
The Combined Use of Cytokine Serum Values with Laboratory Parameters Improves Mortality Prediction of COVID-19 Patients: The Interleukin-15-to-Albumin Ratio

 , , ,
, , ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
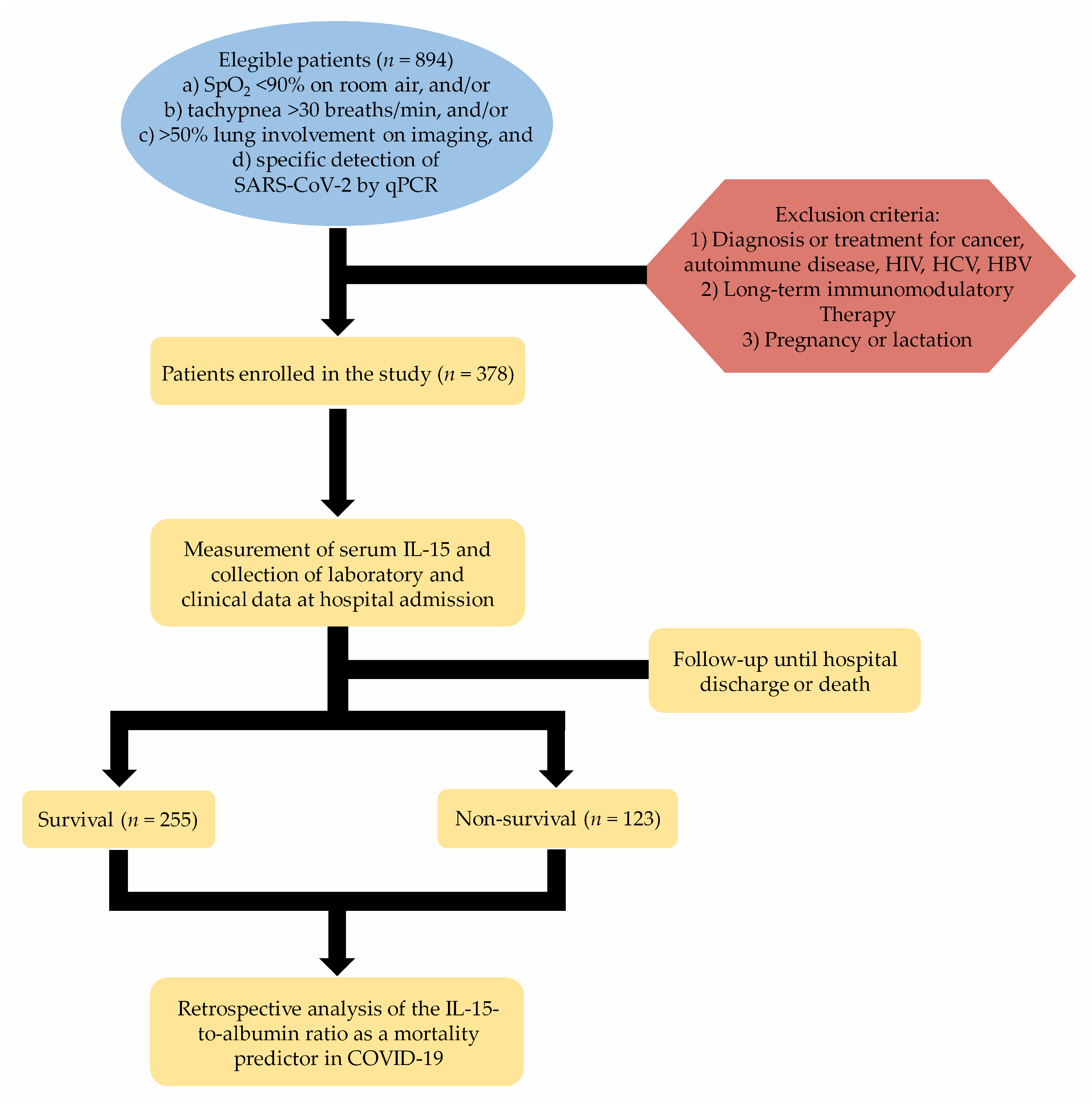
2.1. Patients
2.2. Data Collection
2.3. Laboratory Parameters
2.4. IL-15 Serum Levels
2.5. Statistics
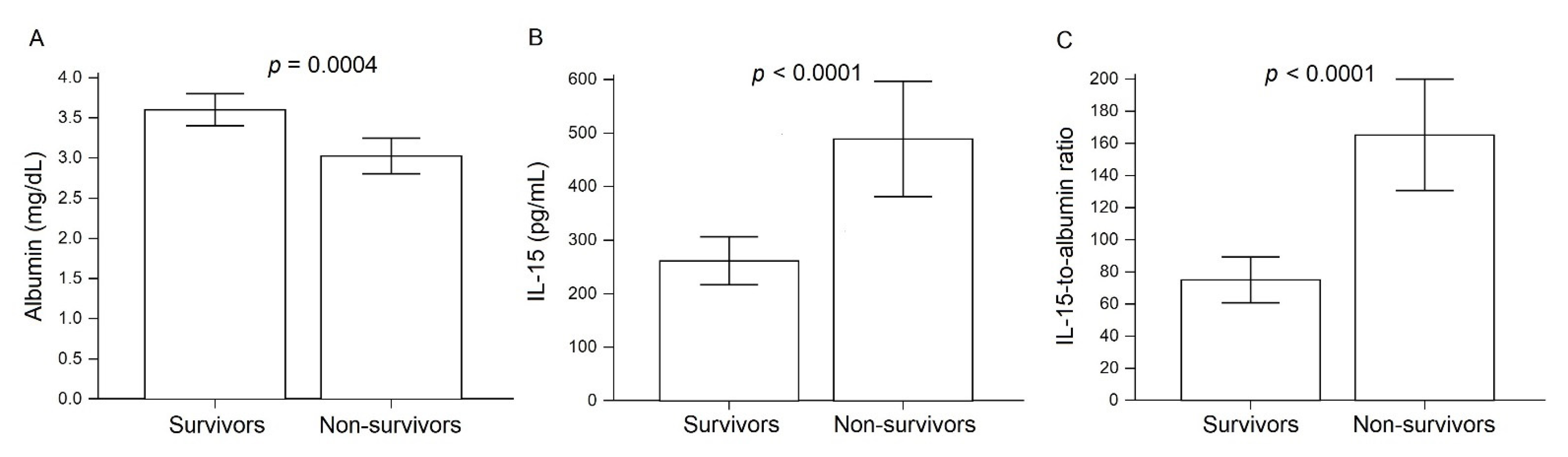
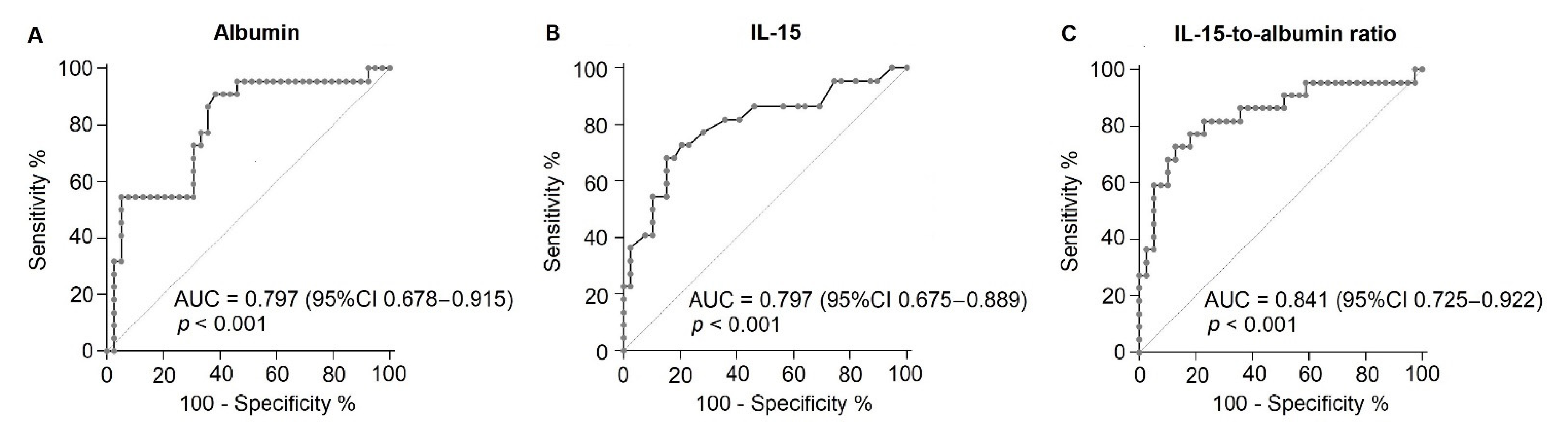
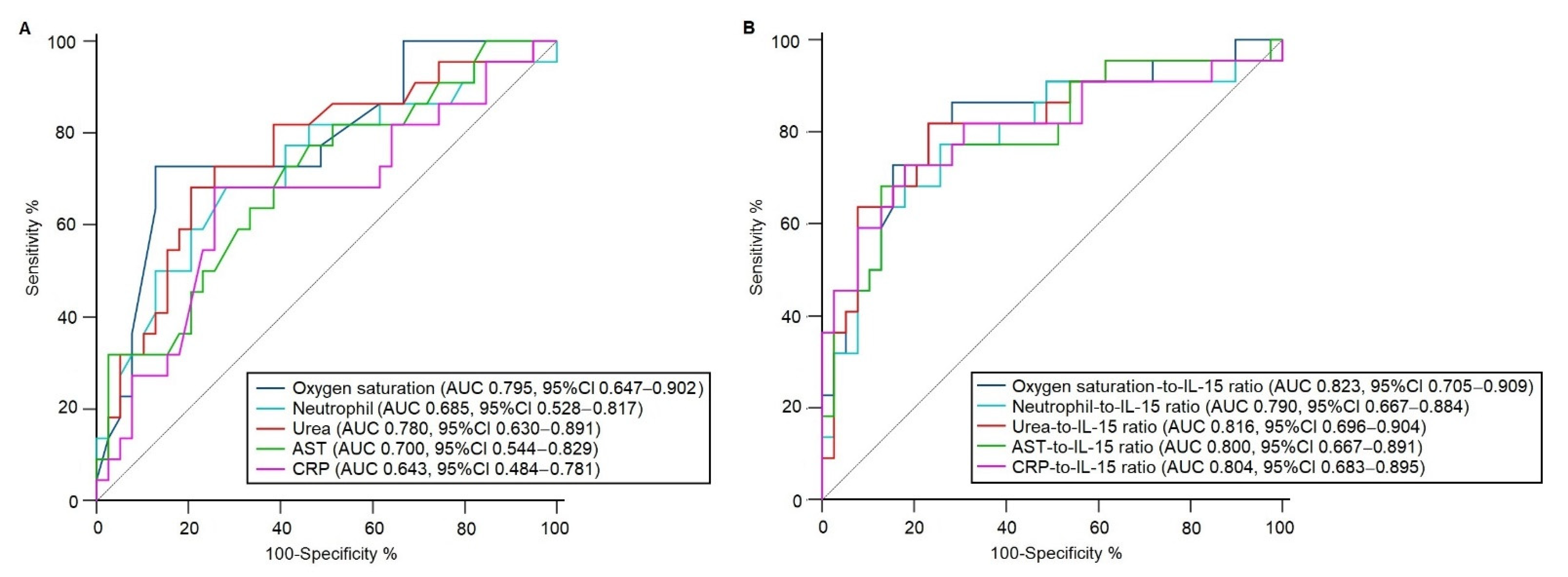
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karlinsky, A.; Kobak, D. Tracking excess mortality across countries during the COVID-19 pandemic with the World Mortality Dataset. eLife 2021, 10, e69336. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Chaibakhsh, S.; Pourhoseingholi, A.; Vahedi, M. Global Incidence and Mortality Rate of COVID-19; Special Focus on Iran, Italy and China. Arch. Iran. Med. 2020, 23, 455–461. [Google Scholar] [CrossRef]
- Dahal, S.; Banda, J.M.; Bento, A.I.; Mizumoto, K.; Chowell, G. Characterizing all-cause excess mortality patterns during COVID-19 pandemic in Mexico. BMC Infect. Dis. 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Özdemir, I.H.; Özlek, B.; Özen, M.B.; Gündüz, R.; Çetin, N.; Özlek, E.; Yıldız, B.S.; Bilge, A.R. Prognostic value of C-reactive protein/albumin ratio in hypertensive COVID-19 patients. Clin. Exp. Hypertens. 2021, 43, 1–7. [Google Scholar] [CrossRef]
- Varim, C.; Yaylaci, S.; Demirci, T.; Kaya, T.; Nalbant, A.; Dheir, H.; Senocak, D.; Kurt, R.; Cengiz, H.; Karacaer, C. Neutrophil count to albumin ratio as a new predictor of mortality in patients with COVID-19 ınfection. Rev. Assoc. Médica Bras. 2020, 66, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Angioni, R.; Sánchez-Rodríguez, R.; Munari, F.; Bertoldi, N.; Arcidiacono, D.; Cavinato, S.; Marturano, D.; Zaramella, A.; Realdon, S.; Cattelan, A.; et al. Age-severity matched cytokine profiling reveals specific signatures in Covid-19 patients. Cell Death Dis. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Masselli, E.; Vitale, M. NK cells on the ViP stage of COVID-19. EBioMedicine 2021, 69, 103458. [Google Scholar] [CrossRef] [PubMed]
- Soraya, G.V.; Ulhaq, Z.S. Crucial laboratory parameters in COVID-19 diagnosis and prognosis: An updated meta-analysis. Med. Clínica 2020, 155, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Cheng, A.; Kumar, R.; Fang, Y.; Chen, G.; Zhu, Y.; Lin, S. Hypoalbuminemia predicts the outcome of COVID-19 independent of age and co-morbidity. J. Med. Virol. 2020, 92, 2152–2158. [Google Scholar] [CrossRef] [PubMed]
- Violi, F.; Cangemi, R.; Romiti, G.F.; Ceccarelli, G.; Oliva, A.; Alessandri, F.; Pirro, M.; Pignatelli, P.; Lichtner, M.; Carraro, A.; et al. Is Albumin Predictor of Mortality in COVID-19? Antioxid. Redox Signal. 2021, 35, 139–142. [Google Scholar] [CrossRef]
- Perera, P.-Y.; Lichy, J.H.; Waldmann, T.A.; Perera, L.P. The role of interleukin-15 in inflammation and immune responses to infection: Implications for its therapeutic use. Microbes Infect. 2012, 14, 247–261. [Google Scholar] [CrossRef] [Green Version]
- Jabri, B.; Abadie, V. IL-15 functions as a danger signal to regulate tissue-resident T cells and tissue destruction. Nat. Rev. Immunol. 2015, 15, 771–783. [Google Scholar] [CrossRef] [PubMed]
- Abers, M.S.; Delmonte, O.M.; Ricotta, E.E.; Fintzi, J.; Fink, D.L.; de Jesus, A.A.A.; Zarember, K.A.; Alehashemi, S.; Oikonomou, V.; Desai, J.V.; et al. An immune-based biomarker signature is associated with mortality in COVID-19 patients. JCI Insight 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Kandikattu, H.K.; Venkateshaiah, S.U.; Kumar, S.; Mishra, A. IL-15 immunotherapy is a viable strategy for COVID-19. Cytokine Growth Factor Rev. 2020, 54, 24–31. [Google Scholar] [CrossRef]
