
Improvement of Atopic Dermatitis by Synbiotic Baths


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Nucleic Acid Extraction
2.3. PCR and Amplicon Sequencing
2.4. Statistics and Network Analyses
3. Results
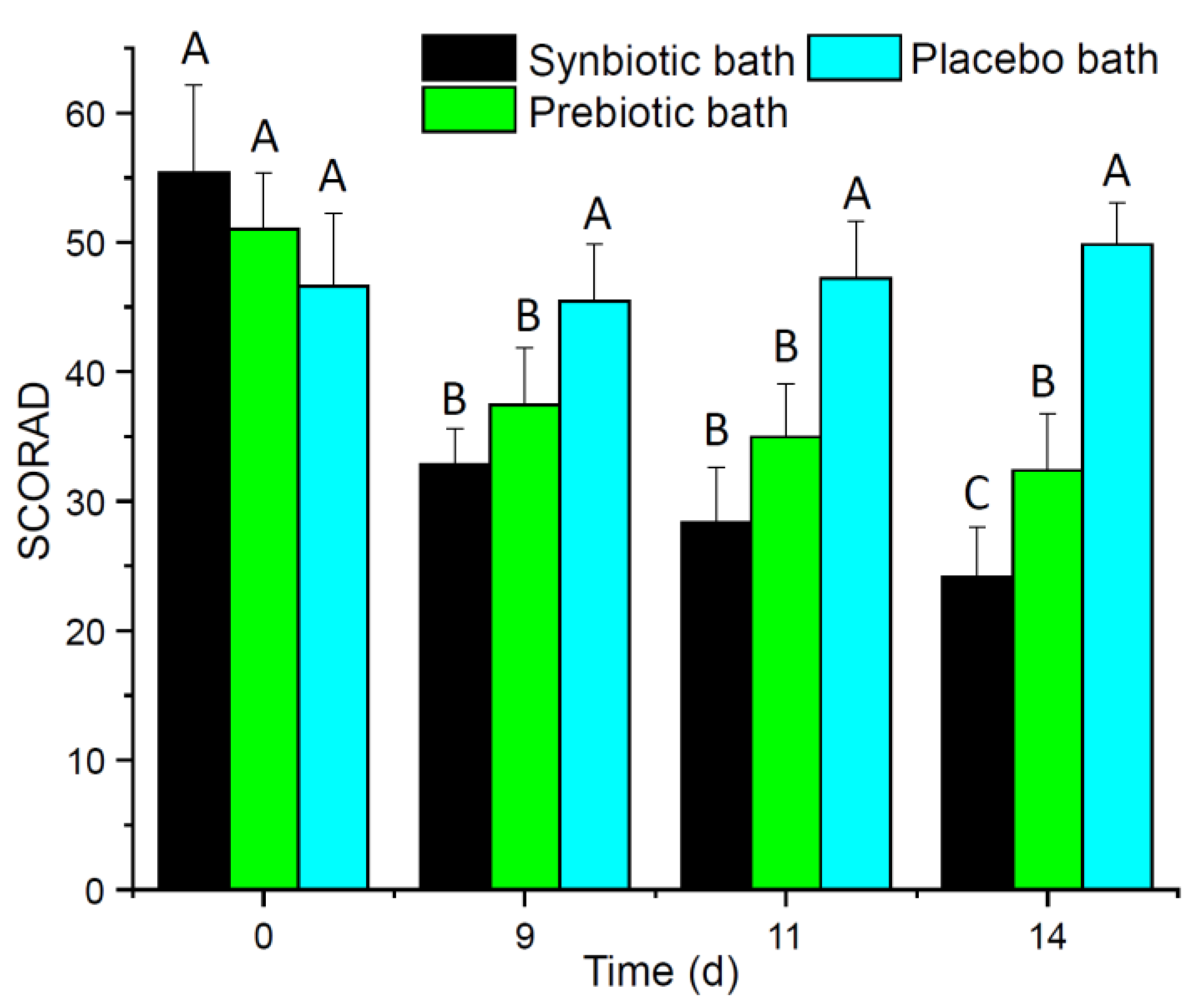
3.1. Synbiotic Baths Improved SCORAD and QoL
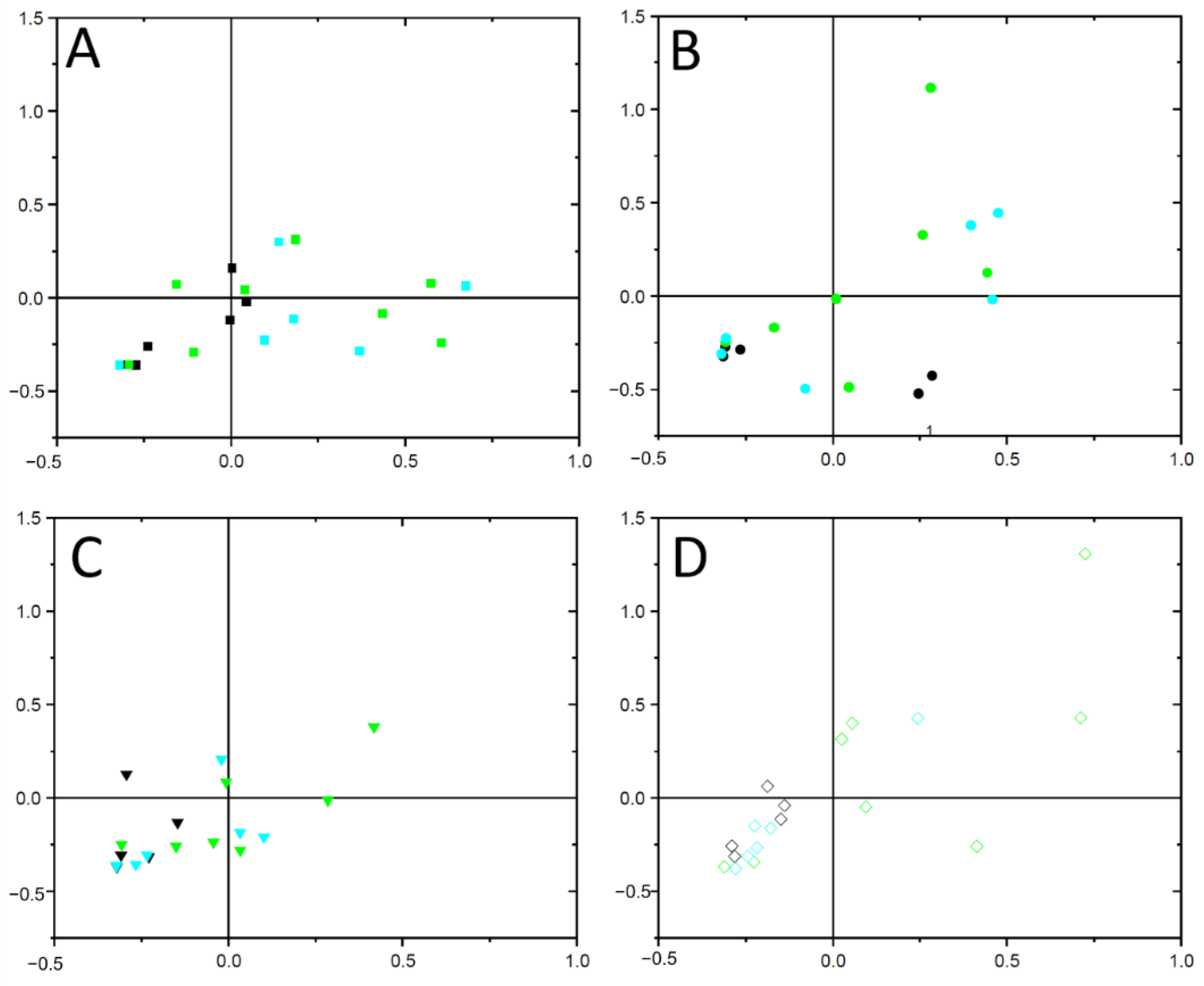
3.2. Composition of the Skin Microbiome Was Shifted
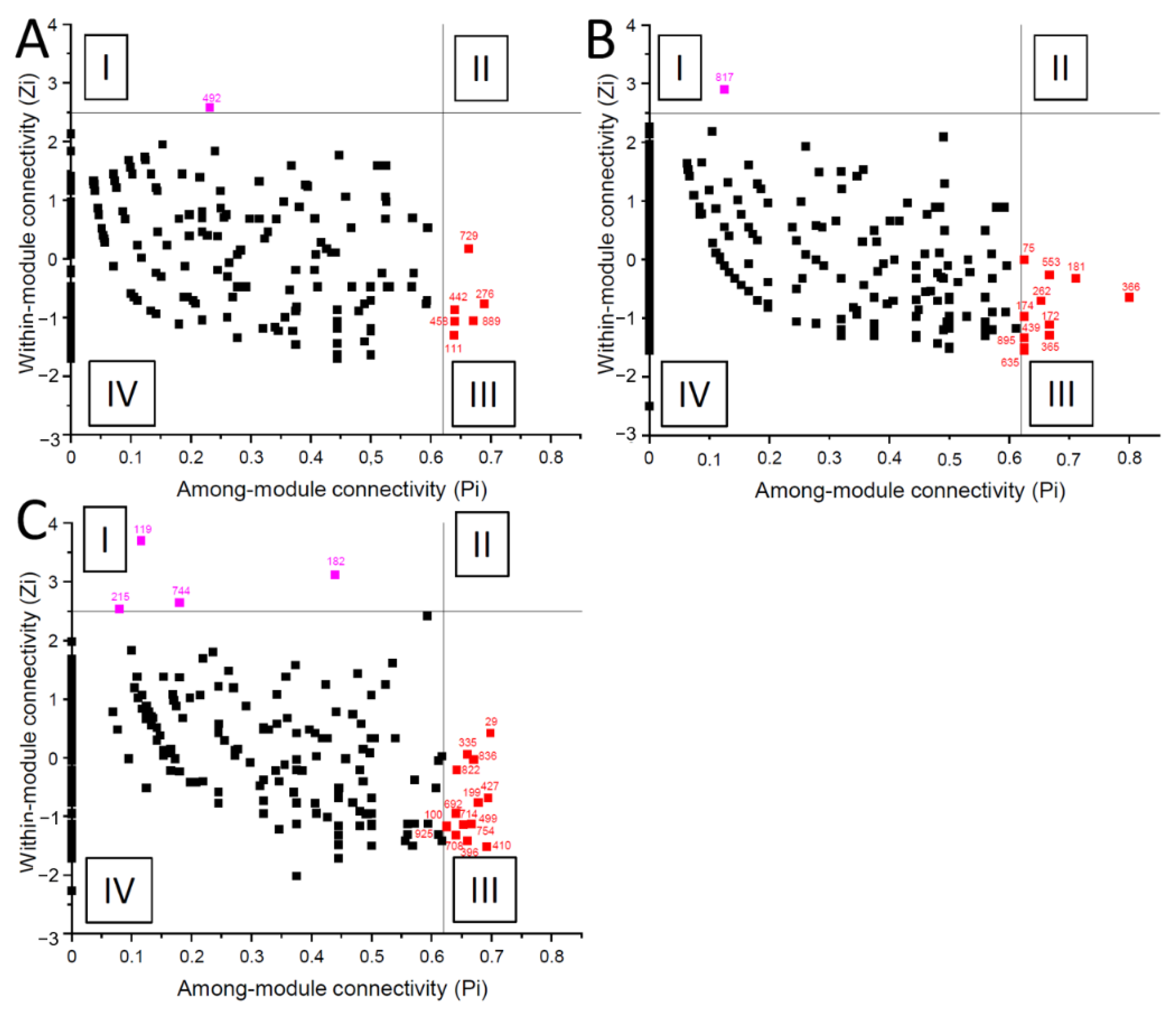
3.3. Bacterial Co-Occurrence Networks of AD Patients Differed
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mayba, J.N.; Gooderham, M.J. Review of atopic dermatitis and topical therapies. J. Cutan. Med. Surg. 2017, 21, 227–236. [Google Scholar] [CrossRef]
- Van Smeden, J.; Bouwstra, J.A. Stratum Corneum Lipids: Their role for the skin barrier function in healthy subjects and atopic dermatitis patients. Curr. Probl. Dermatol. 2016, 49, 8–26. [Google Scholar] [CrossRef] [PubMed]
- McAleer, M.A.; Jakasa, I.; Raj, N.; O’Donnell, C.P.F.; Lane, M.E.; Rawlings, A.V.; Voegeli, R.; McLean, W.H.I.; Kezic, S.; Irvine, A.D. Early-life regional and temporal variation in filaggrin-derived natural moisturizing factor, filaggrin-processing enzyme activity, corneocyte phenotypes and plasmin activity: Implications for atopic dermatitis. Br. J. Dermatol. 2018, 179, 431–441. [Google Scholar] [CrossRef] [Green Version]
- Naeem, A.S.; Tommasi, C.; Cole, C.; Brown, S.J.; Zhu, Y.; Way, B.; Willis Owen, S.A.G.; Moffatt, M.; Cookson, W.O.; Harper, J.I.; et al. A mechanistic target of rapamycin complex 1/2 (mTORC1)/V-Akt murine thymoma viral oncogene homolog 1 (AKT1)/cathepsin H axis controls filaggrin expression and processing in skin, a novel mechanism for skin barrier disruption in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2017, 139, 1228–1241. [Google Scholar] [CrossRef] [Green Version]
- Yuki, T.; Tobiishi, M.; Kusaka-Kikushima, A.; Ota, Y.; Tokura, Y. Impaired tight junctions in atopic dermatitis skin and in a skin-equivalent model treated with interleukin-17. PLoS ONE 2016, 11, e0161759. [Google Scholar] [CrossRef] [PubMed]
- Furue, M.; Chiba, T.; Tsuji, G.; Ulzii, D.; Kido-Nakahara, M.; Nakahara, T.; Kadono, T. Atopic dermatitis: Immune deviation, barrier dysfunction, IgE autoreactivity and new therapies. Allergol. Int. 2017, 66, 398–403. [Google Scholar] [CrossRef]
