Eosinopenia in COVID-19 Patients: A Retrospective Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
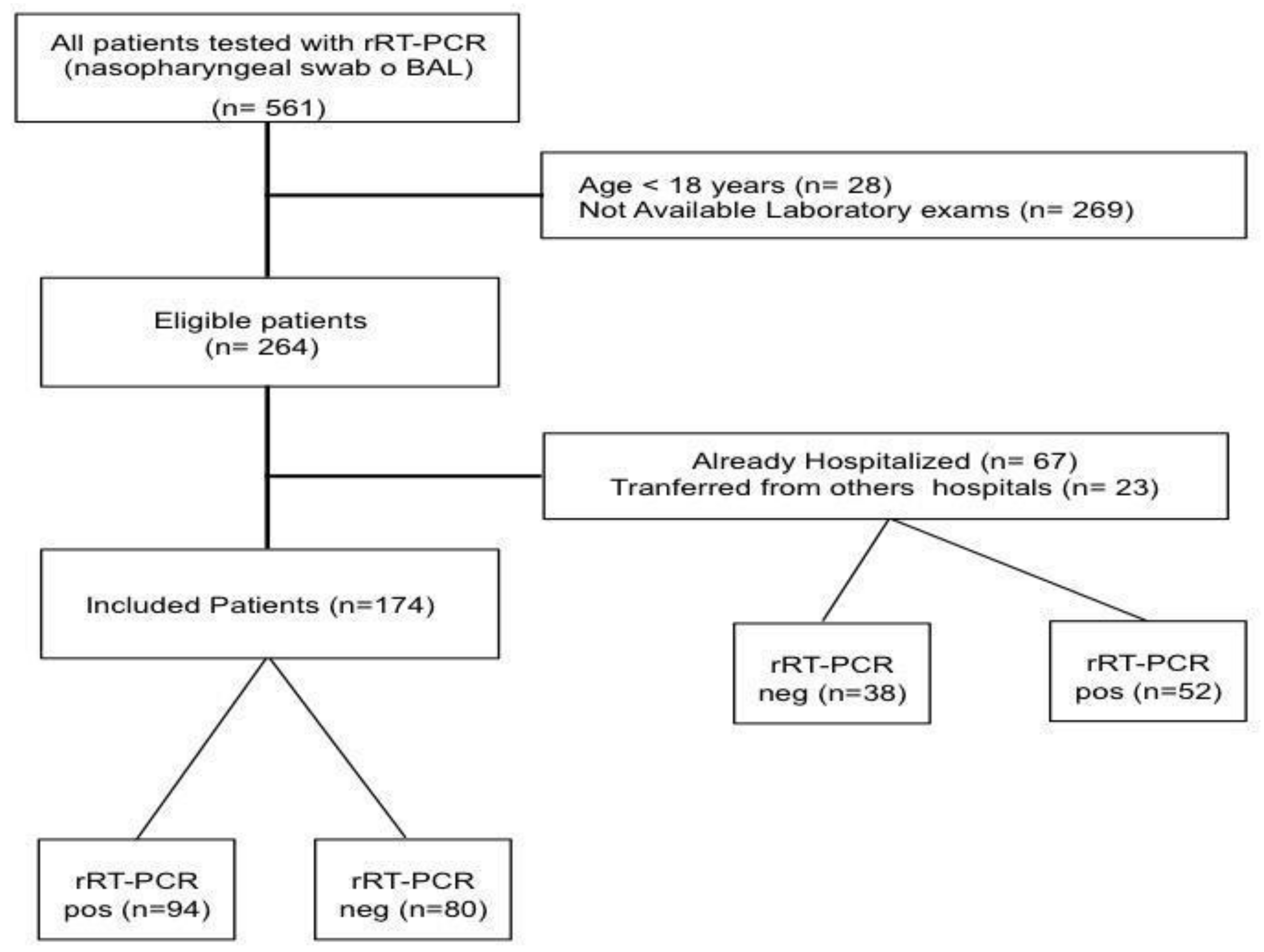
2.2. Study Population
2.3. Data Collection
2.4. Outcome Assessment
2.5. Statistical Analysis
2.6. Availability of Data and Materials
3. Results
3.1. Study Population
