
Clinical and Functional Predictors of Response to a Comprehensive Pulmonary Rehabilitation in Severe Post-COVID-19 Patients

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
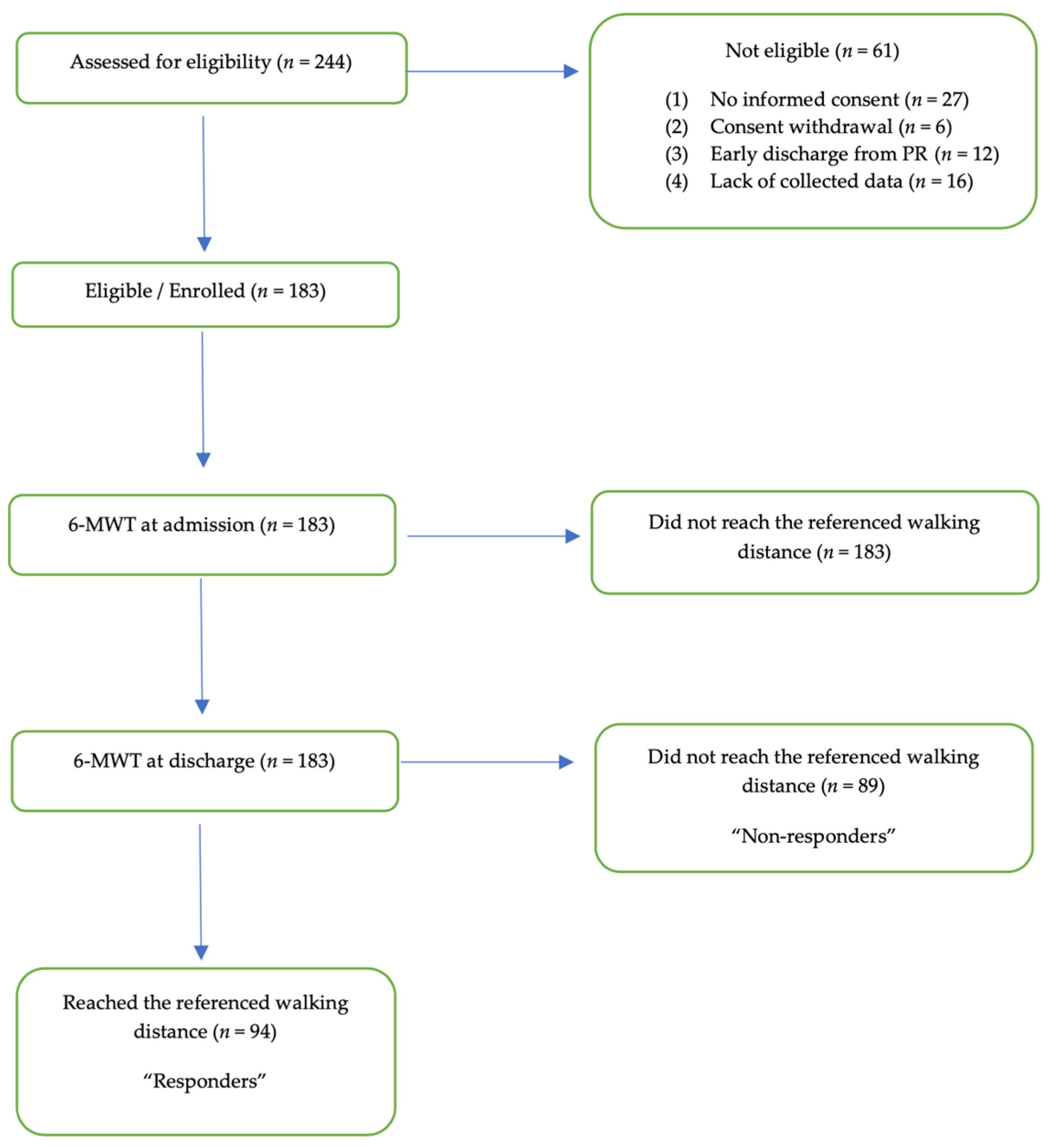
2.1. Participants and Procedures
2.2. Pulmonary Rehabilitation
2.3. Exercise Capacity
2.4. Quality of Life
2.5. Functional Independence Measure (FIM)
2.6. Hospital Anxiety and Depression Scale (HADS)
2.7. Cumulative Illness Rating Scale (CIRS)
2.8. Feeling Thermometer (FT)
2.9. Pulmonary Function Tests (PFT) and Blood Gas Analysis
2.10. Statistics
3. Results
3.1. Baseline Characteristics
3.2. Comorbidities
3.3. Assessments on Admission
- Pulmonary function tests on admission
- Functional and subjective changes during PR
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2014, 189, 1570. [Google Scholar] [CrossRef]
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, 2, CD003793. [Google Scholar] [CrossRef]
- Kenn, K.; Gloeckl, R.; Soennichsen, A.; Sczepanski, B.; Winterkamp, S.; Boensch, M.; Welte, T. Predictors of Success for Pulmonary Rehabilitation in Patients Awaiting Lung Transplantation. Transplantation 2015, 99, 1072–1077. [Google Scholar] [CrossRef]
- Bertolucci, F.; Sagliocco, L.; Tolaini, M.; Posteraro, F. Comprehensive rehabilitation treatment for sub-acute COVID-19 patients: An observational study. Eur. J. Phys. Rehabil. Med. 2021, 57, 208–215. [Google Scholar] [CrossRef]
- Hermann, M.; Pekacka-Egli, A.M.; Witassek, F.; Baumgaertner, R.; Schoendorf, S.; Spielmanns, M. Feasibility and Efficacy of Cardiopulmonary rehabilitation after COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 865–869. [Google Scholar] [CrossRef]
- Spielmanns, M.; Pekacka-Egli, A.-M.; Schoendorf, S.; Windisch, W.; Hermann, M. Effects of a Comprehensive Pulmonary Rehabilitation in Severe Post-COVID-19 Patients. Int. J. Environ. Res. Public Health 2021, 18, 2695. [Google Scholar] [CrossRef]
- Al Chikhanie, Y.; Veale, D.; Schoeffler, M.; Pépin, J.L.; Verges, S.; Hérengt, F. Effectiveness of pulmonary rehabilitation in COVID-19 respiratory failure patients post-ICU. Respir. Physiol. Neurobiol. 2021, 287, 103639. [Google Scholar] [CrossRef] [PubMed]
- Betschart, M.; Rezek, S.; Unger, I.; Beyer, S.; Gisi, D.; Shannon, H.; Sieber, C. Feasibility of an Outpatient Training Program after COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 3978. [Google Scholar] [CrossRef] [PubMed]
