
Prospective Study in Children with Complicated Urinary Tract Infection Treated with Autologous Bacterial Lysates

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Study Population
2.1.2. Biological Samples
2.1.3. Bacterial Culture
2.1.4. Serotyping of E. coli Isolates
2.1.5. Autologous Bacterial Lysate (ABL)
3. Results
3.1. Clinical Characteristics of the Patients
3.2. Urinalysis
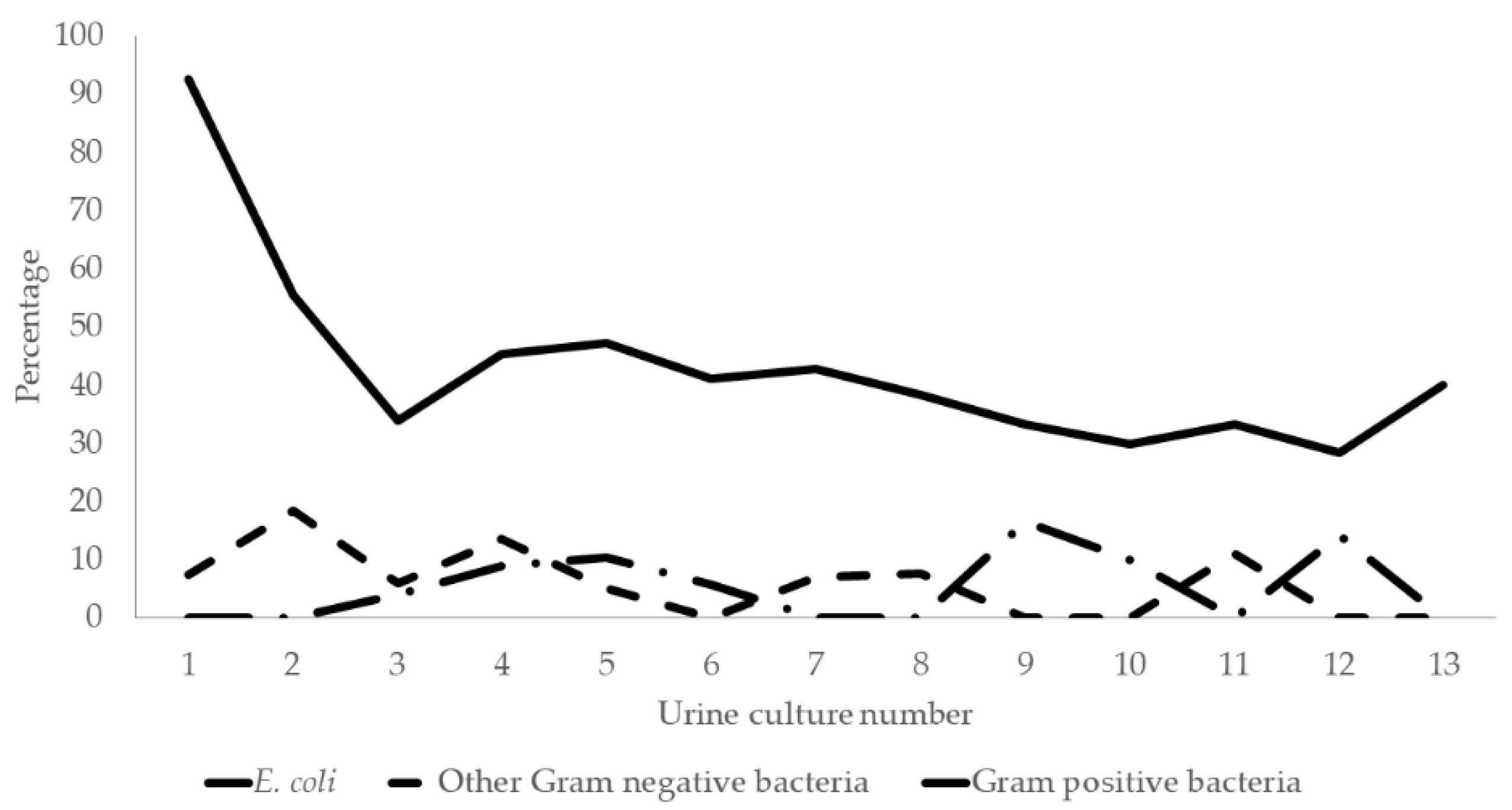
3.3. UTI Etiology
3.4. E. coli Serotyping
3.5. Reinfections and Persistence
3.6. E. coli Strains Recovered from Feces
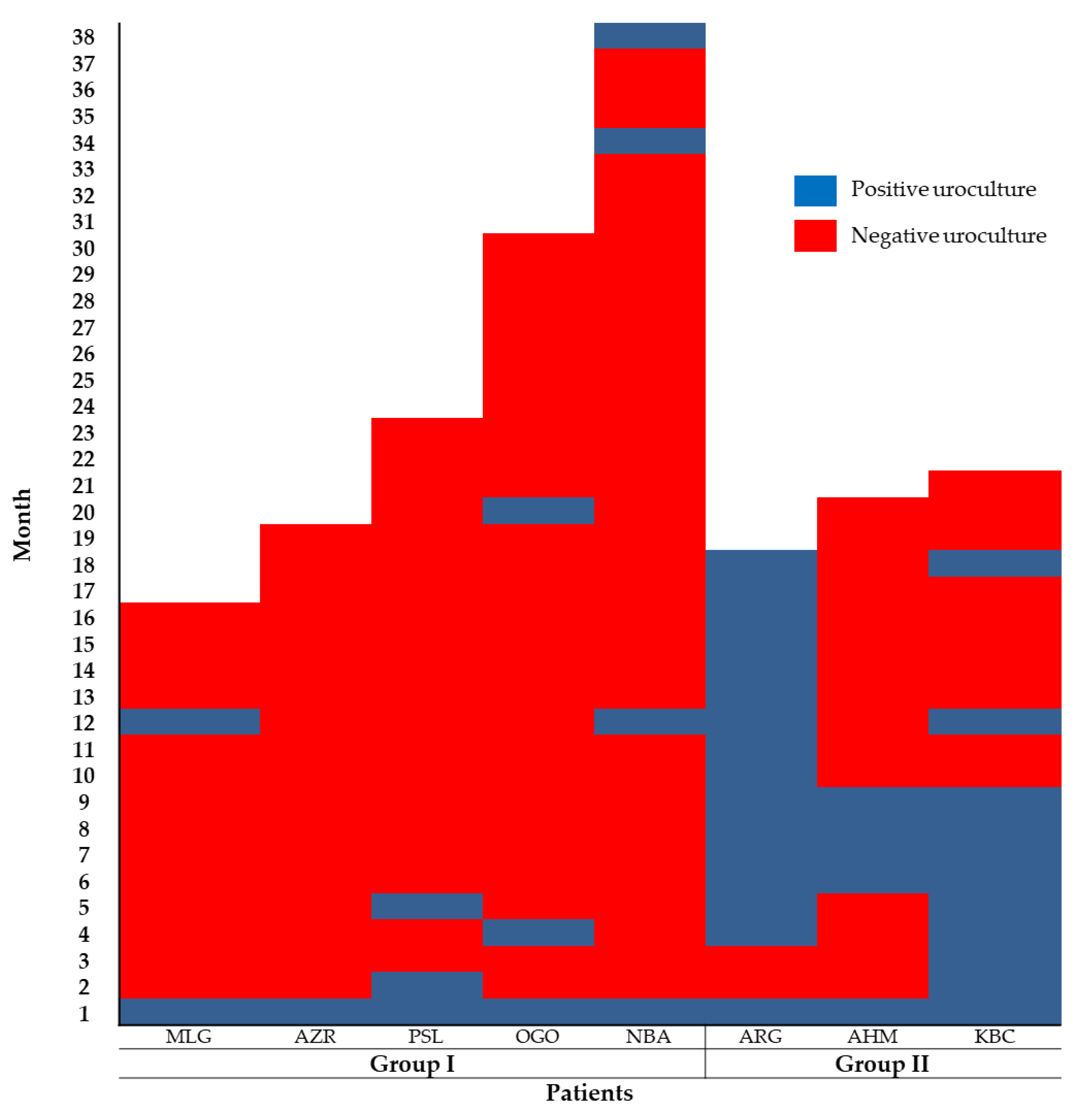
3.7. Effect of the Autologous Bacterial Lysates (ABL) in Children with Complicated UTI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tullus, K.; Shaikh, N. Urinary tract infections in children. Lancet 2020, 395, 1659–1668. [Google Scholar] [CrossRef]
- Khan, A.; Jhaveri, R.; Seed, P.C.; Arshad, M. Update on Associated Risk Factors, Diagnosis, and Management of Recurrent Urinary Tract Infections in Children. J. Pediatr. Infect. Dis. Soc. 2019, 8, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Millner, R.; Becknell, B. Urinary Tract Infections. Pediatr. Clin. 2019, 66, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Asadi Karam, M.R.; Habibi, M.; Bouzari, S. Urinary tract infection: Pathogenicity, antibiotic resistance and development of effective vaccines against Uropathogenic Escherichia coli. Mol. Immunol. 2019, 108, 56–67. [Google Scholar] [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, E.A.; Mak, R.H. Urinary tract infection in pediatrics: An overview. J. Pediatr. 2020, 96, 65–79. [Google Scholar] [CrossRef]
- Russo, T.A.; Johnson, J.R. Proposal for a New Inclusive Designation for Extraintestinal Pathogenic Isolates of Escherichia coli: ExPEC. J. Infect. Dis. 2000, 181, 1753–1754. [Google Scholar] [CrossRef] [Green Version]
- Kaper, J.B.; Nataro, J.P.; Mobley, H.L.T. Pathogenic Escherichia coli. Nat. Rev. Microbiol. 2004, 2, 123–140. [Google Scholar] [CrossRef]
- Ejrnæs, K. Bacterial characteristics of importance for recurrent urinary tract infections caused by Escherichia coli. Dan. Med. Bull. 2011, 58, B4187. [Google Scholar]
- Blango, M.G.; Mulvey, M.A. Persistence of Uropathogenic Escherichia coli in the Face of Multiple Antibiotics. Antimicrob. Agents Chemother. 2010, 54, 1855–1863. [Google Scholar] [CrossRef] [Green Version]
