
In Vitro Susceptibility to Ceftazidime-Avibactam and Comparator Antimicrobial Agents of Carbapenem-Resistant Enterobacterales Isolates
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bacterial Isolates
2.2. Antimicrobial Susceptibility Testing, Interpretation and Screening for Carbapenemases
3. Results
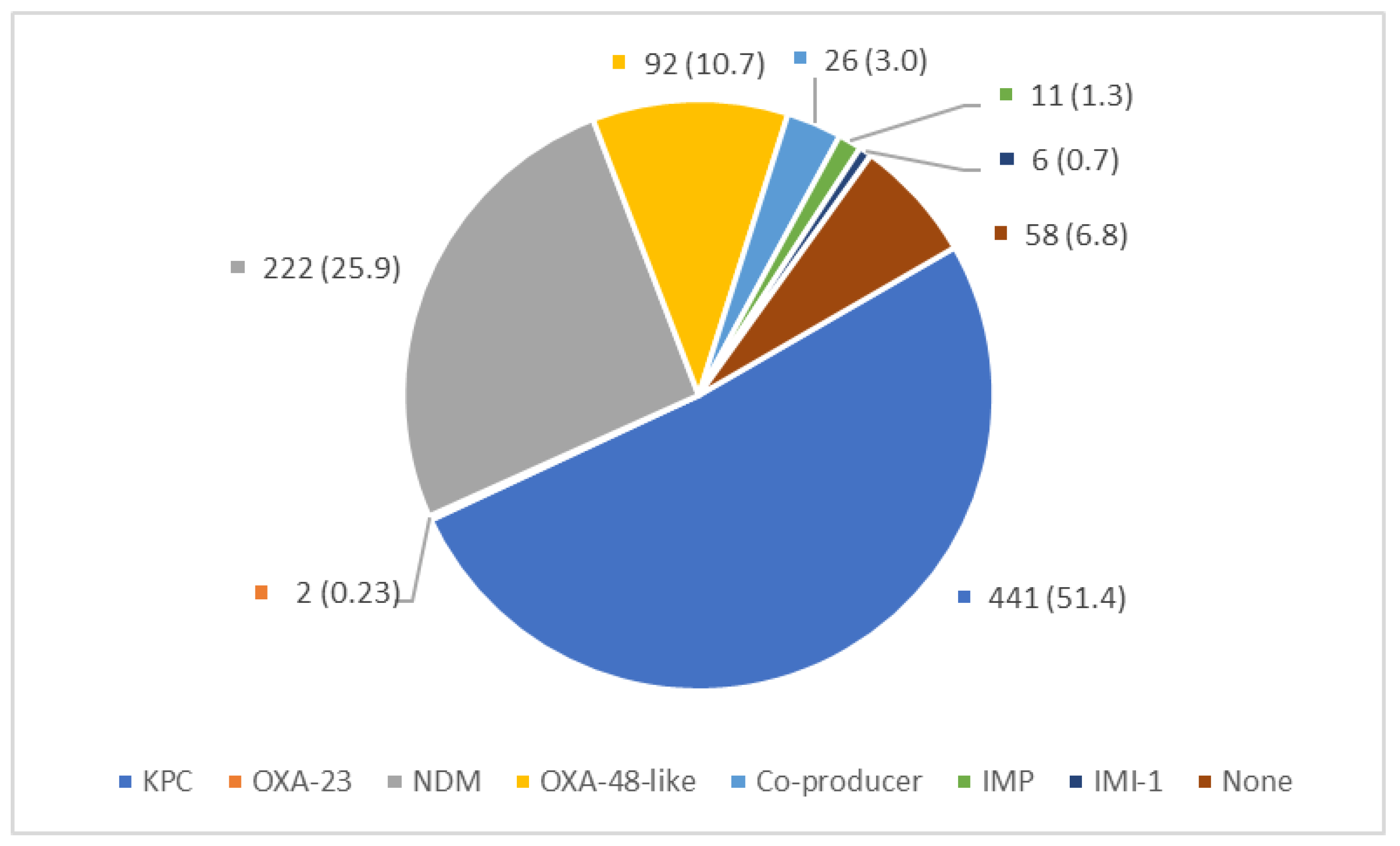
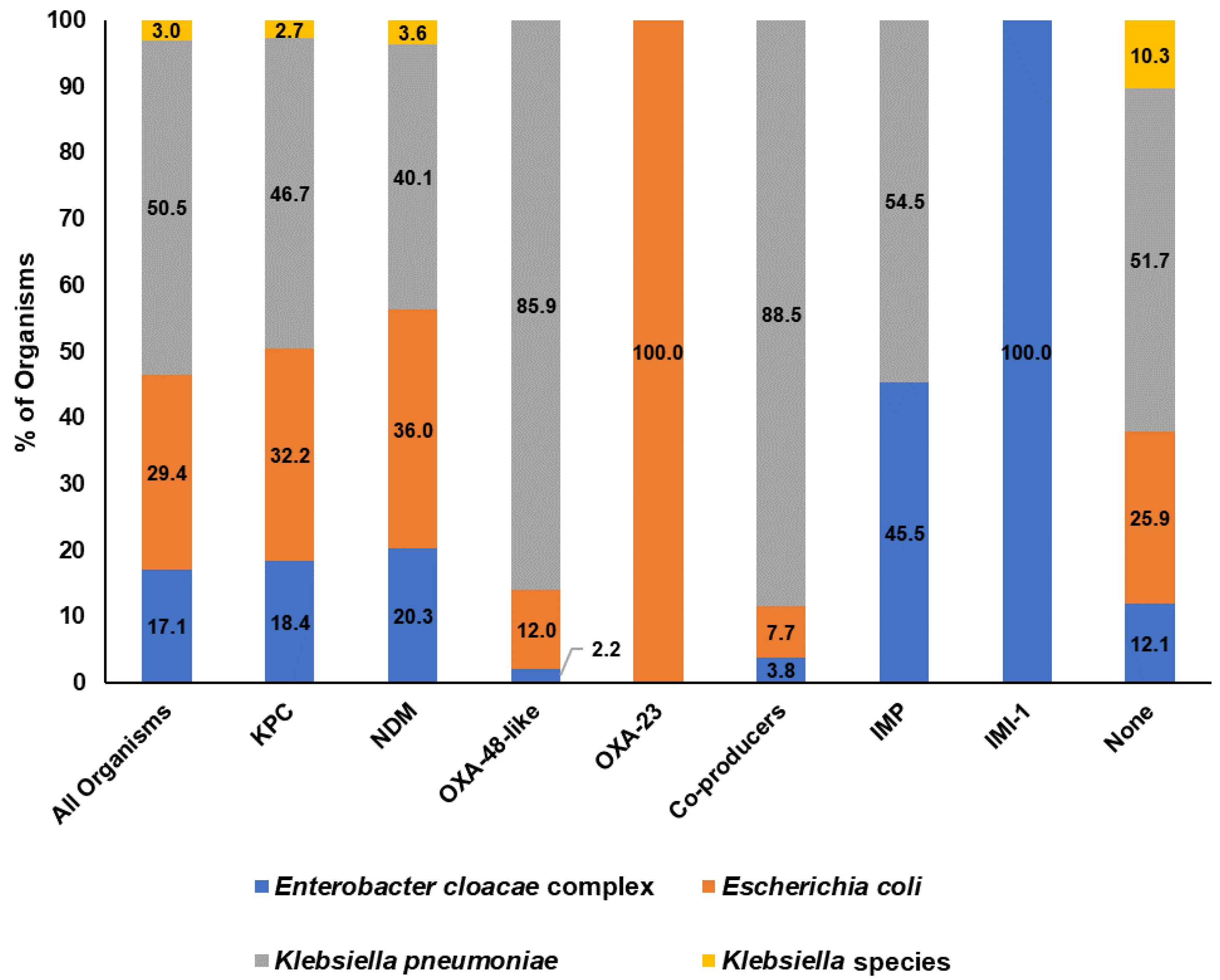
3.1. Bacteria Isolates and Carbapenemase Type
3.2. Antimicrobial Susceptibility Testing and Interpretation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bowers, D.R.; Huang, V. Emerging Issues and Treatment Strategies in Carbapenem-Resistant Enterobacteriaceae (CRE). Curr. Infect. Dis. Rep. 2016, 18, 48. [Google Scholar] [CrossRef]
- Cassini, A.; Hogberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Burden of, Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Thaden, J.T.; Pogue, J.M.; Kaye, K.S. Role of newer and re-emerging older agents in the treatment of infections caused by carbapenem-resistant Enterobacteriaceae. Virulence 2017, 8, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Perez, F.; El Chakhtoura, N.G.; Papp-Wallace, K.M.; Wilson, B.M.; Bonomo, R.A. Treatment options for infections caused by carbapenem-resistant Enterobacteriaceae: Can we apply “precision medicine” to antimicrobial chemotherapy? Expert Opin. Pharmacother. 2016, 17, 761–781. [Google Scholar] [CrossRef] [PubMed]
