
The Cat Mandible (II): Manipulation of the Jaw, with a New Prosthesis Proposal, to Avoid Iatrogenic Complications

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Temporomandibular Joint Luxation
3. Mandibular Fractures
3.1. General Considerations
3.2. Symphyseal Fractures
3.3. Body Fractures
3.4. Fractures of the Ramus
3.5. Impairment of the Nervous Supply
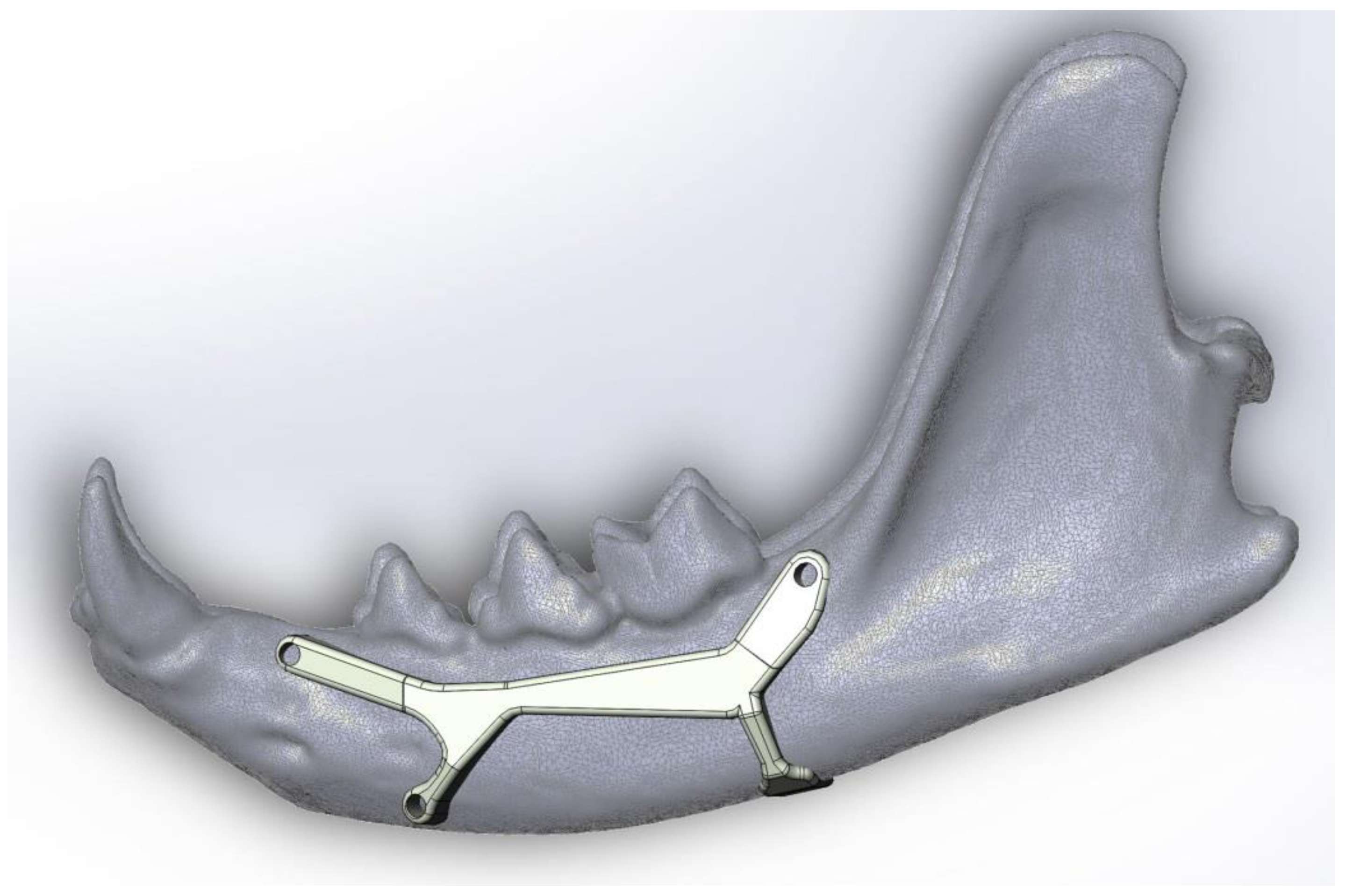
4. Prosthesis Proposal to Fix a Simple Fracture of the Mandibular Body
4.1. Calculations
4.2. Flexural Strength
- F is the biting force (N)
- d is the distance between the point of application of the force and the point of evaluation (the maximum distance to obtain the most critical effort) (mm)
- b corresponds to thickness value (mm)
- h corresponds to height value (mm)
- M corresponds to flexure moment value (N·mm)
- σ corresponds to tension value (MPa)
4.3. Shear Resistance of Screws
- τ corresponds to shear tension in screws (N/mm)
- F corresponds to bite force (F)
- r corresponds to screw radius (mm)
5. Future Trends
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Lombardero, M.; Alonso-Peñarando, D.; Yllera, M.M. The cat mandible (I): Anatomical basis to avoid iatrogenic damage in veterinary clinical practice. Animals 2021, 11, 405. [Google Scholar] [CrossRef] [PubMed]
- Hsuan, L.; Biller, D.S.; Tucker-Mohl, K. Open mouth jaw locking in a cat and a literature review. Isr. J. Vet. Med. 2017, 72, 54–59. [Google Scholar]
- Reiter, A.; Lewis, J.R. Trauma-associated musculoskeletal injury to the head. In Manual of Trauma Management in the Dog and Cat; Drobatz, K.J., Beal, M.W., Syring, R.S., Eds.; Willey-Blackwell: Delhi, India, 2011; pp. 255–292. ISBN 978-0-470-95831-5. [Google Scholar]
- Glyde, M.; Lidbetter, D. Management of fractures of the mandible in small animals. Practice 2003, 25, 570–585. [Google Scholar] [CrossRef]
- Tundo, I.; Southerden, P.; Perry, A.; Haydock, R.M. Location and distribution of craniomaxillofacial fractures in 45 cats presented for the treatment of head trauma. J. Feline Med. Surg. 2019, 21, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Knight, R.; Meeson, R.L. Feline head trauma: A CT analysis of skull fractures and their management in 75 cats. J. Feline Med. Surg. 2018, 21, 1120–1126. [Google Scholar] [CrossRef]
- Kleftouri, S.; Panagopoulou, E.; Kouki, M.T.; Papadimitriou, S.A. Fractures of the mandible in cats. Retrospective study of 23 cases. Hell. J. Companion Anim. Med. 2017, 6, 20–28. [Google Scholar]
