
Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia: A Literature Review

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Relevant Sections
3.1. Epidemiology
3.2. Etiology and Risk Factors
3.3. Pathophysiology
3.4. Diagnostic Tools
3.5. Preventive Methods
3.6. Treatment
4. Future Directions
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
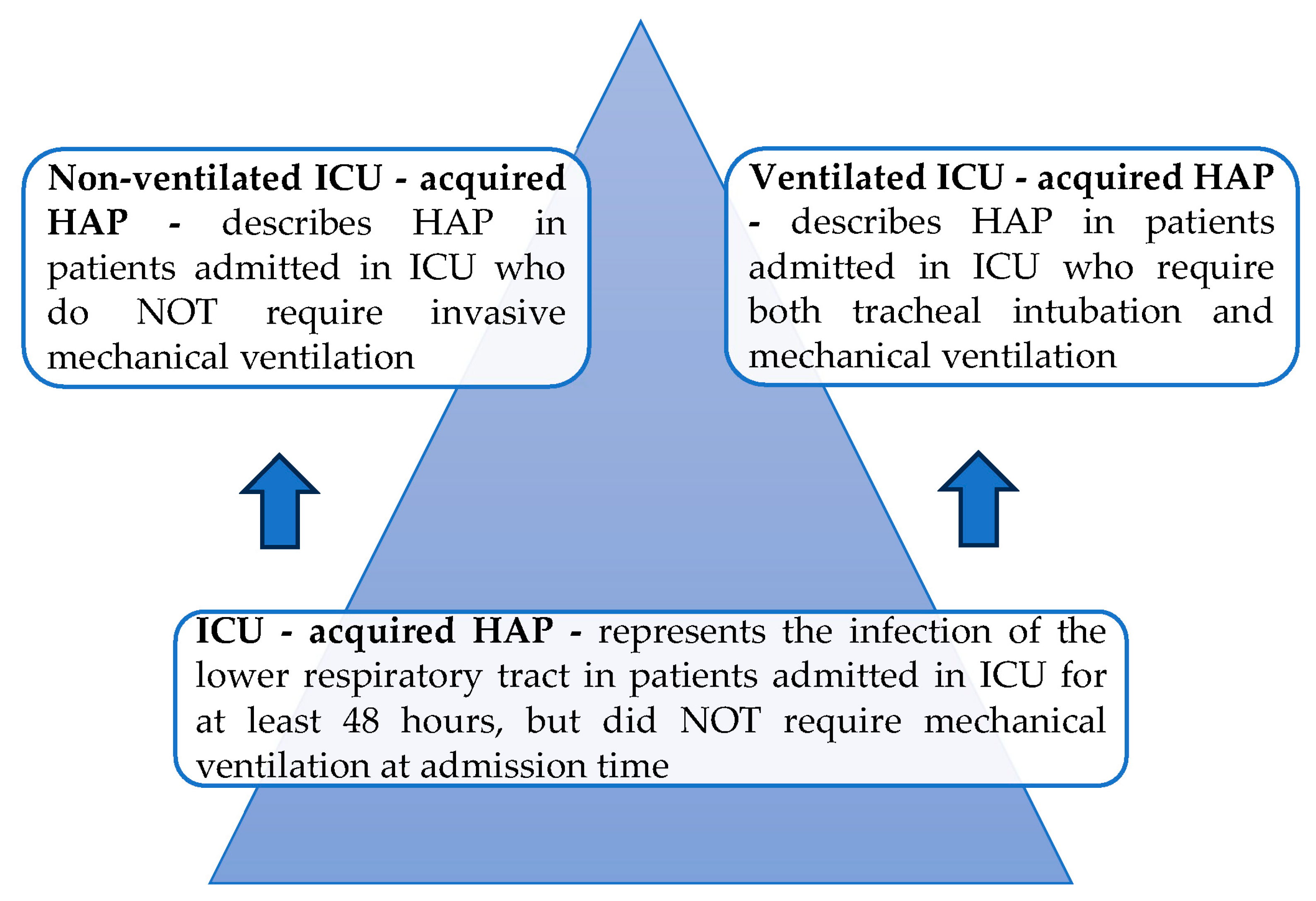
| HAP | hospital-acquired pneumonia; |
| VAP | ventilator-associated pneumonia; |
| FiO2 | fraction of inspired oxygen; |
| PEEP | positive end-expiratory pressure; |
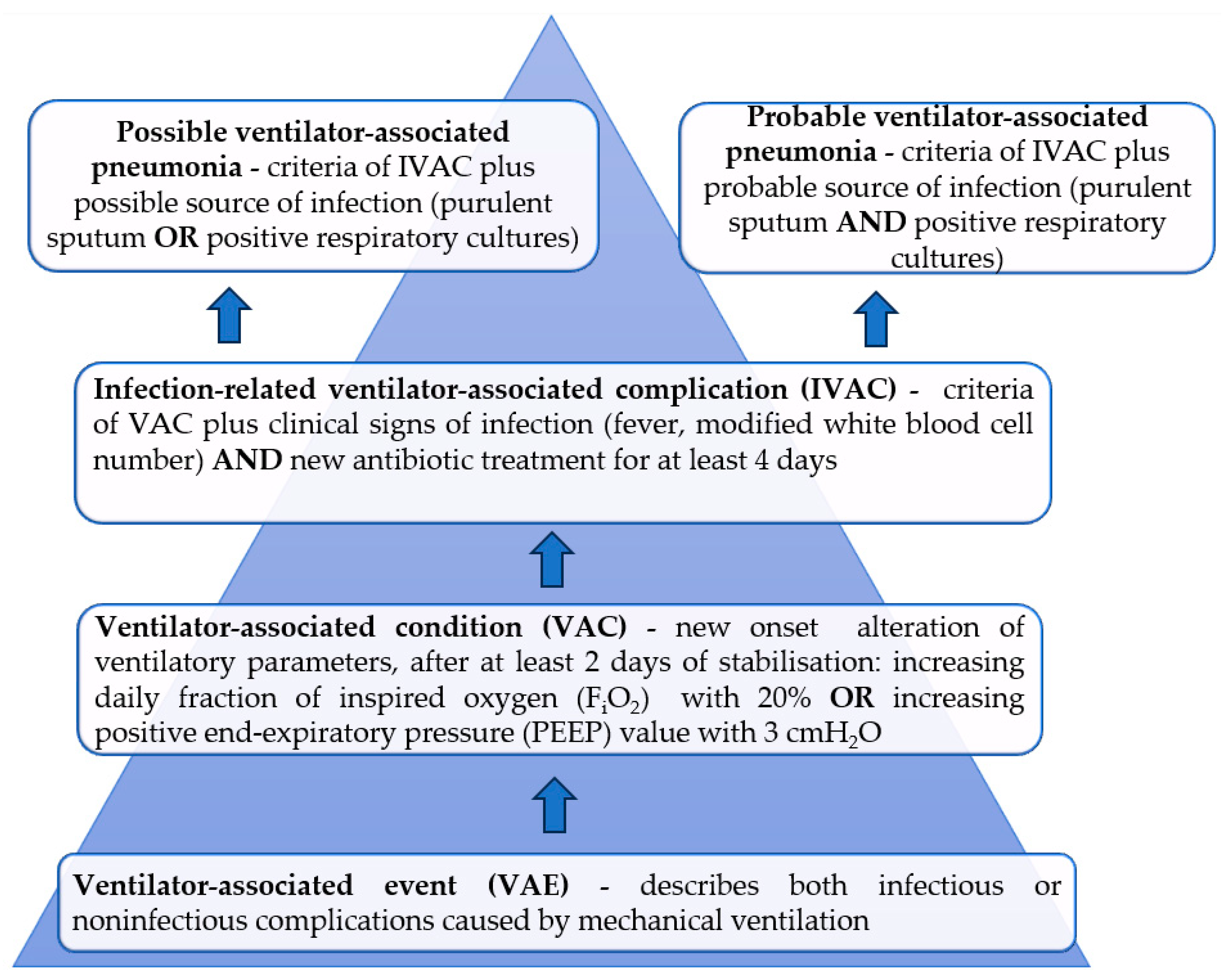
| VAE | ventilator-associated events; |
| VAC | ventilator-associated conditions; |
| IVAC | infection-related ventilator-associated complications; |
| UTIs | urinary tract infections; |
| ICU | intensive care unit; |
| MRSA | methicillin-resistant Staphylococcus aureus; |
| RSV | respiratory syncytial virus; |
| HSV | Herpes Simplex virus; |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2; |
| COVID-19 | coronavirus disease-19; |
| HAIs | healthcare-associated infections; |
| BSIs | bloodstream infections; |
| MDR | multidrug resistant; |
| MDR VAP | multidrug resistant ventilator-associated pneumonia; |
| ARDS | acute respiratory distress syndrome; |
| CPIS | clinical pulmonary infection score; |
| ATS | American Thoracic Society; |
| IDSA | Infectious Diseases Society of America; |
| BAL | bronchoalveolar lavage; |
| PSB | protected specimen brush; |
| CFUs | colony forming units; |
| CRP | C-reactive protein; |
| sTREM-1 | soluble triggering receptor expressed on myelloid cells type 1; |
| MR pro-ANP | mid-regional pro-atrial natriuretic peptide; |
| ANP | atrial natriuretic peptide; |
| MR pro-ADM | mid-region fragment of pro-adrenomedullin; |
| PCT | procalcitonin; |
| Ig G | immunoglobulin G; |
| SDD | selective decontamination of digestive tract; |
| MPCR | multiplex polymerase chain reaction; |
| PRP | penicillin-resistant Streptococcus pneumoniae; |
| non-ESBL | non-extended spectrum β-lactamase; |
| ESBL | extended spectrum β-lactamase; |
| BLI | β-lactamase inhibitor; |
