
The Global Burden of Meningitis in Children: Challenges with Interpreting Global Health Estimates

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of Data Sources
2.2. Analysis of Data Sources
3. Results
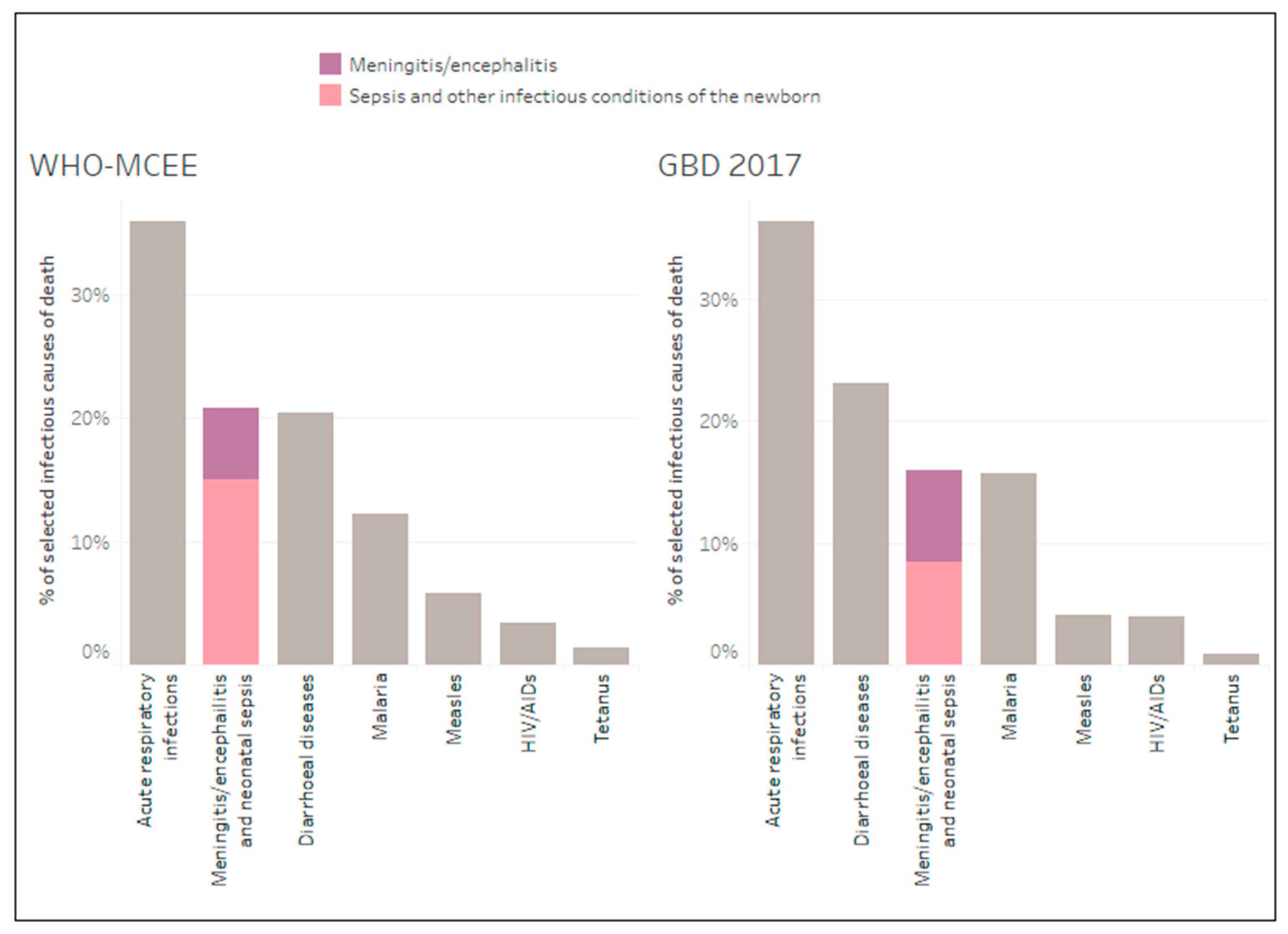
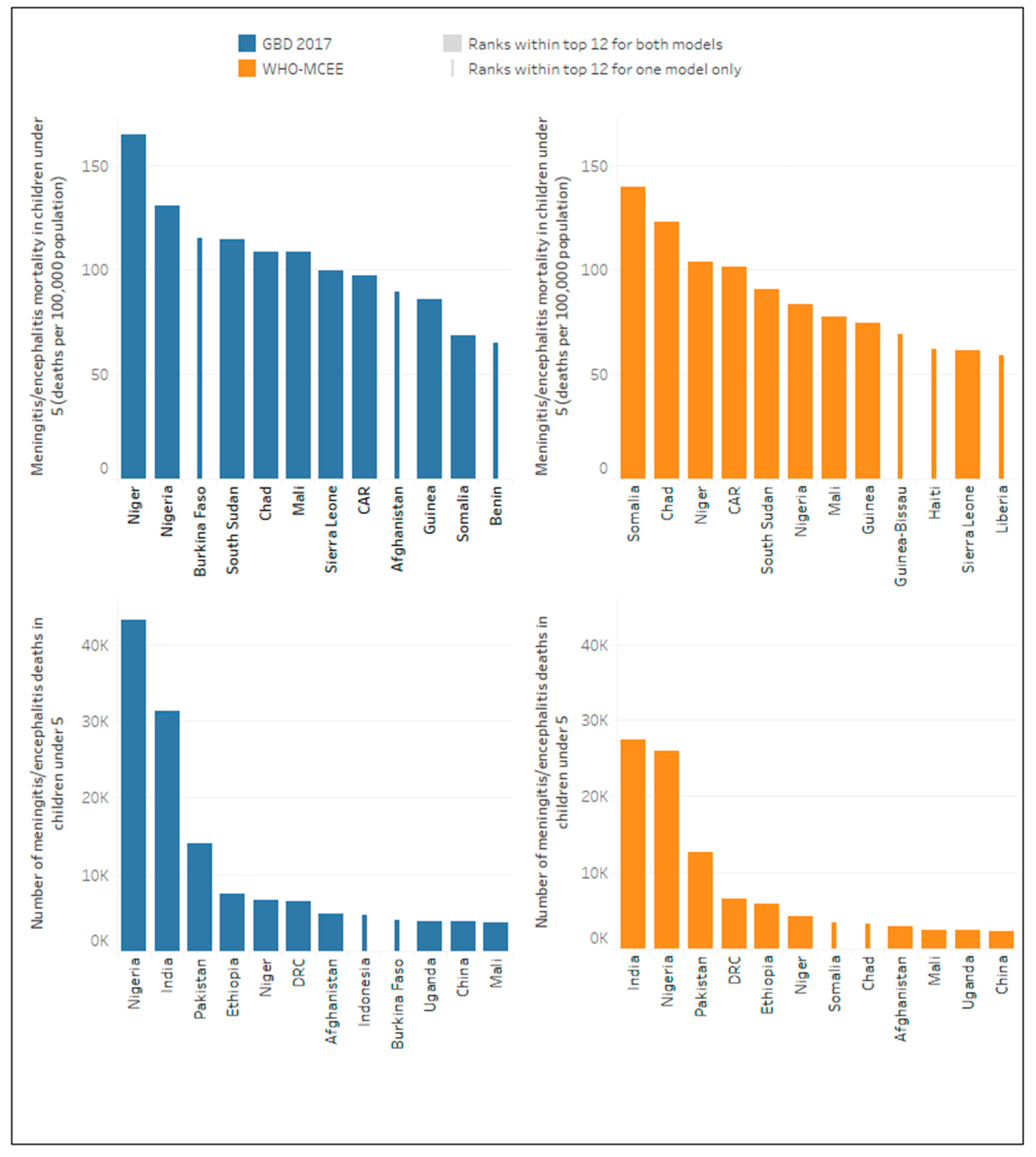
