
Bidimensional and Contrast-Enhanced Ultrasonography of the Spleen in Dogs Affected by Leishmaniosis

 , , , ,
, , , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Inclusion Criteria, and Exclusion Criteria
2.2. Clinical Data Collection
2.3. Sampling Procedures
2.4. Staging of Leishmaniosis according to LeishVet Guidelines
2.5. Clinicopathological Evaluation
2.6. Detection of Antibodies against Leishmania and Other Vector-Borne Pathogens (VBPs)
2.7. DNA Extraction and Leishmania Real-Time PCR
2.8. Molecular Investigations for Other VBPs
2.9. Spleen Ultrasonography Procedures
2.10. Cytological Procedures
2.11. Statistical Analysis
3. Results
3.1. Clinical Evaluation of Dogs and Staging of Leishmaniosis
3.2. B-Mode Ultrasonography
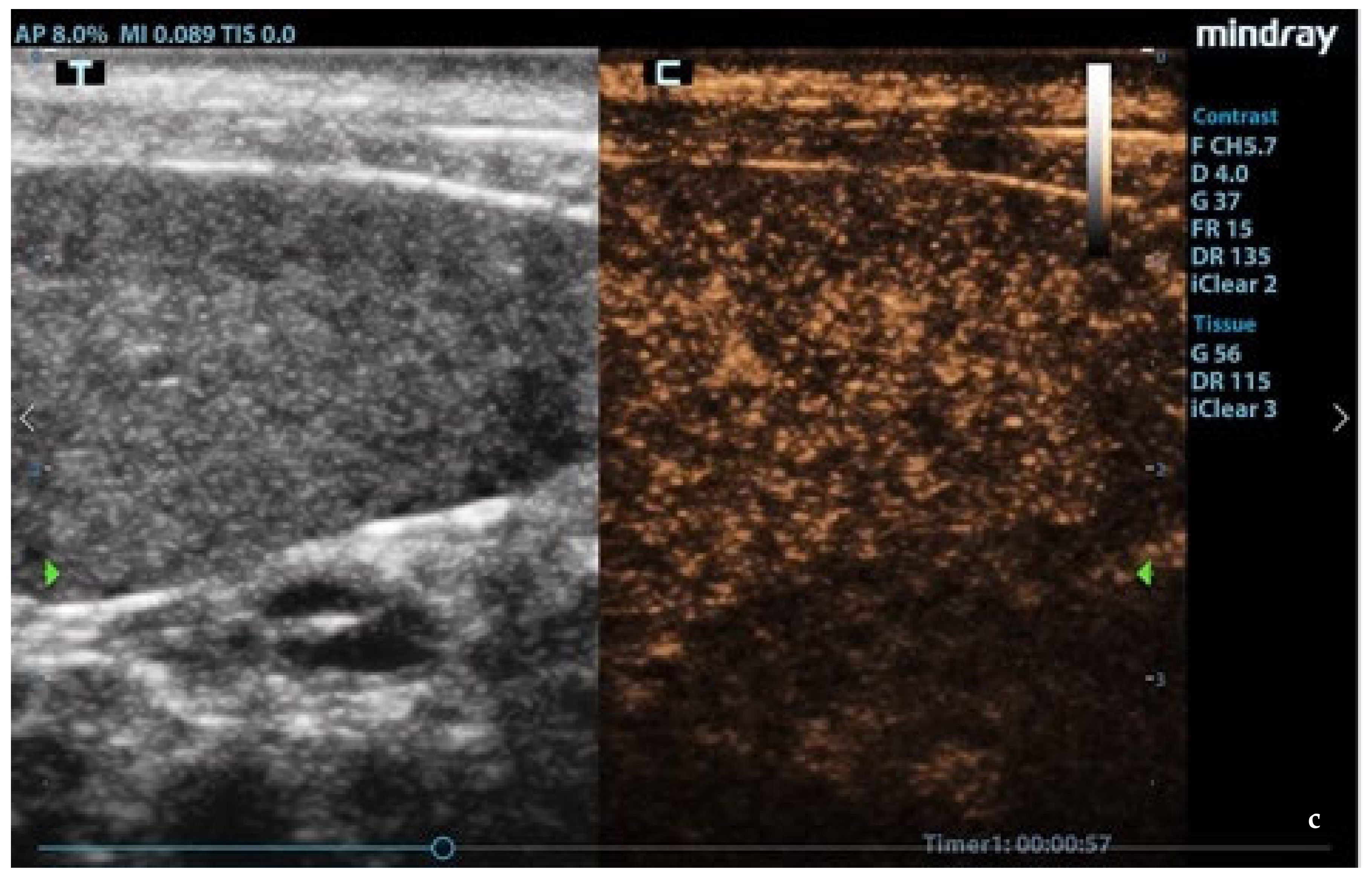
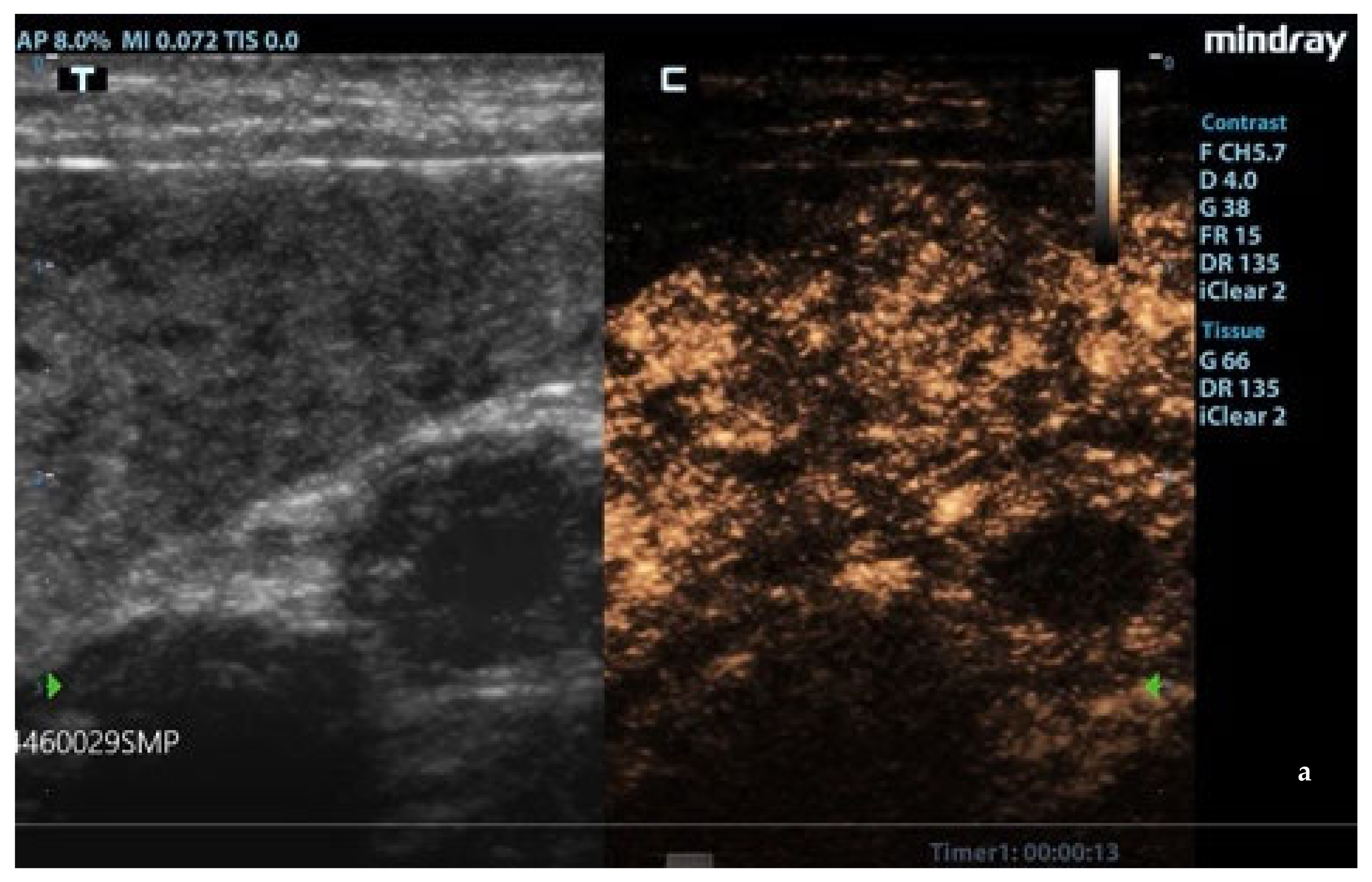
3.3. CEUS
3.4. Cytology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Solano-Gallego, L.; Koutinas, A.; Miró, G.; Cardoso, L.; Pennisi, M.G.; Ferrer, L.; Bourdeau, P.; Oliva, G.; Baneth, G. Directions for the diagnosis, clinical staging, treatment and prevention of canine leishmaniosis. Vet. Parasitol. 2009, 165, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Solano-Gallego, L.; Miró, G.; Koutinas, A.; Cardoso, L.; Pennisi, M.G.; Ferrer, L.; Bourdeau, P.; Oliva, G.; Baneth, G.; The LeishVet Group. LeishVet guidelines for the practical management of canine leishmaniosis. Parasit. Vectors 2011, 4, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miró, G.; Cardoso, L.; Pennisi, M.G.; Oliva, G.; Baneth, G. Canine leishmaniosis—New concepts and insights on an expanding zoonosis: Part two. Trends Parasitol. 2008, 24, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Pennisi, M.G. Leishmaniosis of companion animals in Europe: An update. Vet Parasitol. 2015, 208, 35–47. [Google Scholar] [CrossRef]
- Esch, K.J.; Juelsgaard, R.; Martinez, P.A.; Jones, D.E.; Petersen, C.A. Programmed death 1-mediated T cell exhaustion during visceral leishmaniasis impairs phagocyte function. J. Immunol. 2013, 191, 5542–5550. [Google Scholar] [CrossRef] [Green Version]
- Geisweid, K.; Mueller, R.; Sauter-Louis, C.; Hartmann, K. Prognostic analytes in dogs with Leishmania infantum infection living in a non-endemic area. Vet. Rec. 2012, 171, 399. [Google Scholar] [CrossRef]