- Seite, S.; Flores, G.E.; Henley, J.B.; Martin, R.; Zelenkova, H.; Aguilar, L.; Fierer, N. Microbiome of affected and unaffected skin of patients with atopic dermatitis before and after emollient treatment. J. Drugs Dermatol. 2014, 13, 1365–1372. [Google Scholar] [PubMed]
- Kim, K. Influences of environmental chemicals on atopic dermatitis. Toxicol. Res. 2015, 31, 89–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, E.L.; Chalmers, J.R.; Hanifin, J.M.; Thomas, K.S.; Cork, M.J.; McLean, W.H.I.; Brown, S.J.; Chen, Z.; Chen, Y.; Williams, H.C. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J. Allergy Clin. Immunol. 2014, 134, 818–823. [Google Scholar] [CrossRef] [Green Version]
- Tiplica, G.S.; Boralevi, F.; Konno, P.; Malinauskiene, L.; Kaszuba, A.; Laurens, C.; Saint-Aroman, M.; Delarue, A. The regular use of an emollient improves symptoms of atopic dermatitis in children: A randomized controlled study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1180–1187. [Google Scholar] [CrossRef]
- Del Rosso, J.; Friedlander, S.F. Corticosteroids: Options in the era of steroid-sparing therapy. J. Am. Acad. Dermatol. 2005, 53, S50–S58. [Google Scholar] [CrossRef] [PubMed]
- Bornhövd, E.; Burgdorf, W.H.; Wollenberg, A. Macrolactam immunomodulators for topical treatment of inflammatory skin diseases. J. Am. Acad. Dermatol. 2001, 45, 736–743. [Google Scholar] [CrossRef]
- Daniel, B.S.; Orchard, D. Ocular side-effects of topical corticosteroids: What a dermatologist needs to know. Australas. J. Dermatol. 2015, 56, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Comberiati, P.; D’Auria, E.; Zuccotti, G.; Peroni, D.G. Topical corticosteroids for pediatric atopic dermatitis: Thoughtful tips for practice. Pharmacol. Res. 2020, 158, 104878. [Google Scholar] [CrossRef]
- Spada, F.; Barnes, T.M.; Greive, K.A. Comparative safety and efficacy of topical mometasone furoate with other topical corticosteroids. Australas. J. Dermatol. 2018, 59, e168–e174. [Google Scholar] [CrossRef] [Green Version]