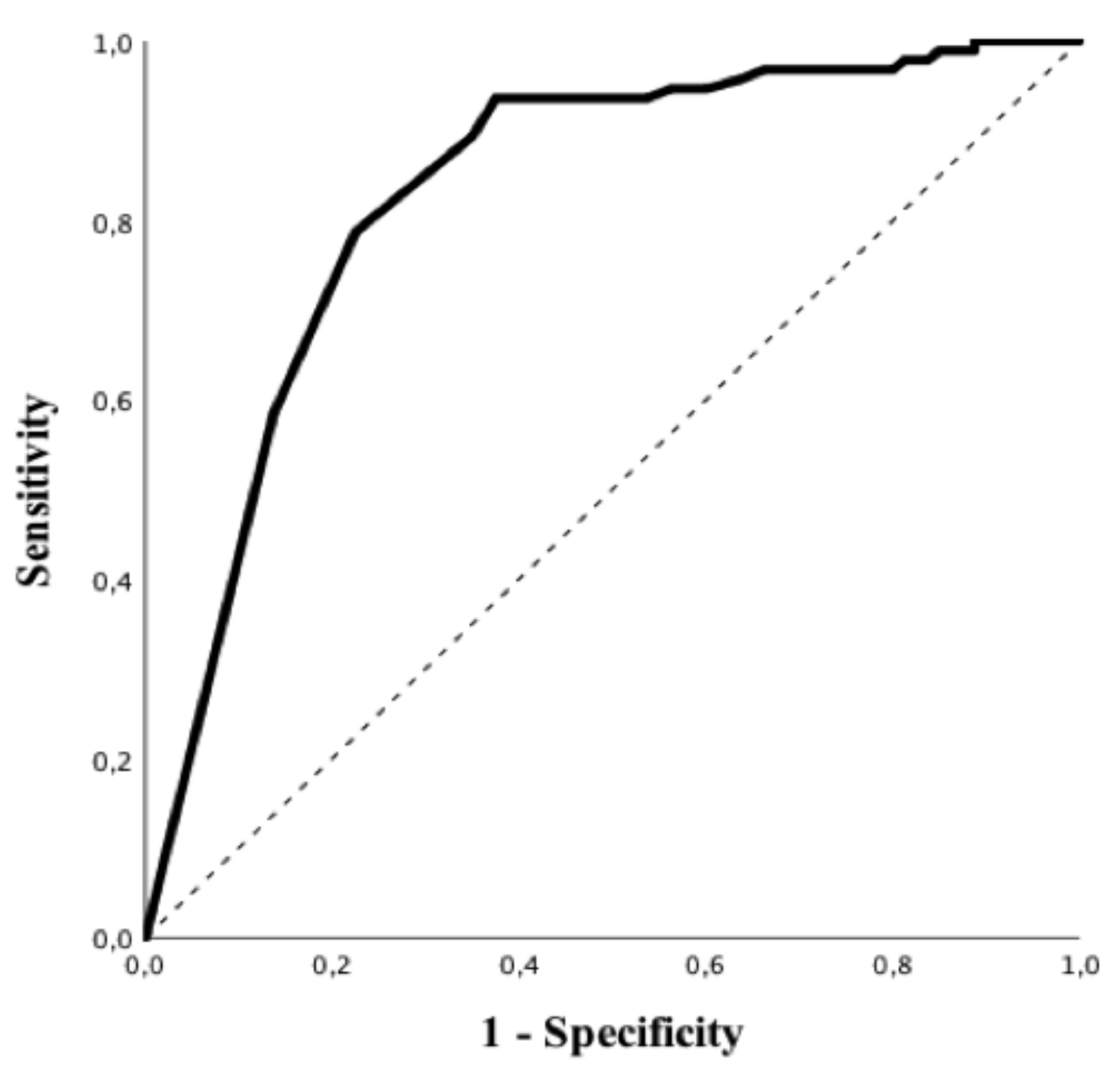
3.2. Eosinophils and RT-PCR
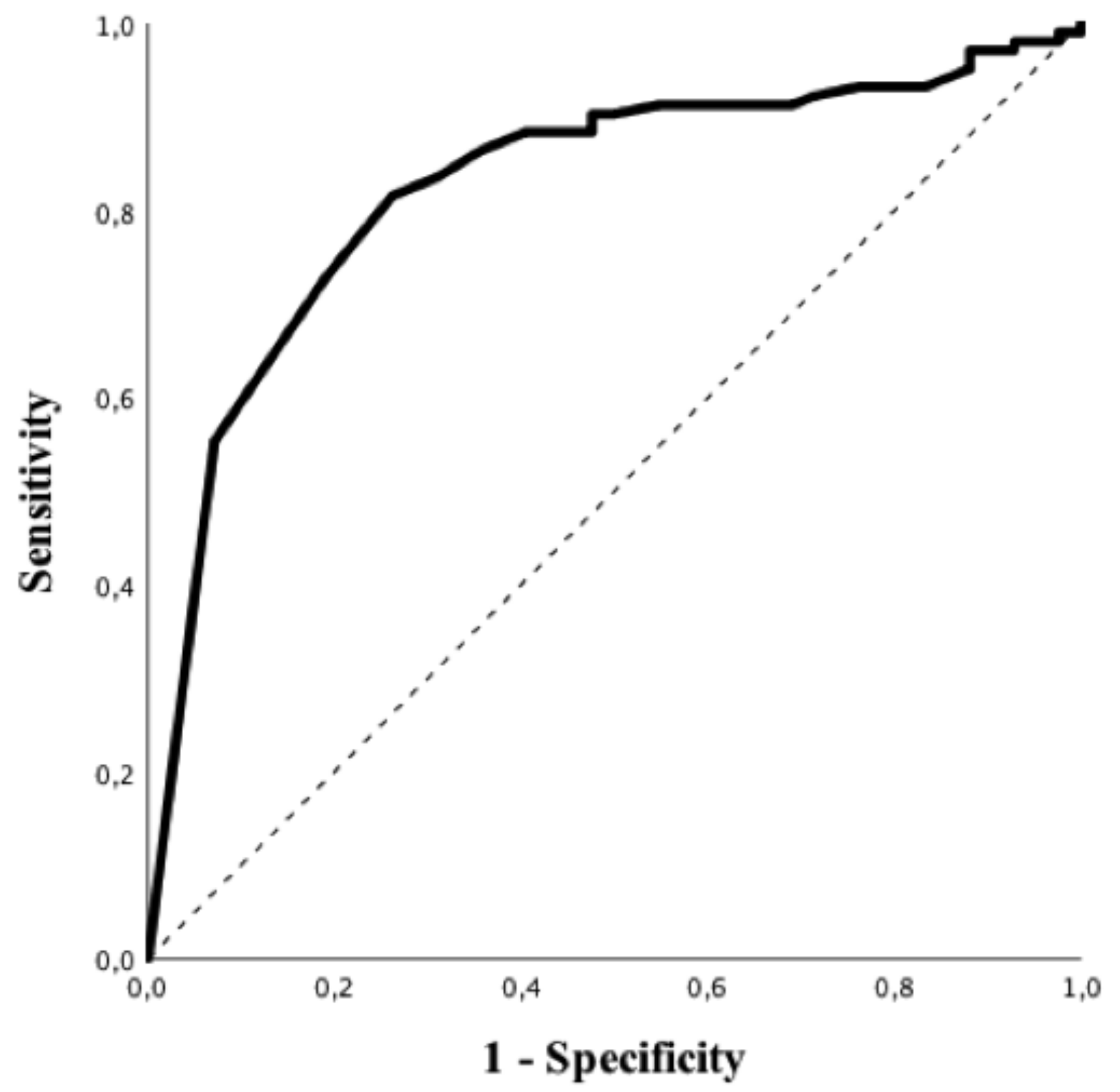
3.3. Eosinophils and Chest CT-Scan
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Novel-Coronavirus—China. Available online: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 14 November 2020).
- Shereen, M.A.; Khan, S.; Kazmi, A.; Bashir, N.; Siddique, R. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J. Adv. Res. 2020, 24, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Coronavirus Disease (COVID-19) Situational Report 51. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed on 13 October 2020).