- Mulvey, M.A.; Schilling, J.D.; Martinez, J.J.; Hultgren, S.J. Bad bugs and beleaguered bladders: Interplay between uropathogenic Escherichia coli and innate host defenses. Proc. Natl. Acad. Sci. USA 2000, 97, 8829–8835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noie Oskouie, A.; Hasani, A.; Ahangarzadeh Rezaee, M.; Soroush Bar Haghi, M.H.; Hasani, A.; Soltani, E. A Relationship Between O-Serotype, Antibiotic Susceptibility and Biofilm Formation in Uropathogenic Escherichia coli. Microb. Drug Resist. 2019, 25, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Shokouhi Mostafavi, S.K.; Najar-Peerayeh, S.; Mohabbati Mobarez, A.; Kardoust Parizi, M. Serogroup distribution, diversity of exotoxin gene profiles, and phylogenetic grouping of CTX-M-1- producing uropathogenic Escherichia coli. Comp. Immunol. Microbiol. Infect. Dis. 2019, 65, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Zhang, D.; Ye, Z.; Zhu, X.; Yang, W.; Dong, L.; Gao, S.; Liu, X. Virulence traits and pathogenicity of uropathogenic Escherichia coli isolates with common and uncommon O serotypes. Microb. Pathog. 2017, 104, 217–224. [Google Scholar] [CrossRef]
- Terai, A.; Yamamoto, S.; Mitsumori, K.; Okada, Y.; Kurazono, H.; Takeda, Y.; Yoshida, O. Escherichia coli Virulence Factors and Serotypes in Acute Bacterial Prostatitis. Int. J. Urol. 1997, 4, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Bidet, P.; Mahjoub-Messai, F.; Blanco, J.; Blanco, J.; Dehem, M.; Aujard, Y.; Bingen, E.; Bonacorsi, S. Combined Multilocus Sequence Typing and O Serogrouping Distinguishes Escherichia coli Subtypes Associated with Infant Urosepsis and/or Meningitis. J. Infect. Dis. 2007, 196, 297–303. [Google Scholar] [CrossRef] [Green Version]
- Dason, S.; Dason, J.T.; Kapoor, A. Guidelines for the diagnosis and management of recurrent urinary tract infection in women. Can. Urol. Assoc. J. 2011, 5, 316–322. [Google Scholar] [CrossRef]
- Malik, R.D.; Wu, Y.R.; Zimmern, P.E. Definition of Recurrent Urinary Tract Infections in Women: Which One to Adopt? Female Pelvic Med. Reconstr. Surg. 2018, 24, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Bader, M.S.; Loeb, M.; Brooks, A.A. An update on the management of urinary tract infections in the era of antimicrobial resistance. Postgrad. Med. 2017, 129, 242–258. [Google Scholar] [CrossRef]
- Behzadi, P.; Urbán, E.; Matuz, M.; Benkő, R.; Gajdács, M. The Role of Gram-Negative Bacteria in Urinary Tract Infections: Current Concepts and Therapeutic Options. In SpringerLink; Springer: New York, NY, USA, 2020; pp. 1–35. [Google Scholar]