- George, S.A.; Bilsland, D.J.; Johnson, B.E.; Ferguson, J. Narrow-band (TL-01) UVB air-conditioned phototherapy for chronic severe adult atopic dermatitis. Br. J. Dermatol. 1993, 128, 49–56. [Google Scholar] [CrossRef]
- Reynolds, N.J.; Franklin, V.; Gray, J.C.; Diffey, B.L.; Farr, P.M. Narrow-band ultraviolet B and broad-band ultraviolet A phototherapy in adult atopic eczema: A randomised controlled trial. Lancet 2001, 357, 2012–2016. [Google Scholar] [CrossRef]
- Simpson, E.L.; Bruin-Weller, M.; Flohr, C.; Ardern-Jones, M.R.; Barbarot, S.; Deleuran, M.; Bieber, T.; Vestergaard, C.; Brown, S.J.; Cork, M.J.; et al. When does atopic dermatitis warrant systemic therapy? Recommendations from an expert panel of the International Eczema Council. J. Am. Acad. Dermatol. 2017, 77, 623–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, D.Y.M. The microbiome and allergic diseases: A struggle between good and bad microbes. Ann. Allergy Asthma Immunol. 2019, 122, 231–232. [Google Scholar] [CrossRef]
- Huang, J.T.; Abrams, M.; Tlougan, B.; Rademaker, A.; Paller, A.S. Treatment of Staphylococcus aureus colonization in atopic dermatitis decreases disease severity. Pediatrics 2009, 123, e808-14. [Google Scholar] [CrossRef] [Green Version]
- Nakatsuji, T.; Chen, T.H.; Narala, S.; Chun, K.A.; Two, A.M.; Yun, T.; Shafiq, F.; Kotol, P.F.; Bouslimani, A.; Melnik, A.V.; et al. Antimicrobials from human skin commensal bacteria protect against Staphylococcus aureus and are deficient in atopic dermatitis. Sci. Transl. Med. 2017, 9, eaah4680. [Google Scholar] [CrossRef] [Green Version]
- Gibson, G.R.; Roberfroid, M.B. Dietary modulation of the human colonic microbiota: Introducing the concept of prebiotics. J. Nutr. 1995, 125, 1401–1412. [Google Scholar] [CrossRef]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The international scientific association for probiotics and prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [Green Version]