- Roura, X.; Cortadellas, O.; Day, M.J.; Benali, S.L.; Zatelli, A.; Canine Leishmaniosis Working Group. Canine leishmaniosis and kidney disease: Q&A for an overall management in clinical practice. J. Small. Anim. Pract. 2021, 62, E1–E19. [Google Scholar] [CrossRef]
- Hermida, M.D.; de Melo, C.V.B.; Lima, I.D.S.; Oliveira, G.G.S.; Dos-Santos, W.L.C. Histological disorganization of spleen compartments and severe visceral leishmaniasis. Front. Cell. Infect. Microbiol. 2018, 8, 394. [Google Scholar] [CrossRef] [Green Version]
- Cavalcanti, A.S.; Ribeiro-Alves, M.; de O. Pereira, L.; Mestre, G.L.; Ferreira, A.B.R.; Morgado, F.N.; Boité, M.C.; Cupolillo, E.; Moraes, M.O.; Porrozzi, R. Parasite load induces progressive spleen architecture breakage and impairs cytokine mRNA expression in Leishmania infantum-naturally infected dogs. PLoS ONE 2015, 10, e0123009. [Google Scholar] [CrossRef]
- Bagues, N.C.T.; Pinheiro, C.G.M.; Bastos, L.A.; Fraga, D.B.M.; Veras, P.S.T.; Pontes-de-Carvalho, L.C.; Dos-Santos, W.L.C.; Oliveira, G.G.S. Parasitic load and histological aspects in different regions of the spleen of dogs with visceral leishmaniasis. Comp. Immunol. Microbiol. Infect. Dis. 2018, 56, 14–19. [Google Scholar] [CrossRef]
- Da Silva, A.V.A.; Figueiredo, F.B.; Menezes, R.C.; Mendes-Junior, A.A.; de Miranda, L.H.M.; Cupolillo, E.; Porrozzi, R.; Morgado, F.N. Morphophysiological changes in the splenic extracellular matrix of Leishmania infantum-naturally infected dogs is associated with alterations in lymphoid niches and the CD4+ T cell frequency in spleens. PLoS Negl. Trop. Dis. 2018, 12, e0006445. [Google Scholar] [CrossRef]
- Paradies, P.; Cipone, M.; Mele, I.; Greco, B.; Romano, D.; Sasanelli, M. Abdominal ultrasound findings associated with canine visceral leishmaniasis in endemic areas. Ann. Clin. Cytol. Pathol. 2018, 4, 1093. [Google Scholar]
- Alexandre-Pires, G.; Pais, D.; Correia, M.; Pina, J.A. Leishmaniosis—A report about the microvascular and cellular architecture of the infected spleen in Canis familiaris. Microsc. Res. Tech. 2006, 69, 227–235. [Google Scholar] [CrossRef]
- Nakamura, K.; Sasaki, N.; Yoshikawa, M.; Ohta, H.; Hwang, S.J.; Mimura, T.; Yamasaki, M.; Takiguchi, M. Quantitative contrast-enhanced ultrasonography of canine spleen. Vet. Radiol. Ultrasound 2009, 50, 104–108. [Google Scholar] [CrossRef]