- Martirosov, D.M.; Lodise, T.P. Emerging trends in epidemiology and management of infections caused by carbapenem-resistant Enterobacteriaceae. Diagn. Microbiol. Infect. Dis. 2016, 85, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; Van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2021, 72, e169–e183. [Google Scholar] [PubMed]
- De Oliveira, D.M.P.; Forde, B.M.; Kidd, T.J.; Harris, P.N.A.; Schembri, M.A.; Beatson, S.A.; Paterson, D.L.; Walker, M.J. Antimicrobial Resistance in ESKAPE Pathogens. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef]
- Cai, Y.; Venkatachalam, I.; Tee, N.W.; Tan, T.Y.; Kurup, A.; Wong, S.Y.; Low, C.Y.; Wang, Y.; Lee, W.; Liew, Y.X.; et al. Prevalence of Healthcare-Associated Infections and Antimicrobial Use Among Adult Inpatients in Singapore Acute-Care Hospitals: Results From the First National Point Prevalence Survey. Clin. Infect. Dis. 2017, 64, S61–S67. [Google Scholar] [CrossRef]
- Ambler, R.P. The structure of beta-lactamases. Philos. Trans. R Soc. Lond. B Biol. Sci. 1980, 289, 321–331. [Google Scholar]
- Patel, G.; Bonomo, R.A. Status report on carbapenemases: Challenges and prospects. Expert Rev. Anti. Infect. Ther. 2011, 9, 555–570. [Google Scholar] [CrossRef]