- Isolauri, E.; Arvola, T.; Sütas, Y.; Moilanen, E.; Salminen, S. Probiotics in the management of atopic eczema. Clin. Exp. Allergy 2000, 30, 1604–1610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rautava, S.; Kalliomäki, M.; Isolauri, E. Probiotics during pregnancy and breast-feeding might confer immunomodulatory protection against atopic disease in the infant. J. Allergy Clin. Immunol. 2002, 109, 119–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Seto, D.; Bielory, L. Meta-analysis of clinical trials of probiotics for prevention and treatment of pediatric atopic dermatitis. J. Allergy Clin. Immunol. 2008, 121, 116–121.e11. [Google Scholar] [CrossRef] [PubMed]
- Cuello-Garcia, C.A.; Brożek, J.L.; Fiocchi, A.; Pawankar, R.; Yepes-Nuñez, J.J.; Terracciano, L.; Gandhi, S.; Agarwal, A.; Zhang, Y.; Schünemann, H.J. Probiotics for the prevention of allergy: A systematic review and meta-analysis of randomized controlled trials. J. Allergy Clin. Immunol. 2015, 136, 952–961. [Google Scholar] [CrossRef] [PubMed]
- Axt-Gadermann, M. Signifikante Verbesserung des atopischen Ekzems durch Therapie mit synbiotischem Badezusatz. Akt Dermatol 2018, 44, 366–373. [Google Scholar] [CrossRef]
- Olesen, J.M.; Bascompte, J.; Dupont, Y.L.; Jordano, P. The modularity of pollination networks. Proc. Natl. Acad. Sci. USA 2007, 104, 19891–19896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stalder, J.F.; Taieb, A.; Atherton, D.J.; Bieber, P. Severity Scoring of Atopic Dermatitis: The SCORAD Index. Consensus Report of the European Task Force on Atopic Dermatitis. Dermatology (Basel) 1993, 186, 23–31. [Google Scholar] [CrossRef]
- Noll, M.; Matthies, D.; Frenzel, P.; Derakshani, M.; Liesack, W. Succession of bacterial community structure and diversity in a paddy soil oxygen gradient. Environ. Microbiol. 2005, 7, 382–395. [Google Scholar] [CrossRef] [PubMed]
- Thijs, S.; Beeck, M.o.d.; Beckers, B.; Truyens, S.; Stevens, V.; van Hamme, J.D.; Weyens, N.; Vangronsveld, J. Comparative evaluation of four Bacteria-specific primer pairs for 16S rRNA gene surveys. Front. Microbiol. 2017, 8, 494. [Google Scholar] [CrossRef] [PubMed]
- Buettner, C.; Noll, M. Differences in microbial key players in anaerobic degradation between biogas and sewage treatment plants. Int. Biodeterior. Biodegrad. 2018, 133, 124–132. [Google Scholar] [CrossRef]
- Bushnell, B.; Rood, J.; Singer, E. BBMerge-Accurate paired shotgun read merging via overlap. PLoS ONE 2017, 12, e0185056. [Google Scholar] [CrossRef]