- Higgins, B. Fractures of the mandible. In Proceedings of the World Small Animal Veterinary Association 38th World Congress, Auckland, New Zealand, 21–24 March 2013. [Google Scholar]
- German, A. Upper and Lower Jaw Fracture in Cats. PetMD. Available online: https://www.petmd.com/cat/conditions/mouth/c_ct_upper_lower_jaw_fracture (accessed on 9 September 2020).
- Umphlet, R.C.; Johnson, A.L. Mandibular Fractures in the Cat. A Retrospective Study. Veter. Surg. 1988, 17, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Umphlet, R.C.; Johnson, A.L. Mandibular Fractures in the Dog. A Retrospective Study of 157 Cases. Veter. Surg. 1990, 19, 272–275. [Google Scholar] [CrossRef] [PubMed]
- Little, S. Dental and Oral Diseases. In The Cat: Medicine and Management; Elsevier-Saunders: Amsterdam, The Netherlands, 2012; pp. 329–370. ISBN 978-1-4377-0660-4. [Google Scholar]
- Colmery, B.H.; Hale, F.A.; Hoffman, S.L.; Johnston, N.W.; Kuntsi-Vaattovaara, H.; Reiter, A.M. Concern about dental trauma after invasive jaw fracture repair. J. Small Anim. Pract. 2011, 52, 448–449. [Google Scholar] [CrossRef]
- Steenkamp, G. Non-Invasive fracture repair techniques in dogs and cats. In Proceedings of the World Small Animal Veterinary Association, Cape Town, South Africa, 16–19 September 2014. [Google Scholar]
- Lobprise, H.; Dodd, J.R. Wiggs’s Veterinary Dentistry, 2nd ed.; Willey-Blackwell: Hoboken, NJ, USA, 2019; ISBN 9781118816165. [Google Scholar]
- Southerden, P.; Haydock, R.M.; Barnes, D.M. Three Dimensional Osteometric Analysis of Mandibular Symmetry and Morphological Consistency in Cats. Front. Veter. Sci. 2018, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Spodnick, G.J.; Boudrieau, R.J. Mandible: Anatomy, Biomechanical Principles, Surgical Approaches. In Proceedings of the Operative treatment of Veterinary CMF Trauma & Reconstruction, Las Vegas, NV, USA, 22–24 January 2018; pp. 47–52. [Google Scholar]
- Lemmons, M. Clinical Feline Dental Radiography. Veter. Clin. N. Am. Small Anim. Prac. 2013, 43, 533–554. [Google Scholar] [CrossRef] [PubMed]
- Reiter, A.M.; Soltero-Rivera, M.M. Applied Feline Oral Anatomy and Tooth Extraction Techniques. J. Feline Med. Surg. 2014, 16, 900–913. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.L. Increased Number of Iatrogenic Jaw Fractures. AVMA PLIT 2015, 34, 3–4. Available online: https://www.im3vet.com/iM3US/media/Documents/professional_liability_Dental_X-ray.pdf (accessed on 2 March 2021).