- Bonomo, R.A.; Burd, E.M.; Conly, J.; Limbago, B.M.; Poirel, L.; Segre, J.A.; Westblade, L.F. Carbapenemase-Producing Organisms: A Global Scourge. Clin. Infect. Dis. 2018, 66, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Hansen, G.T. Continuous Evolution: Perspective on the Epidemiology of Carbapenemase Resistance Among Enterobacterales and Other Gram-Negative Bacteria. Infect. Dis. Ther. 2021, 10, 75–92. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Park, T.E.; Moy, S. Ceftazidime-Avibactam: A Novel Cephalosporin β-Lactamase Inhibitor Combination for the Treatment of Resistant Gram-negative Organisms. Clin. Ther. 2016, 38, 431–444. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, K.; Van Duin, D. Treatment for carbapenem-resistant Enterobacterales infections: Recent advances and future directions. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2053–2068. [Google Scholar] [CrossRef]
- Zasowski, E.J.; Rybak, J.M.; Rybak, M.J. The β-Lactams Strike Back: Ceftazidime-Avibactam. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2015, 35, 755–770. [Google Scholar] [CrossRef]
- Department of Statistics Singapore Singapore Population. Available online: https://www.singstat.gov.sg/modules/infographics/population (accessed on 1 May 2023).