| PBP | penicillin-binding protein; |
| XDR | extremely drug resistant; |
| CRE | carbapenem-resistant Enterobacterales. |
References
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. Summary of the international clinical guidelines for the management of hospital-acquired and ventilator-acquired pneumonia. ERJ Open Res. 2018, 4, 00028-2018. [Google Scholar] [CrossRef]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the Management of Hospital-Acquired Pneumonia (HAP)/Ventilator-Associated Pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef]
- Ramirez-Estrada, S.; Peña-Lopez, Y.; Eshwara, V.K.; Rello, J. Ventilator-associated events versus ventilator-associated respiratory infections—Moving into a new paradigm or merging both concepts, instead? Ann. Transl. Med. 2018, 6, 425. [Google Scholar] [CrossRef]
- Dexter, A.M.; Scott, J.B. Airway Management and Ventilator-Associated Events. Respir. Care 2019, 64, 986–993. [Google Scholar] [CrossRef]
- Ferrer, M.; Torres, A. Epidemiology of ICU-acquired pneumonia. Curr. Opin. Crit. Care 2018, 24, 325–331. [Google Scholar] [CrossRef]
- Leone, M.; Bouadma, L.; Bouhemad, B.; Brissaud, O.; Dauger, S.; Gibot, S.; Hraiech, S.; Jung, B.; Kipnis, E.; Launey, Y.; et al. Hospital-acquired pneumonia in ICU. Anaesth. Crit. Care Pain Med. 2018, 37, 83–98. [Google Scholar] [CrossRef]
- Klompas, M. Epidemiology, pathogenesis, microbiology, and diagnosis of hospital-acquired and ventilator-associated pneumonia in adults. In UpToDate; File, T.M., Jr., Ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlandsa, 2023. [Google Scholar]
- Papazian, L.; Klompas, M.; Luyt, C.-E. Ventilator-associated pneumonia in adults: A narrative review. Intensiv. Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef]
- Koulenti, D.; Tsigou, E.; Rello, J. Nosocomial pneumonia in 27 ICUs in Europe: Perspectives from the EU-VAP/CAP study. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 36, 1999–2006. [Google Scholar] [CrossRef]
- Zilberbeg, M.D.; Khan, I.; Shorr, A.F. Respiratory Viruses in Nosocomial Pneumonia: An Evolving Paradigm. Viruses 2023, 15, 1676. [Google Scholar] [CrossRef]