- Buettcher, M.; Trueck, J.; Niederer-Loher, A.; Heininger, U.; Agyeman, P.; Asner, S.; Berger, C.; Bielicki, J.; Kahlert, C.; Kottanattu, L.; et al. Swiss consensus recommendations on urinary tract infections in children. Eur. J. Pediatr. 2020, 180, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Schmidhammer, S.; Ramoner, R.; Höltl, L.; Bartsch, G.; Thurnher, M.; Zelle-Rieser, C. An Escherichia coli-based oral vaccine against urinary tract infections potently activates human dendritic cells. Urology 2002, 60, 521–526. [Google Scholar] [CrossRef]
- Hopkins, W.J.; Elkahwaji, J.; Beierle, L.M.; Leverson, G.E.; Uehling, D.T. Vaginal Mucosal Vaccine for Recurrent Urinary Tract Infections in Women: Results of a Phase 2 Clinical Trial. J. Urol. 2007, 177, 1349–1353. [Google Scholar] [CrossRef] [PubMed]
- Brumbaugh, A.R.; Mobley, H.L. Preventing urinary tract infection: Progress toward an effective Escherichia coli vaccine. Expert Rev. Vaccines 2012, 11, 663–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prattley, S.; Geraghty, R.; Moore, M.; Somani, B.K. Role of Vaccines for Recurrent Urinary Tract Infections: A Systematic Review. Eur. Urol. Focus 2020, 6, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Billips, B.K.; Yaggie, R.E.; Cashy, J.P.; Schaeffer, A.J.; Klumpp, D.J. A Live-Attenuated Vaccine for the Treatment of Urinary Tract Infection by Uropathogenic Escherichia coli. J. Infect. Dis. 2009, 200, 263–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivick, K.E.; Mobley, H.L.T. Waging War against Uropathogenic Escherichia coli: Winning Back the Urinary Tract. Infect. Immun. 2010, 78, 568–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aziminia, N.; Hadjipavlou, M.; Philippou, Y.; Pandian, S.S.; Malde, S.; Hammadeh, M.Y. Vaccines for the prevention of recurrent urinary tract infections: A systematic review. BJU Int. 2019, 123, 753–768. [Google Scholar] [CrossRef] [Green Version]
- Huber, M.; Baier, W.; Serr, A.; Bessler, W. Immunogenicity of an E. coli extract after oral or intraperitoneal administration: Induction of antibodies against pathogenic bacterial strains. Int. J. Immunopharmacol. 2000, 22, 57–68. [Google Scholar] [CrossRef]
- Bauer, H.W.; Rahlfs, V.W.; Lauener, P.A.; Blessmann, G.S.S. Prevention of recurrent urinary tract infections with immuno-active E. coli fractions: A meta-analysis of five placebo-controlled double-blind studies. Int. J. Antimicrob. Agents 2002, 19, 451–456. [Google Scholar] [CrossRef]
