
Antimicrobial Resistance in Pseudomonas aeruginosa before and during the COVID-19 Pandemic

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection and Processing
2.2. Isolates Identification and Antimicrobial Susceptibility
2.3. Data and Statistical Analysis
2.4. Ethical Consideration Statement
2.5. Limitations
3. Results
3.1. Prevalence of PA Strains and Distribution by Gender and Biological Sources
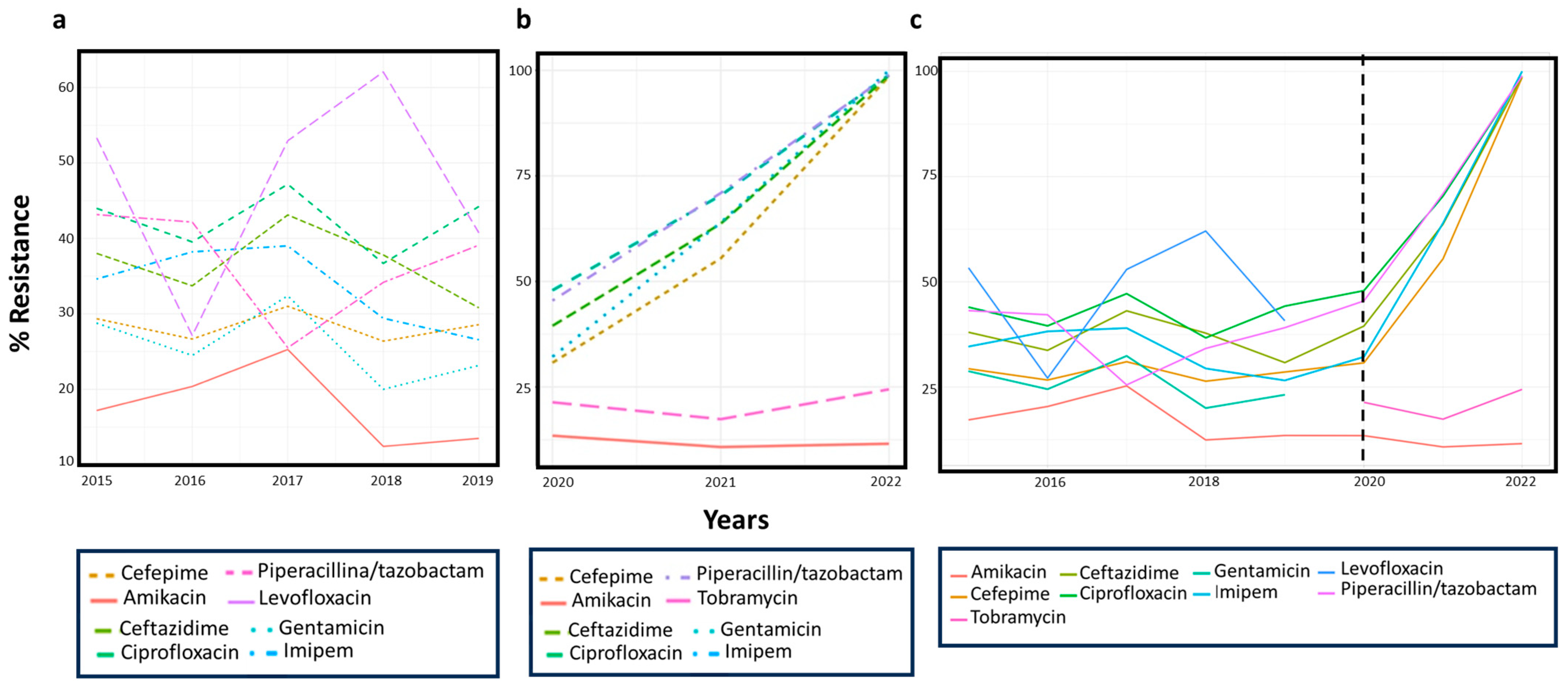
3.2. PA’s Antibiotics-Resistance Profile and Its Trend over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Gidey, K.; Gidey, M.T.; Hailu, B.Y.; Gebreamlak, Z.B.; Niriayo, Y.L. Clinical and Economic Burden of Healthcare-Associated Infections: A Prospective Cohort Study. PLoS ONE 2023, 18, e0282141. [Google Scholar] [CrossRef] [PubMed]
- Voidazan, S.; Albu, S.; Toth, R.; Grigorescu, B.; Rachita, A.; Moldovan, I. Healthcare Associated Infections-A New Pathology in Medical Practice? Int. J. Environ. Res. Public Health 2020, 17, 760. [Google Scholar] [CrossRef] [Green Version]
- Haque, M.; Sartelli, M.; McKimm, J.; Abu Bakar, M. Health Care-Associated Infections—An Overview. Infect. Drug Resist. 2018, 11, 2321–2333. [Google Scholar] [CrossRef] [Green Version]
- Gellatly, S.L.; Hancock, R.E.W. Pseudomonas aeruginosa: New Insights into Pathogenesis and Host Defenses. Pathog. Dis. 2013, 67, 159–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanc, D.S.; Francioli, P.; Zanetti, G. Molecular Epidemiology of Pseudomonas aeruginosa in the Intensive Care Units—A Review. Open Microbiol. J. 2007, 1, 8–11. [Google Scholar] [CrossRef]
- Moradali, M.F.; Ghods, S.; Rehm, B.H.A. Pseudomonas aeruginosa Lifestyle: A Paradigm for Adaptation, Survival, and Persistence. Front. Cell. Infect. Microbiol. 2017, 7, 39. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.L.; Sakr, Y.; Singer, M.; Martin-Loeches, I.; Machado, F.R.; Marshall, J.C.; Finfer, S.; Pelosi, P.; Brazzi, L.; Aditianingsih, D. Prevalence and Outcomes of Infection Among Patients in Intensive Care Units in 2017. JAMA 2020, 323, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Bergin, S.P.; Coles, A.; Calvert, S.B.; Farley, J.; Powers, J.H.; Zervos, M.J.; Sims, M.; Kollef, M.H.; Durkin, M.J.; Kabchi, A.A. PROPHETIC: Prospective Identification of Pneumonia in Hospitalized Patients in the ICU. Chest 2020, 158, 2370–2380. [Google Scholar] [CrossRef] [PubMed]
- Werneburg, G.T. Catheter-Associated Urinary Tract Infections: Current Challenges and Future Prospects. Res. Rep. Urol. 2022, 14, 109–133. [Google Scholar] [CrossRef] [PubMed]
- Rahim, K.; Saleha, S.; Basit, A.; Zhu, X.; Ahmed, I.; Liang, H.; Ping, Z.; Bakhtawar, U.; Shahzad, M.; Octavio, L.F. Pseudomonas aeruginosa as a Powerful Biofilm Producer and Positive Action of Amikacin Against Isolates from Chronic Wounds. Jundishapur. J. Microbiol. 2017, 10, e57564. [Google Scholar] [CrossRef] [Green Version]