- Huang, W.; Li, C.; Wang, Z.; Wang, H.; Zhou, N.; Jiang, J.; Ni, L.; Zhang, X.A.; Wang, D.-W. Decreased serum albumin level indicates poor prognosis of COVID-19 patients: Hepatic injury analysis from 2,623 hospitalized cases. Sci. China Life Sci. 2020, 63, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.-L.; Hou, Y.-L.; Li, D.-T.; Li, F.-Z. Laboratory findings of COVID-19: A systematic review and meta-analysis. Scand. J. Clin. Lab. Investig. 2020, 80, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hou, H.; Zhang, B.; Huang, H.; Luo, Y.; Wu, S.; Tang, G.; Liu, W.; Mao, L.; Wang, F.; Sun, Z. Using IL-2R/lymphocytes for predicting the clinical progression of patients with COVID-19. Clin. Exp. Immunol. 2020, 201, 76–84. [Google Scholar] [CrossRef]
- Luo, M.; Liu, J.; Jiang, W.; Yue, S.; Liu, H.; Wei, S. IL-6 and CD8+ T cell counts combined are an early predictor of in-hospital mortality of patients with COVID-19. JCI Insight 2020, 5, 5. [Google Scholar] [CrossRef]
- Küçükceran, K.; Ayrancı, M.K.; Girişgin, A.S.; Koçak, S.; Dündar, Z.D. The role of the BUN/albumin ratio in predicting mortality in COVID-19 patients in the emergency department. Am. J. Emerg. Med. 2021, 48, 33–37. [Google Scholar] [CrossRef]
- Hu, W.-H.; Eisenstein, S.; Parry, L.; Ramamoorthy, S. Preoperative malnutrition with mild hypoalbuminemia associated with postoperative mortality and morbidity of colorectal cancer: A propensity score matching study. Nutr. J. 2019, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.R.; Machado, M.V. New Insights About Albumin and Liver Disease. Ann. Hepatol. 2018, 17, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Egbert, R.C.; Bouck, T.T.; Gupte, N.; Pena, M.M.; Dang, K.H.; Ornell, S.S.; Zelle, B.A. Hypoalbuminemia and Obesity in Orthopaedic Trauma Patients: Body Mass Index a Significant Predictor of Surgical Site Complications. Sci. Rep. 2020, 10, 1953–1957. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Hypoalbuminemia and the Risk of Acute Kidney Injury in Sepsis. Crit. Care Med. 2019, 47, e377–e378. [Google Scholar] [CrossRef]
- Furukawa, M.; Kinoshita, K.; Yamaguchi, J.; Hori, S.; Sakurai, A. Sepsis patients with complication of hypoglycemia and hypoalbuminemia are an early and easy identification of high mortality risk. Intern. Emerg. Med. 2019, 14, 539–548. [Google Scholar] [CrossRef]
- Nicholson, J.; Wolmarans, M.; Park, G. The role of albumin in critical illness. Br. J. Anaesth. 2000, 85, 599–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, A.D.; Buck, M.; Feitelberg, S.P.; Chojkier, M. Tumor necrosis factor-alpha inhibits albumin gene expression in a murine model of cachexia. J. Clin. Investig. 1990, 85, 248–255. [Google Scholar] [CrossRef]
- Bartalena, L.; Farsetti, A.; Flink, I.L.; Robbins, J. Effects of interleukin-6 on the expression of thyroid hormone-binding protein genes in cultured human hepatoblastoma-derived (Hep G2) cells. Mol. Endocrinol. 1992, 6, 935–942. [Google Scholar] [CrossRef] [Green Version]
- Franch-Arcas, G. The meaning of hypoalbuminaemia in clinical practice. Clin. Nutr. 2001, 20, 265–269. [Google Scholar] [CrossRef]
- Alunno, A.; Carubbi, F.; Rodríguez-Carrio, J. Storm, typhoon, cyclone or hurricane in patients with COVID-19? Beware of the same storm that has a different origin. RMD Open 2020, 6, e001295. [Google Scholar] [CrossRef]
- Badolato, R.; Ponzi, A.N.; Millesimo, M.; Notarangelo, L.D.; Musso, T. Interleukin-15 (IL-15) Induces IL-8 and Monocyte Chemotactic Protein 1 Production in Human Monocytes. Blood 1997, 90, 2804–2809. [Google Scholar] [CrossRef]