- JHU CSSE. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. 2020. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 28 October 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, W.-H.; Guan, W.-J.; Li, C.-C.; Li, Y.-M.; Liang, H.-R.; Zhao, Y.; Liu, X.-Q.; Sang, L.; Chen, R.-C.; Tang, C.-L.; et al. Clinical characteristics and outcomes of hospitalised patients with COVID-19 treated in Hubei (epicentre) and outside Hubei (non-epicentre): A nationwide analysis of China. Eur. Respir. J. 2020, 55, 2000562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (nCoV) Infection Is Suspected: Interim Guidance, 25 January 2020. Available online: https://apps.who.int/iris/handle/10665/330854 (accessed on 30 March 2020).
- Li, Y.; Yao, L.; Li, J.; Chen, L.; Song, Y.; Cai, Z.; Yang, C. Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19. J. Med. Virol. 2020, 92, 903–908. [Google Scholar] [CrossRef] [Green Version]
- Tao, A.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RT-PCR testing for Coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Caruso, D.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Polidori, T.; Rucci, C.; Guido, G.; Bracci, B.; de Dominicis, C.; Laghi, A. Chest CT features of COVID-19 in Rome, Italy. Radiology 2020, 296, E79–E85. [Google Scholar] [CrossRef]
- Zhang, J.-J.; Dong, X.; Cao, Y.-Y.; Yuan, Y.-D.; Yang, Y.-B.; Yan, Y.-Q.; Akdis, C.A.; Gao, Y.-D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- WHO. Clinical-Management-of-COVID-19. 2020. Available online: https://who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 14 November 2020).
- Lindsley, A.W.; Schwartz, J.T.; Rothenberg, M.E. Eosinophil responses during COVID-19 infections and coronavirus vaccination. J. Allergy Clin. Immunol. 2020, 146, 1–7. [Google Scholar] [CrossRef]
- Hirosawa, T.; Harada, Y.; Morinaga, K.; Takase, H.; Nin, M.; Shimizu, T. Eosinopenia as a diagnostic marker of bloodstream infection in a general internal medicine setting: A cohort study. BMC Infect. Dis. 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavoignet, C.-E.; Network, A.T.C.; Le Borgne, P.; Chabrier, S.; Bidoire, J.; Slimani, H.; Chevrolet-Lavoignet, J.; Lefebvre, F.; Jebri, R.; Sengler, L.; et al. White blood cell count and eosinopenia as valuable tools for the diagnosis of bacterial infections in the ED. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Gil, H.; Bouldoires, B.; Bailly, B.; Ruault, N.M.; Humbert, S.; Magy-Bertrand, N. L’éosinopénie en 2018. Rev. Méd. Interne 2019, 40, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Bass, D.A. Behavior of eosinophil leukocytes in acute inflammation. II. Eosinophil dynamics during acute inflammation. J. Clin. Investig. 1975, 56, 870–879. [Google Scholar] [CrossRef] [Green Version]
- Gleich, G.J. Mechanisms of eosinophil-associated inflammation. J. Allergy Clin. Immunol. 2000, 105, 651–663. [Google Scholar] [CrossRef]
