
New/Different Look at the Presence of Aspergillus in Mycobacterial Pulmonary Diseases. Long-Term Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Data Collection
2.3. Diagnosis of Chronic Pulmonary Aspergillosis (CPA)
2.4. Radiological Evaluation
2.5. Sputum Examination
2.6. Statistical Analysis
3. Results
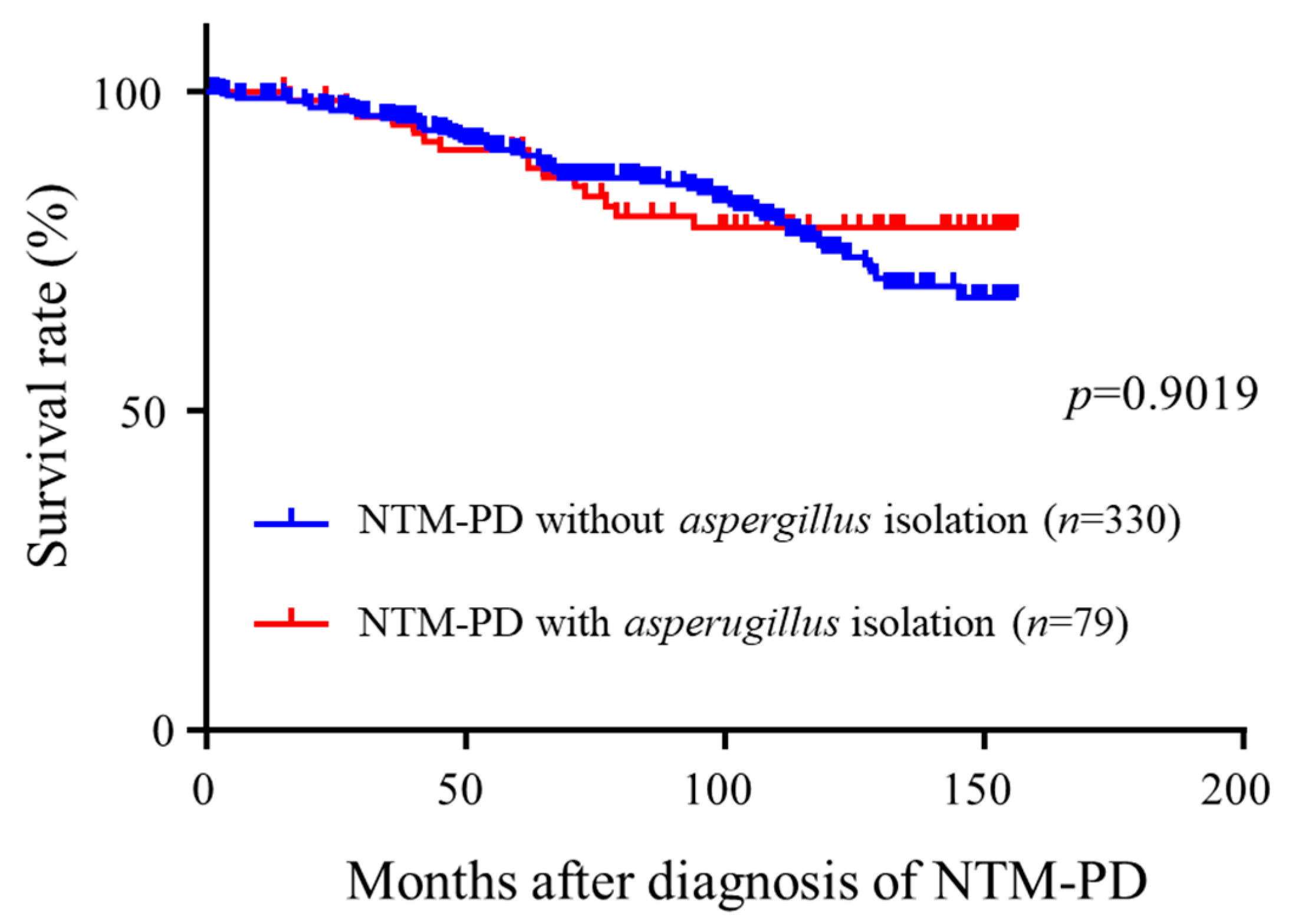
3.1. Baseline Characteristics and Analysis of Prognostic Impacts of Aspergillus Isolation
3.2. Risk Factors for Aspergillus Isolation
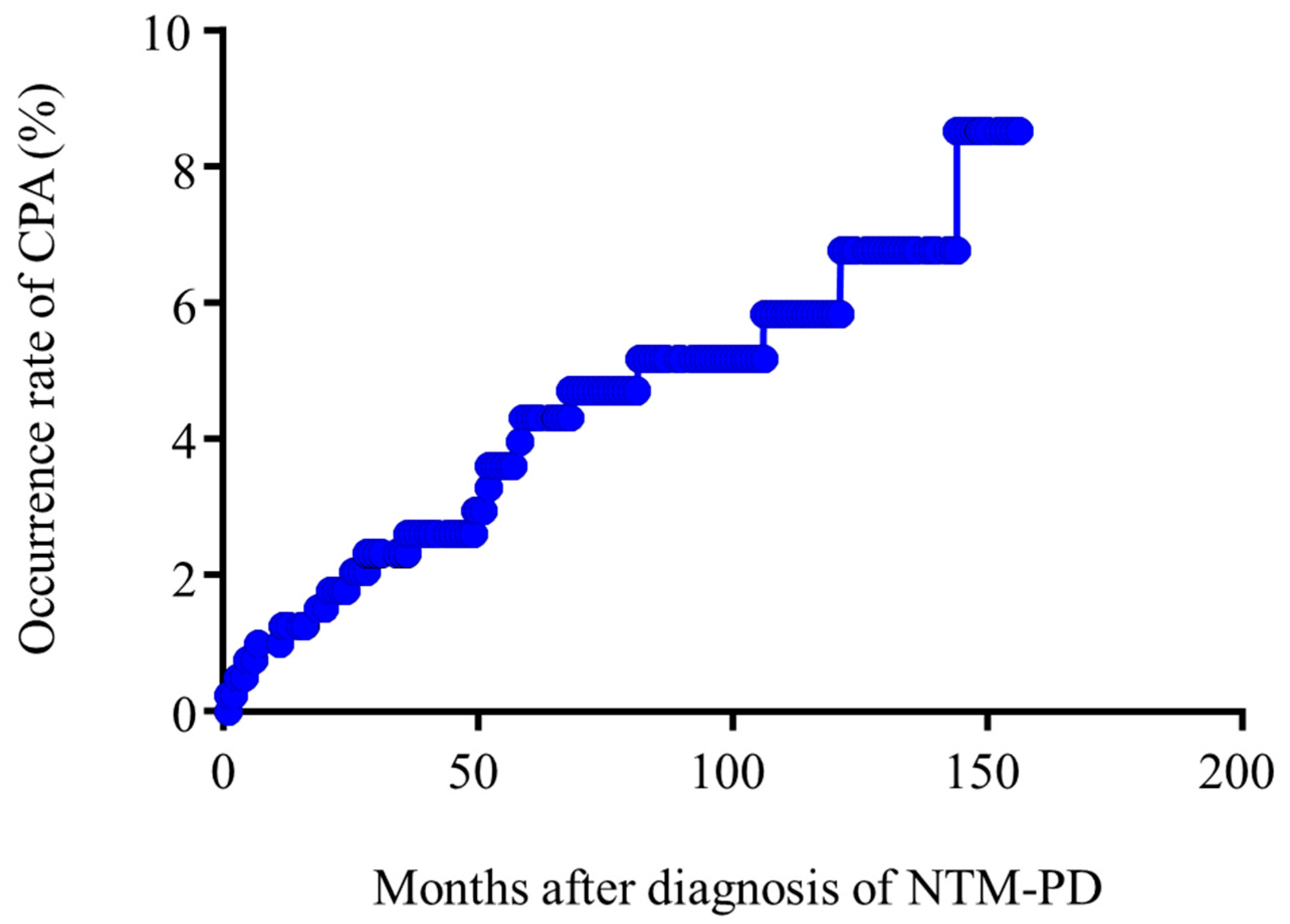
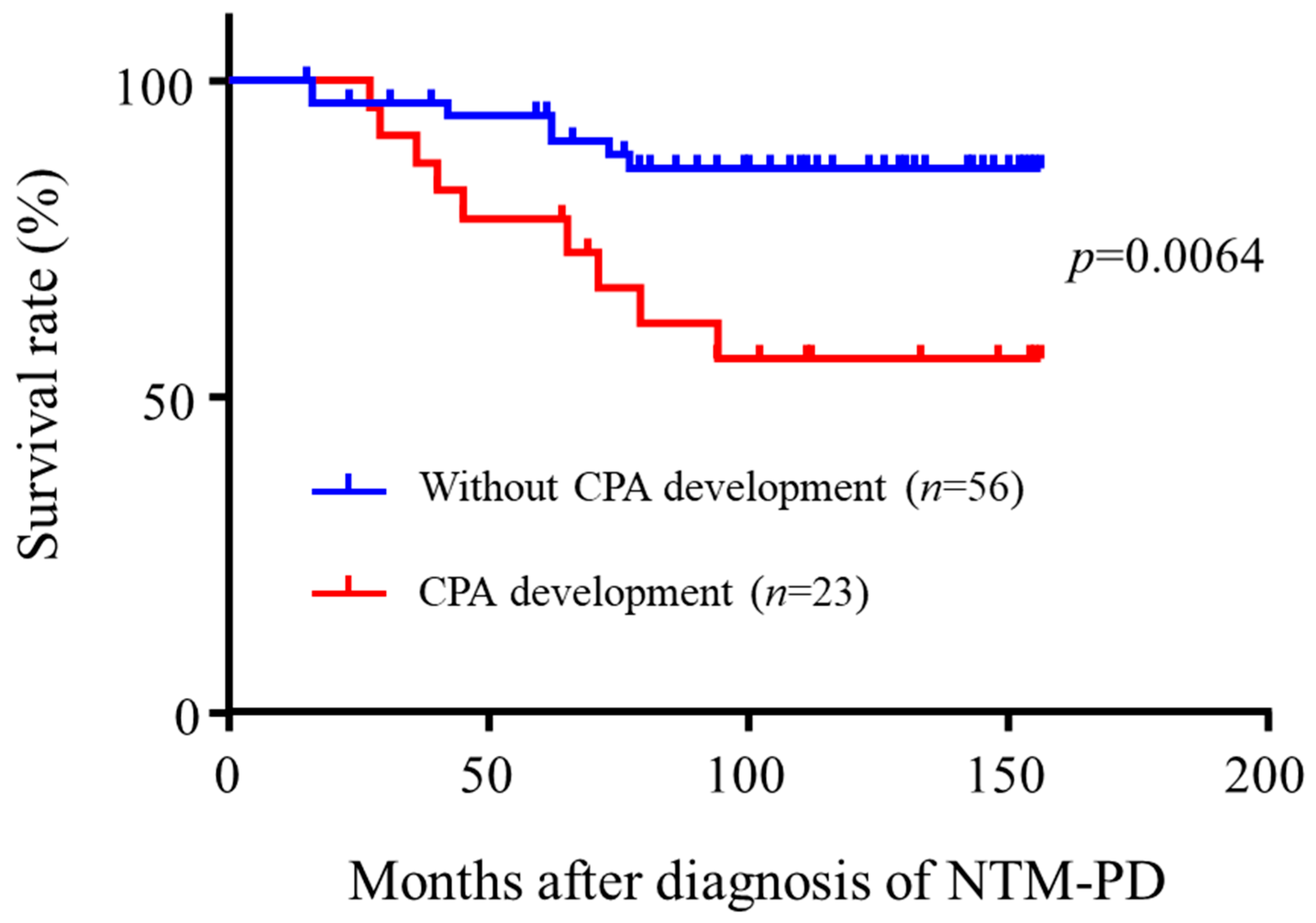
3.3. Risk Factors for CPA Development
3.4. Analysis of Risk Factors for Mortality in Aspergillus Isolated NTM-PD Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Furuuchi, K.; Ito, A.; Hashimoto, T.; Kumagai, S.; Ishida, T. Clinical significance of Aspergillus species isolated from respiratory specimens in patients with Mycobacterium avium complex lung disease. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2018, 37, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Jhun, B.W.; Jung, W.J.; Hwang, N.Y.; Park, H.Y.; Jeon, K.; Kang, E.S.; Koh, W.J. Risk factors for the development of chronic pulmonary aspergillosis in patients with nontuberculous mycobacterial lung disease. PLoS ONE 2017, 12, e0188716. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K.; Kitada, S.; Abe, Y.; Yamamoto, Y.; Matsuki, T.; Kagawa, H.; Oshitani, Y.; Tsujino, K.; Yoshimura, K.; Miki, M.; et al. Long-Term Treatment Outcome of Progressive Mycobacterium avium Complex Pulmonary Disease. J. Clin. Med. 2020, 9, 1315. [Google Scholar] [CrossRef] [PubMed]