- Cavalcante-Silva, L.H.A.; Carvalho, D.C.M.; Lima, É.D.A.; Galvão, J.G.F.M.; Silva, J.S.D.F.D.; de Sales-Neto, J.M.; Rodrigues-Mascarenhas, S. Neutrophils and COVID-19: The road so far. Int. Immunopharmacol. 2020, 90, 107233. [Google Scholar] [CrossRef] [PubMed]
- Knoll, R.; Schultze, J.L.; Schulte-Schrepping, J. Monocytes and Macrophages in COVID-19. Front. Immunol. 2021, 12, 2952. [Google Scholar] [CrossRef]
- Chen, J.; Li, D.; Zhang, X.; Mehta, J.L. Tumor Necrosis Factor-α-Induced Apoptosis of Human Coronary Artery Endothelial Cells: Modulation by the Peroxisome Proliferator-Activated Receptor-γ Ligand Pioglitazone. J. Cardiovasc. Pharmacol. Ther. 2004, 9, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Polunovsky, V.A.; Wendt, C.H.; Ingbar, D.H.; Peterson, M.S.; Bitterman, P.B. Induction of Endothelial Cell Apoptosis by TNFα: Modulation by Inhibitors of Protein Synthesis. Exp. Cell Res. 1994, 214, 584–594. [Google Scholar] [CrossRef]
- Munshi, N.; Fernandis, A.Z.; Cherla, R.P.; Park, I.-W.; Ganju, R.K. Lipopolysaccharide-Induced Apoptosis of Endothelial Cells and Its Inhibition by Vascular Endothelial Growth Factor. J. Immunol. 2002, 168, 5860–5866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assaly, R.; Olson, D.; Hammersley, J.; Fan, P.-S.; Liu, J.; Shapiro, J.I.; Kahaleh, M.B. Initial Evidence of Endothelial Cell Apoptosis as a Mechanism of Systemic Capillary Leak Syndrome. Chest 2001, 120, 1301–1308. [Google Scholar] [CrossRef]
- de Chambrun, M.P.; Cohen-Aubart, F.; Donker, D.W.; Cariou, P.-L.; Luyt, C.-E.; Combes, A.; Amoura, Z. SARS-CoV-2 Induces Acute and Refractory Relapse of Systemic Capillary Leak Syndrome (Clarkson’s Disease). Am. J. Med. 2020, 133, e663–e664. [Google Scholar] [CrossRef]
- Singh, A.K.; Kasarpalkar, N.; Bhowmick, S.; Paradkar, G.; Talreja, M.; Shah, K.; Tiwari, A.; Palav, H.; Kaginkar, S.; Kul-karni, R.; et al. IL-15 and sMAdCAM: Novel roles in COVID-19 pathogenesis. medRxiv 2021. [Google Scholar] [CrossRef]
