N.S.; Ali, M.F.; Ali, M.M.; Ibrahim, A. Surgical castration versus chemical castration in donkeys: Response of stress, lipid profile and redox potential biomarkers. BMC Vet. Res. 2020, 16, 310. [Google Scholar] [CrossRef]
- Taylor, P.M. Chemical restraint of the standing horse. Equine Vet. J. 1985, 17, 269–273. [Google Scholar] [CrossRef]
- Whiteheads, G.; French, J.; Ikin, P. Welfare and veterinary care of donkeys. Practice 1991, 13, 62–68. [Google Scholar] [CrossRef]
- Lizarraga, I.; Castillo-Alcada, F.; Varner, K.M.; Robinson, L.S. Sedation and mechanical hypoalgesia after sublingual admin-istration of detomidine hydrochloride gel to donkeys. J. Am. Vet. Med Assoc. 2016, 249, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Samimi, A.S. Evaluation of the sedative and clinical effects of xylazine, detomidine, medetomidine and dexmedetomidine in miniature donkeys. N. Z. Vet. J. 2019, 68, 198–202. [Google Scholar] [CrossRef]
- El-Kammar, M.H.; Gad, S.B. Antagonism of detomidine-induced sedation, analgesia, clinicophysiological, and biochemical effects in donkeys using IV tolazoline or atipamezole. J. Equine Vet. Sci. 2014, 34, 784–792. [Google Scholar] [CrossRef]
- Schatzmann, U.; Armbruster, S.; Stucki, F.; Busato, A.; Kohler, I. Analgesic Effect of Butorphanol and Levomethadone in Detomidine Sedated Horses. J. Vet. Med. Ser. A 2001, 48, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Kruluc, P.; Nemec, A. Electroencephalographic and electromyographic changes during the use of detomidine and detomidine-butorphanol combination in standing horses. Acta Vet. Hung. 2006, 54, 35–42. [Google Scholar] [CrossRef]
- Nyman, G.; Marntell, S.; Edner, A.; Funkquist, P.; Morgan, K.; Hedenstierna, G. Effect of sedation with detomidine and butorphanol on pulmonary gas exchange in the horse. Acta Vet. Scand. 2009, 51, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knych, H.K.; Casbeer, H.C.; McKemie, D.S.; Arthur, R.M. Pharmacokinetics and pharmacodynamics of butorphanol following intravenous administration to the horse. J. Vet. Pharmacol. Ther. 2013, 36, 21–30. [Google Scholar] [CrossRef]
- Marly, C.; Bettschart, R.; Nussbaumer, P.; Moine, S.; Ringer, S.K. Evaluation of a romifidine constant rate infusion protocol with or without butorphanol for dentistry and ophthalmologic procedures in standing horses. Vet. Anaesth. Analg. 2014, 41, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Chiavaccini, L.; Claude, A.K.; Lee, J.H.; Ross, M.K.; Meyer, R.E.; Langston, V.C. Pharmacokinetics and pharmacodynamics comparison between subcutaneous and intravenous butorphanol administration in horses. J. Vet. Pharmacol. Ther. 2015, 38, 365–374. [Google Scholar] [CrossRef]