- Li, Y.; Liu, C.; Xiao, W.; Song, T.; Wang, S. Incidence, Risk Factors, and Outcomes of Ventilator-Associated Pneumonia in Traumatic Brain Injury: A Meta-analysis. Neurocrit. Care 2020, 32, 272–285. [Google Scholar] [CrossRef]
- Mangram, A.J.; Sohn, J.; Zhou, N.; Hollingworth, A.K.; Ali-Osman, F.R.; Sucher, J.F.; Moyer, M.; Dzandu, J.K. Trauma-associated pneumonia: Time to redefine ventilator-associated pneumonia in trauma patients. Am. J. Surg. 2015, 210, 1056–1061, discussion 1061–1062. [Google Scholar] [CrossRef]
- Gudiol, C.; Sabé, N.; Carratalà, J. Is hospital-acquired pneumonia different in transplant recipients? Clin. Microbiol. Infect. 2019, 25, 1186–1194. [Google Scholar] [CrossRef]
- Stoclin, A.; Rotolo, F.; Hicheri, Y.; Mons, M.; Chachaty, E.; Gachot, B.; Pignon, J.P.; Wartelle., M.; Blot, F. Ventilator-associated pneumonia and bloodstream infections in intensive care unit cancer patients: A retrospective 12-year study on 3388 prospectively monitored patients. Support. Care Cancer 2020, 28, 193–200. [Google Scholar] [CrossRef]
- Liu, Y.; Di, Y.; Fu, S. Risk factors for ventilator-associated pneumonia among patients undergoing major oncological surgery for head and neck cancer. Front. Med. 2017, 11, 239–246. [Google Scholar] [CrossRef]
- Charles, M.P.; Kali, A.; Easow, J.M.; Joseph, N.M.; Ravishankar, M.; Srinivasan, S.; Kumar, S.; Umadevi, S. Ventilator-associated pneumonia. Australas. Med. J. 2014, 7, 334–344. [Google Scholar] [CrossRef]
- Fine, L.S. Non-ventilator health care-associated pneumonia (NV-HAP): Pathogenesis and microbiology of NV-HAP. Am. J. Infect. Control 2020, 48, A7–A9. [Google Scholar] [CrossRef]
- Grasselli, G.; Scaravilli, V.; Mangioni, D.; Scudeller, L.; Alagna, L.; Bartoletti, M.; Bellani, G.; Biagioni, E.; Bonfanti, P.; Bottino, N.; et al. Hospital-Acquired Infections in Critically Ill Patients With COVID-19. Chest 2021, 160, 454–465. [Google Scholar] [CrossRef]
- Aligui, A.A.A.F.; Abad, C.L.R. Multidrug-resistant VAP before and during the COVID-19 pandemic among hospitalized patients in a tertiary private hospital. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e192. [Google Scholar] [CrossRef]