- Vagaggini, B.; Costa, F.; Antonelli, S.; De Simone, C.; De Cusatis, G.; Martino, F.; Santerini, S.; Paggiaro, P. Clinical predictors of the efficiency of a pulmonary rehabilitation programme in patients with COPD. Respir. Med. 2009, 103, 1224–1230. [Google Scholar] [CrossRef] [Green Version]
- Scott, A.S.; Baltzan, M.A.; Fox, J.; Wolkove, N. Success in pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Can. Respir. J. 2010, 17, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Enright, P.L.; Sherrill, D.L. Reference equations for the six-minute walk in healthy adults. Am. J. Respir. Crit. Care Med. 1998, 158, 1384–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, C.B. Exercise in chronic pulmonary disease: Aerobic exercise prescription. Med. Sci. Sports Exerc. 2001, 33, S671–S679. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- ATS. Committee on proficiency standards for clinical pulmonary function laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Alahdab, M.T.; Mansour, I.N.; Napan, S.; Stamos, T.D. Six minute walk test predicts long-term all-cause mortality and heart failure rehospitalization in African-American patients hospitalized with acute decompensated heart failure. J. Card. Fail. 2009, 15, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Boxer, R.; Kleppinger, A.; Ahmad, A.; Annis, K.; Hager, D.; Kenny, A. The 6-minute walk is associated with frailty and predicts mortality in older adults with heart failure. Congest. Heart Fail. 2010, 16, 208–213. [Google Scholar] [CrossRef] [Green Version]
- Castel, M.A.; Méndez, F.; Tamborero, D.; Mont, L.; Magnani, S.; Tolosana, J.M.; Berruezo, A.; Godoy, M.; Sitges, M.; Vidal, B.; et al. Six-minute walking test predicts long-term cardiac death in patients who received cardiac resynchronization therapy. Europace 2009, 11, 338–342. [Google Scholar] [CrossRef]
- Enfield, K.; Gammon, S.; Floyd, J.; Falt, C.; Patrie, J.; Platts-Mills, T.A.; Truwit, J.D.; Shim, Y.M. Six-minute walk distance in patients with severe end-stage COPD: Association with survival after inpatient pulmonary rehabilitation. J. Car-Diopulm. Rehabil. Prev. 2010, 30, 195–202. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Berman, L.B.; Townsend, M.; Pugsley, S.O.; Chambers, L.W. A measure of quality of life for clinical trials in chronic lung disease. Thorax 1987, 42, 773–778. [Google Scholar] [CrossRef] [Green Version]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the functional independence measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Beninato, M.; Gill-Body, K.M.; Salles, S.; Stark, P.C.; Black-Schaffer, R.M.; Stein, J. Determination of the Minimal Clinically Important Difference in the FIM Instrument in Patients With Stroke. Arch. Phys. Med. Rehabil. 2006, 87, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osborn, K.; Nothelle, S.; Slaven, J.E. Cumulative illness rating scale (cirs) can be used to predict hospital outcomes in older adults. J. Geriatr. Med. Gerontol. 2017, 3, 30. [Google Scholar] [CrossRef] [Green Version]
- Schunemann, H.J.; Griffith, L.; Jaeschke, R.; Goldstein, R.; Stubbing, D.; Guyatt, G.H. Evaluation of the minimal important difference for the feeling thermometer and the St. George’s Respiratory Questionnaire in patients with chronic airflow obstruction. J. Clin. Epidemiol. 2003, 56, 1170–1176. [Google Scholar] [CrossRef]
- McCormack, M.C.; Bascom, R.; Brandt, M.; Burgos, F.; Butler, S.; Caggiano, C.; Dimmock, A.E.F.; Fineberg, A.; Goldstein, J.; Guzman, F.C.; et al. Electronic Health Records and Pulmonary Function Data: Developing an Interoperability Roadmap. An Official American Thoracic Society Workshop Report. Ann. Am. Thorac. Soc. 2021, 18, 1–11. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Davis, M.D.; Walsh, B.K.; Sittig, S.E.; Restrepo, R.D. AARC Clinical Practice Guideline: Blood Gas Analysis and Hemoximetry: 2013. Respir. Care 2013, 58, 1694–1703. [Google Scholar] [CrossRef]
- WHO: Clinical Management of COVID-19. Available online: https://www.who.int/publications/i/item/clinical-management-of-COVID-19 (accessed on 18 October 2021).
- Maniscalco, M.; Fuschillo, S.; Ambrosino, P.; Martucci, M.; Papa, A.; Matera, M.G.; Cazzola, M. Preexisting cardiorespiratory comorbidity does not preclude the success of multidisciplinary rehabilitation in post-COVID-19 patients. Respir. Med. 2021, 184, 106470. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Holland, A.E.; Singh, S.J.; Tonia, T.; Wilson, K.C.; Troosters, T. COVID-19: Interim Guidance on Rehabilitation in the Hospital and Post-Hospital Phase from a European Respiratory Society and American Thoracic Society-coordinated Inter-national Task Force. Eur. Respir. J. 2020, 56, 2002197. [Google Scholar] [CrossRef]