- Raimondi, F.; Novelli, L.; Ghirardi, A.; Russo, F.M.; Pellegrini, D.; Biza, R.; Trapasso, R.; Giuliani, L.; Anelli, M.; Amoroso, M.; et al. Covid-19 and gender: Lower rate but same mortality of severe disease in women—an observational study. BMC Pulm. Med. 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Nyabera, A.; Lakhdar, S.; Li, M.; Trandafirescu, T.; Tall, S.O. The Association Between BMI and Inpatient Mortality Outcomes in Older Adults With COVID-19. Cureus 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Zhang, J.; Wang, M.; Chen, L. Obesity is associated with severe COVID-19 but not death: A dose−response meta-analysis. Epidemiol. Infect. 2021, 149, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.; Yang, J.; Shi, J.; Zhang, P.; Wang, X. Obesity is associated with increased severity of disease in COVID-19 pneumonia: A systematic review and meta-analysis. Eur. J. Med. Res. 2020, 25, 1–15. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Total (n = 378) | Survival (n = 255) | Non-Survival (n = 123) | p Value |
|---|---|---|---|---|
| Gender (W/M) | 137/241 | 97/158 | 40/83 | 0.3 |
| Age (years) | 54 ± 13.7 | 51.4 ± 13.2 | 58.9 ± 13.7 | <0.001 * |
| BMI (kg/m2) | 26.7 ± 4.8 | 25.8 ± 6.7 | 27.5 ± 4.4 | 0.3 |
| Heart rate (bpm) | 89 ± 13.2 | 87.7 ± 12.9 | 92 ± 13.5 | 0.005 * |
| Breathing rate (bpm) | 24.1 ± 4.1 | 23.6 ± 3.9 | 25.2 ± 4.5 | 0.001 * |
| Oxygen saturation (%) | 83 ± 9.5 | 84.5 ± 8.7 | 79.8 ± 12.5 | <0.001 * |
| ICU needing (%) | 143 (37.8) | 60 (23.5) | 84 (68.3) | <0.001 * |
| Inpatient days | 12.1 ± 9.2 | 14.7 ± 9.9 | 7.3 ± 5.2 | 0.014 * |
| Parameters | Total (n = 378) | Survival (n = 255) | Non-Survival (n = 123) | p Value |
|---|---|---|---|---|
| Neutrophils (×103/mL) | 8.6 ± 5.6 | 6.7 ± 3.9 | 12 ± 6.7 | <0.001 |
| Urea (mg/dL) | 59.8 ± 54.7 | 35.1 ± 14.1 | 96.8 ± 70.8 | <0.001 |