- Wardlaw, A.J. Eosinophils in the 1990s: New perspectives on their role in health and disease. Postgrad. Med. J. 1994, 70, 536–552. [Google Scholar] [CrossRef] [Green Version]
- Walsh, G.M. Advances in the immunobiology of eosinophils and their role in disease. Crit. Rev. Clin. Lab. Sci. 1999, 36, 453–496. [Google Scholar] [CrossRef]
- Qian, G.-Q.; Yang, N.-B.; Ding, F.; Ma, A.H.Y.; Wang, Z.-Y.; Shen, Y.-F.; Shi, C.-W.; Lian, X.; Chu, J.-G.; Chen, L.; et al. Epidemiologic and clinical characteristics of 91 hospitalized patients with COVID-19 in Zhejiang, China: A retrospective, multi-centre case series. Qjm: Int. J. Med. 2020, 113, 474–481. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Shen, L.; Fan, J.; Gu, F.; Hu, M.; An, Y.; Zhou, Q.; Fan, H.; Bi, J. Clinical features of patients with coronavirus disease 2019 from a designated hospital in Beijing, China. J. Med. Virol. 2020, 92, 2055–2066. [Google Scholar] [CrossRef]
- Du, Y.; Tu, L.; Zhu, P.; Mu, M.; Wang, R.; Yang, P.; Wang, X.; Hu, C.; Ping, R.; Hu, P.; et al. Clinical features of 85 fatal cases of COVID-19 from Wuhan. A retrospective observational study. Am. J. Respir. Crit. Care Med. 2020, 201, 1372–1379. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Xu, A.; Zhang, Y.; Xuan, W.; Yan, T.; Pan, K.; Yu, W.; Zhang, J. Patients of COVID-19 may benefit from sustained Lopinavir-combined regimen and the increase of Eosinophil may predict the outcome of COVID-19 progression. Int. J. Infect. Dis. 2020, 95, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.; He, Z.-B.; Zhang, S.; Zhang, J.-G.; Zhang, X.; Yan, W.-H. Early risk factors for the duration of severe acute respiratory syndrome Coronavirus 2 viral positivity in patients with coronavirus disease 2019. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tanni, F.; Akker, E.; Zaman, M.M.; Figueroa, N.; Tharian, B.; Hupart, K.H. Eosinopenia and COVID-19. J. Am. Osteopat. Assoc. 2020, 120, 504. [Google Scholar] [CrossRef] [PubMed]
- Xie, G.; Ding, F.; Han, L.; Yin, D.; Lu, H.; Zhang, M. The role of peripheral blood eosinophil counts in COVID-19 patients. Allergy 2020. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Cai, X.; Wang, H.; He, G.; Lin, Y.; Lu, B.; Chen, C.; Pan, Y.; Hu, X. Abnormalities of peripheral blood system in patients with COVID-19 in Wenzhou, China. Clin. Chim. Acta 2020, 507, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Ding, X.; Xia, G.; Chen, H.-G.; Chen, F.; Geng, Z.; Xu, L.; Lei, S.; Pan, A.; Wang, L.; et al. Eosinopenia and elevated C-reactive protein facilitate triage of COVID-19 patients in fever clinic: A retrospective case-control study. EClinicalMedicine 2020, 23, 100375. [Google Scholar] [CrossRef]
- Cong-Ying, S.; Jia, X.; Jian, Q.; Yuan-Qiang, L. COVID-19 early warning score: A multi-parameter screening tool to identify highly suspected patients. MedXRiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wynants, L.; van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.; Dahly, D.L.; Damen, J.A.A.G.; Debray, T.P.; et al. Prediction models for diagnosis and prognosis of covid-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Overall (n = 174) | rRT-PCR Positive (n = 94) | rRT-PCR Negative (n = 80) | p Value | |