- Bellows, J. The ABCs of Veterinary Dentistry: “J” Is for Jaw Fractures. 2017. Available online: https://www.dvm360.com/view/abcs-veterinary-dentistry-j-jaw-fractures (accessed on 9 September 2020).
- Milella, L.; Smithson, A. Radiology: Dental. Felis. Available online: www.vetstream.com/treat/felis/freeform/radiology-dental (accessed on 13 November 2020).
- Niemiec, B.A. Feline dental radiography and radiology. J. Feline Med. Surg. 2014, 16, 887–899. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.L.; Kressin, D.J.; Verstraete, F.J.M. Myths and misconceptions in veterinary dentistry. J. Am. Veter. Med. Assoc. 2007, 231, 1818–1824. [Google Scholar] [CrossRef]
- Lantz, G.C. Interarcade wiring as a method of fixation for selected mandibular injuries. J. Am. Anim. Hosp. Assoc. 1981, 17, 599–603. [Google Scholar]
- Woodbridge, N.; Owen, M. Feline Mandibular Fractures. J. Feline Med. Surg. 2013, 15, 211–218. [Google Scholar] [CrossRef]
- Clinician’s Brief. Considerations for Feline Mandibular Fractures. Available online: https://www.cliniciansbrief.com/article/considerations-feline-mandibular-fractures (accessed on 31 November 2020).
- Greiner, C.L.; Verstraete, F.J.M.; Stover, S.M.; Garcia, T.C.; Leale, D.; Arzi, B. Biomechanical evaluation of two plating configurations for fixation of a simple transverse caudal mandibular fracture model in cats. Am. J. Veter. Res. 2017, 78, 702–711. [Google Scholar] [CrossRef] [Green Version]
- Misch, C.E.; Resnik, R. Mandibular Nerve Neurosensory Impairment after Dental Implant Surgery: Management and Protocol. Implant. Dent. 2010, 19, 378–386. [Google Scholar] [CrossRef]
- Gobel, S.; Binck, J.M. Degenerative changes in primary trigeminal axons and in neurons in nucleus caudalis following tooth pulp extirpations in the cat. Brain Res. 1977, 132, 347–354. [Google Scholar] [CrossRef]
- Niemann, G. Cálculo de la resistencia. In Tratado Teórico-Práctico de Elementos de Máquinas; Editorial Labor, S.A.: Barcelona, Spain, 1973; Volume 1, pp. 46–79. ISBN 84-335-6287-8. [Google Scholar]
- Ow, A.; Tan, W.; Pienkowski, L. Mandibular Reconstruction Using a Custom-Made Titanium Prosthesis: A Case Report on the Use of Virtual Surgical Planning and Computer-Aided Design/Computer-Aided Manufacturing. Craniomaxillofacial Trauma Reconstr. 2016, 9, 246–250. [Google Scholar] [CrossRef] [Green Version]
- Heney, C.M.; Arzi, B.; Kass, P.H.; Hatcher, D.C.; Verstraete, F.J.M. The Diagnostic Yield of Dental Radiography and Cone-Beam Computed Tomography for the Identification of Dentoalveolar Lesions in Cats. Front. Vet. Sci. 2019, 6, 1–15. [Google Scholar] [CrossRef]
- Liptak, J.M.; Thatcher, G.P.; Bray, J.P. Reconstruction of a mandibular segmental defect with a customized 3-dimensional–printed titanium prosthesis in a cat with a mandibular osteosarcoma. J. Am. Veter. Med. Assoc. 2017, 250, 900–908. [Google Scholar] [CrossRef] [Green Version]
- Northrup, N.C.; Selting, K.A.; Rassnick, K.M.; Kristal, O.; O’Brien, M.G.; Dank, G.; Dhaliwal, R.S.; Jagannatha, S.; Cornell, K.K.; Gieger, T.L. Outcomes of Cats With Oral Tumors Treated With Mandibulectomy: 42 Cases. J. Am. Anim. Hosp. Assoc. 2006, 42, 350–360. [Google Scholar] [CrossRef]
- Vaughan, D. 3-Dimensional printing in veterinary medicine. Am. Vet. Crit. News Expert. Insights Anim. Health Med. 2018, 3, 19–23. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Incidence (%) | Cause | Treatment Methods | Pay Special Attention to… | |