- Breidenstein, E.B.M.; de la Fuente-Núñez, C.; Hancock, R.E.W. Pseudomonas aeruginosa: All Roads Lead to Resistance. Trends Microbiol. 2011, 19, 419–426. [Google Scholar] [CrossRef]
- Römling, U.; Balsalobre, C. Biofilm Infections, Their Resilience to Therapy and Innovative Treatment Strategies. J. Intern. Med. 2012, 272, 541–561. [Google Scholar] [CrossRef]
- Thi, M.T.T.; Wibowo, D.; Rehm, B.H.A. Pseudomonas aeruginosa Biofilms. Int. J. Mol. Sci. 2020, 21, 8671. [Google Scholar] [CrossRef]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, Research, and Development of New Antibiotics: The WHO Priority List of Antibiotic-Resistant Bacteria and Tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Rusic, D.; Vilovic, M.; Bukic, J.; Leskur, D.; Seselja Perisin, A.; Kumric, M.; Martinovic, D.; Petric, A.; Modun, D.; Bozic, J. Implications of COVID-19 Pandemic on the Emergence of Antimicrobial Resistance: Adjusting the Response to Future Outbreaks. Life 2021, 11, 220. [Google Scholar] [CrossRef]
- Hussain, M.; Khurram Syed, S.; Fatima, M.; Shaukat, S.; Saadullah, M.; Alqahtani, A.M.; Alqahtani, T.; Bin Emran, T.; Alamri, A.H.; Barkat, M.Q.; et al. Acute Respiratory Distress Syndrome and COVID-19: A Literature Review. J. Inflamm. Res. 2021, 14, 7225–7242. [Google Scholar] [CrossRef]
- Subramanya, S.H.; Czyż, D.M.; Acharya, K.P.; Humphreys, H. The Potential Impact of the COVID-19 Pandemic on Antimicrobial Resistance and Antibiotic Stewardship. Virusdisease 2021, 32, 330–337. [Google Scholar] [CrossRef]
- Kariyawasam, R.M.; Julien, D.A.; Jelinski, D.C.; Larose, S.L.; Rennert-May, E.; Conly, J.M.; Dingle, T.C.; Chen, J.Z.; Tyrrell, G.J.; Ronksley, P.E.; et al. Antimicrobial Resistance (AMR) in COVID-19 Patients: A Systematic Review and Meta-Analysis (November 2019–June 2021). Antimicrob. Resist. Infect. Control 2022, 11, 45. [Google Scholar] [CrossRef]
- Clancy, C.J.; Buehrle, D.J.; Nguyen, M.H. PRO: The COVID-19 Pandemic Will Result in Increased Antimicrobial Resistance Rates. JAC Antimicrob. Resist. 2020, 2, dlaa049. [Google Scholar] [CrossRef]
- Rehman, S. A Parallel and Silent Emerging Pandemic: Antimicrobial Resistance (AMR) amid COVID-19 Pandemic. J. Infect. Public Health 2023, 16, 611–617. [Google Scholar] [CrossRef]
- Sulayyim, H.J.A.; Ismail, R.; Hamid, A.A.; Ghafar, N.A. Antibiotic Resistance during COVID-19: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11931. [Google Scholar] [CrossRef]
- Despotovic, A.; Milosevic, B.; Cirkovic, A.; Vujovic, A.; Cucanic, K.; Cucanic, T.; Stevanovic, G. The Impact of COVID-19 on the Profile of Hospital-Acquired Infections in Adult Intensive Care Units. Antibiotics 2021, 10, 1146. [Google Scholar] [CrossRef]
- Ng, Q.X.; Ong, N.Y.; Lee, D.Y.X.; Yau, C.E.; Lim, Y.L.; Kwa, A.L.H.; Tan, B.H. Trends in Pseudomonas aeruginosa (P. aeruginosa) Bacteremia during the COVID-19 Pandemic: A Systematic Review. Antibiotics 2023, 12, 409. [Google Scholar] [CrossRef] [PubMed]