- Wicky, P.-H.; Niedermann, M.S.; Timsit, J.-F. Ventilator-associated pneumonia in the era of COVID-19 pandemic: How common and what is the impact? Crit. Care 2021, 25, 153. [Google Scholar] [CrossRef]
- Klompas, M. Risk factors and prevention of hospital-acquired and ventilator-associated pneumonia in adults. In Up-ToDate; File, T.M., Jr., Ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2023; Available online: https://www.uptodate.com/contents/6995#! (accessed on 24 January 2023).
- Hess, D.R.; Kallstrom, T.J.; Mottram, C.D.; Myers, T.R.; Sorenson, H.M.; Vines, D.L.; American Association for Respiratory Care. Care of the ventilator circuit and its relation to ventilator-associated pneumonia. Respir. Care 2003, 48, 869–879. [Google Scholar]
- Rouzé, A.; Martin-Loeches, I.; Nseir, S. Airway Devices in Ventilator-Associated Pneumonia Pathogenesis and Prevention. Clin. Chest Med. 2018, 39, 775–783. [Google Scholar] [CrossRef]
- Kalanuria, A.A.; Zai, W.; Mirski, M. Ventilator-associated pneumonia in the ICU. Crit. Care 2014, 18, 208. [Google Scholar] [CrossRef]
- Fernando, S.M.; Tran, A.; Cheng, W.; Klompas, M.; Kyeremanteng, K.; Mehta, S.; English, S.W.; Muscedere, J.; Cook, D.J.; Torres, A.; et al. Diagnosis of ventilator-associated pneumonia in critically ill adult patients—A systematic review and meta-analysis. Intensiv. Care Med. 2020, 46, 1170–1179. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratala, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111, Erratum in Clin. Infect. Dis. 2017, 64, 1298. Erratum in Clin. Infect. Dis. 2017, 65, 1435. Erratum in Clin. Infect. Dis. 2017, 65, 2161. [Google Scholar] [CrossRef]
- Kollef, M.H. Clinical presentation and diagnostic evaluation of ventilator-associated pneumonia. In UpToDate; Manaker, S., Ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2023; Available online: https://www.uptodate.com/contents/clinical-presentation-and-diagnostic-evaluation-of-ventilator-associated-pneumonia (accessed on 13 November 2023).