- Schloss, P.D.; Westcott, S.L.; Ryabin, T.; Hall, J.R.; Hartmann, M.; Hollister, E.B.; Lesniewski, R.A.; Oakley, B.B.; Parks, D.H.; Robinson, C.J.; et al. Introducing mothur: Open-source, platform-independent, community-supported software for describing and comparing microbial communities. Appl. Environ. Microbiol. 2009, 75, 7537–7541. [Google Scholar] [CrossRef] [Green Version]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA ribosomal RNA gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef]
- Oksanen, J.F.; Blanchet, G.; Friendly, M.; Kindt, R.; Legendre, P.; McGlinn, D.; Minchin, P.R.; O’Hara, R.B.; Simpson, G.L.; Solymos, P.; et al. Package “vegan”: Community Ecology Package. Available online: https://github.com/vegandevs/vegan (accessed on 20 February 2021).
- Royston, P. Approximating the Shapiro-Wilk W-test for non-normality. Stat. Comput. 1992, 2, 117–119. [Google Scholar] [CrossRef]
- Faust, K.; Raes, J. CoNet app: Inference of biological association networks using Cytoscape. F1000Res 2016, 5, 1519. [Google Scholar] [CrossRef] [PubMed]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A software environment for integrated models of biomolecular interaction networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef]
- Brown, M.B. 400: A method for combining non-independent, one-sided tests of significance. Biometrics 1975, 31, 987. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Series B (Methodological) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Su, G.; Kuchinsky, A.; Morris, J.H.; States, D.J.; Meng, F. GLay: Community structure analysis of biological networks. Bioinformatics 2010, 26, 3135–3137. [Google Scholar] [CrossRef] [Green Version]
- Guimerà, R.; Nunes Amaral, L.A. Functional cartography of complex metabolic networks. Nature 2005, 433, 895–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neves Forte, W.C.; Mayumi Sumita, J.; Gianini Rodrigues, A.; Liuson, D.; Tanaka, E. Rebound phenomenon to systemic corticosteroid in atopic dermatitis. Allergol. Immunopathol. 2005, 33, 307–311. [Google Scholar] [CrossRef]
- Geoghegan, J.A.; Irvine, A.D.; Foster, T.J. Staphylococcus aureus and atopic dermatitis: A complex and evolving relationship. Trends Microbiol. 2018, 26, 484–497. [Google Scholar] [CrossRef]