- Moorman, V.J.; Bass, L.; King, M.R. Evaluation of the effects of commonly used α2-adrenergic receptor agonists alone and in combination with butorphanol tartrate on objective measurements of lameness in horses. Am. J. Vet. Res. 2019, 80, 868–877. [Google Scholar] [CrossRef] [PubMed]
- De Grauw, J.; van Loon, T. Clinical effects of two doses of butorphanol with detomidine for intravenous premedication of healthy warmblood horses. Vet. Anaesth. Analg. 2020, 47, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Paine, S.W.; Bright, J.; Scarth, J.P.; Hincks, P.R.; Pearce, C.M.; Hannan, C.; Machnik, M.; Hillyer, L. The intravenous pharmacokinetics of butorphanol and detomidine dosed in combination compared with individual dose administrations to exercised horses. J. Vet. Pharmacol. Ther. 2020, 43, 162–170. [Google Scholar] [CrossRef]
- Muir, W.W.; Robertson, J.T. Visceral analgesia: Effects of xylazine, butorphanol, meperidine, and pentazocine in horses. Am. J. Vet. Res. 1985, 46, 2081–2084. [Google Scholar]
- Bidwell, L.A. How to anesthetize donkeys for surgical procedures in the field. AAEP Proc. 2010, 56, 38–40. [Google Scholar]
- Lizarraga, I.; Castillo-Alcala, F. Sedative and mechanical hypoalgesic effects of butorphanol in xylazine -premedicated don-keys. Equine Vet. J. 2015, 47, 308–312. [Google Scholar] [CrossRef]
- El-Kammar, M.H.; Gad, S.B. Evaluation of the sedative, analgesic, clinicophysiological and haematological effects of intra-venous detomidine, detomidine-butorphanol, romifidine and romifidine-butorphanol in standing donkeys. Eq. Vet. Educ. 2014, 26, 202–207. [Google Scholar] [CrossRef]
- Van Dierendonck, M.C.; Burden, F.A.; Rickards, K.; Van Loon, J.P. Monitoring Acute Pain in Donkeys with the Equine Utrecht University Scale for Donkeys Composite Pain Assessment (EQUUS-DONKEY-COMPASS) and the Equine Utrecht University Scale for Donkey Facial Assessment of Pain (EQUUS-DONKEY-FAP). Animals 2020, 10, 354. [Google Scholar] [CrossRef] [Green Version]
- Van Loon, J.P.; de Grauw, J.C.; Burden, F.; Vos, K.J.; Bardelmeijer, L.H.; Rickards, K. Objective assessment of chronic pain in donkeys using the donkey chronic pain scale (DCPS): A scale-construction study. Vet. J. 2021, 267, 105580. [Google Scholar] [CrossRef]