|---|---|---|---|---|
| Age, years | 58 [43–71] | 58 [46–67] | 65 [39–74] | 0.99 |
| Male, n (%) | 90 (52) | 54 (57) | 36 (45) | 0.13 |
| BMI, kg/m2 | 27.5 [23.5–31.6] | 28.9 [25–31.8] | 25.6 [22.9–31] | 0.02 |
| Hypertension, n (%) | 77 (45) | 46 (49) | 31 (40) | 0.28 |
| Diabetes, n (%) | 48 (28) | 30 (32) | 18 (23) | 0.23 |
| Heart Disease, n (%) | 39 (22) | 19 (20) | 20 (26) | 0.47 |
| Previous Neurologic Disease, n (%) | 28 (16) | 14 (15) | 14 (18) | 0.68 |
| Chronic Kidney Disease, n (%) | 32 (18) | 19 (20) | 13 (17) | 0.69 |
| Asthma/COPD, n (%) | 32 (18) | 13 (14) | 19 (24) | 0.11 |
| Autoimmune Disease, n (%) | 18 (10) | 10 (11) | 8 (10) | 1 |
| Allergies, n (%) | 31 (18) | 16 (17) | 15 (19) | 0.84 |
| Cancer, n (%) | 27 (16) | 10 (11) | 17 (22) | 0.06 |
| Psychiatric Disease, n (%) | 17 (10) | 7 (7) | 10 (13) | 0.3 |
| Liver Cirrhosis, n (%) | 6 (3) | 3 (3) | 3 (4) | 1 |
| Alcohol, n (%) | 13 (8) | 8 (9) | 5 (6) | 0.77 |
| Active Smoking, n (%) | 30 (17) | 13 (14) | 17 (22) | 0.23 |
| Immunosuppressive Therapy, n (%) | 22 (13) | 13 (14) | 9 (12) | 0.82 |
| NSAIDs, n (%) | 21 (12) | 8 (9) | 13 (17) | 0.16 |
| ARB-ACE, n (%) | 39 (22) | 26 (28) | 13 (17) | 0.1 |
| Corticosteroids, n (%) | 27 (15) | 14 (15) | 13 (17) | 0.83 |
| Fever on admission (%) | 96 (60) | 64 (70) | 32 (48) | <0.01 |
| Cough on admission (%) | 107 (68) | 65 (71) | 42 (63) | 0.30 |
| Dyspnea on admission (%) | 90 (57) | 59 (66) | 31 (46) | 0.01 |
| Anosmia on admission (%) | 11 (6) | 10 (11) | 1 (1) | 0.03 |
| Bacterial co-infection on admission | 25 (15) | 11 (12) | 14 (18) | 0.39 |
| Viral co-infection on admission | 6 (4) | 1 (1) | 5 (6) | 0.07 |
| Time from symptoms to Hospital, days | 6 [2–7] | 7 [4–8] | 3 [1–7] | <0.01 |
| Time from admission to test, days | 0 [0–1] | 1 [0–1] | 0 [0–1] | 0.08 |
| ICU admission, n (%) | 18 (10) | 13 (14) | 5 (6) | 0.13 |
| Suggestive chest CT-scan, n (%) | 103 (59) | 79 (92) | 24 (41) | <0.01 |
| Clinical score on admission | 2 [2–3] | 2 [2–3] | 2 [1–2] | <0.01 |
| PT on admission, % | 88 [78–96] | 93 [85–98] | 85 [74–96] | 0.01 |
| Fibrinogen on admission, mg/dL | 475 [361–593] | 505 [400–634] | 438 [351–522] | 0.23 |
| WBC on admission, n/mm3 | 10430 [8230–11340] | 5750 [4470–7470] | 9820 [6550–12660] | <0.01 |
| RBC on admission, n*10⁶/mm3 | 4.68 [4.11–5.11] | 4.85 [4.19–5.19] | 4.66 [3.97–4.94] | 0.19 |
| Haemoglobin on admission, g/dL | 13.6 [11.6–14.6] | 13.9 [11.8–14.7] | 13.2 [11.2–14.2] | 0.14 |
| RDW on admission, % | 13.45 [12.7–14.8] | 13.2 [12.6–14.3] | 13.9 [13–16.2] | <0.01 |
| Platelets on admission, n*103/mm3 | 209 [163–273] | 188 [152–237] | 251 [175–311] | <0.01 |
| Neutrophils on admission, n/mm3 | 4910 [340–7840] | 4240 [3160–5760] | 6690 [4590–10030] | <0.01 |
| Lymphocytes on admission, n/mm3 | 1160 [730–1740] | 920 [690–1380] | 1440 [840–2190] | <0.01 |