- Li, Z.; Zheng, C.; Duan, C.; Zhang, Y.; Li, Q.; Dou, Z.; Li, J.; Xia, W. Rehabilitation needs of the first cohort of post-acute COVID-19 patients in Hubei, China. Eur. J. Phys. Rehabil. Med. 2020, 56, 339–344. [Google Scholar] [CrossRef]
- Kiekens, C.; Boldrini, P.; Andreoli, A.; Avesani, R.; Gamna, F.; Grandi, M.; Lombardi, F.; Lusuardi, M.; Molteni, F.; Perboni, A. Rehabilitation and respiratory management in the acute and early post-acute phase. “Instant paper from the field” on rehabilitation answers to the COVID-19 emergency. Eur. J. Phys. Rehabil. Med. 2020, 56, 323–326. [Google Scholar] [CrossRef]
- Rasekaba, T.; Lee, A.L.; Naughton, M.T.; Williams, T.J.; Holland, A.E. The six-minute walk test: A useful metric for the cardiopul-monary patient. Intern. Med. J. 2009, 39, 495–501. [Google Scholar] [CrossRef]
- Redelmeier, D.A.; Bayoumi, A.M.; Goldstein, R.S.; Guyatt, G.H. Interpreting small differences in functional status: The Six Minute Walk test in chronic lung disease patients. Am. J. Respir. Crit Care Med. 1997, 155, 1278–1282. [Google Scholar] [CrossRef]
- Spielmanns, M.; Gloeckl, R.; Schmoor, C.; Windisch, W.; Storre, J.H.; Boensch, M.; Kenn, K. Effects on pulmonary rehabilitation in patients with COPD or ILD: A retrospective analysis of clinical and functional predictors with particular emphasis on gen-der. Respir. Med. 2016, 113, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Skjørten, I.; Ankerstjerne, O.A.W.; Trebinjac, D.; Brønstad, E.; Rasch-Halvorsen, Ø.; Einvik, G.; Lerum, T.V.; Stavem, K.; Edvardsen, A.; Ingul, C.B. Cardiopulmonary exercise capacity and limitations 3 months after COVID-19 hospitalisation. Eur. Respir. J. 2021, 58, 2100996. [Google Scholar] [CrossRef]
- Tudoran, C.; Tudoran, M.; Pop, G.N.; Giurgi-Oncu, C.; Cut, T.G.; Lazureanu, V.E.; Oancea, C.; Parv, F.; Ciocarlie, T.; Bende, F. Associations between the Severity of the Post-Acute COVID-19 Syndrome and Echocardiographic Abnormalities in Previously Healthy Outpatients Following Infection with SARS-CoV-2. Biology 2021, 10, 469. [Google Scholar] [CrossRef]