- Taha Neto, K.A.; Nogueira Castilho, L.; Reis, L.O. Vacuna oral (OM-89) en la profilaxis de infección urinaria recurrente: Una revisión sistemática realista con metaanálisis. Actas Urol. Esp. 2016, 40, 203–208. [Google Scholar] [CrossRef]
- Cazzola, M.; Anapurapu, S.; Page, C.P. Polyvalent mechanical bacterial lysate for the prevention of recurrent respiratory infections: A meta-analysis. Pulm. Pharmacol. Ther. 2011, 25, 62–68. [Google Scholar] [CrossRef]
- Ahumada-Cota, R.E.; Hernandez-Chiñas, U.; Milián-Suazo, F.; Chávez-Berrocal, M.E.; Navarro-Ocaña, A.; Martínez-Gómez, D.; Patiño-López, G.; Salazar-Jiménez, E.P.; Eslava, C.A. Effect and Analysis of Bacterial Lysates for the Treatment of Recurrent Urinary Tract Infections in Adults. Pathogens 2020, 9, 102. [Google Scholar] [CrossRef] [Green Version]
- LaRocco, M.T.; Franek, J.; Leibach, E.K.; Weissfeld, A.S.; Kraft, C.S.; Sautter, R.L.; Baselski, V.; Rodahl, D.; Peterson, E.J.; Cornish, N.E. Effectiveness of Preanalytic Practices on Contamination and Diagnostic Accuracy of Urine Cultures: A Laboratory Medicine Best Practices Systematic Review and Meta-analysis. Clin. Microbiol. Rev. 2016, 29, 105–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, M.L.; Gaido, L. Laboratory Diagnosis of Urinary Tract Infections in Adult Patients. Clin. Infect. Dis. 2004, 38, 1150–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrow, G.I.; Feltham, R.K.A. Characters of Gram-negative bacteria. In Cowan and Steel’s Manual for the Identification of Medical Bacteria; Cambridge Uniersity Press: Cambridge, UK, 1993; pp. 94–164. ISBN 978-0-511-52710-4. [Google Scholar]
- Orskov, F.; Orskov, I. Escherichia coli serotyping and disease in man and animals. Can. J. Microbiol. 1992, 38, 699–704. [Google Scholar] [CrossRef]
- Tewary, K.; Narchi, H. Recurrent urinary tract infections in children: Preventive interventions other than prophylactic antibiotics. World J. Methodol. 2015, 5, 13–19. [Google Scholar] [CrossRef]
- Vosti, K.L. A prospective, longitudinal study of the behavior of serologically classified isolates of Escherichia coli in women with recurrent urinary tract infections. J. Infect. 2007, 55, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Magruder, M.; Sholi, A.N.; Gong, C.; Zhang, L.; Edusei, E.; Huang, J.; Albakry, S.; Satlin, M.J.; Westblade, L.F.; Crawford, C.; et al. Gut uropathogen abundance is a risk factor for development of bacteriuria and urinary tract infection. Nat. Commun. 2019, 10, 1–9. [Google Scholar] [CrossRef]