| Uric Acid (mg/dL) | 6.2 ± 3.1 | 5.2 ± 1.7 | 8 ± 4.3 | 0.001 |
| AST (IU/L) | 37.2 ± 19 | 33 ± 15.3 | 46 ± 23 | 0.008 |
| ALP (IU/L) | 93.3 ± 33.2 | 84.8 ± 28.3 | 109.9 ± 36.4 | 0.003 |
| LDH (IU/L) | 393.3 ± 224.9 | 311.2 ± 144.4 | 539 ± 268.2 | 0.001 |
| CK-MB (IU/L) | 22.1 ± 7.8 | 19.8 ± 5.6 | 27 ± 9.9 | 0.002 |
| BNP (pg/mL) | 151.2 ± 304.6 | 19.1 ± 11.5 | 291.4 ± 396.4 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizo-Téllez, S.A.; Méndez-García, L.A.; Rivera-Rugeles, A.C.; Miranda-García, M.; Manjarrez-Reyna, A.N.; Viurcos-Sanabria, R.; Solleiro-Villavicencio, H.; Becerril-Villanueva, E.; Carrillo-Ruíz, J.D.; Cota-Arce, J.M.; et al. The Combined Use of Cytokine Serum Values with Laboratory Parameters Improves Mortality Prediction of COVID-19 Patients: The Interleukin-15-to-Albumin Ratio. Microorganisms 2021, 9, 2159. https://doi.org/10.3390/microorganisms9102159
Rizo-Téllez SA, Méndez-García LA, Rivera-Rugeles AC, Miranda-García M, Manjarrez-Reyna AN, Viurcos-Sanabria R, Solleiro-Villavicencio H, Becerril-Villanueva E, Carrillo-Ruíz JD, Cota-Arce JM, et al. The Combined Use of Cytokine Serum Values with Laboratory Parameters Improves Mortality Prediction of COVID-19 Patients: The Interleukin-15-to-Albumin Ratio. Microorganisms. 2021; 9(10):2159. https://doi.org/10.3390/microorganisms9102159
Chicago/Turabian StyleRizo-Téllez, Salma A., Lucia A. Méndez-García, Ana C. Rivera-Rugeles, Marcela Miranda-García, Aarón N. Manjarrez-Reyna, Rebeca Viurcos-Sanabria, Helena Solleiro-Villavicencio, Enrique Becerril-Villanueva, José D. Carrillo-Ruíz, Julian M. Cota-Arce, and et al. 2021. "The Combined Use of Cytokine Serum Values with Laboratory Parameters Improves Mortality Prediction of COVID-19 Patients: The Interleukin-15-to-Albumin Ratio" Microorganisms 9, no. 10: 2159. https://doi.org/10.3390/microorganisms9102159