- Qin, W.; Chen, S.; Zhang, Y.; Dong, F.; Zhang, Z.; Hu, B.; Zhu, Z.; Li, F.; Wang, X.; Wang, Y.; et al. Diffusion capacity abnormalities for carbon monoxide in patients with COVID-19 at three-month follow-up. Eur. Respir. J. 2021, 58. [Google Scholar] [CrossRef] [PubMed]
- Ramalho, S.H.R.; Shah, A.M. Lung function and cardiovascular disease: A link. Trends Cardiovasc. Med. 2021, 31, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Bay, M.L.; Pedersen, B.K. Muscle-organ crosstalk: Focus on immunometabolism. Front. Physiol. 2020, 11, 567881. [Google Scholar] [CrossRef]
- Huang, Y.; Tan, C.; Wu, J.; Chen, M.; Wang, Z.; Luo, L.; Zhou, X.; Liu, X.; Huang, X.; Yuan, S. Impact of coronavirus disease 2019 on pulmonary function in early convalescence phase. Respir. Res. 2020, 21, 163. [Google Scholar] [CrossRef] [PubMed]
- Tudoran, M.; Tudoran, C.; Lazureanu, V.E.; Marinescu, A.R.; Pop, G.N.; Pescariu, A.S.; Enache, A.; Cut, T.G. Alterations of Left Ventricular Function Persisting during Post-Acute COVID-19 in Subjects without Previously Diagnosed Cardiovascular Pathology. J. Pers. Med. 2021, 11, 225. [Google Scholar] [CrossRef] [PubMed]
- Carda, S.; Invernizzi, M.; Bavikatte, G.; Bensmail, D.; Bianchi, F.; Deltombe, T.; Draulans, N.; Esquenazi, A.; Francisco, G.E.; Gross, R.; et al. The role of physical and re-habilitation medicine in the COVID-19 pandemic: The clinician’s view. Ann. Phys. Rehabil. Med. 2020, 63, 554–556. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall | Responder | Non-Responder | p-Value | |
|---|---|---|---|---|
| n | 183 | 94 | 89 | |
| Age years (mean (SD)) | 68.99 (10.21) | 69.62 (10.09) | 68.45 (10.34) | 0.441 |
| BMI kg/m2 (mean (SD)) | 27.25 (5.5) | 27.38 (4.5) | 27.11 (6.4) | 0.746 |
| Sex, female (%) | 60 (33) | 27 (29) | 32 (36) | 0.375 |
| ICU-days (mean (SD)) | 9.23 (11.8) | 7.98 (10.6) | 10.65 (12.9) | 0.129 |
| Ventilation days (mean (SD)) | 5.65 (9.5) | 4.65 (8.0) | 6.78 (10.9) | 0.132 |
| Hospital days (mean (SD)) | 23.50 (13.5) | 21.46 (11.0) | 25.81 (15.4) | 0.29 |
| Rehabilitation days (mean (SD)) | 21.58 (8.7) | 21.39 (8.4) | 21.80 (9.1) | 0.755 |
| Therapy minutes/week | 1658 (1268) | 1752 (1393) | 1563 (1125) | 0.316 |
| 6-MWD admission % reference value (SD) | 53.11 (38.02) | 73.06 (35.96) | 32.04 (27.36) | <0.001 |
| 6-MWD admission meters (mean (SD)) | 187 (134) | 250 (126) | 119 (104) | <0.001 |