- Cai, Y.; Chua, N.G.; Lim, T.P.; Teo, J.Q.; Lee, W.; Kurup, A.; Koh, T.H.; Tan, T.T.; Kwa, A.L. From Bench-Top to Bedside: A Prospective In Vitro Antibiotic Combination Testing (iACT) Service to Guide the Selection of Rationally Optimized Antimicrobial Combinations against Extensively Drug Resistant (XDR) Gram Negative Bacteria (GNB). PLoS ONE 2016, 11, e0158740. [Google Scholar] [CrossRef]
- Cai, B.; Cai, Y.; Liew, Y.X.; Chua, N.G.; Teo, J.Q.; Lim, T.P.; Kurup, A.; Ee, P.L.; Tan, T.T.; Lee, W.; et al. Clinical Efficacy of Polymyxin Monotherapy versus Nonvalidated Polymyxin Combination Therapy versus Validated Polymyxin Combination Therapy in Extensively Drug-Resistant Gram-Negative Bacillus Infections. Antimicrob. Agents Chemother. 2016, 60, 4013–4022. [Google Scholar] [CrossRef]
- Teo, J.Q.; Cai, Y.; Lim, T.P.; Tan, T.T.; Kwa, A.L. Carbapenem Resistance in Gram-Negative Bacteria: The Not-So-Little Problem in the Little Red Dot. Microorganisms 2016, 4, 13. [Google Scholar] [CrossRef]
- EUCAST. The European Committee on Antimicrobial Susceptibility Testing Breakpoint tables for interpretation of MICs and zone diameters. Version 13.0, 2023. Available online: http://www.eucast.org (accessed on 1 June 2023).
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 33rd ed.; CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2023. [Google Scholar]
- Teo, J.Q.-M.; Fauzi, N.; Ho, J.J.-Y.; Tan, S.H.; Lee, S.J.-Y.; Lim, T.P.; Cai, Y.; Chang, H.Y.; Mohamed Yusoff, N.; Sim, J.H.-C.; et al. In vitro Bactericidal Activities of Combination Antibiotic Therapies Against Carbapenem-Resistant Klebsiella pneumoniae With Different Carbapenemases and Sequence Types. Front. Microbiol. 2021, 12, 779988. [Google Scholar] [CrossRef]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef]
- Andrews, S. FastQC: A Quality Control Tool for High Throughput Sequence Data; Babraham Bioinformatics, Babraham Institute: Cambridge, UK, 2010. [Google Scholar]
- Bankevich, A.; Nurk, S.; Antipov, D.; Gurevich, A.A.; Dvorkin, M.; Kulikov, A.S.; Lesin, V.M.; Nikolenko, S.I.; Pham, S.; Prjibelski, A.D.; et al. SPAdes: A new genome assembly algorithm and its applications to single-cell sequencing. J. Comput. Biol. 2012, 19, 455–477. [Google Scholar] [CrossRef] [PubMed]
- Feldgarden, M.; Brover, V.; Haft, D.H.; Prasad, A.B.; Slotta, D.J.; Tolstoy, I.; Tyson, G.H.; Zhao, S.; Hsu, C.-H.; McDermott, P.F.; et al. Validating the AMRFinder Tool and Resistance Gene Database by Using Antimicrobial Resistance Genotype-Phenotype Correlations in a Collection of Isolates. Antimicrob. Agents Chemother. 2019, 63, e00483-19. [Google Scholar] [CrossRef] [PubMed]