- Bickenbach, J.; Marx, G. Diagnosis of pneumonia in mechanically ventilated patients: What is the meaning of the CPIS? Minerva Anestesiol. 2013, 79, 1406–1414. [Google Scholar]
- Palazzo, S.J.; Simpson, T.; Schnapp, L. Biomarkers for ventilator-associated pneumonia: Review of the literature. Heart Lung 2011, 40, 293–298. [Google Scholar] [CrossRef]
- Póvoa, P.; Martin-Loeches, I.; Ramirez, P.; Bos, L.D.; Esperatti, M.; Silvestre, J.; Gili, G.; Goma, G.; Berlanga, E.; Espasa, M.; et al. Biomarker kinetics in the prediction of VAP diagnosis: Results from the BioVAP study. Ann. Intensiv. Care 2016, 6, 32. [Google Scholar] [CrossRef]
- Rhee, C.; Mansour, M.K. Procalcitonin use in lower respiratory tract infections. In UpToDate; Ramirez, J.A., File, T.M., Jr., Eds.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2022; Available online: https://www.uptodate.com/contents/procalcitonin-use-in-lower-respiratory-tract-infections (accessed on 3 November 2022).
- Grover, V.; Pantelidis, P.; Soni, N.; Takata, M.; Shah, P.L.; Wells, A.U.; Henderson, D.C.; Kelleher, P.; Singh, S. A Biomarker Panel (Bioscore) Incorporating Monocytic Surface and Soluble TREM-1 Has High Discriminative Value for Ventilator-Associated Pneumonia: A Prospective Observational Study. PLoS ONE 2014, 9, e109686. [Google Scholar] [CrossRef]
- Seligman, R.; Papassotiriou, J.; Morgenthaler, N.G.; Meisner, M.; Teixeira, P.J.Z. Prognostic value of midregional pro-atrial natriuretic peptide in ventilator-associated pneumonia. Intensiv. Care Med. 2008, 34, 2084–2091. [Google Scholar] [CrossRef]
- Boeck, L.; Eggimann, P.; Smyrnios, N.; Pargger, H.; Thakkar, N.; Siegemund, M.; Marsch, S.; Rakic, J.; Tamm, M.; Stolz, D. Midregional pro-atrial natriuretic peptide and procalcitonin improve survival prediction in VAP. Eur. Respir. J. 2010, 37, 595–603. [Google Scholar] [CrossRef]
- Spoto, S.; Legramante, J.M.; Minieri, M.; Fogolari, M.; Terrinoni, A.; Valeriani, E.; Sebastiano, C.; Bernardini, S.; Ciccozzi, M.; Angeletti, S. How biomarkers can improve pneumonia diagnosis and prognosis: Procalcitonin and mid-regional-pro-adrenomedullin. Biomark. Med. 2020, 14, 549–562. [Google Scholar] [CrossRef]
- Choi, J.J.; McCarthy, M.W. The prognostic value of mid-regional pro-adrenomedullin in the evaluation of acute dyspnea. Expert Rev. Mol. Diagn. 2017, 18, 147–153. [Google Scholar] [CrossRef]
- Önal, U.; Valenzuela-Sánchez, F.; Vandana, K.E.; Rello, J. Mid-Regional Pro-Adrenomedullin (MR-proADM) as a Biomarker for Sepsis and Septic Shock: Narrative Review. Healthcare 2018, 6, 110. [Google Scholar] [CrossRef]
- Liu, D.; Xie, L.; Zhao, H.; Liu, X.; Cao, J. Prognostic value of mid-regional pro-adrenomedullin (MR-proADM) in patients with community-acquired pneumonia: A systematic review and meta-analysis. BMC Infect. Dis. 2016, 16, 232. [Google Scholar] [CrossRef]
- de Montmollin, E.; Peoc’h, K.; Marzouk, M.; Ruckly, S.; Wicky, P.-H.; Patrier, J.; Jaquet, P.; Sonneville, R.; Bouadma, L.; Timsit, J.-F. Mid-Regional Pro-Adrenomedullin as a Prognostic Factor for Severe COVID-19 ARDS. Antibiotics 2022, 11, 1166. [Google Scholar] [CrossRef]
