
The Risk of Invasive Pneumococcal Disease Differs between Risk Groups in Norway Following Widespread Use of the 13-Valent Pneumococcal Vaccine in Children

Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Changes in IPD Incidence Rates and Estimates of Indirect Effects
2.3. The Relative Effects of Age and Medical Conditions on the Risk of IPD
3. Results
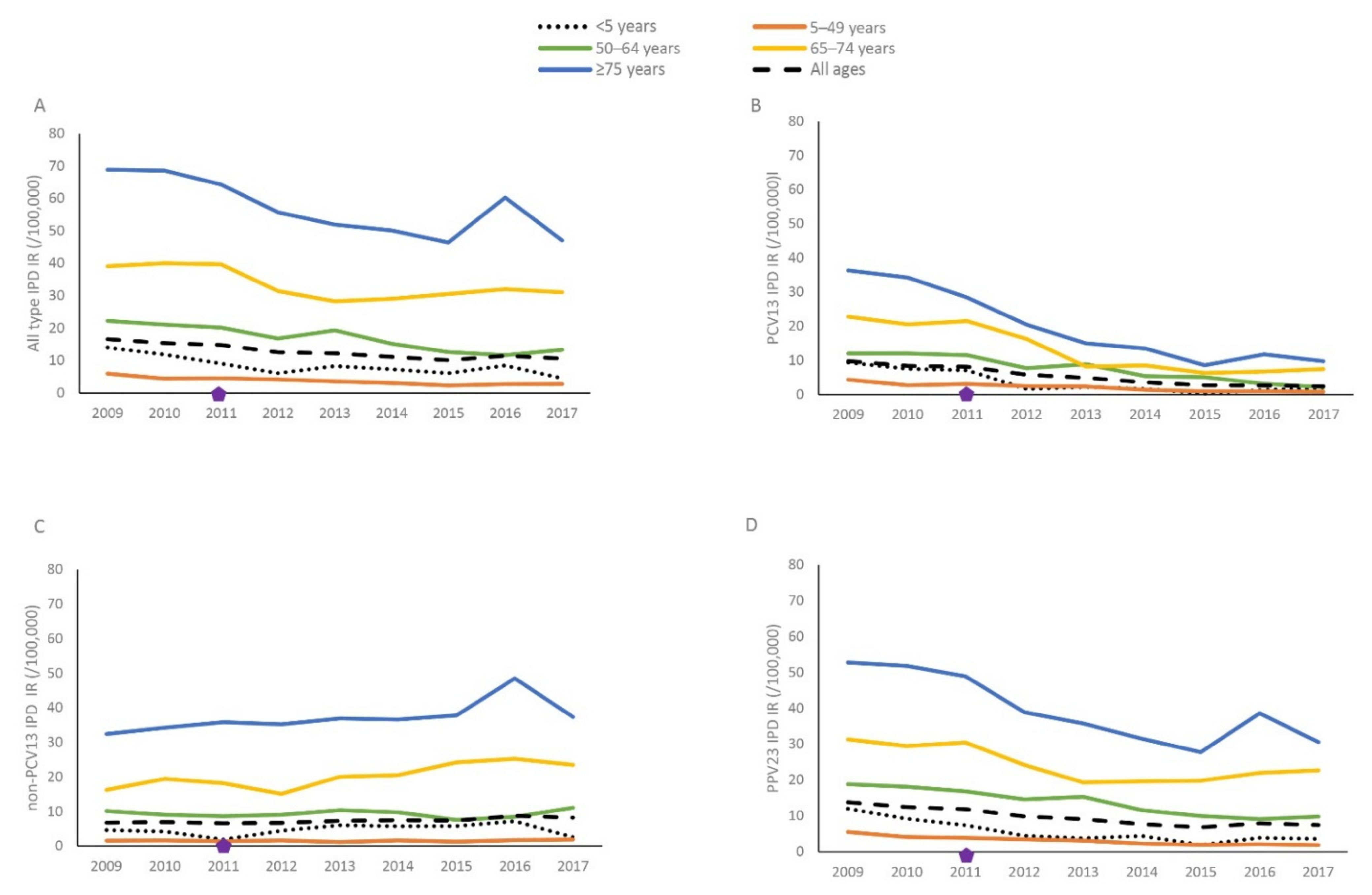
3.1. Changes in Age Group-, Vaccine Type- and Medical Risk Group-Specific IPD Incidence Rates over Time
3.2. Relative Risk of IPD in Medical Risk Groups Compared to Those with No Risk by Age Group
3.3. Serotype-Specific IPD in Medical Risk Groups 2015–2017
4. Discussion
4.1. Incidence Rate by Age and Vaccine-Type IPD
4.2. Indirect Effect in Groups with and without Medical Risk Factors
4.3. Risk of IPD in Medical Risk Groups
4.4. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shiri, T.; Datta, S.; Madan, J.; Tsertsvadze, A.; Royle, P.; Keeling, M.J.; McCarthy, N.D.; Petrou, S. Indirect effects of childhood pneumococcal conjugate vaccination on invasive pneumococcal disease: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e51–e59. [Google Scholar] [CrossRef] [Green Version]
- Savulescu, C.; Krizova, P.; Lepoutre, A.; Mereckiene, J.; Vestrheim, D.F.; Ciruela, P.; Ordobas, M.; Guevara, M.; McDonald, E.; Morfeldt, E.; et al. Effect of high-valency pneumococcal conjugate vaccines on invasive pneumococcal disease in children in SpIDnet countries: An observational multicentre study. Lancet Respir. Med. 2017, 5, 648–656. [Google Scholar] [CrossRef] [Green Version]
- Muhammad, R.D.; Oza-Frank, R.; Zell, E.; Link-Gelles, R.; Narayan, K.M.; Schaffner, W.; Thomas, A.; Lexau, C.; Bennett, N.M.; Farley, M.M.; et al. Epidemiology of invasive pneumococcal disease among high-risk adults since the introduction of pneumococcal conjugate vaccine for children. Clin. Infect Dis. 2013, 56, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Van Deursen, A.M.M.; van Mens, S.P.; Sanders, E.A.; Vlaminckx, B.J.; De Melker, H.E.; Schouls, L.M.; de Greeff, S.C.; van der Ende, A. Invasive pneumococcal disease and 7-valent pneumococcal conjugate vaccine, the Netherlands. Emerg. Infect. Dis. 2012, 18, 1729. [Google Scholar] [CrossRef]