- Spiliopoulou, I.; Kazmierczak, K.; Stone, G.G. In vitro activity of ceftazidime/avibactam against isolates of carbapenem-non-susceptible Enterobacteriaceae collected during the INFORM global surveillance programme (2015–17). J. Antimicrob. Chemother. 2020, 75, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Bakthavatchalam, Y.D.; Routray, A.; Mane, A.; Kamat, S.; Gupta, A.; Bari, A.K.; Rohit, A.; Poojary, A.; Mukherjee, D.N.; Sethuraman, N.; et al. In vitro activity of Ceftazidime–Avibactam and its comparators against Carbapenem resistant Enterobacterales collected across India: Results from ATLAS surveillance 2018 to 2019. Diagn. Microbiol. Infect. Dis. 2022, 103, 115652. [Google Scholar] [CrossRef]
- Abboud, M.I.; Damblon, C.; Brem, J.; Smargiasso, N.; Mercuri, P.; Gilbert, B.; Rydzik, A.M.; Claridge, T.D.; Schofield, C.J.; Frere, J.M. Interaction of Avibactam with Class B Metallo-beta-Lactamases. Antimicrob. Agents Chemother. 2016, 60, 5655–5662. [Google Scholar] [CrossRef]
- Hobson, C.A.; Pierrat, G.; Tenaillon, O.; Bonacorsi, S.; Bercot, B.; Jaouen, E.; Jacquier, H.; Birgy, A. Klebsiella pneumoniae Carbapenemase Variants Resistant to Ceftazidime-Avibactam: An Evolutionary Overview. Antimicrob. Agents Chemother. 2022, 66, e0044722. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, J.; Wang, R.; Cai, Y. Resistance to ceftazidime-avibactam and underlying mechanisms. J. Glob. Antimicrob. Resist. 2020, 22, 18–27. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Alffenaar, J.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Bianco, G.; Boattini, M.; Comini, S.; Leone, A.; Bondi, A.; Zaccaria, T.; Cavallo, R.; Costa, C. Implementation of Chromatic Super CAZ/AVI® medium for active surveillance of ceftazidime-avibactam resistance: Preventing the loop from becoming a spiral. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 1165–1171. [Google Scholar] [CrossRef]
- Bianco, G.; Boattini, M.; Comini, S.; Iannaccone, M.; Cavallo, R.; Costa, C. Rapid determination of ceftazidime/avibactam susceptibility of carbapenemase-producing Enterobacterales directly from blood cultures: A comparative evaluation of EUCAST disc diffusion RAST and direct Etest(R) RAST. J. Antimicrob. Chemother. 2022, 77, 1670–1675. [Google Scholar] [CrossRef]
- Lodise, T.P.; Smith, N.M.; O’Donnell, N.; Eakin, A.E.; Holden, P.N.; Boissonneault, K.R.; Zhou, J.; Tao, X.; Bulitta, J.B.; Fowler, V.G.; et al. Determining the optimal dosing of a novel combination regimen of ceftazidime/avibactam with aztreonam against NDM-1-producing Enterobacteriaceae using a hollow-fibre infection model. J. Antimicrob. Chemother. 2020, 75, 2622–2632. [Google Scholar] [CrossRef] [PubMed]