| Comorbidities | ||||
| non-smoker (%) | 132 (71.7) | 73 (77.7) | 58 (65.2) | 0.88 |
| COPD n (%) | 10 (5.5) | 3 (3.2) | 10 (11.2) | 0.3 |
| No COPD | 173 | 91 | 79 | |
| COPD stage I | 1 (0.6) | 0 (0.0) | 1 (1.2) | |
| COPD stage II | 3 (1.7) | 1 (1.1) | 2 (2.3) | |
| COPD stage III | 4 (2.2) | 1 (1.1) | 3 (3.5) | |
| COPD stage IV | 2 (1.1) | 1 (1.1) | 1 (1.2) | |
| Alcohol abuse n (%) | 13 (7.1) | 6 (6.4) | 7 (7.9) | 0.919 |
| Coronary Artery Disease n (%) | 32 (17.4) | 11 (11.7) | 21 (23.6) | 0.55 |
| Diabetes n (%) | 51 (27.7) | 22 (23.4) | 29 (32.6) | 0.223 |
| Peripheral Arterial Disease n (%) | 12 (6.5) | 4 (4.3) | 8 (9.0) | 0.320 |
| Atrial Fibrillation n (%) | 18 (9.8) | 5 (5.3) | 13 (14.6) | 0.63 |
| Stroke n (%) | 8 (4.3) | 3 (3.2) | 5 (5.6) | 0.659 |
| VTE n (%) | 4 (2.2) | 1 (0.0) | 3 (3.2) | 0.453 |
| Dyslipidaemia n (%) | 34 (18.5) | 15 (16.0) | 19 (21.3) | 0.455 |
| Arterial hypertension n (%) | 99 (53.8) | 47 (50.0) | 51 (57.3) | 0.400 |
| Pulmonary hypertension n (%) | 2 (1.1) | 1 (1.1) | 1 (1.1) | 1.000 |
| Psychiatric disease n (%) | 17 (9.2) | 9 (9.6) | 8 (9.0) | 1.000 |
| Renal failure n (%) | 31 (16.9) | 12 (12.8) | 19 (21.6) | 0.166 |
| CIRS pts (mean (SD)) | 12.74 (5.54) | 11.76 (5.02) | 13.80 (5.91) | 0.13 |
| Assessments | ||||
| HADS A (mean (SD)) | 5.28 (3.62) | 4.62 (3.07) | 5.91 (3.99) | 0.30 |
| HADS D (mean (SD)) | 5.52 (3.24) | 5.16 (3.00) | 5.88 (3.47) | 0.178 |
| CRQ (mean (SD)) | 4.71 (1.03) | 4.70 (1.10) | 4.71 (0.97) | 0.929 |
| FIM total (mean (SD)) | 98.12 (15.75) | 103.16 (12.33) | 92.93 (17.30) | <0.001 |
| FIM socio (mean (SD)) | 29.70 (5.87) | 30.63 (6.44) | 28.73 (5.09) | 0.29 |
| FIM motoric (mean (SD)) | 68.68 (12.89) | 73.04 (11.05) | 64.20 (13.20) | <0.001 |
| FT (mean (SD)) | 53.79 (16.99) | 52.96 (17.05) | 54.91 (16.87) | 0.468 |
| Overall | Responder | Non-Responder | p-Value | |
|---|---|---|---|---|
| Pulmonary function testing (PFT) | ||||
| FEV1% pred. (mean (SD)) | 74.28 (21.59) | 83.16 (19.43) | 63.07 (18.91) | <0.001 |
| FVC% pred. (mean (SD)) | 71.88 (20.76) | 80.03 (18.60) | 61.59 (18.79) | <0.001 |
| FEV1% FVC (mean (SD)) | 80.28 (10.74) | 80.53 (9.24) | 79.97 (12.45) | 0.760 |
| DLCO% pred. (mean (SD)) | 56.35 (17.81) | 62.33 (17.94) | 46.95 (13.02) | <0.001 |
| Laboratory Parameters | ||||