- Nakamura, K.; Sasaki, N.; Murakami, M.; Bandula Kumara, W.R.; Ohta, H.; Yamasaki, M.; Takagi, S.; Osaki, T.; Takiguchi, M. Contrast-enhanced ultrasonography for characterization of focal splenic lesions in dogs. J. Vet. Intern. Med. 2010, 24, 1290–1297. [Google Scholar] [CrossRef]
- Rossi, F.; Leone, V.F.; Vignoli, M.; Laddaga, E.; Terragni, R. Use of contrast-enhanced ultrasound for characterization of focal splenic lesions. Vet. Radiol. Ultrasound 2008, 49, 154–164. [Google Scholar] [CrossRef]
- Ohlerth, S.; Dennler, M.; Rüefli, E.; Hauser, B.; Poirier, V.; Siebeck, N.; Roos, M.; Kaser-Hotz, B. Contrast harmonic imaging characterization of canine splenic lesions. J. Vet. Intern. Med. 2008, 22, 1095–1102. [Google Scholar] [CrossRef]
- Mangano, C.; Macrì, F.; Di Pietro, S.; Pugliese, M.; Santoro, S.; Iannelli, N.M.; Mazzullo, G.; Crupi, R.; De Majo, M. Use of contrast-enhanced ultrasound for assessment of nodular lymphoid hyperplasia (NLH) in canine spleen. BMC Vet. Res. 2019, 15, 196. [Google Scholar] [CrossRef]
- Acierno, M.J.; Brown, S.; Coleman, A.E.; Jepson, R.E.; Papich, M.; Stepien, R.L.; Syme, H.M. ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J. Vet. Intern. Med. 2018, 32, 1803–1822. [Google Scholar] [CrossRef]
- International Renal Interest Society. IRIS Staging of CKD (2019). Available online: http://www.iris-kidney.com/guidelines/staging.html (accessed on 28 August 2019).
- Piaton, E.; Fabre, M.; Goubin-Versini, I.; Bretz-Grenier, M.F.; Courtade-Saïdi, M.; Vincent, S.; Belleannée, G.; Thivolet, F.; Boutonnat, J.; Debaque, H.; et al. Cochand-Priollet, B.Guidelines for May-Grünwald-Giemsa staining in haematology and non-gynaecological cytopathology: Recommendations of the French Society of Clinical Cytology (SFCC) and of the French Association for Quality Assurance in Anatomic and Cytologic Pathology (AFAQAP). Cytopathology 2016, 27, 359–368. [Google Scholar] [CrossRef]
- Vitale, F.; Reale, S.; Vitale, M.; Petrotta, E.; Torina, A.; Caracappa, S. TaqMan-based detection of Leishmania infantum DNA using canine samples. Ann. N. Y. Acad. Sci. 2004, 1026, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Tzianabos, T.; Anderson, B.E.; McDade, J.E. Detection of Rickettsia rickettsii DNA in clinical specimens by using polymerase chain reaction technology. J. Clin. Microbiol. 1989, 27, 2866–2868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carret, C.; Walas, F.; Carcy, B.; Grande, N.; Précigout, E.; Moubri, K.; Schetters, T.P.; Gorenflot, A. Babesia canis canis, Babesia canis vogeli, Babesia canis rossi: Differentiation of the three subspecies by a restriction fragment length polymorphism analysis on amplified small subunit ribosomal RNA genes. J. Eukaryot. Microbiol. 1999, 46, 298–303. [Google Scholar] [CrossRef] [PubMed]