- Van Hoek, A.J.; Andrews, N.; Waight, P.A.; Stowe, J.; Gates, P.; George, R.; Miller, E. The effect of underlying clinical conditions on the risk of developing invasive pneumococcal disease among hospitalised patients in England. J. Infect. 2012, 65, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Cabaj, J.L.; Nettel-Aguirre, A.; MacDonald, J.; Vanderkooi, O.G.; Kellner, J.D. Influence of childhood pneumococcal conjugate vaccines on invasive pneumococcal disease in adults with underlying comorbidities in Calgary, Alberta (2000–2013). Clin. Infect Dis. 2016, 62, 1521–1526. [Google Scholar] [CrossRef] [Green Version]
- Cohen, R.; Varon, E.; Bechet, S.; Bonacorsi, S.; Levy, C. Comparative impact of pneumococcal conjugate vaccines on pneumococcal meningitis according to underlying conditions. Vaccine 2016, 34, 4850–4856. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Matsumoto, H.; Horita, N.; Hara, Y.; Kobayashi, N.; Kaneko, T. Prognostic factors for mortality in invasive pneumococcal disease in adult: A system review and meta-analysis. Sci. Rep. 2021, 11, 11865. [Google Scholar]
- Weinberger, D.M.; Warren, J.L.; Dalby, T.; Shapiro, E.D.; Valentiner-Branth, P.; Slotved, H.C.; Harboe, Z.B. Differences in the Impact of Pneumococcal Serotype Replacement in Individuals with and without Underlying Medical Conditions. Clin. Infect. Dis. 2019, 69, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.S.; Pondo, T.; Xing, W.; McGee, L.; Farley, M.; Schaffner, W.; Thomas, A.; Reingold, A.; Harrison, L.H.; Lynfield, R.; et al. Early Impact of 13-Valent Pneumococcal Conjugate Vaccine Use on Invasive Pneumococcal Disease among Adults with and without Underlying Medical Conditions-United States. Clin. Infect. Dis. 2020, 70, 2484–2492. [Google Scholar] [CrossRef]
- Wagenvoort, G.H.; Knol, M.J.; de Melker, H.E.; Vlaminckx, B.J.; van der Ende, A.; Rozenbaum, M.H.; Sanders, E.A.M. Risk and outcomes of invasive pneumococcal disease in adults with underlying conditions in the post-PCV7 era, The Netherlands. Vaccine 2016, 34, 334–340. [Google Scholar] [CrossRef]
- Balsells, E.; Dagan, R.; Yildirim, I.; Gounder, P.P.; Steens, A.; Munoz-Almagro, C.; Mameli, C.; Kandasamy, R.; Lavi, N.G.; Daprai, L.; et al. The relative invasive disease potential of Streptococcus pneumoniae among children after PCV introduction: A systematic review and meta-analysis. J. Infect. 2018, 77, 368–378. [Google Scholar] [CrossRef] [Green Version]
- Epiconcept. SpIDnet Project. Available online: https://sites.google.com/a/epiconcept.fr/ipd-surveillance/home-2 (accessed on 19 August 2020).