| PaO2 kPa (mean (SD)) | 9.55 (6.50) | 9.15 (1.81) | 9.97 (9.14) | 0.433 |
| PaCO2 kPa (mean (SD)) | 4.53 (0.77) | 4.47 (0.72) | 4.58 (0.81) | 0.405 |
| SpO2 % (mean (SD)) | 93.46 (2.94) | 93.55 (2.80) | 93.36 (3.11) | 0.658 |
| Procalcitonin ng/mL (mean (SD)) | 1.44 (4.31) | 0.59 (0.74) | 2.46 (6.23) | 0.25 |
| CRP mg/dL (mean (SD)) | 139.87 (109.79) | 131.78 (97.72) | 149.12 (121.76) | 0.292 |
| Creatinine mg/L (mean (SD)) | 118.08 (109.49) | 107.92 (78.66) | 129.55 (134.53) | 0.183 |
| Ferritin mg/L (mean (SD)) | 1536.85 (1552.31) | 1513.36 (1644.27) | 1570.07 (1431.46) | 0.859 |
| Hemoglobin g/L (mean (SD)) | 104.47 (23.25) | 107.46 (23.88) | 101.10 (22.27) | 0.65 |
| Leukocytes ×109/L (mean (SD)) | 12.31 (6.06) | 11.53 (5.69) | 13.20 (6.34) | 0.62 |
| Thrombocytes ×109/L (mean (SD)) | 211.35 (94.09) | 205.67 (93.40) | 213.66 (89.01) | 0.555 |
| CPK U/L (mean (SD)) | 415.84 (742.37) | 435.63 (762.69) | 392.38 (725.81) | 0.780 |
| D-dimer µ/L (mean (SD)) | 5.98 (13.08) | 4.67 (8.28) | 7.54 (17.09) | 0.241 |
| Sodium mEq/L (mean (SD)) | 136.67 (4.65) | 136.53 (4.76) | 136.79 (4.57) | 0.713 |
| Potassium mEq/L (mean (SD)) | 4.12 (0.52) | 4.02 (0.50) | 4.23 (0.51) | 0.6 |
| Protein g/dL (mean (SD)) | 70.74 (47.25) | 74.71 (46.68) | 65.97 (49.12) | 0.605 |
| Overall | Responder | Non-Responder | p-Value | |
|---|---|---|---|---|
| n | 183 | 94 | 89 | |
| 6MWD at discharge % reference value (SD) | 98.55 (37.78) | 126.87 (22.54) | 68.63 (25.56) | <0.001 |
| Δ6MWD meter (mean (SD)) | 154.20 (101.11) | 175.80 (109.13) | 131.65 (87.49) | 0.003 |
| ∆6-MWD meter >54 m (minimal important difference) n (%) | 156 (84.8) | 81 (86.2) | 74 (83.1) | 0.717 |
| ΔFIM tot (mean (SD)) | 15.36 (13.99) | 14.85 (14.69) | 15.76 (13.24) | 0.666 |
| ΔFIM motoric (mean (SD)) | 12.27 (10.79) | 10.68 (9.99) | 13.86 (11.40) | 0.048 |
| ΔFT (mean (SD)) | 21.12 (14.46) | 22.53 (15.32) | 19.67 (13.41) | 0.242 |
| Overall | Responder | Non-Responder | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | 183 | 94 | 89 | ||||||
| Pre | Post | p | Pre | Post | p | Pre | Post | p | |
| 6-MWD meter (mean (SD)) | 187.25 (133.77) | 341.42 (131.80) | <0.001 | 250.35 (126.45) | 426.10 (83.40) | <0.001 | 118.55 (104.45) | 250.20 (111.41) | <0.001 |
| FIM tot. (mean (SD)) | 98.12 (15.75) | 113.51 (12.94) | <0.001 | 103.16 (12.33) | 117.11 (8.30) | <0.001 | 92.93 (17.30) | 109.51 (15.81) | <0.001 |