- Byrd, A.L.; Belkaid, Y.; Segre, J.A. The human skin microbiome. Nat. Rev. Microbiol. 2018, 16, 143–155. [Google Scholar] [CrossRef]
- Zeeuwen, P.L.J.M.; Boekhorst, J.; Ederveen, T.H.A.; Kleerebezem, M.; Schalkwijk, J.; van Hijum, S.A.F.T.; Timmerman, H.M. Reply to Meisel et al. J. Investig. Dermatol. 2017, 137, 961–962. [Google Scholar] [CrossRef] [Green Version]
- Nizioł-Łukaszewska, Z.; Bujak, T.; Wasilewski, T.; Szmuc, E. Inulin as an effectiveness and safe ingredient in cosmetics. Polish J. Chem. Technol. 2019, 21, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Parvez, S.; Malik, K.A.; Ah Kang, S.; Kim, H.-Y. Probiotics and their fermented food products are beneficial for health. J. Appl. Microbiol. 2006, 100, 1171–1185. [Google Scholar] [CrossRef]
- Yildirim, Z.; Winters, D.K.; Johnson, M.G. Purification, amino acid sequence and mode of action of bifidocin B produced by Bifidobacterium bifidum NCFB 1454. J. Appl. Microbiol. 1999, 86, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, X.; Chen, J.; Sun, H.; Luo, L.; Gu, Y.; Yi, Y.; Wang, X.; Shan, Y.; Liu, B.; Zhou, Y.; et al. Mining, heterologous expression, purification and characterization of 14 novel bacteriocins from Lactobacillus rhamnosus LS-8. Int. J. Biol. Macromol. 2020, 164, 2162–2176. [Google Scholar] [CrossRef]
- Diep, D.B.; Håvarstein, L.S.; Nes, I.F. Characterization of the locus responsible for the bacteriocin production in Lactobacillus plantarum C11. J. Bacteriol. 1996, 178, 4472–4483. [Google Scholar] [CrossRef] [Green Version]
- Kawai, Y.; Saito, T.; Kitazawa, H.; Itoh, T. Gassericin A; an uncommon cyclic bacteriocin produced by Lactobacillus gasseri LA39 linked at N- and C-terminal ends. Biosci. Biotechnol. Biochem. 1998, 62, 2438–2440. [Google Scholar] [CrossRef] [PubMed]
- Rammelsberg, M.; Mller, E.; Radler, F. Caseicin 80: Purification and characterization of a new bacteriocin from Lactobacillus casei. Arch. Microbiol. 1990, 154, 249–252. [Google Scholar] [CrossRef]
- Park, S. Potentiation of hydrogen peroxide, nitric oxide, and cytokine production in RAW 264.7 macrophage cells exposed to human and commercial isolates of Bifidobacterium. Int. J. Food Microbiol. 1999, 46, 231–241. [Google Scholar] [CrossRef]