- Weary, D.; Niel, L.; Flower, F.C.; Fraser, D. Identifying and preventing pain in animals. Appl. Anim. Behav. Sci. 2006, 100, 64–76. [Google Scholar] [CrossRef] [Green Version]
- Haga, H.A.; Dolvik, N.I. Electroencephalographic and cardiovascular variables as nociceptive indicators in isoflurane-anaesthetized horses. Vet. Anaesth. Analg. 2005, 32, 1–9. [Google Scholar] [CrossRef]
- Suriano, R.; Varasano, V.; Robbe, D.; Carluccio, A.; Straticò, P.; Contri, A.; Petrizzi, L. Intraoperative analgesic effect of intrafunicolar lidocaine injection during orchiectomy in isoflurane anaesthetized Martina Franca donkeys. J. Eq. Vet. Sci. 2014, 34, 793–798. [Google Scholar] [CrossRef]
- Hubbel, J.A.E.; Muir, W.W. Monitoring anaesthesia. In Equine Anaesthesia, Monitoring and Emergency Therapy, 2nd ed.; Saunders Elsevier Ed.: St. Louis, MO, USA, 2009; pp. 149–170. [Google Scholar]
- Yamaoka, T.; Flaherty, D.; Pawson, P.; Scott, M.; Auckburally, A. Comparison of arterial blood pressure measurements ob-tained invasively or oscillometrically using a Datex S/5 compact monitor in anaesthetized adult horses. Vet. Anaesth. Analg. 2017, 44, 492–501. [Google Scholar] [CrossRef] [Green Version]
- El-Ghoul, W.; Zabady, M.; Saleh, I. Total intravenous anaesthesia in donkeys (equus asinus): Comparison of anaesthetic and cardiorespiratory effects of four anaesthetic drug combinations. Vet. Med. J. Giza 2004, 52, 69–87. [Google Scholar]
- Haga, H.A.; Ljkkjen, S.; Revold, T.; Ranheim, B. Effect of intratesticular injection of lidocaine on cardiovascular responses to castration in isoflurane-anaesthetized stallions. Am. J. Vet. Res. 2006, 67, 403–408. [Google Scholar] [CrossRef]
- Wood, G.N.; Molony, V.; Fleetwood-Walker, S.M.; Hodgson, J.C.; Mellor, D.J. Effects of local anesthesia and intravenous naloxone on the changes in behaviour and plasma concentration of cortisol produced by castration and tail docking with tight rubber rings in young lambs. Res. Vet. Sci. 1991, 51, 193–199. [Google Scholar] [CrossRef]
- Stafford, K.J.; Mellor, D.J.; Todd, S.E.; Bruce, R.A.; Ward, R.N. Effects of local anaesthesia or local anaesthesia plus a non-steroidal an-ti-inflammatory drug on the acute cortisol response of calves to five different methods of castration. Res. Vet. Sci. 2002, 73, 61–70. [Google Scholar] [CrossRef]