- To, H.; Kako, N.; Zhang, G.Q.; Otsuka, H.; Ogawa, M.; Ochiai, O.; Nguyen, S.V.; Yamaguchi, T.; Fukushi, H.; Nagaoka, N.; et al. Q fever pneumonia in children in Japan. J. Clin. Microbiol. 1996, 34, 647–651. [Google Scholar] [CrossRef] [Green Version]
- Inokuma, H.; Fujii, K.; Matsumoto, K.; Okuda, M.; Nakagome, K.; Kosugi, R.; Hirakawa, M.; Onishi, T. Demonstration of Anaplasma (Ehrlichia) platys inclusions in peripheral blood platelets of a dog in Japan. Vet. Parasitol. 2002, 110, 145–152. [Google Scholar] [CrossRef]
- Choi, Y.J.; Jang, W.J.; Kim, J.H.; Ryu, J.S.; Lee, S.H.; Park, K.H.; Paik, H.S.; Koh, Y.S.; Choi, M.S.; Kim, I.S. Spotted fever group and typhus group rickettsioses in humans, South Korea. Emerg. Infect. Dis. 2005, 11, 237–244. [Google Scholar] [CrossRef]
- De la Fuente, J.; Massung, R.F.; Wong, S.J.; Chu, F.K.; Lutz, H.; Meli, M.; von Loewenich, F.D.; Grzeszczuk, A.; Torina, A.; Caracappa, S.; et al. Sequence analysis of the msp4 gene of Anaplasma phagocytophilum strains. J. Clin. Microbiol. 2005, 43, 1309–1317. [Google Scholar] [CrossRef] [Green Version]
- Oteo, J.A.; Portillo, A.; Santibáñez, S.; Blanco, J.R.; Pérez-Martínez, L.; Ibarra, V. Cluster of cases of human Rickettsia felis infection from Southern Europe (Spain) diagnosed by PCR. J. Clin. Microbiol. 2006, 44, 2669–22671. [Google Scholar] [CrossRef] [Green Version]
- Siarkou, V.I.; Mylonakis, M.E.; Bourtzi-Hatzopoulou, E.; Koutinas, A.F. Sequence and phylogenetic analysis of the 16S rRNA gene of Ehrlichia canis strains in dogs with clinical monocytic ehrlichiosis. Vet. Microbiol. 2007, 125, 304–312. [Google Scholar] [CrossRef]
- Hecht, S. Spleen. In Atlas of Small Animal Ultrasonography, 1st ed.; Penninck, D., d’Anjou, M., Eds.; Blackwell Publishing: Ames, IA, USA, 2008; pp. 263–280. [Google Scholar]
- Bertal, M.; Norman Carmel, E.; Diana, A.; Desquilbet, L.; Specchi, S.; Pey, P. Association between ultrasonographic appearance of splenic parenchyma and cytology in cats. J. Feline Med. Surg. 2018, 20, 23–29. [Google Scholar] [CrossRef]