- I-MOVE +. WP3: Pneumococcal Vaccines. Available online: http://www.i-moveplus.eu/wp3 (accessed on 1 September 2020).
- Hanquet, G.; Krizova, P.; Valentiner-Branth, P.; Ladhani, S.N.; Nuorti, J.P.; Lepoutre, A.; Mereckiene, J.; Knol, M.; Winje, B.A.; Ciruela, P.; et al. Effect of childhood pneumococcal conjugate vaccination on invasive disease in older adults of ten European countries. Implications for adult vaccination. Thorax 2019, 74, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Winje, B.A.; Berild, J.D.; Vestrheim, D.F.; Denison, E.; Lepp, T.; Roth, A.; Valentiner-Branth, P.; Slotved, H.C.; Storsæter, J. Efficacy and Effectiveness of Pneumococcal Vaccination in Elderly—An Update of the Literature; Norwegian Institute of Public Health: Oslo, Norway, 2019; ISBN 978-82-8406-053-8. [Google Scholar]
- Folkehelseinstituttet. Vaksinasjonsveilederen for Helsepsersonell (Vaskinasjonsboka) [nettdokument] Oslo: Folkehelseinstituttet. 2015. Available online: https://www.fhi.no/nettpub/vaksinasjonsveilederen-for-helsepersonell/ (accessed on 14 January 2020).
- Pfizer. Top-Line Results from Phase 3 Study of 20-Valent Pneumococcal Conjugate Vaccine in Pneumococcal Vaccine-Naïve Adults Aged 18 Years or Older. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer_announces_top_line_results_from_phase_3_study_of_20_valent_pneumococcal_conjugate_vaccine_in_pneumococcal_vaccine_na_ve_adults_aged_18_years_or_older (accessed on 16 June 2020).
- Merck. Positive Topline Results from Two Phase 3 Adult Studies Evaluating V114, Merck’s Investigational 15-Valent Pneumococcal Conjugate Vaccine, Including Pivotal. Available online: https://www.merck.com/news/merck-announces-positive-topline-results-from-two-phase-3-adult-studies-evaluating-v114-mercks-investigational-15-valent-pneumococcal-conjugate-vaccine-including-pivotal-trial/ (accessed on 21 October 2020).