- Matsui, Y.; Hu, Y.; Rubin, J.; de Assis, R.S.; Suh, J.; Riley, L.W. Multilocus sequence typing of Escherichia coli isolates from urinary tract infection patients and from fecal samples of healthy subjects in a college community. MicrobiologyOpen 2020, 9, e1032. [Google Scholar] [CrossRef] [Green Version]
- Paniagua-Contreras, G.L.; Monroy-Pérez, E.; Rodríguez Moctezuma, J.R. Virulence factors, antibiotic resistance phenotypes and O-serogroups of Escherichia coli strains isolated from community-acquired urinary tract infection patients in Mexico. J. Microbiol. Immunol. Infect. 2017, 50, 478–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández-Chiñas, U.; Pérez-Ramos, A.; Belmont-Monroy, L.; Chávez-Berrocal, M.E.; González-Villalobos, E.; Navarro-Ocaña, A.; Eslava, C.A.; Molina-Lopez, J. Characterization of auto-agglutinating and non-typeable uropathogenic Escherichia coli strains. J. Infect. Dev. Ctries. 2019, 13, 465–472. [Google Scholar] [CrossRef]
- Sharma, S.; Kaur, N.; Malhotra, S.; Madan, P.; Ahmad, W.; Hans, C. Serotyping and Antimicrobial Susceptibility Pattern of Escherichia coli Isolates from Urinary Tract Infections in Pediatric Population in a Tertiary Care Hospital. J. Pathog. 2016, 2016, 2548517. [Google Scholar] [CrossRef] [Green Version]
- Aragón, I.M.; Herrera-Imbroda, B.; Queipo-Ortuño, M.I.; Castillo, E.; Moral, J.S.-G.D.; Gómez-Millán, J.; Yucel, G.; Lara, M.F. The Urinary Tract Microbiome in Health and Disease. Eur. Urol. Focus 2018, 4, 128–138. [Google Scholar] [CrossRef]
- Duriez, P.; Clermont, O.; Bonacorsi, S.; Bingen, E.; Chaventré, A.; Elion, J.; Picard, B.; Denamur, E. Commensal Escherichia coli isolates are phylogenetically distributed among geographically distinct human populations. Microbiology 2001, 147, 1671–1676. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.; Li, Z.; Chen, W.; Rong, T.; Wang, G.; Ma, X. Microbiome-Metabolomics Analysis Investigating the Impacts of Dietary Starch Types on the Composition and Metabolism of Colonic Microbiota in Finishing Pigs. Front. Microbiol. 2019, 10, 1143. [Google Scholar] [CrossRef] [Green Version]
- Lindstedt, B.-A.; Finton, M.D.; Porcellato, D.; Brandal, L.T. High frequency of hybrid Escherichia coli strains with combined Intestinal Pathogenic Escherichia coli (IPEC) and Extraintestinal Pathogenic Escherichia coli (ExPEC) virulence factors isolated from human faecal samples. BMC Infect. Dis. 2018, 18, 544. [Google Scholar] [CrossRef]