3.1. Global Meningitis and Neonatal Sepsis Mortality Estimates in Children Aged Under Five Years
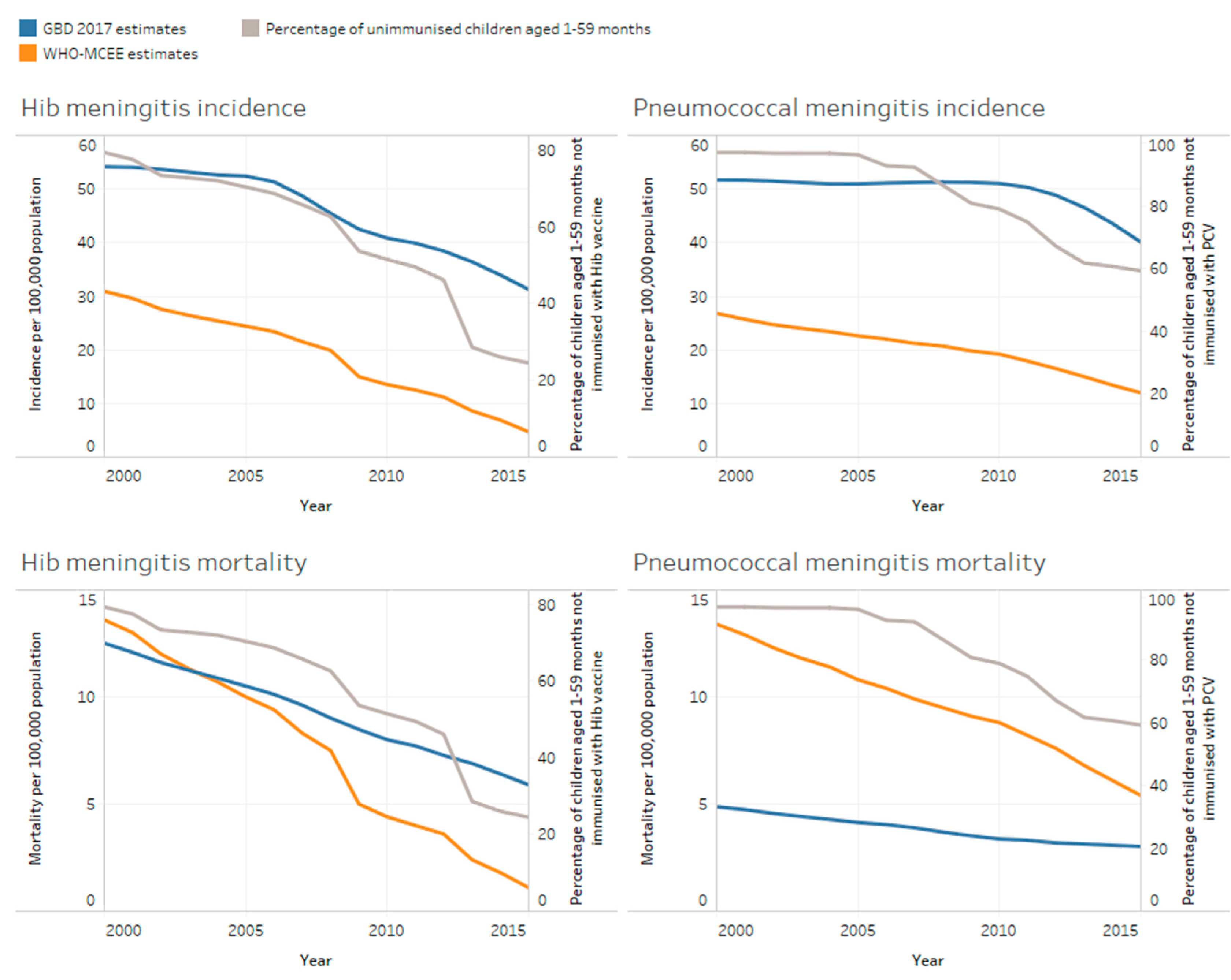
3.2. Meningitis Incidence and Mortality Estimates by Aetiology in Children Aged Under Five Years
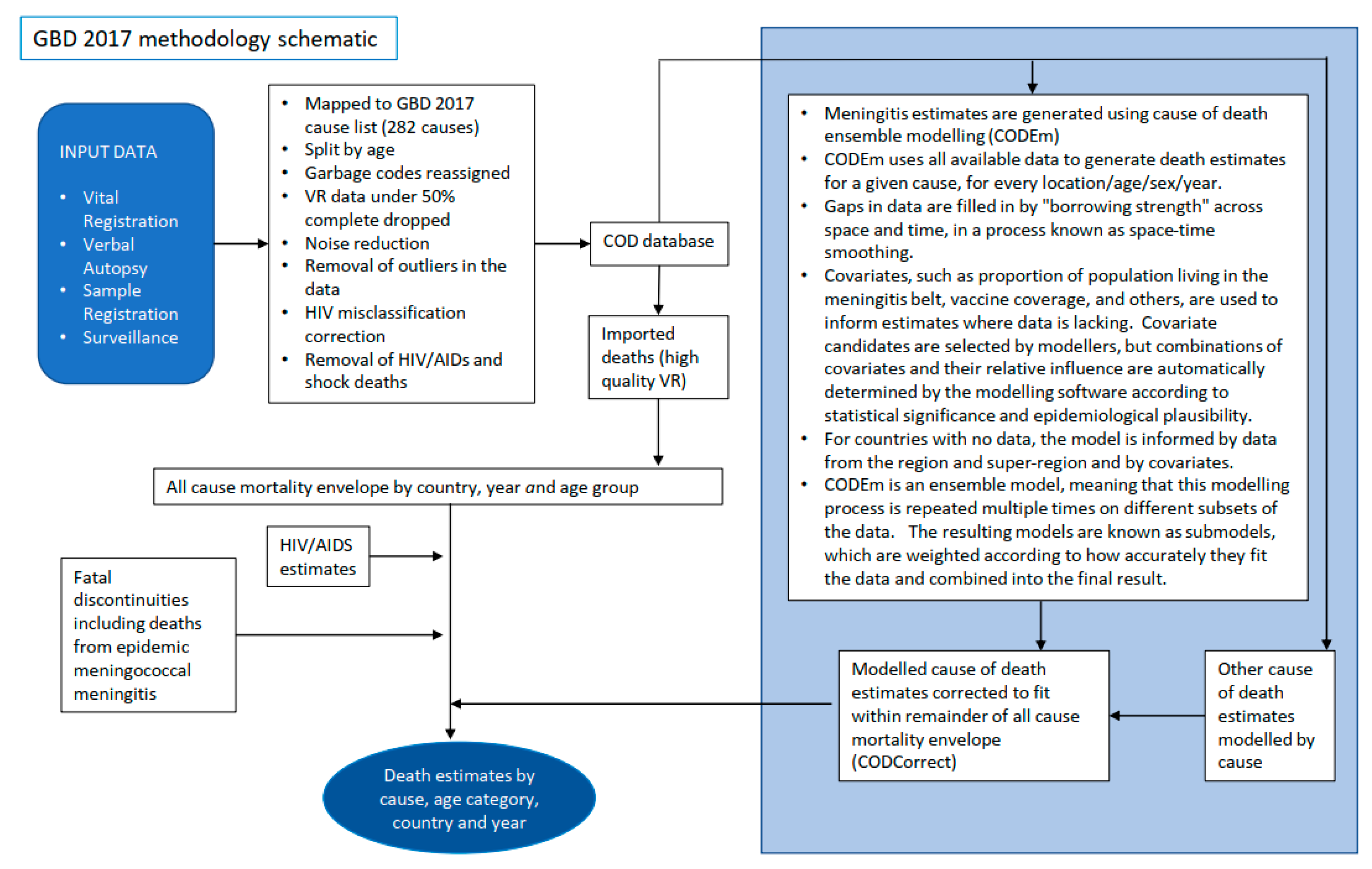
3.3. Modelling Methodology Which Could Account for Differences in Mortality and Pathogen Specific Estimates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). Levels & Trends in Child Mortality: Report 2020, Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation. 2020. Available online: https://www.un.org/development/desa/pd/news/levels-and-trends-child-mortality-2020-report (accessed on 1 December 2020).