| Monocytes on admission, n/mm3 | 550 [330–780] | 430 [30–580] | 680 [480–900] | <0.01 |
| Eosinophils on admission, n/mm3 | 10 [0–30] | 0 [0–10] | 80 [20–180] | <0.01 |
| Basophils on admission, n/mm3 | 10 [10–30] | 10 [0–10] | 30 [20–50] | <0.01 |
| NLR on admission | 4.08 [2.59–7.31] | 4.82 [3.01–7.13] | 3.79 [2.5–8.43] | 0.81 |
| LCR on admission | 0.03 [0.01–0.14] | 0.01 [0.01–0.05] | 0.07 [0.02–0.42] | <0.01 |
| C-Reactive Protein on admission, mg/L | 53 [13–110] | 72 [22–120] | 19 [5–71] | <0.01 |
| Procalcitonine on admission, mcg/L | 0.11 [0.05–0.29] | 0.12 [0.05–0.28] | 0.09 [0.05–0.32] | 0.78 |
| Urea on t admission, mg/dL | 33.2 [21.9–48.3] | 34.4 [22.4–50.6] | 32.6 [21.5–47.4] | 0.76 |
| Creatinine on admission, mg/dL | 0.95 [0.77–1.34] | 1 [0.8–1.33] | 0.9 [0.74–1.36] | 0.19 |
| Bilirubin on admission, mg/dL | 0.48 [0.33–0.61] | 0.47 [0.33–0.6] | 0.51 [0.32–0.65] | 0.3 |
| SGPT on admission, UI/L | 23 [14–40] | 29 [16–43] | 19 [11–31] | <0.01 |
| SGOT on admission, UI/L | 28 [20–50] | 40 [26–55] | 22 [17–41] | <0.01 |
| LDH on admission, UI/L | 272 [190–394] | 282 [214–417] | 241 [175–336] | 0.02 |
| Troponin on admission, ng/L | 12 [6–28] | 12 [6–24] | 13 [7–33] | 0.39 |
| Albumin on admission, g/L | 40 [37–42] | 39 [35–42] | 42 [38–43] | <0.01 |
| CT Scan Suggestive (n = 103) | CT Scan Not Suggestive (n = 42) | p Value | |
|---|---|---|---|
| Age, years | 60 [49–71] | 65 [43–74] | 0.98 |
| Male, n (%) | 61 (59) | 15 (36) | 0.01 |
| BMI, kg/m2 | 29.1 [25.0–32.4] | 24.4 [23.1–28.8] | <0.01 |
| Hypertension, n (%) | 56 (55) | 13 (31) | 0.01 |
| Diabetes, n (%) | 34 (33) | 13 (31) | 0.85 |
| Heart Disease, n (%) | 22 (22) | 14 (33) | 0.15 |
| Previous Neurologic Disease, n (%) | 16 (16) | 8 (19) | 0.63 |
| Chronic Kidney Disease, n (%) | 20 (20) | 10 (24) | 0.65 |
| Asthma/COPD, n (%) | 16 (16) | 12 (29) | 0.10 |
| Autoimmune Disease, n (%) | 10 (10) | 5 (12) | 0.77 |
| Allergies, n (%) | 17 (17) | 9 (21) | 0.49 |
| Cancer, n (%) | 12 (12) | 13 (31) | <0.01 |
| Psychiatric Disease, n (%) | 11 (11) | 5 (12) | 0.99 |
| Liver Cirrhosis, n (%) | 3 (3) | 3 (7) | 0.36 |
| Alcohol, n (%) | 9 (9) | 4 (10) | 0.99 |
| Active Smoking, n (%) | 15 (15) | 11 (26) | 0.15 |
| Immunosuppressive Therapy, n (%) | 14 (14) | 6 (14) | 0.99 |
| NSAIDs, n (%) | 13 (13) | 6 (14) | 0.79 |
| ARB-ACE, n (%) | 29 (28) | 8 (19) | 0.30 |
| Corticosteroids, n (%) | 15 (15) | 10 (24) | 0.23 |
| Fever on admission (%) | 67 (67) | 16 (47) | 0.04 |
| Cough on admission (%) | 71 (72) | 19 (56) | 0.10 |
| Dyspnea on admission (%) | 63 (64) | 20 (59) | 0.68 |
| Anosmia on admission (%) | 10 (10) | 0 (0) | 0.06 |
| Bacterial co-infection on admission | 11 (11) | 12 (29) | 0.01 |
| Viral co-infection on admission | 3 (3) | 1 (2) | 1.00 |
| ICU admission, n (%) | 15 (15) | 1 (3) | 0.04 |
| rRT-PCR positive Test, n (%) | 83 (81) | 7 (17) | <0.01 |
| Clinical score on admission | 2 [2–3] | 2 [1–2] | <0.01 |
| PT on admission, % | 91 [83–98] | 85 [73–95] | 0.03 |