- Bakken, I.J.; Ariansen, A.S.; Knudsen, G.P.; Johansen, K.I.; Vollset, S.E. The Norwegian Patient Registry and the Norwegian Registry for Primary Health Care: Research potential of two nationwide health-care registries. Scand. J. Public Health 2020, 48, 49–55. [Google Scholar] [CrossRef]
- Statistics Norway. Population, by Sex and One-Year Age Groups, 1 January (M) 1986–2018; Statistics Norway: Oslo, Norway, 2018. [Google Scholar]
- Mahmud, S.M.; Sinnock, H.; Mostaco-Guidolin, L.C.; Pabla, G.; Wierzbowski, A.K.; Bozat-Emre, S. Long-term trends in invasive pneumococcal disease in Manitoba, Canada. Hum. Vaccin. Immunother. 2017, 13, 1884–1891. [Google Scholar] [CrossRef] [Green Version]
- Andrade, A.L.; Minamisava, R.; Policena, G.; Cristo, E.B.; Domingues, C.M.; de Cunto Brandileone, M.C.; Almeida, S.C.; Toscano, C.M.; Bierrenbach, A.L. Evaluating the impact of PCV-10 on invasive pneumococcal disease in Brazil: A time-series analysis. Hum. Vaccin. Immunother. 2016, 12, 285–292. [Google Scholar] [CrossRef] [Green Version]
- Vadlamudi, N.K.; Chen, A.; Marra, F. Impact of the 13-Valent Pneumococcal Conjugate Vaccine among Adults: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2019, 69, 34–49. [Google Scholar] [CrossRef]
- Ladhani, S.N.; Collins, S.; Djennad, A.; Sheppard, C.L.; Borrow, R.; Fry, N.K.; Andrews, N.J.; Miller, E.; Ramsay, M.E. Rapid increase in non-vaccine serotypes causing invasive pneumococcal disease in England and Wales, 2000–2017: A prospective national observational cohort study. Lancet Infect Dis. 2018, 18, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Lewnard, J.A.; Hanage, W.P. Making sense of differences in pneumococcal serotype replacement. Lancet Infect. Dis. 2019, 19, e213–e220. [Google Scholar] [CrossRef]
- Tin Tin Htar, M.; Morato Martinez, J.; Theilacker, C.; Schmitt, H.J.; Swerdlow, D. Serotype evolution in Western Europe: Perspectives on invasive pneumococcal diseases (IPD). Expert Rev. Vaccines 2019, 18, 1145–1155. [Google Scholar] [CrossRef]
- Van der Linden, M.; Imohl, M.; Perniciaro, S. Limited indirect effects of an infant pneumococcal vaccination program in an aging population. PLoS ONE 2019, 14, e0220453. [Google Scholar] [CrossRef] [Green Version]
- Steens, A.; Winje, B.A.; White, R.A.; Odsbu, I.; Brantsaeter, A.B.; Vestrheim, D.F. Indirect effects of pneumococcal childhood vaccination in individuals treated with immunosuppressants in ambulatory care: A case-cohort study. Clin. Infect. Dis. 2019, 68, 1367–1373. [Google Scholar] [CrossRef] [PubMed]
- Van Aalst, M.; Lotsch, F.; Spijker, R.; van der Meer, J.T.M.; Langendam, M.W.; Goorhuis, A.; Grobusch, M.P.; de Bree, G.J. Incidence of invasive pneumococcal disease in immunocompromised patients: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2018, 24, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Garcia Garrido, H.M.; Knol, M.J.; Heijmans, J.; van Sorge, N.M.; Sanders, E.A.M.; Klumpen, H.J.; Grobusch, M.P.; Goorhuis, A. Invasive pneumococcal disease among adults with hematological and solid organ malignancies: A population-based cohort study. Int. J. Infect Dis. 2021, 106, 237–245. [Google Scholar] [CrossRef]