- Schwenger, E.M.; Tejani, A.M.; Loewen, P.S. Probiotics for preventing urinary tract infections in adults and children. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- O’Brien, V.P.; Hannan, T.J.; Nielsen, H.V.; Hultgren, S.J. Drug and Vaccine Development for the Treatment and Prevention of Urinary Tract Infections. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, A.K.C.; Wong, A.H.C.; Leung, A.A.M.; Hon, K.L. Urinary Tract Infection in Children. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 2–18. [Google Scholar] [CrossRef]
- Brodie, A.; El-Taji, O.; Jour, I.; Foley, C.; Hanbury, D. A Retrospective Study of Immunotherapy Treatment with Uro-Vaxom (OM-89®) for Prophylaxis of Recurrent Urinary Tract Infections. Curr. Urol. 2020, 14, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, V. Effect of a Bacterial Extract on Cellular and Humoral Immiine Responses in Humans. Immunopharmacol. Immunotoxicol. 1986, 8, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Naber, K.G.; Cho, Y.-H.; Matsumoto, T.; Schaeffer, A.J. Immunoactive prophylaxis of recurrent urinary tract infections: A meta-analysis. Int. J. Antimicrob. Agents 2009, 33, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.A.; Sidjabat, H.E.; Paterson, D.L. Escherichia coli O25b-ST131: A pandemic, multiresistant, community-associated strain. J. Antimicrob. Chemother. 2011, 66, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrios-Villa, E.; Cortés-Cortés, G.; Lozano-Zaraín, P.; de la Paz Arenas, M.M.; de la Peña, C.F.; Martínez-Laguna, Y.; Torres, C.; del Carmen Rocha-Gracia, R. Adherent/invasive Escherichia coli (AIEC) isolates from asymptomatic people: New E. coli ST131 O25:H4/H30-Rx virotypes. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nimmich, W.; Voigt, W.; Seltmann, G. Characterization of urinary Escherichia coli O75 strains. J. Clin. Microbiol. 1997, 35, 1112–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| UPEC Classification | Serogroup ‡ | No. of Patients * | No. of Isolates * | n (%) |
|---|---|---|---|---|
| Classic | O25 | 6 | 160 | 440 (41.7) |
| O1 and O75 * | 3 | 130 | ||
| O8 and O9 * | 2 | 100 | ||
| O2, O4, O6 and O7 | 1 | 50 | ||
| Non-classic | O11, O17 and O102 | 3 | 75 | 380 (36) |
| O57, O96 and O170 | 2 | 65 | ||