- Phoompoung, P.; Chayakulkeeree, M. Chronic Pulmonary Aspergillosis Following Nontuberculous Mycobacterial Infections: An Emerging Disease. J. Fungi 2020, 6, 346. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Godet, C.; Philippe, B.; Laurent, F.; Cadranel, J. Chronic pulmonary aspergillosis: An update on diagnosis and treatment. Respir. Int. Rev. Thorac. Dis. 2014, 88, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Delliere, S.; Angebault, C.; Fihman, V.; Foulet, F.; Lepeule, R.; Maitre, B.; Schlemmer, F.; Botterel, F. Concomitant Presence of Aspergillus Species and Mycobacterium Species in the Respiratory Tract of Patients: Underestimated Co-occurrence? Front. Microbiol. 2019, 10, 2980. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef] [PubMed]
- Zoumot, Z.; Boutou, A.K.; Gill, S.S.; van Zeller, M.; Hansell, D.M.; Wells, A.U.; Wilson, R.; Loebinger, M.R. Mycobacterium avium complex infection in non-cystic fibrosis bronchiectasis. Respirology 2014, 19, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, S.; Yano, S.; Kadowaki, T.; Wakabayashi, K.; Kimura, M.; Kobayashi, K.; Ikeda, T. Clinical analysis of non-tuberculous mycobacteriosis cases complicated with pulmonary aspergillosis. Kekkaku 2011, 86, 781–785. [Google Scholar] [PubMed]
- Fujiuchi, S.; Sakunami, M.; Yamamoto, Y.; Takeda, A.; Nishigaki, Y.; Fujita, Y.; Yamazaki, Y.; Fujikane, T. Analysis of chronic necrotizing pulmonary aspergillosis (CNPA) cases complicated with non-tuberculous mycobacteriosis (NTM). Kekkaku 2008, 83, 573–575. [Google Scholar] [PubMed]
- Smith, N.L.; Denning, D.W. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. Eur. Respir. J. 2011, 37, 865–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, M.; Takayanagi, N.; Kanauchi, T.; Miyahara, Y.; Yanagisawa, T.; Sugita, Y. Prognostic factors of 634 HIV-negative patients with Mycobacterium avium complex lung disease. Am. J. Respir. Crit. Care Med. 2012, 185, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K.; Miki, M.; Matsumoto, Y.; Uda, E.; Yamamoto, Y.; Kogita, Y.; Kagawa, Y.; Matsuki, T.; Kagawa, H.; Oshitani, Y.; et al. The impact of adjuvant surgical treatment of nontuberculous mycobacterial pulmonary disease on prognosis and outcome. Respir. Res. 2020, 21, 153. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K.; Kitada, S.; Komukai, S.; Kuge, T.; Matsuki, T.; Kagawa, H.; Tsujino, K.; Miki, M.; Miki, K.; Kida, H. First line treatment selection modifies disease course and long-term clinical outcomes in Mycobacterium avium complex pulmonary disease. Sci. Rep. 2021, 11, 1178. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, Y.; Maeda, H.; Ogawa, Y.; Hashimoto, T. Experimental pulmonary cavity formation by mycobacterial components and synthetic adjuvants. Microbiol. Immunol. 1986, 30, 1175–1187. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.; Post, F.A.; Moreira, A.L.; Wainwright, H.; Kreiswirth, B.N.; Tanverdi, M.; Mathema, B.; Ramaswamy, S.V.; Walther, G.; Steyn, L.M.; et al. Mycobacterium tuberculosis growth at the cavity surface: A microenvironment with failed immunity. Infect. Immunity 2003, 71, 7099–7108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garnacho-Montero, J.; Amaya-Villar, R.; Ortiz-Leyba, C.; Leon, C.; Alvarez-Lerma, F.; Nolla-Salas, J.; Iruretagoyena, J.R.; Barcenilla, F. Isolation of Aspergillus spp. from the respiratory tract in critically ill patients: Risk factors, clinical presentation and outcome. Crit. Care 2005, 9, R191–R199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeda, K.; Imamura, Y.; Takazono, T.; Yoshida, M.; Ide, S.; Hirano, K.; Tashiro, M.; Saijo, T.; Kosai, K.; Morinaga, Y.; et al. The risk factors for developing of chronic pulmonary aspergillosis in nontuberculous mycobacteria patients and clinical characteristics and outcomes in chronic pulmonary aspergillosis patients coinfected with nontuberculous mycobacteria. Med. Mycol. 2016, 54, 120–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Total NTM-PD (n = 409) | Sensored (n = 336) | Death (n = 73) | p-Value | HR (95%CI) | p-Value | Adjusted HR (95% CI) | |