- Andersen, M.A.; Niemann, C.U.; Rostgaard, K.; Dalby, T.; Sorrig, R.; Weinberger, D.M.; Hjalgrim, H.; Harboe, Z.B. Differences and Temporal Changes in Risk of Invasive Pneumococcal Disease in Adults with Hematological Malignancies: Results from a Nationwide 16-Year Cohort Study. Clin. Infect. Dis. 2021, 72, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Aiello, A.; Farzaneh, F.; Candore, G.; Caruso, C.; Davinelli, S.; Gambino, C.M.; Ligotti, M.E.; Zareian, N.; Accardi, G. Immunosenescence and Its Hallmarks: How to Oppose Aging Strategically? A Review of Potential Options for Therapeutic Intervention. Front. Immunol. 2019, 10, 2247. [Google Scholar] [CrossRef] [Green Version]
- Grant, L.R.; Slack, M.P.E.; Yan, Q.; Trzcinski, K.; Barratt, J.; Sobczyk, E.; Appleby, J.; Cané, A.; Jodar, L.; Isturiz, R.E.; et al. The epidemiologic and biologic basis for classifying older age as a high-risk, immunocompromising condition for pneumococcal vaccine policy. Expert Rev. Vaccines 2021, 4, 1–15. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Number (%) of IPD Cases 5 to 49 y | % In the Population 5 to 49 y | Number (%) of IPD Cases 50 to 64 y | % In the Population 50 to 64 y | Number (%) of IPD Cases 65+ y | % In the Population 65+ y | |
|---|---|---|---|---|---|---|
| Population size | 1012 (18) | 63.8 | 1406 (25) | 19.5 | 3117 (56) | 16.7 |
| Male sex | 569 (56) | 51.3 | 690 (49) * | 51.8 | 1536 (49) | 47.3 |
| Female sex | 443 (44) | 48.7 | 714 (51) * | 49.2 | 1581 (51) | 55.3 |
| Medical Risk Groups 1 | ||||||
| No risk conditions a | 784 (78) | 95.96 | 836 (59) | 84.95 | 1513 (49) | 67.02 |
| Medium risk conditions b | 104(10) | 3.50 | 316 (23) | 12.82 | 955 (31) | 26.42 |
| High risk conditions c | 124 (12) | 0.54 | 254 (18) | 2.22 | 649 (21) | 6.56 |
| Any risk condition | 228 (23) | 4.15 | 570 (41) | 16.00 | 1604 (51) | 36.40 |
| One risk condition | 147 (15) | 3.14 | 300 (21) | 10.46 | 820 (26) | 20.87 |
| Two risk conditions | 63 (6) | 0.66 | 189 (13) | 2.98 | 498 (16) | 7.54 |
| ≥2 risk conditions | 18 (2) | 0.35 | 81 (6) | 2.56 | 286 (9) | 7.99 |
| Medical Risk Conditions 1 | ||||||
| Immunodeficiency, HIV disease or asplenia | 24 (2) | 0.20 | 19 (1) | 0.36 | 25 (1) | 0.30 |
| Chronic kidney disease | 25 (2) | 0.10 | 39 ((3) | 0.50 | 222 (7) | 2.98 |
| Haematological cancer | 52 (5) | 0.10 | 127 (9) | 0.43 | 287 (9) | 1.10 |
| Generalised malignancy | 23 (2) | 0.09 | 96 (7) | 0.85 | 190 (6) | 2.37 |
| Other malignancies | 47 (5) | 0.61 | 171 (12) | 4.58 | 549 (18) | 12.88 |
| Solid organ transplantation | 43 (4) | 0.08 | 32 (2) | 0.28 | 27 (1) | 0.29 |
| CSF leakage or cochlear implant | 5 (0,5) | 0.01 | 0 | 0.01 | 2 (0.1) | 0.01 |
| Chronic heart disease | 10 (1) | 0.24 | 92 (7) | 3.26 | 506 (16) | 11.40 |
| Chronic lung disease | 32 (3) | 1.62 | 151 (11) | 3.03 | 551 (18) | 7.07 |
| Diabetes mellitus | 35 (3) | 1.10 | 128 (9) | 5.30 | 338 (11) | 10.05 |
| Alcoholism | 24 (2) | 0.25 | 61 (4) | 0.62 | 36 (1) | 0.50 |
| Chronic liver disease | 12 (1) | 0.08 | 33 (2) | 0.31 | 34 (1) | 0.43 |
| Risk Group/Condition | Risk Ratios (95% CI) | |
|---|---|---|
| 5 to 64 Years (n = 602) | 65+ Years (n = 1020) | |
| All types of IPD, n = 1622 | ||
| Medical Risk Groups | ||
| Medium risk II | 4.9 (4.0 to 6.0) | 1.8 (1.5 to 2.0) |
| High risk III | 25.5 (20.6 to 31.7) | 4.2 (3.6 to 5.0) |