- Zunt, J.R.; Kassebaum, N.J.; Blake, N.; Glennie, L.; Wright, C.; Nichols, E.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; A Adamu, A.; et al. Global, regional, and national burden of meningitis, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 1061–1082. [Google Scholar] [CrossRef] [Green Version]
- GBD Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. Available online: https://www.who.int/antimicrobial-resistance/publications/global-action-plan/en/ (accessed on 3 February 2020).
- Global Strategy for Women’s, Children’s, and Adolescents’ Health 2016–2030. Available online: https://www.who.int/life-course/partners/global-strategy/globalstrategyreport2016-2030-lowres.pdf (accessed on 3 February 2020).
- World Health Organization/The United Nations Children’s Fund (UNICEF). Global Action Plan for Prevention and Control of Pneumonia (GAPP). Available online: https://www.unicef.org/media/files/GAPP3_web.pdf (accessed on 3 February 2020).
- World Health Organization/The United Nations Children’s Fund (UNICEF). Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025. The Integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD). Available online: https://www.unicef.org/media/files/Final_GAPPD_main_Report-_EN-8_April_2013.pdf (accessed on 3 February 2020).
- Transforming Our World: The 2030 Agenda for Sustainable Development. Goal 3. Ensure Healthy Lives and Promote Well-Being for All at All Ages. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 3 February 2020).
- Working Group of the Specialised Technical Committee on Health, Population and Drug Control, Africa Health Strategy 2016–2030. Available online: https://au.int/sites/default/files/newsevents/workingdocuments/27513-wd-sa16951_e_africa_health_strategy-1.pdf (accessed on 3 February 2020).
- World Health Organization. Defeating meningitis by 2030. Available online: https://www.who.int/initiatives/defeating-meningitis-by-2030 (accessed on 8 February 2021).
- Rudan, I.; Campbell, H.; Marusic, A.; Sridhar, D.; Nair, H.; Adeloye, D.; Theodoratou, E.; Chan, K.Y. Assembling GHERG: Could “academic crowd–sourcing” address gaps in global health estimates? J. Glob. Heal. 2015, 5, 010101. [Google Scholar] [CrossRef]
- World Health Organization. Disease Burden and Mortality Estimates. Child Causes of Death, 2000–2017. Available online: https://www.who.int/healthinfo/global_burden_disease/estimates/en/index2.html (accessed on 14 October 2019).
- World Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. Available online: http://www.who.int/healthinfo/global_burden_disease/estimates/en/ (accessed on 10 June 2019).
- Wahl, B.; O’Brien, K.L.; Greenbaum, A.; Majumder, A.; Liu, L.; Chu, Y.; Lukšić, I.; Nair, H.; A McAllister, D.; Campbell, H.; et al. Burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in the era of conjugate vaccines: Global, regional, and national estimates for 2000–15. Lancet Glob. Heal. 2018, 6, e744–e757. [Google Scholar] [CrossRef] [Green Version]
- Seale, A.C.; Bianchi-Jassir, F.; Russell, N.J.; Kohli-Lynch, M.; Tann, C.J.; Hall, J.; Madrid, L.; Blencowe, H.; Cousens, S.; Baker, C.J.; et al. Estimates of the Burden of Group B Streptococcal Disease Worldwide for Pregnant Women, Stillbirths, and Children. Clin. Infect. Dis. 2017, 65, S200–S219. [Google Scholar] [CrossRef]
- Okike, I.O.; Johnson, A.P.; Henderson, K.L.; Blackburn, R.M.; Muller-Pebody, B.; Ladhani, S.N.; Anthony, M.; Ninis, N.; Heath, P.T. Incidence, Aetiology and Outcome of Bacterial Meningitis in Infants Aged <90 days in the UK and Republic of Ireland: Prospective, enhanced, national population-based surveillance. Clin. Infect. Dis 2014. [Google Scholar] [CrossRef]
- Ku, L.C.; Boggess, K.A.; Cohen-Wolkowiez, M. Bacterial Meningitis in Infants. Clin. Perinatol. 2015, 42, 29–45. [Google Scholar] [CrossRef] [Green Version]
- English, M.; Esamai, F.; Wasunna, A.; Were, F.; Ogutu, B.; Wamae, A.; Snow, R.W.; Peshu, N. Assessment of inpatient paediatric care in first referral level hospitals in 13 districts in Kenya. Lancet 2004, 363, 1948–1953. [Google Scholar] [CrossRef]
- Okomo, U.; Dibbasey, T.; Kassama, K.; E Lawn, J.; Zaman, S.M.A.; Kampmann, B.; Howie, S.R.C.; Bojang, K. Neonatal admissions, quality of care and outcome: 4 years of inpatient audit data from The Gambia’s teaching hospital. Paediatr. Int. Child Heal. 2015, 35, 252–264. [Google Scholar] [CrossRef]
- United Nations Department of Economic and Social Affairs Population Division. Population Databases. Available online: https://www.un.org/en/development/desa/population/publications/database/index.asp (accessed on 10 June 2019).