| Characteristic | |||||||
| Sex, male | 145 (35.5) | 112 (33.3) | 33 (45.2) | 0.0169 * | 1.77 (1.11–2.81) | 0.0487 * | 1.83 (1.00–3.33) |
| Age, years | 62.41 (±11.06) | 61.78 (±11.02) | 65.29 (±10.86) | <0.0001 * | 1.05 (1.03–1.08) | <0.0001 * | 1.06 (1.03–1.09) |
| BMI | 18.98 (±2.949) | 19.28 (±2.76) | 17.75 (±3.371) | <0.0001 * | 0.03 (0.006–0.17) | <0.0001 * | 1.0 (1.03–1.21) |
| Underlying disease | |||||||
| COPD | 43 (10.5) | 32 (9.5) | 11 (15.1) | 0.2033 | 1.55 (0.77–2.82) | ||
| Old Tb | 17 (4.2) | 13 (3.9) | 4 (5.5) | 0.8891 | 1.08 (0.33–2.60) | ||
| DM | 64 (15.6) | 46 (13.7) | 18 (24.7) | 0.0221 * | 1.94 (1.11–3.23) | 0.3376 | 1.37 (0.70–2.52) |
| Use of systemic steroid | 49 (12.0) | 31 (9.2) | 18 (24.7) | 0.0054 * | 2.30 (1.30–3.88) | 0.2926 | 1.40 (0.73–2.54) |
| CRP | 1.69 (±2.804) | 1.344 (±2.641) | 2.884 (±3.035) | 0.0001 * | 1.14 (1.07–1.19) | 0.0077 * | 1.12 (1.03–1.21) |
| NB form | 317 (77.5) | 267 (79.5) | 50 (68.5) | 0.0092 * | 0.50 (0.31–0.84) | 0.3868 | 0.75 (0.39–1.43) |
| Cavity | 149 (36.4) | 103 (30.7) | 46 (63.0) | <0.0001 * | 4.07 (2.54–6.67) | 0.0036 * | 2.38 (1.33–4.38) |
| Species | |||||||
| MAC | 325 (79.5) | 270 (80.4) | 55 (75.3) | 0.6984 | 0.89 (0.50–1.69) | ||
| M. abscessus | 32 (7.8) | 26 (7.7) | 6 (8.2) | ||||
| M. kansasii | 26 (6.4) | 22 (6.5) | 4 (5.5) | ||||
| Others | 24 (5.9) | 18 (5.4) | 6 (8.2) | ||||
| AFB stain positive | 111 (27.1) | 72 (21.4) | 39 (53.4) | <0.0001 * | 4.11 (2.59–6.55) | 0.0001 * | 2.87 (1.68–4.95) |
| Aspergillus isolation | 79 (19.3) | 64 (19.0) | 13 (17.8) | 0.9016 | 0.97 (0.54–1.64) | ||
| Isolated Aspergillus species | |||||||
| A. fumigatus | 56 (13.7) | 42 (12.5) | 14 (19.2) | ||||
| A. niger | 18 (4.4) | 17 (5.1) | 1 (1.4) | ||||
| Others | 5 (1.2) | 5 (1.5) | 0 (0.0) | ||||