| One comorbidity | 5.7 (4.6 to 7.1) | 2.0 (1.7 to 2.3) |
| Two comorbidities | 16.0 (12.6 to 20.3) | 3.0 (2.5 to 3.6) |
| ≥Two comorbidities | 6.6 (4.4 to 9.9) | 1.7 (1.4 to 2.1) |
| Medical Risk Conditions | ||
| Immunodeficiency, HIV-disease and asplenia | 11.9 (6.8 to 20.6) | 4.1 (2.2 to 7.6) |
| Chronic kidney disease | 13.9 (8.2 to 23.7) | 2.8 (2.2 to 3.6) |
| Haematological cancer | 68.1 (50.7 to 91.4) | 10.1 (8.1 to 12.7) |
| Generalised malignancies | 32.4 (23.0 to 45.5) | 4.2 (3.3 to 5.4) |
| Solid organ transplants | 36.8 (23.7 to 57.1) | 6.8 (4.2 to 11.0) |
| Chronic heart disease | 6.2 (4.1 to 9.4) | 2.3 (1.9 to 2.7) |
| Chronic lung disease | 6.1 (4.5 to 8.3) | 3.6 (3.0 to 4.3) |
| Diabetes mellitus | 6.5 (4.9 to 8.6) | 1.6 (1.3 to 2.0) |
| Alcoholism | 17.7 (11.9 to 26.3) | 2.8 (1.6 to 5.1) |
| Chronic liver disease | 21.2 (12.2 to 36.8) | 3.7 (2.1 to 6.5) |
| PCV13 IPD, n = 398 | ||
| Medium risk II | 3.5 (2.3 to 5.2) | 1.2 (0.9 to 1.7) |
| High risk III | 16.0 (10.3 to 24.9) | 3.2 (2.2 to 4.6) |
| One comorbidity | 4.0 (2.7 to 6.0) | 1.4 (1.0 to 1.9) |
| Two comorbidities | 9.8 (6.0 to 15.9) | 2.5 (1.7 to 3.6) |
| ≥Two comorbidities | 4.6 (2.0 to 10.3) | 1.1 (0.6 to 1.8) |
| non-PCV13 IPD, n = 1211 | ||
| Medium risk II | 5.0 (3.9 to 6.4) | 2.0 (1.7 to 2.3) |
| High risk III | 29.6 (23.3 to 37.7) | 4.5 (3.7 to 5.4) |
| One comorbidity | 6.1 (4.8 to 7.8) | 2.2 (1.9 to 2.6) |
| Two comorbidities | 17.4 (13.3 to 22.8) | 3.2 (2.6 to 3.9) |
| ≥Two comorbidities | 7.1 (4.5 to 11.4) | 1.9 (1.5 to 2.4) |
| PPV23 IPD, n = 1132 | ||
| Medium risk II | 4.3 (3.4 to 5.5) | 1.6 (1.3 to 1.9) |
| High risk III | 19.7 (15.2 to 25.6) | 3.4 (2.8 to 4.2) |
| One comorbidity | 4.9 (3.8 to 6.2) | 1.8 (1.5 to 2.2) |
| Two comorbidities | 12.8 (9.7 to 17.0) | 2.6 (2.1 to 3.3) |
| ≥Two comorbidities | 5.1 (3.1 to 8.5) | 1.2 (0.9 to 1.9) |
| Risk Group | N | PCV13 | PCV15 | PCV20 | PPV23 |
|---|---|---|---|---|---|
| All IPD | 1593 | 24% | 43% | 59% | 70% |
| No risk | 841 | 29% | 49% | 66% | 76% |
| Medium risk | 438 | 19% | 40% | 55% | 66% |
| High risk | 314 | 19% | 31% | 46% | 59% |
| One comorbidity | 377 | 19% | 40% | 56% | 66% |
| Two comorbidities | 249 | 20% | 35% | 47% | 63% |
| ≥Two comorbidities | 126 | 17% | 28% | 43% | 54% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winje, B.A.; Vestrheim, D.F.; White, R.A.; Steens, A. The Risk of Invasive Pneumococcal Disease Differs between Risk Groups in Norway Following Widespread Use of the 13-Valent Pneumococcal Vaccine in Children. Microorganisms 2021, 9, 1774. https://doi.org/10.3390/microorganisms9081774
Winje BA, Vestrheim DF, White RA, Steens A. The Risk of Invasive Pneumococcal Disease Differs between Risk Groups in Norway Following Widespread Use of the 13-Valent Pneumococcal Vaccine in Children. Microorganisms. 2021; 9(8):1774. https://doi.org/10.3390/microorganisms9081774
Chicago/Turabian StyleWinje, Brita Askeland, Didrik Frimann Vestrheim, Richard Aubrey White, and Anneke Steens. 2021. "The Risk of Invasive Pneumococcal Disease Differs between Risk Groups in Norway Following Widespread Use of the 13-Valent Pneumococcal Vaccine in Children" Microorganisms 9, no. 8: 1774. https://doi.org/10.3390/microorganisms9081774