- Santella, B.; Serretiello, E.; De Filippis, A.; Veronica, F.; Iervolino, D.; Dell’Annunziata, F.; Manente, R.; Valitutti, F.; Santoro, E.; Pagliano, P.; et al. Lower Respiratory Tract Pathogens and Their Antimicrobial Susceptibility Pattern: A 5-Year Study. Antibiotics 2021, 10, 851. [Google Scholar] [CrossRef]
- Serretiello, E.; Folliero, V.; Santella, B.; Giordano, G.; Santoro, E.; De Caro, F.; Pagliano, P.; Ferro, M.; Aliberti, S.M.; Capunzo, M.; et al. Trend of Bacterial Uropathogens and Their Susceptibility Pattern: Study of Single Academic High-Volume Center in Italy (2015–2019). Int. J. Microbiol. 2021, 2021, 5541706. [Google Scholar] [CrossRef]
- Folliero, V.; Caputo, P.; Della Rocca, M.T.; Chianese, A.; Galdiero, M.; Iovene, M.R.; Hay, C.; Franci, G.; Galdiero, M. Prevalence and Antimicrobial Susceptibility Patterns of Bacterial Pathogens in Urinary Tract Infections in University Hospital of Campania “Luigi Vanvitelli” between 2017 and 2018. Antibiotics 2020, 9, 215. [Google Scholar] [CrossRef]
- Santella, B.; Folliero, V.; Pirofalo, G.M.; Serretiello, E.; Zannella, C.; Moccia, G.; Santoro, E.; Sanna, G.; Motta, O.; De Caro, F.; et al. Sepsis-A Retrospective Cohort Study of Bloodstream Infections. Antibiotics 2020, 9, 851. [Google Scholar] [CrossRef]
- Milite, C.; Castellano, S.; Benedetti, R.; Tosco, A.; Ciliberti, C.; Vicidomini, C.; Boully, L.; Franci, G.; Altucci, L.; Mai, A.; et al. Modulation of the Activity of Histone Acetyltransferases by Long Chain Alkylidenemalonates (LoCAMs). Bioorg. Med. Chem. 2011, 19, 3690–3701. [Google Scholar] [CrossRef] [Green Version]
- Horcajada, J.P.; Montero, M.; Oliver, A.; Sorlí, L.; Luque, S.; Gómez-Zorrilla, S.; Benito, N.; Grau, S. Epidemiology and Treatment of Multidrug-Resistant and Extensively Drug-Resistant Pseudomonas aeruginosa Infections. Clin. Microbiol. Rev. 2019, 32, e00031-19. [Google Scholar] [CrossRef]
- Urban-Chmiel, R.; Marek, A.; Stępień-Pyśniak, D.; Wieczorek, K.; Dec, M.; Nowaczek, A.; Osek, J. Antibiotic Resistance in Bacteria—A Review. Antibiotics 2022, 11, 1079. [Google Scholar] [CrossRef]
- De Rosa, A.; Mutters, N.T.; Mastroianni, C.M.; Kaiser, S.J.; Günther, F. Distribution of Carbapenem Resistance Mechanisms in Clinical Isolates of XDR Pseudomonas aeruginosa. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1547–1552. [Google Scholar] [CrossRef] [PubMed]
- Bessa, L.J.; Fazii, P.; Di Giulio, M.; Cellini, L. Bacterial Isolates from Infected Wounds and Their Antibiotic Susceptibility Pattern: Some Remarks about Wound Infection. Int. Wound J. 2015, 12, 47–52. [Google Scholar] [CrossRef]
- Saeed, M.; Rasheed, F.; Afzal, R.K.; Hussain, S.; Riaz, S.; Ahmad, A. Pseudomonas aeruginosa: Evaluation of Pathogen Burden and Drug-Resistance Trends in a Tertiary Care Hospital. J. Coll Physicians Surg. Pak. 2018, 28, 279–283. [Google Scholar] [CrossRef]