- Modi, A.R.; Kovacs, C.S. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Clevel. Clin. J. Med. 2020, 87, 633–639. [Google Scholar] [CrossRef]
- Burja, S.; Belec, T.; Bizjak, N.; Mori, J.; Markota, A.; Sinkovič, A. Efficacy of a bundle approach in preventing the incidence of ventilator associated pneumonia (VAP). Bosn. J. Basic Med. Sci. 2017, 18, 105–109. [Google Scholar] [CrossRef]
- Klompas, M.; Branson, R.; Cawcutt, K.; Crist, M.; Eichenwald, E.C.; Greene, L.R.; Lee, G.; Maragakis, L.L.; Powell, K.; Priebe, G.P.; et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 Update. Infect. Control Hosp. Epidemiol. 2022, 43, 687–713. [Google Scholar] [CrossRef]
- Martinez-Reviejo, R.; Tejada, S.; Jansson, M.; Ruiz-Spinelli, A.; Ramirez-Estrada, S.; Ege, D.; Vieceli, T.; Maertens, B.; Blot, S.; Rello, J. Prevention of ventilator-associated pneumonia through care bundles: A systematic review and meta-analysis. J. Intensiv. Med. 2023, 3, 352–364. [Google Scholar] [CrossRef]
- Alnimr, A. Antimicrobial Resistance in Ventilator-Associated Pneumonia: Predictive Microbiology and Evidence-Based Therapy. Infect. Dis. Ther. 2023, 12, 1527–1552. [Google Scholar] [CrossRef]
- Zaragoza, R.; Vidal-Cortés, P.; Aguilar, G.; Borges, M.; Diaz, E.; Ferrer, R.; Maseda, E.; Nieto, M.; Nuvials, F.X.; Ramirez, P.; et al. Update of the treatment of nosocomial pneumonia in the ICU. Crit. Care 2020, 24, 383. [Google Scholar] [CrossRef]
- Millot, G.; Voisin, B.; Loiez, C.; Wallet, F.; Nseir, S. The next generation of rapid point-of-care testing identification tools for ventilator-associated pneumonia. Ann. Transl. Med. 2017, 5, 451. [Google Scholar] [CrossRef]
- Bassetti, M.; Mularoni, A.; Giacobbe, D.R.; Castaldo, N.; Vena, A. New Antibiotics for Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia. Semin. Respir. Crit. Care Med. 2022, 43, 280–294. [Google Scholar] [CrossRef]
- Yusuf, E.; Bax, H.I.; Verkaik, N.J.; van Westreenen, M. An Update on Eight “New” Antibiotics against Multidrug-Resistant Gram-Negative Bacteria. J. Clin. Med. 2021, 10, 1068. [Google Scholar] [CrossRef]
- Shortridge, D.; Carvalhaes, C.; Deshpande, L.; Castanheira, M. Activity of meropenem/vaborbactam and comparators against Gram-negative isolates from Eastern and Western European patients hospitalized with pneumonia including ventilator-associated pneumonia (2014–19). J. Antimicrob. Chemother. 2021, 76, 2600–2605. [Google Scholar] [CrossRef]
- Shirley, M. Ceftazidime-Avibactam: A Review in the Treatment of Serious Gram-Negative Bacterial Infections. Drugs 2018, 78, 675–692. [Google Scholar] [CrossRef]
- Girón, R.M.; Ibáñez, A.; Gómez-Punter, R.M.; Alarcón, T. New evidence in severe pneumonia: Imipenem/ cilastatin/relebactam. Rev. Esp. Quimioter. 2022, 35 (Suppl. S1), 46–49. [Google Scholar] [CrossRef]
- Rando, E.; Cutuli, S.L.; Sangiorgi, F.; Tanzarella, E.S.; Giovannenze, F.; De Angelis, G.; Murri, R.; Antonelli, M.; Fantoni, M.; De Pascale, G. Cefiderocol-containing regimens for the treatment of carbapenem-resistant A. baumannii ventilator-associated pneumonia: A propensity-weighted cohort study. JAC-Antimicrob. Resist. 2023, 5, dlad085. [Google Scholar] [CrossRef]