- Thigpen, M.C.; Whitney, C.G.; Messonnier, N.E.; Zell, E.R.; Lynfield, R.; Hadler, J.L.; Harrison, L.H.; Farley, M.M.; Reingold, A.; Bennett, N.M.; et al. Bacterial meningitis in the United States, 1998–2007. N. Engl. J. Med. 2011, 364, 2016–2025. [Google Scholar] [CrossRef] [PubMed]
- Swartz, M.N. Bacterial meningitis—A view of the past 90 years. N. Engl. J. Med. 2004, 351, 1826–1828. [Google Scholar] [CrossRef]
- van de Beek, D.; de Gans, J.; Spanjaard, L.; Weisfelt, M.; Reitsma, J.B.; Vermeulen, M. Clinical features and prognostic factors in adults with bacterial meningitis. N. Engl. J. Med. 2004, 351, 1849–1859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boisier, P.; Maínassara, H.B.; Sidikou, F.; Djibo, S.; Kairo, K.K.; Chanteau, S. Case-fatality ratio of bacterial meningitis in the African meningitis belt: We can do better. Vaccine 2007, 25, A24–A29. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, F.; E Pérez, A. Bacterial Meningitis in children and adolescents: An observational study based on the national surveillance system. BMC Infect. Dis. 2005, 5, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurley, E.S.; Montgomery, S.P.; Mayer, L.W.; Uddin, A.K.M.R.; Petersen, L.R.; Hossain, M.J.; Luby, S.P.; Rahman, M.E.; Breiman, R.F.; Whitney, A.; et al. Etiologies of bacterial meningitis in Bangladesh: Results from a hospital-based study. Am. J. Trop. Med. Hyg. 2009, 81, 475–483. [Google Scholar] [CrossRef] [PubMed]
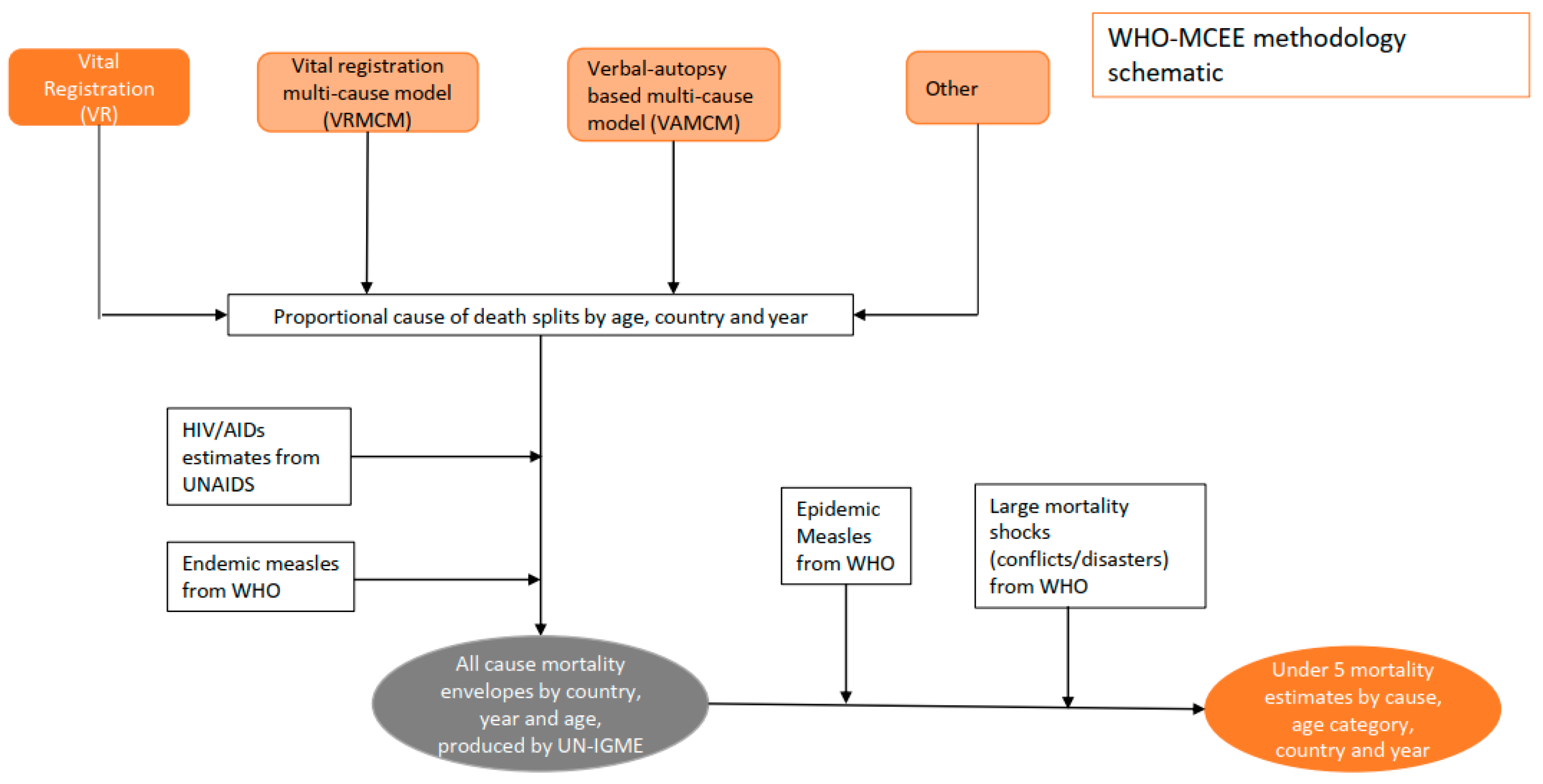
- Department of Evidence, Information and Research (WHO, Geneva) and Maternal Child Epidemiology Estimation (MCEE). MCEE-WHO Methods and Data Sources for Child Causes of Death 2000–2017. Available online: https://www.who.int/healthinfo/global_burden_disease/childcod_methods_2000_2017.pdf?ua=1 (accessed on 4 February 2019).
- O’Brien, K.L.; Wolfson, L.J.; Watt, J.P.; Henkle, E.; Deloria-Knoll, M.; McCall, N.; Lee, E.; Mulholland, K.; Levine, O.S.; Cherian, T.; et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: Global estimates. Lancet 2009, 374, 893–902. [Google Scholar] [CrossRef]
- Benara, S.K.; Singh, P. Validity of causes of infant death by verbal autopsy. Indian J. Pediatr. 1999, 66, 647–650. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Standard Verbal Autopsy Method for Investigating Causes of Death in Infants and Children. Available online: https://www.who.int/csr/resources/publications/surveillance/whocdscsrisr994.pdf?ua=1 (accessed on 9 September 2019).