- Bonfanti, U.; Ghibaudo, G.; Zatelli, A.; Santilli, R.; Bussadori, C. Diagnosi citologica in corso di patologie epatiche e spleniche del cane e del gatto. Studio retrospettivo su 122 casi (1998–2000). Veterinaria 2003, 17, 9–15. [Google Scholar]
- Nyland, T.G.; Mattoon, J.S. Spleen. In Small Animal Diagnostic Ultrasound, 3rd ed.; Elsevier: St. Louis, MO, USA, 2015; pp. 400–437. [Google Scholar]
- Eberhardt, F.; Köhler, C.; Krastel, D.; Winter, K.; Alef, M.; Kiefer, I. Sonographisch erfassbare milzveränderungen bei hunden mit malignem lymphom. Tierarztl. Prax. Ausg. K Kleintiere Heimtiere 2015, 43, 215–220. [Google Scholar] [CrossRef]
- Harel, M.; Touzet, C.; Barthélemy, A.; Ségard-Weisse, E.M. Prevalence and diagnostic value of the ultrasonographic honeycomb appearance of the spleen in cats. J. Feline Med. Surg. 2020, 22, 186–192. [Google Scholar] [CrossRef]
- Silva, J.S.; Andrade, A.C.; Santana, C.C.; Santos, L.Q.; Oliveira, C.I.; Veras, P.S.; Vassallo, J.; dos-Santos, W.L. Low CXCL13 expression, splenic lymphoid tissue atrophy and germinal center disruption in severe canine visceral leishmaniasis. PLoS ONE 2012, 7, e29103. [Google Scholar] [CrossRef] [Green Version]
- Lima, I.S.; Silva, J.S.; Almeida, V.A.; Junior, F.G.; Souza, P.A.; Larangeira, D.F.; Moura-Neto, J.P.; Fraga, D.B.; de Freitas, L.A.; dos-Santos, W.L. Severe clinical presentation of visceral leishmaniasis in naturally infected dogs with disruption of the splenic white pulp. PLoS ONE 2014, 9, e87742. [Google Scholar] [CrossRef] [Green Version]
- Ohlerth, S.; Rüefli, E.; Poirier, V.; Roos, M.; Kaser-Hotz, B. Contrast harmonic imaging of the normal canine spleen. Vet. Radiol. Ultrasound 2007, 48, 451–456. [Google Scholar] [CrossRef]
- Cosgrove, D. Future prospects for SonoVue and CPS. Eur. Radiol. 2004, 14, 116–124. [Google Scholar] [CrossRef]
- Bronte, V.; Pittet, M.J. The spleen in local and systemic regulation of immunity. Immunity 2013, 39, 806–818. [Google Scholar] [CrossRef] [Green Version]
- Movilla, R.; Altet, L.; Serrano, L.; Tabar, M.D.; Roura, X. Molecular detection of vector-borne pathogens in blood and splenic samples from dogs with splenic disease. Parasit. Vectors 2017, 10, 131. [Google Scholar] [CrossRef] [Green Version]
- Sarma, K.; Mondal, D.B.; Saravanan, M. Ultrasonographic changes in dogs naturally infected with tick borne intracellular diseases. J. Parasit. Dis. 2016, 40, 248–251. [Google Scholar] [CrossRef] [Green Version]