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Without Aspergillus Isolation (n = 330) | With Aspergillus Isolation (n = 79) | p-Value | OR (95%CI) | p-Value | Adjusted OR (95%CI) | |
| Characteristic | ||||||
| Sex, male | 110 (33.3) | 35 (44.3) | 0.0684 | 1.59 (0.97–2.62) | ||
| Age | 62.68 (±11.3) | 61.25 (±9.8) | 0.3188 | 0.99 (0.97–1.01) | ||
| BMI | 19.02 (±2.9) | 18.81 (±3.1) | 0.5924 | 0.98 (0.89–1.07) | ||
| Underlying disease | ||||||
| COPD | 33 (10.0) | 10 (12.7) | 0.4900 | 1.30 (0.61–2.77) | ||
| Old Tb | 13 (3.9) | 4 (5.1) | 0.6539 | 1.30 (0.41–4.10) | ||
| DM | 52 (15.8) | 12 (15.2) | 0.9007 | 0.96 (0.48–1.89) | ||
| Use of systemic steroid | 33 (10.0) | 16 (20.3) | 0.0104 * | 2.37 (1.22–4.57) | 0.3053 | 1.48 (0.70–3.15) |
| CRP | 1.45 (±2.4) | 2.57 (±3.8) | 0.0087 * | 1.13 (1.03–1.23) | 0.0213 * | 1.11 (1.02–1.22) |
| NB form | 259 (78.5) | 58 (73.4) | 0.3336 | 0.76 (0.43–1.33) | ||
| Cavity | 119 (36.1) | 30 (38.0) | 0.7896 | 1.07 (0.65–1.78) | ||
| Species | ||||||
| MAC | 260 (78.8) | 65 (82.3) | 0.6897 | 1.14 (0.60–2.16) | ||
| M. abscessus | 26 (7.9) | 6 (7.6) | ||||
| M. kansasii | 21 (6.4) | 5 (6.3) | ||||
| Others | 21 (6.4) | 3 (3.8) | ||||
| AFB stain positive | 79 (23.9) | 32 (40.5) | 0.0033 * | 2.16 (1.29–3.62) | 0.0101 * | 2.14 (1.20–3.83) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| p-Value | OR (95%CI) | p-Value | Adjusted OR (95%CI) | |
| Characteristic | ||||
| Sex, male | 0.4096 | 1.43 (0.61–3.35) | ||
| Age | 0.5835 | 0.96 (0.93–1.00) | ||
| BMI | 0.3792 | 0.94 (0.81–1.08) | ||
| Underlying disease | ||||
| COPD | 0.6846 | 1.30 (0.37–4.56) | ||
| Old Tb | 0.0409 * | 0.29 (1.06–15.00) | 0.0613 | 4.10 (0.94–17.99) |
| DM | 0.1633 | 2.00 (0.76–5.27) | ||
| Use of systemic steroid | 0.0069 * | 3.68 (0.12–0.68) | 0.0189 * | 3.31 (1.22–9.01) |
| CRP | 0.1228 | 1.10 (0.98–1.24) | ||
| NB form | 0.0045 * | 0.29 (0.12–0.68) | 0.1804 | 0.52 (0.20–1.35) |