- Butler, D. Verbal autopsy methods questioned. Nature 2010, 467, 1015. [Google Scholar] [CrossRef] [Green Version]
- Misganaw, A.; Mariam, D.H.; Araya, T.; Anteneh, A. Validity of verbal autopsy method to determine causes of death among adults in the urban setting of Ethiopia. BMC Med. Res. Methodol. 2012, 12, 130. [Google Scholar] [CrossRef] [Green Version]
- Mpimbaza, A.; Filler, S.; Katureebe, A.; Kinara, S.O.; Nzabandora, E.; Quick, L.; Ratcliffe, A.; Wabwire-Mangen, F.; Chandramohan, D.; Staedke, S.G. Validity of Verbal Autopsy Procedures for Determining Malaria Deaths in Different Epidemiological Settings in Uganda. PLoS ONE 2011, 6, e26892. [Google Scholar] [CrossRef]
- Snow, R.W.; Armstrong, J.R.; Forster, D.; Winstanley, M.T.; Marsh, V.M.; Newton, C.R.; Waruiru, C.; Mwangi, I.; Winstanley, P.A.; Marsh, K. Childhood deaths in Africa: Uses and limitations of verbal autopsies. Lancet 1992, 340, 351–355. [Google Scholar] [CrossRef]
- Anglewicz, P.; Kohler, H.P. Overestimating HIV infection: The construction and accuracy of subjective probabilities of HIV infection in rural Malawi. Demogr. Res. 2009, 20, 65–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandler, C.I.; Jones, C.; Boniface, G.; Juma, K.; Reyburn, H.; Whitty, C.J. Guidelines and mindlines: Why do clinical staff over-diagnose malaria in Tanzania? A qualitative study. Malar. J. 2008, 7, 53. [Google Scholar] [CrossRef] [Green Version]
- Gwer, S.; Newton, C.R.; Berkley, J.A. Over-diagnosis and co-morbidity of severe malaria in African children: A guide for clinicians. Am. J. Trop. Med. Hyg. 2007, 77, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2019 Diseases Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Mathers, C.D. History of global burden of disease assessment at the World Health Organization. Arch. Public Health 2020, 78, 1–13. [Google Scholar] [CrossRef]
- Meningitis Research Foundation. Meningitis Progress Tracker. Available online: https://public.tableau.com/profile/meningitis.research.foundation#!/vizhome/MeningitisandNeonatalSepsisTracker_15543731247200/CasesandDeaths (accessed on 14 September 2020).