- Yasmin, M.; Fouts, D.E.; Jacobs, M.R.; Haydar, H.; Marshall, S.H.; White, R.; D’Souza, R.; Lodise, T.P.; Rhoads, D.D.; Hujer, A.M.; et al. Monitoring Ceftazidime-Avibactam and Aztreonam Concentrations in the Treatment of a Bloodstream Infection Caused by a Multidrug-Resistant Enterobacter sp. Carrying Both Klebsiella pneumoniae Carbapenemase–4 and New Delhi Metallo-β-Lactamase–1. Clin. Infect. Dis. 2020, 71, 1095–1098. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Hujer, A.M.; Rojas, L.J.; Papp-Wallace, K.M.; Humphries, R.M.; Spellberg, B.; Hujer, K.M.; Marshall, E.K.; Rudin, S.D.; Perez, F.; et al. Can Ceftazidime-Avibactam and Aztreonam Overcome β-Lactam Resistance Conferred by Metallo-β-Lactamases in Enterobacteriaceae? Antimicrob. Agents Chemother. 2017, 61, e02243-16. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, M.; Doyle, T.B.; Hubler, C.; Sader, H.S.; Mendes, R.E. Ceftazidime-avibactam activity against a challenge set of carbapenem-resistant Enterobacterales: Ompk36 L3 alterations and β-lactamases with ceftazidime hydrolytic activity lead to elevated MIC values. Int. J. Antimicrob. Agents 2020, 56, 106011. [Google Scholar] [CrossRef]
- Appel, T.M.; Mojica, M.F.; De La Cadena, E.; Pallares, C.J.; Radice, M.A.; Castañeda-Méndez, P.; Jaime-Villalón, D.A.; Gales, A.C.; Munita, J.M.; Villegas, M.V. In Vitro Susceptibility to Ceftazidime/Avibactam and Comparators in Clinical Isolates of Enterobacterales from Five Latin American Countries. Antibiotics 2020, 9, 62. [Google Scholar] [CrossRef]
- Hsu, L.Y.; Apisarnthanarak, A.; Khan, E.; Suwantarat, N.; Ghafur, A.; Tambyah, P.A. Carbapenem-Resistant Acinetobacter baumannii and Enterobacteriaceae in South and Southeast Asia. Clin. Microbiol. Rev. 2017, 30, 1–22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Antibiotics | No. of Isolates (%) | MIC50 (mg/L) | MIC90 (mg/L) | ||
|---|---|---|---|---|---|
| S | I | R | |||
| Amikacin | 685 (79.8) | 19 (2.2) | 154 (17.9) | ≤4 | ≥128 |
| Aztreonam | 58 (6.8) | 18 (2.1) | 782 (91.1) | ≥64 | ≥64 |
| Cefepime | 24 (2.8) | 71 (8.3) | 763 (88.9) | ≥64 | ≥64 |
| CZA | 591 (68.9) | - | 267 (31.1) | ≤1 | ≥128 |
| Doripenem | 40 (4.7) | 101 (11.8) | 717 (83.6) | 8 | ≥32 |
| Ertapenem | 0 | 11 (1.3) | 847 (98.7) | ≥32 | ≥32 |
| Imipenem | 9 (1.0) | 31 (3.6) | 818 (95.4) | 16 | ≥32 |
| Levofloxacin | 216 (25.2) | 128 (14.9) | 514 (59.9) | 8 | ≥64 |
| Meropenem | 24 (2.8) | 38 (4.4) | 796 (92.8) | 16 | ≥32 |
| Piperacillin/Tazobactam | 9 (1.0) | 14 (1.6) | 835 (97.3) | ≥128 | ≥128 |
| Polymyxin B | - | 718 (83.7) | 140 (16.3) | 0.5 | ≥16 |
| Tigecycline | 495 (57.7) | - | 363 (42.3) | 0.5 | 2 |
| Bacteria Species | No. of Isolates (n = 858) | CZA | Susceptibility to Comparators (% Isolates Susceptible) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cumulative Percentage of Isolates at Each MIC (mg/L) | |||||||||||||||||||||
| ≤1 | 2 | 4 | 8 | 16 | 32 | 64 | ≥128 | %S | AMK | AZT | FEP | DOR | ETR | IMI | LEV | MER | PT/4 | PMB * | TGC | ||
| Enterobacter cloacae complex | 147 | 53.1 | 63.9 | 64.6 | 64.6 | 65.3 | 65.3 | 65.3 | 100 | 64.6 | 91.2 | 8.2 | 4.8 | 4.1 | 0.0 | 0.0 | 29.9 | 2.7 | 3.4 | 0.0 | 63.9 |
| Escherichia coli | 252 | 58.3 | 61.1 | 63.1 | 66.3 | 66.3 | 66.3 | 66.3 | 100 | 66.3 | 88.9 | 10.3 | 2.4 | 10.3 | 0.0 | 1.2 | 27.4 | 5.2 | 0.8 | 0.0 | 92.1 |