| Cavity | 0.0005 * | 5.39 (2.08–13.99) | 0.0207 * | 3.48 (1.21–9.98) |
| Species | ||||
| MAC | 0.1707 | 0.52 (0.21–1.32) | ||
| AFB stain positive | 0.0021 * | 3.82 (1.62–8.99) | 0.1168 | 2.11 (0.83–5.37) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| p-Value | HR (95%CI) | p-Value | Adjusted HR (95%CI) | |
| Characteristic | ||||
| Sex, male | 0.041 * | 2.82 (1.04–8.33) | 0.0345 | 3.08 (1.09–9.61) |
| Age, | 0.1001 | 1.05 (0.99–1.12) | ||
| BMI | 0.1115 | 0.86 (0.71–1.03) | ||
| Underlying disease | ||||
| COPD | 0.9468 | 1.05 (0.17–3.77) | ||
| Old Tb | 0.8338 | 1.25 (0.07–6.18) | ||
| DM | 0.2909 | 1.91 (0.53–5.48) | ||
| Use of systemic steroid | 0.3113 | 1.77 (0.56–4.86) | ||
| CRP | 0.2518 | 1.08 (0.94–1.21) | ||
| NB form | 0.11 | 0.44 (0.16–1.22) | ||
| Cavity | 0.0007 * | 5.96 (2.07–21.3) | 0.0056 * | 4.53 (1.53–16.59) |
| Species | ||||
| MAC | 0.7789 | 0.83 (0.26–3.64) | ||
| AFB stain positive | 0.0006 * | 6.16 (2.14–22.1) | 0.0051 | 4.63 (1.56–16.96) |
| Isolated Aspergillus species | ||||
| A. fumigatus | 0.0529 | 3.54 (0.99–22.54) | 0.1548 | 2.67 (0.72–17.36) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukushima, K.; Kida, H. New/Different Look at the Presence of Aspergillus in Mycobacterial Pulmonary Diseases. Long-Term Retrospective Cohort Study. Microorganisms 2021, 9, 270. https://doi.org/10.3390/microorganisms9020270
Fukushima K, Kida H. New/Different Look at the Presence of Aspergillus in Mycobacterial Pulmonary Diseases. Long-Term Retrospective Cohort Study. Microorganisms. 2021; 9(2):270. https://doi.org/10.3390/microorganisms9020270
Chicago/Turabian StyleFukushima, Kiyoharu, and Hiroshi Kida. 2021. "New/Different Look at the Presence of Aspergillus in Mycobacterial Pulmonary Diseases. Long-Term Retrospective Cohort Study" Microorganisms 9, no. 2: 270. https://doi.org/10.3390/microorganisms9020270