- Baurecht, H.; Rühlemann, M.C.; Rodríguez, E.; Thielking, F.; Harder, I.; Erkens, A.-S.; Stölzl, D.; Ellinghaus, E.; Hotze, M.; Lieb, W.; et al. Epidermal lipid composition, barrier integrity, and eczematous inflammation are associated with skin microbiome configuration. J. Allergy Clin. Immunol. 2018, 141, 1668–1676.e16. [Google Scholar] [CrossRef] [Green Version]
- Kwaszewska, A.; Sobiś-Glinkowska, M.; Szewczyk, E.M. Cohabitation--relationships of corynebacteria and staphylococci on human skin. Folia Microbiol. (Praha) 2014, 59, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Talento, A.F.; Malnick, H.; Cotter, M.; Brady, A.; McGowan, D.; Smyth, E.; Fitzpatrick, F. Brevibacterium otitidis: An elusive cause of neurosurgical infection. J. Med. Microbiol. 2013, 62, 486–488. [Google Scholar] [CrossRef]
- Gong, J.Q.; Lin, L.; Lin, T.; Hao, F.; Zeng, F.Q.; Bi, Z.G.; Yi, D.; Zhao, B. Skin colonization by Staphylococcus aureus in patients with eczema and atopic dermatitis and relevant combined topical therapy: A double-blind multicentre randomized controlled trial. Br. J. Dermatol. 2006, 155, 680–687. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | DF | F Value | p Value | DF | F Value | p Value |
|---|---|---|---|---|---|---|
| Overall assessment | Pain | |||||
| Time | 2 | 282.99 | 0.07 | 2 | 116.54 | 0.32 |
| Bath treatment | 2 | 559.11 | <0.01 | 2 | 522.90 | <0.01 |
| Bath treatment × Time | 4 | 0.77 | 0.55 | 4 | 0.27 | 0.90 |
| Restriction | Lichenification | |||||
| Time | 2 | 15.76 | 0.22 | 2 | 183.79 | 0.17 |
| Bath treatment | 2 | 688.58 | < 0.01 | 2 | 147.13 | <0.01 |
| Bath treatment × Time | 4 | 0.25 | 0.91 | 4 | 0.66 | 0.62 |
| Pruritus | Dryness | |||||
| Time | 2 | 416.52 | 0.02 | 2 | 89.01 | <0.01 |
| Bath treatment | 2 | 759.94 | <0.01 | 2 | 921.14 | <0.01 |
| Bath treatment × Time | 4 | 0.92 | 0.46 | 4 | 136.97 | 0.26 |
| Redness | SCORAD | |||||
| Time | 2 | 0.92 | 0.40 | 2 | 889.67 | <0.01 |
| Bath treatment | 2 | 986.83 | <0.01 | 2 | 1060.98 | <0.01 |
| Bath treatment × Time | 4 | 0.68 | 0.61 | 4 | 408.78 | <0.01 |
| Treatment | OTU Number | Module | Taxon |