| Mandibular fractures in general | 11–23 [4] 14,5 [10] | → Road traffic accidents, fighting injuries, falls from heights, human abuse [4,5,6,7]. → Secondary to neoplasia, metabolic disease, and dental treatment [8]. | → A non-invasive treatment should be considered first [13]. → In multiple fractures, repair the mandible from caudal to rostral [17]. | → The naturally contaminated environment of the oral cavity. → Not damaging teeth and tooth roots. → Keep the integrity of the neurovascular supply in the mandibular canal. → Multiple or open fractures cause more complications [10]. → Infection and persistent periodontal disease can lead to osteomyelitis and non-union of fracture fragments [15]. |
| Mandibular Fracture Types | Incidence (%) [10] | Treatment Methods | Clinical Union (Weeks) [10] | Pay Special Attention to… Recommendations |
| Symphyseal | 73.3 | → Cerclage wire [4,15,26]. | 6 (3–12) | → Be sure that the incisor teeth remain in alignment; otherwise, step defects can be generated [15]. |
| Parasymphyseal | → Osseous circumferential wiring [15]. | → Fracture is often non-displaced [19]. → Possibility of iatrogenic fracture after canine extraction when pre-existing periodontal disease, insufficient preparation prior to extraction or use of excessive force, or a combination [12,15,19]. → Do two radiographies: before and after dental extraction [20]. → Inform the client in advance that iatrogenic fracture is a possibility after canine extraction [20]. | ||
| Body | 16.0 | → Simple fractures (fracture line is perpendicular to the long axis of the mandible): internal fixation with interfragmentary wires [26]. → Oblique fractures: ◆ Favourable (mastication muscles compress the bone fragments, relatively stable): Conservative methods are enough to get stabilization of the tension surface [15,21]. ◆ Unfavourable (mastication muscles distract bone fragments): (A) Two intraosseus wires (one dorsally and the other ventrally) between the two fragments [15]; (B) Triangular method (two wires caudally to the fracture in a 90° angle to reach the same rostral hole [15]; (C) Internal fixation with conventional bone miniplates and screws [8,16]. → Open or comminuted fractures: external fixation with pins and mandibular bumper bar [26]. | 10 (8–16) | → Keep the integrity of the neurovascular supply in the mandibular canal. → Avoid damaging the roots and periodontal ligament of the teeth [4,15]. → In-line tooth removal is not advised unless the teeth involved are fractured [8,17]. → Do postoperative radiographs, especially when severe periodontitis or other debilitating mandibular bone pathologies [19]. → The wiring must be placed so that its acts as a tension band to create interfragmentary compression [8]. → The most common complications of surgical repair are malocclusion and osteomyelitis [8]. → Ventral approach facilitates exposure, bone fragment reduction and stabilization [17]. → Use bone plates and screws in accordance with the cat mandibular size. |
| Ramus: | ||||
| Condylar process | 6.7 | → Simple fractures heal by themselves as a functional and painless nonunion [3]. | 6 (4–8) | → Comminuted fractures could generate TMJ ankylosis in young cats [3]. |
| Coronoid process | 4.0 | → A non-invasive treatment should be considered first [13]. | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardero, M.; López-Lombardero, M.; Alonso-Peñarando, D.; Yllera, M.d.M. The Cat Mandible (II): Manipulation of the Jaw, with a New Prosthesis Proposal, to Avoid Iatrogenic Complications. Animals 2021, 11, 683. https://doi.org/10.3390/ani11030683
Lombardero M, López-Lombardero M, Alonso-Peñarando D, Yllera MdM. The Cat Mandible (II): Manipulation of the Jaw, with a New Prosthesis Proposal, to Avoid Iatrogenic Complications. Animals. 2021; 11(3):683. https://doi.org/10.3390/ani11030683
Chicago/Turabian StyleLombardero, Matilde, Mario López-Lombardero, Diana Alonso-Peñarando, and María del Mar Yllera. 2021. "The Cat Mandible (II): Manipulation of the Jaw, with a New Prosthesis Proposal, to Avoid Iatrogenic Complications" Animals 11, no. 3: 683. https://doi.org/10.3390/ani11030683