| Klebsiella pneumoniae | 433 | 54.0 | 66.5 | 70.9 | 72.1 | 72.3 | 72.3 | 72.3 | 100 | 72.1 | 70.4 | 3.5 | 2.3 | 1.2 | 0.0 | 1.6 | 20.3 | 1.6 | 0.2 | 0.0 | 34.9 |
| Klebsiella species | 26 | 42.3 | 61.5 | 65.4 | 65.4 | 65.4 | 65.4 | 65.4 | 100 | 65.4 | 84.6 | 19.2 | 3.8 | 11.5 | 0.0 | 0.0 | 57.7 | 0.0 | 3.8 | 0.0 | 69.2 |
| No. of Isolates (n) | Carbapenemase Type | % (n) Isolates Susceptible to Each Antibiotic | |||||||
|---|---|---|---|---|---|---|---|---|---|
| CZA | Ertapenem | Imipenem | Meropenem | Doripenem | Aztreonam | Piperacillin-Tazobactam | Cefepime | ||
| 26 | Co-producer * | 0 (0) | 0 | 0 | 0 | 0 | 7.7(2) | 0 | 0 |
| 6 | IMI a | 100 (6) | 0 | 0 | 0 | 0 | 83.3 (5) | 83.3 (5) | 100 (6) |
| 11 | IMP | 0 (0) | 0 | 0 | 0 | 0 | 9.1 (1) | 9.1 (1) | 0 |
| 441 | KPC b | 99.3 (438) | 0 | 0.5 (2) | 2.3 (10) | 4.5 (20) | 0.7 (3) | 0.2 (1) | 2.0 (9) |
| 222 | NDM c | 0.5 (1) | 0 | 0 | 0 | 0 | 19.4 (43) | 0 | 0 |
| 58 | None | 91.4 (53) | 0 | 10.3 (6) | 8.6 (5) | 17.2 (10) | 1.7 (1) | 3.4 (2) | 6.9 (4) |
| 2 | OXA-23 | 100.0 (2) | 0 | 0 | 100.0 (2) | 100.0 (2) | 100.0 (2) | 0 | 50.0 (1) |
| 92 | OXA-48-like d | 98.9 (93) | 0 | 1.1 (1) | 7.6 (7) | 8.7 (8) | 1.1 (1) | 0 | 4.3 (4) |
| Organism | Carbapenemases | β-Lactamases | CZA MIC (mg/L) |
|---|---|---|---|
| Enterobacter cloacae complex | KPC-2 | ACT-1, SHV-12 | 16 |
| Escherichia coli | KPC-2 | EC | ≥128 |
| Escherichia coli | None | CMY-42, EC, OXA-1 | ≥128 |
| Escherichia coli | None | CTX-M-55, EC, TEM-1 | ≥128 |
| Klebsiella pneumoniae | None | CTX-M-15, SHV-11, TEM-1, OXA-1 | ≥128 |
| Klebsiella pneumoniae | OXA-232 | CTX-M-15, TEM-1, OXA-1 | ≥128 |
| Klebsiella pneumoniae | None | CTX-M-55, SHV-27, OXA-1 | 16 |
| Klebsiella pneumoniae | KPC-2 | CTX-M-65, LAP-2, SHV-12, TEM-1 | ≥128 |
| Klebsiella species | None | AmpC, DHA-1 | ≥128 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, T.-P.; Ho, J.-Y.; Teo, J.Q.-M.; Sim, J.H.-C.; Tan, S.-H.; Tan, T.-T.; Kwa, A.L.-H. In Vitro Susceptibility to Ceftazidime-Avibactam and Comparator Antimicrobial Agents of Carbapenem-Resistant Enterobacterales Isolates. Microorganisms 2023, 11, 2158. https://doi.org/10.3390/microorganisms11092158
Lim T-P, Ho J-Y, Teo JQ-M, Sim JH-C, Tan S-H, Tan T-T, Kwa AL-H. In Vitro Susceptibility to Ceftazidime-Avibactam and Comparator Antimicrobial Agents of Carbapenem-Resistant Enterobacterales Isolates. Microorganisms. 2023; 11(9):2158. https://doi.org/10.3390/microorganisms11092158
Chicago/Turabian StyleLim, Tze-Peng, Jun-Yuan Ho, Jocelyn Qi-Min Teo, James Heng-Chiak Sim, Si-Hui Tan, Thuan-Tong Tan, and Andrea Lay-Hoon Kwa. 2023. "In Vitro Susceptibility to Ceftazidime-Avibactam and Comparator Antimicrobial Agents of Carbapenem-Resistant Enterobacterales Isolates" Microorganisms 11, no. 9: 2158. https://doi.org/10.3390/microorganisms11092158