- Fraga, E.; Barreiro, J.D.; Goicoa, A.; Espino, L.; Fraga, G.; Barreiro, A. Abdominal ultrasonographic findings in dogs naturally infected with babesiosis. Vet. Radiol. Ultrasound 2011, 52, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Maronezi, M.C.; Feliciano, M.A.R.; Crivellenti, L.Z.; Borin-Crivellenti, S.; Silva, P.E.S.; Zampolo, C.; Pavan, L.; Gasser, B.; Simões, A.P.R.; Macie, G.S.; et al. Spleen evaluation using contrast enhanced ultrasonography and Doppler in dogs with subclinical ehrlichiosis. Arq. Bras. Med. Vet. Zootec. 2015, 67, 1528–1532. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathogen | Region Amplified | Primers (5′-3′) | Fragment Length (bp) | Reference |
|---|---|---|---|---|
| Rickettsia spp. | 17KDa antigen | TZ15–19 5’-TTC TCA ATT CGG TAA GGG C-3’ | 246 | [23] |
| TZ16–20 5’-ATA TTG ACC AGT GCT ATT TC-3’ | ||||
| Rickettsia spp. | Omp A | Rr190.70p ATGGCGAATATTTCTCCAAAA | 532 | [29] |
| Rr190.701n GTTCCGTTAATGGCAGCATCT | ||||
| Rr190.602n AGTGCAGCATTCGCTCCCCCT | ||||
| Rickettsia spp. | Omp B | rompB OF GTAACCGGAAGTAATCGTTTCGTAA | 511/425 | [27] |
| rompB OR GCTTTATAACCAGCTAAACCACC | ||||
| rompB SFG IF GTTTAATACGTGCTGCTAACCAA | ||||
| rompB SFG/TG IR GGTTTGGCCCATATACCATAAG | ||||
| E. canis | 16SrRNA | ECC AGAACGAACGCTGGCGGCAAGCC | 480/390 | [30] |
| ECB CGTATTACCGCGGCTGCTGGCA | ||||
| ‘‘canis’’ CAATTATTTATAGCCTCTGGCTATAGGA | ||||
| HE3 TATAGGTACCGTCATTATCTTCCCTAT | ||||
| Anaplasma phagocytophilum | msp4 | MSP4AP5 5’-ATGAATTACAGAGAATTGCTTGTAGG-3’ | 849 | [28] |
| MSP4AP3 5’-TTAATTGAAAGCAAATCTTGCTCCTATG-3’ | ||||
| Anaplasma platys | 16SrRNA | PLATY-F 5’-AAG TCG AAC GGA TTT TTG TC-3′ | ~500 | [26] |
| PLATYS-R 5′-CTT TAA CTT ACC GAA CC-3′ | ||||
| Coxiella burnetiid | htpB | Q5 (5′-GCG GGT GAT GGT ACC ACA ACA-3′) | 501 | [25] |
| Q3 (5′-GGC AAT CAC CAA TAA GGG CCG-3′) | ||||
| Q6 (5′-TT GCT GGA ATG AAC CCC A-3′) | 325 | |||
| Q4 (5′-TC AAG CTC CGC ACT CAT G-3′) | ||||
| Babesia canis | ssu-rDNA | PIRO-A 5′AATACCCAATCCTGACACAGGG 3’ | ~400 | [24] |
| PIRO-B 5’TTAAATACGAATGCCCCCAAC 3’ |
| Clinical Classification | Number of Dogs (%) |
|---|---|
| ICH | 1 (4.5) |
| Stage I (mild disease) | 5 (22.8) |
| Stage II (moderate disease) | |
| IIa | 9 (40.9) |
| IIb | 1 (4.5) |
| Stage III (severe disease) | 2 (9.1) |
| Stage IV (very severe disease) | 4 (18.2) |
| Samples | Tested Samples | Positive Samples (%) | Parasite Load |