|---|---|---|---|
| Synbiotic bath | 889 | connector | Acidibacter |
| 442 | connector | Lachnoanaerobaculum | |
| 492 | module hub | Micrococcus | |
| 111 | connector | Brevibacterium | |
| 729 | connector | Conexibacter | |
| 276 | connector | Dermabacter | |
| 458 | connector | Leptotrichia | |
| 456 | connector | Pediococcus | |
| 696 | connector | Rickettsiales | |
| Prebiotic bath | 365 | connector | Bergeyella |
| 366 | connector | Chryseobacterium | |
| 75 | connector | Geobacillus | |
| 172 | connector | Alloiococcus | |
| 181 | connector | Brevundimonas | |
| 174 | connector | Carnobacterium | |
| 895 | connector | Dialister | |
| 439 | connector | Howardella | |
| 553 | connector | Marinomonas | |
| 817 | module hub | Obscuribacterales | |
| 262 | connector | Ohtaekwangia | |
| 635 | connector | Propionibacterium | |
| Placebo bath | 499 | connector | Actinoplanes |
| 119 | module hub | Aquabacterium | |
| 215 | module hub | Chthoniobacter | |
| 410 | connector | Janibacter | |
| 754 | connector | Jeotgalicoccus | |
| 29 | connector | Ilumatobacter | |
| 836 | connector | Acidobacteria | |
| 100 | connector | Bifidobacteriaceae | |
| 182 | module hub | Caulobacter | |
| 396 | connector | Hydrogenophilus | |
| 335 | connector | Peptoniphilus | |
| 925 | connector | Rhodanobacter | |
| 692 | connector | Rhodospirillales | |
| 708 | connector | Ruminococcaceae | |
| 822 | connector | Saccharimonadales | |
| 744 | module hub | Sphingopyxis | |
| 714 | connector | Subdoligranulum |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noll, M.; Jäger, M.; Lux, L.; Buettner, C.; Axt-Gadermann, M. Improvement of Atopic Dermatitis by Synbiotic Baths. Microorganisms 2021, 9, 527. https://doi.org/10.3390/microorganisms9030527
Noll M, Jäger M, Lux L, Buettner C, Axt-Gadermann M. Improvement of Atopic Dermatitis by Synbiotic Baths. Microorganisms. 2021; 9(3):527. https://doi.org/10.3390/microorganisms9030527
Chicago/Turabian StyleNoll, Matthias, Michael Jäger, Leonie Lux, Christian Buettner, and Michaela Axt-Gadermann. 2021. "Improvement of Atopic Dermatitis by Synbiotic Baths" Microorganisms 9, no. 3: 527. https://doi.org/10.3390/microorganisms9030527