- A Haga, H.; Ranheim, B. Castration of piglets: The analgesic effects of intratesticular and intrafunicular lidocaine injection. Veter. Anaesth. Analg. 2005, 32, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Straticò, P.; Varasano, V.; Suriano, R.; Mariscoli, M.; Robbe, D.; Giammarco, M.; Vignola, G.; Petrizzi, L. Analgesic effects of intravenous flunixin and intrafunicular lidocaine or their combination for castration of lambs. Veter. Rec. Open 2018, 5, e000266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portier, K.G.; Jaillardon, L.; Leece, E.A.; Walsh, C.M. Castration of horses under total intravenous anaesthesia: Analgesic effects of lidocaine. Vet. Anaesth. Analg. 2009, 36, 173–179. [Google Scholar] [CrossRef] [PubMed]
- McMurphy, R.M.; Young, L.E.; Marlin, D.J.; Walsh, K. Comparison of the cardiopulmonary effects of anaesthesia in horses. J. Vet. Res. 2002, 63, 1655–1661. [Google Scholar] [CrossRef]
- E Wagner, A.; Bednarski, R.M.; Muir, W.W. Hemodynamic effects of carbon dioxide during intermittent positive-pressure ventilation in horses. Am. J. Vet. Res. 1990, 51, 1922–1929. [Google Scholar]
- Matthews, N.; Van Loon, J.P.A.M. Anaesthesia and analgesia of the donkey and the mule. Equine Vet. Educ. 2011, 25, 47–51. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
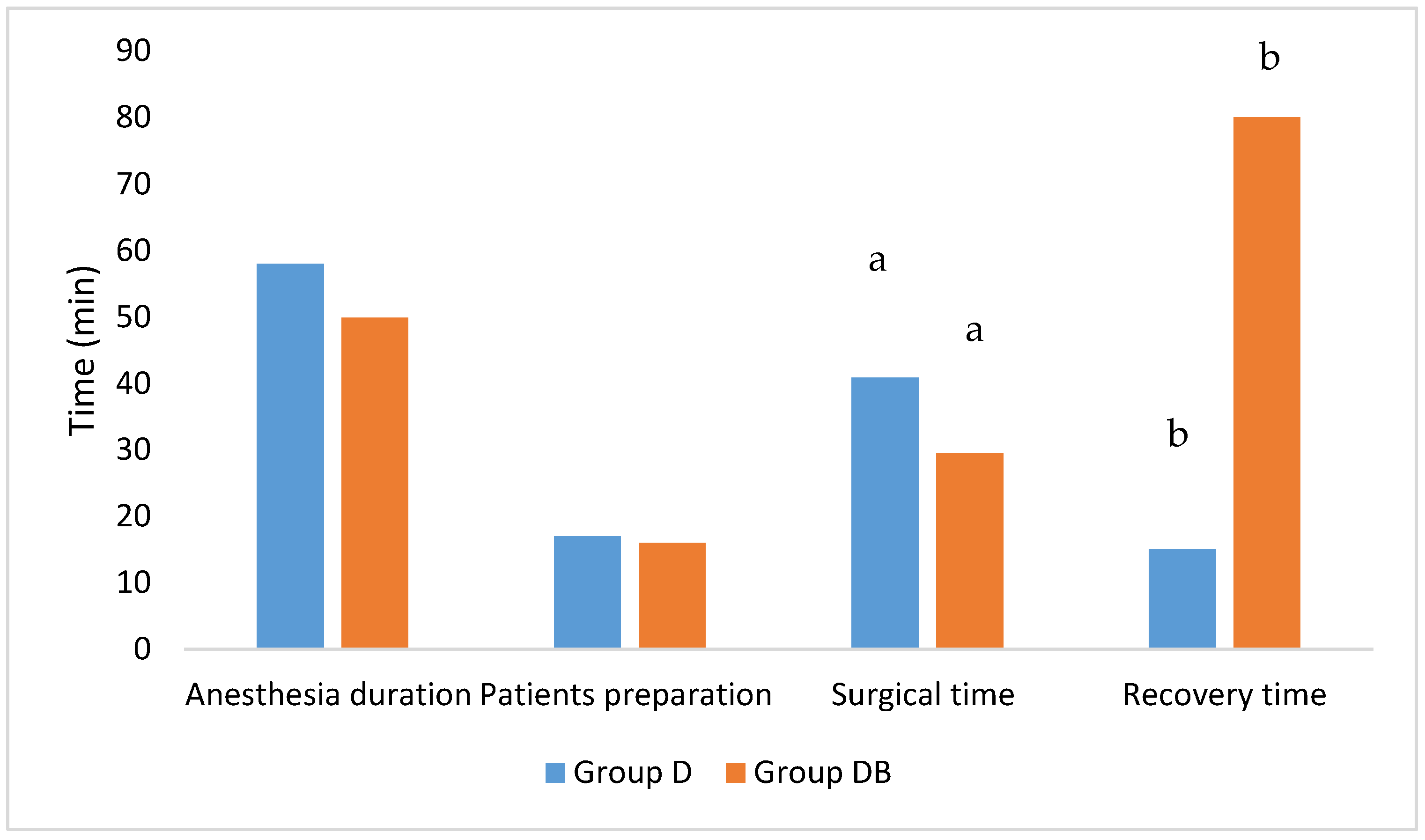
| Age (Months) | Body Weight (kg) | Anaesthesia Duration (min) | Patients Preparation (min) | Surgical Time (min) | Recovery Time (min) | |
|---|---|---|---|---|---|---|
| Group D | 25 ± 6 | 158 ± 46 | 58 ± 16 | 17 ± 5 | 41 ± 9 a | 15 ± 10 b |
| Group DB | 22 ± 10 | 157 ± 73 | 50 ± 11 | 16 ± 7 | 29.5 ± 8.6 a | 80 ± 38 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Straticò, P.; Carluccio, A.; Varasano, V.; Guerri, G.; Suriano, R.; Robbe, D.; Cerasoli, I.; Petrizzi, L. Analgesic Effect of Butorphanol during Castration in Donkeys under Total Intravenous Anaesthesia. Animals 2021, 11, 2346. https://doi.org/10.3390/ani11082346
Straticò P, Carluccio A, Varasano V, Guerri G, Suriano R, Robbe D, Cerasoli I, Petrizzi L. Analgesic Effect of Butorphanol during Castration in Donkeys under Total Intravenous Anaesthesia. Animals. 2021; 11(8):2346. https://doi.org/10.3390/ani11082346
Chicago/Turabian StyleStraticò, Paola, Augusto Carluccio, Vincenzo Varasano, Giulia Guerri, Riccardo Suriano, Domenico Robbe, Ilaria Cerasoli, and Lucio Petrizzi. 2021. "Analgesic Effect of Butorphanol during Castration in Donkeys under Total Intravenous Anaesthesia" Animals 11, no. 8: 2346. https://doi.org/10.3390/ani11082346