|---|---|---|---|
| Conjunctival swabs | 52 | 1 (1.9) | 85 |
| Oral swabs | 26 | 1 (3.8) | 115 |
| Auricular swabs | 25 | 2 (8) | 15–430 |
| K2EDTA samples | 26 | 4 (15.4) | 30–70 |
| Lymph node aspirates | 15 | 9 (60) | 110–6400 |
| Spleen aspirates | 26 | 8 (30.8) | 10–18,000 |
| Nodule aspirates | 2 | 1 (50) | 130 |
| Clinical Signs | Number of Dogs (%) | |
|---|---|---|
| Dogs with CanL | Control Dogs | |
| Low Body Condition Score (BCS/9) | 8 (36.4) | 0 |
| Low Muscle Condition Score (MCS/4) | 5 (22.7) | 0 |
| Decreased appetite | 1 (4.5) | 0 |
| Lethargy | 0 | 0 |
| Fever | 0 | 0 |
| Lymphadenomegaly | 17 (77.3) | 1 (33.3) |
| Local | 15 (68.2) | 0 |
| Generalized | 2 (9.1) | 1 (33.3) |
| Skin lesionsNodular dermatitis | 9 (40.9)3 (13.6) | 0- |
| Ulcerative dermatitis | 1 (4.5) | - |
| Squamous dermatitis | 4 (18.2) | - |
| Alopecia | 5 (22.7) | - |
| Splenomegaly | 8 (36.4) | 0 |
| Epistaxis | 0 | 0 |
| Ocular lesions | 6 (27.3) | 0 |
| Blepharoconjunctivitis | 4 (18.2) | - |
| Conjunctival granulomas | 0 | - |
| Keratouveitis | 2 (9.1) | - |
| Parameter (units) | High (%) | Low (%) | WRI (%) | Reference Interval | |||
|---|---|---|---|---|---|---|---|
| Dogs with CanL | Control Dogs | Dogs with CanL | Control Dogs | Dogs with CanL | Control Dogs | ||
| Hematology | |||||||
| Red blood cells (M/µL) | 2 (9.1) | 1 (33.3) | 6 (27.3) | 0 | 14 (63.6) | 2 (66.7) | 5.65–8.87 |
| Hematocrit (%) | 1 (4.6) | 0 | 7 (31.8) | 0 | 14 (63.6) | 3 (100) | 37.3–61.7 |
| Hemoglobin (g/dL) | 1 (4.5) | 0 | 9 (40.9) | 1 (33.3) | 12 (54.6) | 2 (66.7) | 13.1–20.5 |
| MCV (fL) | 0 | 0 | 4 (18.2) | 0 | 18 (81.8) | 3 (100) | 61.6–73.5 |
| MCHC (g/dL) | 0 | 0 | 3 (13.6) | 0 | 19 (86.4) | 3 (100) | 32.0–37.9 |
| RDW (%) | 0 | 0 | 0 | 0 | 22 | 3 (100) | 13.6–21.7 |
| Reticulocytes (K/µL) | 1 (4.5) | 1 (33.3) | 0 | 0 | 21 (95.5) | 2 (66.7) | 10.0–110.0 |
| White blood cells (K/µL) | 1 (4.5) | 0 | 0 | 0 | 21 (95.5) | 3 (100) | 5.05–16.76 |
| Neutrophils (K/µL) | 1 (4.5) | 0 | 0 | 1 (33.3) | 21 (95.5) | 2 (66.7) | 2.95–11.64 |
| Lymphocytes (K/µL) | 0 | 0 | 3 (13.6) | 0 | 19 (86.4) | 3 (100) | 1.05–5.10 |
| Monocytes (K/µL) | 3 (13.6) | 0 | 0 | 0 | 19 (86.4) | 3 (100) | 0.16–1.12 |
| Eosinophils (K/µL) | 7 (31.8) | 1 (33.3) | 2 (9.1) | 0 | 13 (59.1) | 2 (66.7) | 0.06–1.23 |
| Basophils (K/µL) | 3 (13.6) | 0 | 0 | 0 | 19 (86.4) | 3 (100) | 0.00–0.10 |