- Traore, Y.; Tameklo, T.A.; Njanpop-Lafourcade, B.-M.; Lourd, M.; Yaro, S.; Niamba, D.; Drabo, A.; E Mueller, J.; Koeck, J.-L.; Gessner, B.D. Incidence, Seasonality, Age Distribution, and Mortality of Pneumococcal Meningitis in Burkina Faso and Togo. Clin. Infect. Dis. 2009, 48, S181–S189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmgren, H. Meningococcal disease and climate. Glob. Health Action 2009, 2. [Google Scholar] [CrossRef] [PubMed]
- Lingani, C.; Bergeron-Caron, C.; Stuart, J.M.; Fernandez, K.; Djingarey, M.H.; Ronveaux, O.; Schnitzler, J.C.; Perea, W.A. Meningococcal Meningitis Surveillance in the African Meningitis Belt, 2004–2013. Clin. Infect. Dis. 2015, 61, S410–S415. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Meningitis Weekly Bulletin. Available online: https://www.who.int/emergencies/diseases/meningitis/epidemiological/en/ (accessed on 16 September 2020).
- Patel, J.C.; Soeters, H.M.; Diallo, A.O.; Bicaba, B.W.; Kadadé, G.; Dembélé, A.Y.; Acyl, M.A.; Nikiema, C.; Lingani, C.; Hatcher, C.; et al. MenAfriNet: A Network Supporting Case-Based Meningitis Surveillance and Vaccine Evaluation in the Meningitis Belt of Africa. J. Infect. Dis. 2019, 220, S148–S154. [Google Scholar] [CrossRef]
- Wolfson, L.J.; Strebel, P.M.; Gacic-Dobo, M.; Hoekstra, E.J.; McFarland, J.W.; Hersh, B.S.; Measles, I. Has the 2005 measles mortality reduction goal been achieved? A natural history modelling study. Lancet 2007, 369, 191–200. [Google Scholar] [CrossRef]
- Castillo, P.; Ussene, E.; Ismail, M.R.; Jordao, D.; Lovane, L.; Carrilho, C.; Lorenzoni, C.; Lacerda, M.V.; Palhares, A.; Rodríguez-Carunchio, L.; et al. Pathological Methods Applied to the Investigation of Causes of Death in Developing Countries: Minimally Invasive Autopsy Approach. PLoS ONE 2015, 10, e0132057. [Google Scholar] [CrossRef] [PubMed]
- Bassat, Q.; Ordi, J.; Vila, J.; Ismail, M.R.; Carrilho, C.; Lacerda, M.; Munguambe, K.; Odhiambo, F.; Lell, B.; Sow, S.; et al. Development of a post-mortem procedure to reduce the uncertainty regarding causes of death in developing countries. Lancet Glob. Health 2013, 1, e125–e126. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Health Statistics 2017. Monitoring Health for the SDGs. Available online: https://apps.who.int/iris/bitstream/handle/10665/255336/9789241565486-eng.pdf;jsessionid=C00C94A637FA197A27B773D735A711A4?sequence=1 (accessed on 19 September 2019).
- Thatte, N.; Kalter, H.D.; Baqui, A.H.; Williams, E.M.; Darmstadt, G.L. Ascertaining causes of neonatal deaths using verbal autopsy: Current methods and challenges. J. Perinatol. 2009, 29, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2017 Diseases Injuries Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GBD 2017 | WHO GHE | WHO-MCEE Syndromic Model | WHO-MCEE Pathogen Model | LSHTM | |
|---|---|---|---|---|---|
| Years | 1990–2017 | 2000–2016 | 2000–2017 | 2000–2015 | 2015 |
| Number of countries & territories | 195 | 183 | 194 | 194 | 195 |
| Global under five population estimate in 2015 | 678,053,340 | 673,253,870 ** | 671,355,776 ** | 657,127,399 *** | N/A |
| Age range | All ages (Including: Early neonatal: 0–6 days Late neonatal: 7–27 days Post neonatal: 28–364 days 1–4 years) | All ages (including: 0–28 days 1–59 months) | 0–59 months (including: 0–28 days 1–59 months) | 1–59 months | 0–89 days |
| Relevant disease categories | Meningitis, neonatal sepsis and other neonatal infections | Meningitis *, neonatal sepsis and infections | Meningitis/encephalitis, sepsis and other infectious conditions of the newborn | Meningitis, Non-pneumonia/non-meningitis (which is primarily but not exclusively sepsis) | Meningitis, Sepsis |