| Fibrinogen on admission, mg/dL | 505 [417–634] | 422 [348–483] | 0.01 |
| WBC on admission, n/mm3 | 5900 [4730–8710] | 9080 [6310–12520] | <0.01 |
| RBC on admission, n*10⁶/mm3 | 4.80 [4.29–5.15] | 4.46 [3.96–4.80] | 0.01 |
| Haemoglobin on admission, g/dL | 13.9 [11.9–14.7] | 12.8 [10.9–14.0] | 0.04 |
| RDW on admission, % | 13.3 [12.7–14.7] | 14.1 [13.2–16.5] | 0.03 |
| Platelets on admission, n*103/mm3 | 190 [151–245] | 243 [173–309] | 0.02 |
| Neutrophils on admission, n/mm3 | 4.510 [3220–6610] | 6160 [4670–10000] | <0.01 |
| Lymphocytes on admission, n/mm3 | 1.040 [730–1430] | 1150 [660–2210] | 0.12 |
| Monocytes on admission, n/mm3 | 430 [300–620] | 650 [500–870] | <0.01 |
| Eosinophils on admission, n/mm3 | 0 [0–20] | 95 [20–170] | <0.01 |
| Basophils on admission, n/mm3 | 10 [0–20] | 30 [20–50] | <0.01 |
| NLR on admission | 4.17 [2.87–7.50] | 4.39 [2.49–9.63] | 0.92 |
| LCR on admission | 0.02 [0.01–0.05] | 0.10 [0.01–0.44] | <0.01 |
| C-Reactive Protein on admission, mg/L | 70 [17–115] | 13 [4–56] | <0.01 |
| Procalcitonine on admission, mcg/L | 0.12 [0.07–0.29] | 0.11 [0.05-–0.38] | 0.51 |
| Urea on t admission, mg/dL | 38 [24–52] | 32 [22–82] | 0.71 |
| Creatinine on admission, mg/dL | 1.00 [0.84–1.38] | 0.96 [0.73–1.59] | 0.97 |
| Bilirubin on admission, mg/dL | 0.49 [0.33–0.61] | 0.44 [0.32–0.71] | 0.78 |
| SGPT on admission, UI/L | 25 [15–41] | 21 [13–32] | 0.15 |
| SGOT on admission, UI/L | 39 [24–52] | 25 [17–45] | 0.01 |
| LDH on admission, UI/L | 309 [246–415] | 219 [170–289] | <0.01 |
| Troponin on admission, ng/L | 13 [9–29] | 15 [6–35] | 0.74 |
| Albumin on admission, g/L | 39 [36–42] | 40 [39–44] | 0.04 |
| OR [95% CIs] | p Value | |
|---|---|---|
| rRT-PCR positive for SARS-CoV-2 | ||
| Eosinopenia | 13.42 [4.11–43.77] | <0.01 |
| LDH, IU/L | 1.01 [1.00–1.01] | 0.02 |
| CT Scan suggestive for COVID-19 | ||
| BMI, Kg/m2 | 1.09 [1.01–1.19] | 0.04 |
| Arterial Hypertension | 3.30 [1.29–8.46] | 0.01 |
| Eosinopenia | 8.12 [2.61–25.23] | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndieugnou Djangang, N.; Peluso, L.; Talamonti, M.; Izzi, A.; Gevenois, P.A.; Garufi, A.; Goffard, J.-C.; Henrard, S.; Severgnini, P.; Vincent, J.-L.; et al. Eosinopenia in COVID-19 Patients: A Retrospective Analysis. Microorganisms 2020, 8, 1929. https://doi.org/10.3390/microorganisms8121929
Ndieugnou Djangang N, Peluso L, Talamonti M, Izzi A, Gevenois PA, Garufi A, Goffard J-C, Henrard S, Severgnini P, Vincent J-L, et al. Eosinopenia in COVID-19 Patients: A Retrospective Analysis. Microorganisms. 2020; 8(12):1929. https://doi.org/10.3390/microorganisms8121929
Chicago/Turabian StyleNdieugnou Djangang, Narcisse, Lorenzo Peluso, Marta Talamonti, Antonio Izzi, Pierre Alain Gevenois, Alessandra Garufi, Jean-Christophe Goffard, Sophie Henrard, Paolo Severgnini, Jean-Louis Vincent, and et al. 2020. "Eosinopenia in COVID-19 Patients: A Retrospective Analysis" Microorganisms 8, no. 12: 1929. https://doi.org/10.3390/microorganisms8121929