| Platelets (K/µL) | 0 | 0 | 5 * (22.7) | 1 *(33.3) | 17 (77.3) | 2 (66.7) | 148–484 |
| Biochemistry | |||||||
| BUN (mg/dL) | 3 (13.6) | 0 | 0 | 0 | 19 (86.4) | 3 (100) | 10–25 |
| Creatinine (mg/dL) | 1 (4.5) | 0 | 0 | 0 | 21 (95.5) | 3 (100) | <2 |
| TP (g/dL) | 2 (9.1) | 1 (33.3) | 1 (4.5) | 0 | 19 (86.4) | 2 (66.7) | 5.5–7.8 |
| Albumin (g/dL) | 0 | 0 | 6 (27.3) | 1 (33.3) | 16 (72.7) | 2 (66.7) | 2.5–3.5 |
| ALT (UI/L) | 2 (9.1) | 0 | 0 | 0 | 20 (90.9) | 3 (100) | <100 |
| AST (UI/L) | 0 | 0 | 0 | 0 | 22 | 3 (100) | <90 |
| UPC (no units) | 7 (31.8) | 0 | 0 | 0 | 15 (68.2) | 3 (100) | <0.5 |
| Pathogens | Seroreactive Dogs (%) | |
|---|---|---|
| CanL | Control Dogs | |
| Ehrlichia canis | 3/22 (13.6) | 1/3 (33.3) |
| Rickettsia conorii | 13/22 (59.1) | 3/3 (100) |
| Anaplasma phagocytophilum | 5/21 (23.8) | 2/3 (66.7) |
| Coxiella burnetii | 2/22 (9.1) | 1/3 (33.3) |
| GOF | BI | AT | TTP | PI | AS | DT/2 | DS | AUC | |
|---|---|---|---|---|---|---|---|---|---|
| ROI1 | 0.83 | 15.62 | 2.27 | 31.02 | 21.33 | 0.18 | 109.72 | −0.03 | 3303.61 |
| ROI2 | 0.82 | 15.90 | 2.18 | 28.53 | 21.47 | 0.15 | 109.08 | −0.03 | 3283.48 |
| ROI3 | 0.90 | 15.87 | 1.30 | 30.28 | 21.44 | 0.14 | 116.12 | −0.03 | 3335.92 |
| SEM | 0.05 | 0.21 | 0.08 | 1.71 | 2.65 | 0.15 | 2.55 | 0.09 | 18.38 |
| p-value | 0.06 | 0.48 | 0.08 | 0.24 | 0.49 | 0.30 | 0.16 | 0.12 | 0.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Majo, M.; Donato, G.; Masucci, M.; Mangano, C.; Persichetti, M.F.; Liotta, L.; Mazzullo, G.; Visalli, R.; Quartuccio, M.; Iannelli, N.M.; et al. Bidimensional and Contrast-Enhanced Ultrasonography of the Spleen in Dogs Affected by Leishmaniosis. Animals 2021, 11, 1437. https://doi.org/10.3390/ani11051437
De Majo M, Donato G, Masucci M, Mangano C, Persichetti MF, Liotta L, Mazzullo G, Visalli R, Quartuccio M, Iannelli NM, et al. Bidimensional and Contrast-Enhanced Ultrasonography of the Spleen in Dogs Affected by Leishmaniosis. Animals. 2021; 11(5):1437. https://doi.org/10.3390/ani11051437
Chicago/Turabian StyleDe Majo, Massimo, Giulia Donato, Marisa Masucci, Cyndi Mangano, Maria Flaminia Persichetti, Luigi Liotta, Giuseppe Mazzullo, Rosanna Visalli, Marco Quartuccio, Nicola Maria Iannelli, and et al. 2021. "Bidimensional and Contrast-Enhanced Ultrasonography of the Spleen in Dogs Affected by Leishmaniosis" Animals 11, no. 5: 1437. https://doi.org/10.3390/ani11051437