| O12. O20, O23, O29, O32, O35, O45, O49, O73, O100, O101, O105, O109, O124, O144, O147, O153, O154, O164, O174, O178, O49766 and O684474 | 1 | 240 | ||
| Non-Typeable | OND ‡ | 7 | 165 | 235 (22.3) |
| OR ‡ | 6 | 70 |
| Patients | Urine Cultures | Serotypes (No. of Isolated Bacteria) | Stool Cultures | Serotype (No. of Isolated Bacteria) |
|---|---|---|---|---|
| NBA | 5 | O45:NM (10), O35:H10 (10), O64474:HNM (10), O96:H16 (8), OR:HNM (2) and O105:H18 (10) | 1 | O6:H1 (8) * |
| ARV | 2 | O11:H25 (10), O23:HNM (6) and O7:H4 (4) | 1 | O7:H4 (2) *, OND:NM (3) *, O1:H6 (2) * |
| VR | 2 | O4:H5 (10) and OR:H15 (10) | 2 | O169:H ND (4), O4:H5 (2) *, O45:HNM (1) ‡, O157:HND (3), OND:NM (3) and O138:H34 (1) |
| AMR | 2 | O25:H4 (12) and O17:H18(8) | 1 | O48:HND (8) |
| RMR | 7 | O25:H4 (70) | 3 | OND:H16 (2), OND:HND (1), O89:H38(1), O25:H4 (8) *, O25:H10 (1), O29:H10 (1), O51:HND (3) *, OR:HNM (2) and O129:H30 (1) |
| AA | 12 | O75:HNM (90) | 1 | O28ab:H7 (2), O34:NM (1) *, O8:H7 (5) *, O20:H30 (1) ‡ |
| OGO | 14 | O170:HNM (10) and O25:H4 (10) | 2 | O3:H14 (1), O18ac:H14 (2), O21:H14 (1), O128ab:H5 (2), O154:H4 (1), O164:HNM (1) ‡‡, O128ac:HNM (1), OND:HNM (3), OR:HNM (1), O76:HNM (1) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Chiñas, U.; Chávez-Berrocal, M.E.; Ahumada-Cota, R.E.; Navarro-Ocaña, A.; Rocha-Ramírez, L.M.; Pérez-del Mazo, Y.; Alvarado-Cabello, M.; Pérez-Soto, G.; León-Alamilla, L.A.; Acevedo-Monroy, S.E.; et al. Prospective Study in Children with Complicated Urinary Tract Infection Treated with Autologous Bacterial Lysates. Microorganisms 2021, 9, 1811. https://doi.org/10.3390/microorganisms9091811
Hernández-Chiñas U, Chávez-Berrocal ME, Ahumada-Cota RE, Navarro-Ocaña A, Rocha-Ramírez LM, Pérez-del Mazo Y, Alvarado-Cabello M, Pérez-Soto G, León-Alamilla LA, Acevedo-Monroy SE, et al. Prospective Study in Children with Complicated Urinary Tract Infection Treated with Autologous Bacterial Lysates. Microorganisms. 2021; 9(9):1811. https://doi.org/10.3390/microorganisms9091811
Chicago/Turabian StyleHernández-Chiñas, Ulises, María E. Chávez-Berrocal, Ricardo E. Ahumada-Cota, Armando Navarro-Ocaña, Luz M. Rocha-Ramírez, Yolanda Pérez-del Mazo, Maribel Alvarado-Cabello, Gabriel Pérez-Soto, Luis A. León-Alamilla, Salvador E. Acevedo-Monroy, and et al. 2021. "Prospective Study in Children with Complicated Urinary Tract Infection Treated with Autologous Bacterial Lysates" Microorganisms 9, no. 9: 1811. https://doi.org/10.3390/microorganisms9091811