| FIM motoric (mean (SD)) | 68.68 (12.89) | 81.22 (10.75) | <0.001 | 73.04 (11.05) | 83.72 (8.78) | <0.001 | 64.20 (13.20) | 78.41 (12.08) | <0.001 |
| FT degrees (mean (SD)) | 53.79 (16.99) | 75.18 (13.14) | <0.001 | 52.96 (17.05) | 75.24 (13.52) | <0.001 | 54.91 (16.87) | 75.62 (12.18) | <0.001 |
| Model without FVC (n = 181) | Model with FVC (n = 136) | |||
|---|---|---|---|---|
| Odds Ratios [95% CI] | p | Odds Ratios [95% CI] | p | |
| ICU days | 0.98 [0.92–1.04] | 0.564 | 0.98 [0.91–1.06] | 0.638 |
| Hospital days | 1.02 [0.96–1.07] | 0.587 | 1.00 [0.93–1.07] | 0.977 |
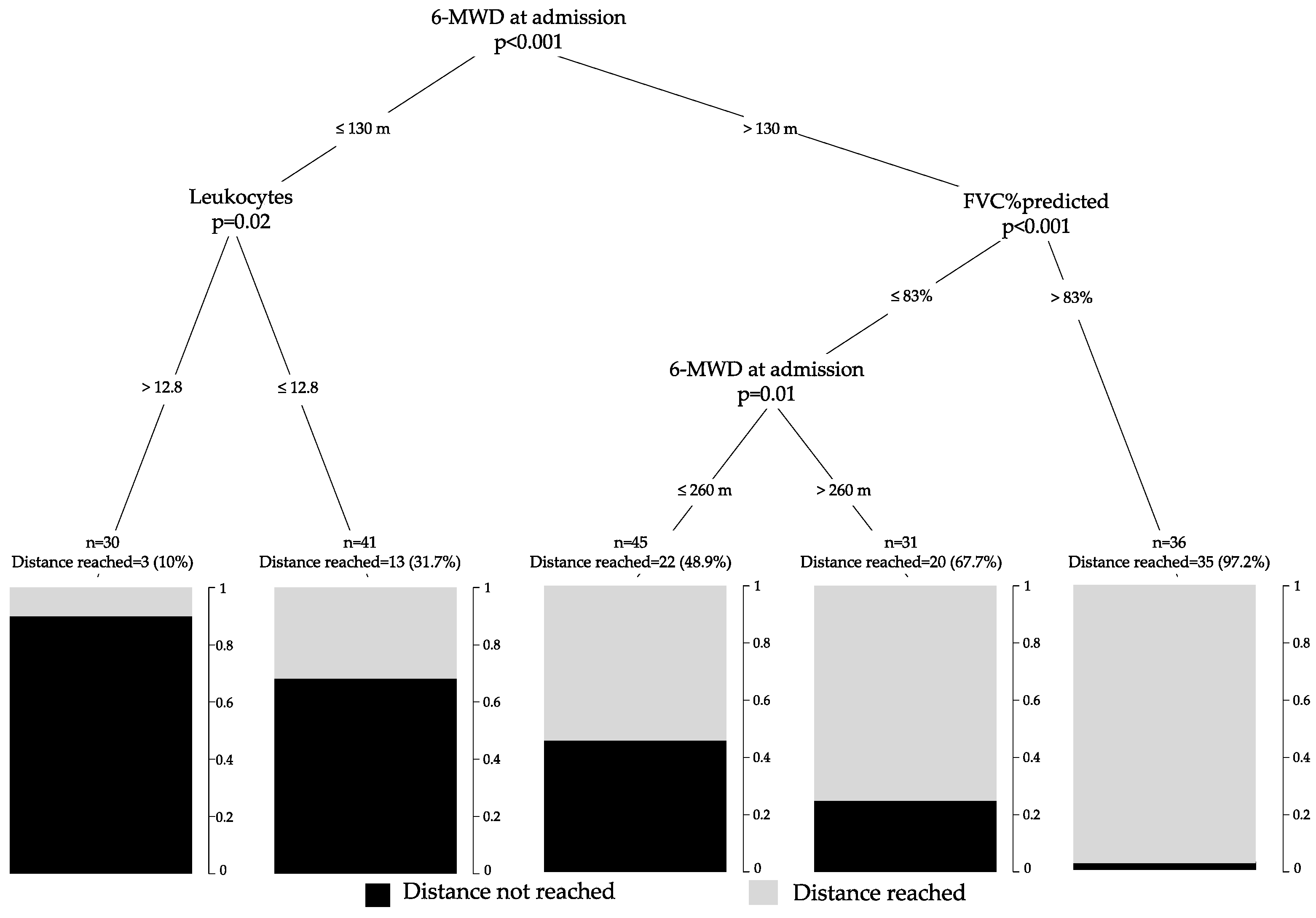
| 6MWD admission (per meter) | 0.99 [0.99–1.00] | <0.001 | 0.99 [0.99–1.00] | 0.002 |
| Smoker (non-smoker) | 0.57 [0.25–1.32] | 0.193 | 0.64 [0.22–1.83] | 0.403 |
| CAD | 1.50 [0.57–4.05] | 0.415 | 2.39 [0.72–8.55] | 0.163 |
| Arterial fibrillation | 2.76 [0.74–11.44] | 0.140 | 3.85 [0.73–23.18] | 0.121 |
| FIM motoric (per each point) | 0.96 [0.93–0.99] | 0.020 | 0.93 [0.88–0.97] | 0.004 |
| Hemoglobin | 1.01 [0.99–1.03] | 0.474 | 1.01 [0.98–1.03] | 0.633 |
| Leukocytes | 1.06 [0.99–1.13] | 0.084 | 1.03 [0.93–1.13] | 0.549 |
| Potassium | 1.57 [0.79–3.27] | 0.206 | 1.32 [0.49–3.66] | 0.578 |
| FVC % pred | 0.95 [0.93–0.97] | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spielmanns, M.; Buelow, M.M.; Pekacka-Egli, A.M.; Cecon, M.; Spielmanns, S.; Windisch, W.; Hermann, M. Clinical and Functional Predictors of Response to a Comprehensive Pulmonary Rehabilitation in Severe Post-COVID-19 Patients. Microorganisms 2021, 9, 2452. https://doi.org/10.3390/microorganisms9122452
Spielmanns M, Buelow MM, Pekacka-Egli AM, Cecon M, Spielmanns S, Windisch W, Hermann M. Clinical and Functional Predictors of Response to a Comprehensive Pulmonary Rehabilitation in Severe Post-COVID-19 Patients. Microorganisms. 2021; 9(12):2452. https://doi.org/10.3390/microorganisms9122452
Chicago/Turabian StyleSpielmanns, Marc, Melissa Masha Buelow, Anna Maria Pekacka-Egli, Mikis Cecon, Sabine Spielmanns, Wolfram Windisch, and Matthias Hermann. 2021. "Clinical and Functional Predictors of Response to a Comprehensive Pulmonary Rehabilitation in Severe Post-COVID-19 Patients" Microorganisms 9, no. 12: 2452. https://doi.org/10.3390/microorganisms9122452