- Syed, Y.Y. Cefiderocol: A Review in Serious Gram-Negative Bacterial Infections. Drugs 2021, 81, 1559–1571. [Google Scholar] [CrossRef]
- Viale, P.; Sandrock, C.E.; Ramirez, P.; Rossolini, G.M.; Lodise, T.P. Treatment of critically ill patients with cefiderocol for infections caused by multidrug-resistant pathogens: Review of the evidence. Ann. Intensiv. Care 2023, 13, 52. [Google Scholar] [CrossRef]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): A randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Risk Factors for Developing HAP/VAP |
|---|
| Invasive mechanical ventilation |
| Extreme age |
| Altered conscious level |
| Chronic lung disease, chronic kidney disease |
| Severe trauma |
| Malnutrition |
| Previous exposure to wide-spectrum antibiotics |
| Aspiration |
| Prolonged surgical procedures (thoracic/upper abdominal) |
| Use of glucocorticoids/opioids/neuromuscular blocking agents |
| Stress ulcer prophylaxis |
| Acute respiratory distress syndrome (ARDS) |
| Anemia |
| Risk Factors for MDR Pathogens |
|---|
| ARDS before VAP |
| Intravenous wide-spectrum antibiotic use in the last 3 months |
| Septic shock at the moment of suspecting VAP |
| At least 5 days length of hospitalization before suspecting VAP (late-onset subtype) |
| Renal replacement therapy before VAP |
| Parameter/Value | 0 Points | 1 Point | 2 Points |
|---|---|---|---|
| Tracheal secretions * | Few | Moderate | Large |
| Chest radiography infiltrates | No new infiltrates | Diffuse new infiltrates | Localized new infiltrates |
| Temperature (°C) | 36.5–38.4 | 38.5–38.9 | >38.9 or <36 |
| Hypoxemic index (PaO2/FiO2 mmHg) | >240 or ARDS | <240 and NO ARDS | |
| White blood cell count (×103/µL) | 4–11 | <4 or >11 | |
| Microbiological culture | Negative | Positive |
| Invasive techniques | Bronchoalveolar lavage (BAL) |
| Mini-bronchoalveolar lavage (mini-BAL) | |
| Protected specimen brush (PSB) | |
| Non-invasive technique | Endotracheal aspirate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miron, M.; Blaj, M.; Ristescu, A.I.; Iosep, G.; Avădanei, A.-N.; Iosep, D.-G.; Crișan-Dabija, R.; Ciocan, A.; Perțea, M.; Manciuc, C.D.; et al. Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia: A Literature Review. Microorganisms 2024, 12, 213. https://doi.org/10.3390/microorganisms12010213
Miron M, Blaj M, Ristescu AI, Iosep G, Avădanei A-N, Iosep D-G, Crișan-Dabija R, Ciocan A, Perțea M, Manciuc CD, et al. Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia: A Literature Review. Microorganisms. 2024; 12(1):213. https://doi.org/10.3390/microorganisms12010213
Chicago/Turabian StyleMiron, Mihnea, Mihaela Blaj, Anca Irina Ristescu, Gabriel Iosep, Andrei-Nicolae Avădanei, Diana-Gabriela Iosep, Radu Crișan-Dabija, Alexandra Ciocan, Mihaela Perțea, Carmen Doina Manciuc, and et al. 2024. "Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia: A Literature Review" Microorganisms 12, no. 1: 213. https://doi.org/10.3390/microorganisms12010213