| Outputs | Cases, Incidence rate, Prevalence, Deaths, Mortality rate, DALYs | Deaths, Mortality rate, DALYs | Deaths, Mortality rate | Cases, Incidence rate, Deaths, Mortality rate | Cases, Incidence rate, Deaths, Mortality rate |
| Published rate per population | Per 100,000 population | Per 100,000 population | Per 1000 livebirths | Per 100,000 population | Per 1000 livebirths |
| Aetiology | Nm, Spn, Hib, Other | No breakdown by aetiology | No breakdown by aetiology | Nonepidemic disease from: Spn, Hib, Nm | GBS |
| GBD 2017 | WHO-MCEE Pathogen Model | Difference * | ||||
|---|---|---|---|---|---|---|
| n | Rate † | n | Rate † | % | ||
| All causes | Under 5 | 5,917,285 | 872.69 | 5,792,509 | 862.81 a | 2% |
| (5,723,776–6,120,099) | (844.15–902.60) | (5,573,633–6,123,477) | ||||
| 1–59 months | 3,354,404 | 502.51 | 3,122,698 | 473.02 a | 7% | |
| (3,231,491–3,483,015) | (484.10–521.78) | (2,700,899–3,581,030 | ||||
| 0–28 days | 2,562,881 | 18.40 | 2,669,811 | 19.01 | −4% | |
| (2,478,272–2,655,261) | (17.20–19.58) | (2,542,447–2,872,734) | (18.10–20.50) | |||
| Infectious diseases ** | Under 5 | 2,519,567 | 371.59 | 2,426,882 | 361.49 a | 4% |
| (2,379,024–2,671,856) | (350.86–394.05) | (2,279,602–3,169,783) | ||||
| 1–59 months | 1,967,826 | 294.79 | 1,810,771 | 274.29 a | 8% | |
| (1,847,763–2,091,762) | (276.81–313.36) | (1,703,587–2,350,572) | ||||
| 0–28 days | 551,740 | 3.96 | 616,111 | 4.39 | −11% | |
| (510,918–603,527 | (3.60–4.38) | (605,290–877,610) | (4.31–6.25) | |||
| Meningitis & Encephalitis | Under 5 | 190,515 | 28.10 | 142,841 | 21.28 a | 29% |
| (163,374–217,259) | (24.09–32.04) | (87,427–178,552) | ||||
| 1–59 months | 167,880 | 25.15 | 105,406 | 15.97 a | 46% | |
| (143,529–192,447) | (21.50–28.83) | (87,188–145,213) | ||||
| 0–28 days | 22,636 | 0.16 | 37,435 | 0.27 | −49% | |
| (18,532–25,642) | (0.13–0.19) | (157–51,299) | (0.001–0.37) | |||
| Neonatal sepsis | Under 5 | 211,273 | 31.16 | 364,188 | 54.25 a | −53% |
| (186,657–275,821) | (27.53–40.68) | (282,744–524,021) | ||||
| 1–59 months | 12,693 | 1.90 | 386 b | 0.06 a | 188% | |
| (10,626–16,586) | (1.59–2.48) | (14–579) | ||||
| 0–28 days | 198,580 | 1.43 | 363,802 | 2.59 | −59% | |
| (175,866–263,096) | (1.24–1.86) | (282,341–523,853) | (2.01–3.73) | |||
| GBD 2017 | WHO-MCEE Pathogen Model | Difference * | ||||
|---|---|---|---|---|---|---|
| n | Rate † | n | Rate † | % | ||
| Pneumococcal meningitis | Cases | 267,686 | 40.10 | 83,809 | 13 | 105% |
| (179,314–374,902) | (26.86–56.16) | (36,160–168,500) | (5–26) | |||
| Deaths | 20,156 | 3.02 | 37,964 | 5 | −61% | |
| (16,114–25,199) | (2.41–3.78) | (15,397–79,718) | (2–11) | |||
| Hib meningitis | Cases | 208,658 | 31.26 | 31,243 | 5 | 148% |
| (139,815–304,035) | (20.95–45.55) | (13,386–50,595) | (2–8) | |||
| Deaths | 39,380 | 5.90 | 7156 | 1 | 138% | |
| (31,782–48,754) | (4.76–7.30) | (2707–11,320) | (0–2) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wright, C.; Blake, N.; Glennie, L.; Smith, V.; Bender, R.; Kyu, H.; Wunrow, H.Y.; Liu, L.; Yeung, D.; Knoll, M.D.; et al. The Global Burden of Meningitis in Children: Challenges with Interpreting Global Health Estimates. Microorganisms 2021, 9, 377. https://doi.org/10.3390/microorganisms9020377
Wright C, Blake N, Glennie L, Smith V, Bender R, Kyu H, Wunrow HY, Liu L, Yeung D, Knoll MD, et al. The Global Burden of Meningitis in Children: Challenges with Interpreting Global Health Estimates. Microorganisms. 2021; 9(2):377. https://doi.org/10.3390/microorganisms9020377
Chicago/Turabian StyleWright, Claire, Natacha Blake, Linda Glennie, Vinny Smith, Rose Bender, Hmwe Kyu, Han Yong Wunrow, Li Liu, Diana Yeung, Maria Deloria Knoll, and et al. 2021. "The Global Burden of Meningitis in Children: Challenges with Interpreting Global Health Estimates" Microorganisms 9, no. 2: 377. https://doi.org/10.3390/microorganisms9020377