- Cabot, G.; Ocampo-Sosa, A.A.; Tubau, F.; Macia, M.D.; Rodríguez, C.; Moya, B.; Zamorano, L.; Suárez, C.; Peña, C.; Martínez-Martínez, L.; et al. Overexpression of AmpC and Efflux Pumps in Pseudomonas aeruginosa Isolates from Bloodstream Infections: Prevalence and Impact on Resistance in a Spanish Multicenter Study. Antimicrob. Agents Chemother. 2011, 55, 1906–1911. [Google Scholar] [CrossRef] [Green Version]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Antimicrobial Susceptibility of Gram-Negative Organisms Isolated from Patients Hospitalised with Pneumonia in US and European Hospitals: Results from the SENTRY Antimicrobial Surveillance Program, 2009–2012. Int. J. Antimicrob. Agents 2014, 43, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Iacchini, S.; Bellino, S.; D’Ancona, F.; Del Grosso, M.; Camilli, R.; Errico, G.; Pezzotti, P.; Pantosti, A.; Monaco, M. Referenti Regionali della rete AR-ISS. National surveillance of AR-ISS antibiotic resistance, data for the first half of 2020. Boll Epidemiol Naz 2020, 1, 46–50. [Google Scholar]
- Ventola, C.L. The Antibiotic Resistance Crisis: Part 1: Causes and Threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Lila, G.; Mulliqi-Osmani, G.; Bajrami, R.; Kurti, A.; Azizi, E.; Raka, L. The Prevalence and Resistance Patterns of Pseudomonas aeruginosa in a Tertiary Care Hospital in Kosovo. Infez. Med. 2017, 25, 21–26. [Google Scholar]
- Vázquez-López, R.; Solano-Gálvez, S.G.; Juárez Vignon-Whaley, J.J.; Abello Vaamonde, J.A.; Padró Alonzo, L.A.; Rivera Reséndiz, A.; Muleiro Álvarez, M.; Vega López, E.N.; Franyuti-Kelly, G.; Álvarez-Hernández, D.A.; et al. Acinetobacter Baumannii Resistance: A Real Challenge for Clinicians. Antibiotics 2020, 9, 205. [Google Scholar] [CrossRef] [Green Version]
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic Resistance: A Rundown of a Global Crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [Green Version]
- Raoofi, R.; Namavari, N.; Rahmanian, V.; Dousthaghi, M.H. Evaluation of antibiotics resistance in Southern Iran in light of COVID-19 pandemic: A retrospective observational study. Health Sci. Rep. 2023, 6, e1153. [Google Scholar] [CrossRef] [PubMed]
- Coșeriu, R.L.; Vintilă, C.; Mare, A.D.; Ciurea, C.N.; Togănel, R.O.; Cighir, A.; Simion, A.; Man, A. Epidemiology, Evolution of Antimicrobial Profile and Genomic Fingerprints of Pseudomonas aeruginosa before and during COVID-19: Transition from Resistance to Susceptibility. Life 2022, 12, 2049. [Google Scholar] [CrossRef] [PubMed]
- Surveillance Atlas of Infectious Diseases. Available online: https://www.ecdc.europa.eu/en/surveillance-atlas-infectious-diseases (accessed on 28 September 2022).
- da Rosa, T.F.; Coelho, S.S.; Foletto, V.S.; Bottega, A.; Serafin, M.B.; de Souza Machado, C.; Franco, L.N.; de Paula, B.R.; Hörner, R. Alternatives for the Treatment of Infections Caused by ESKAPE Pathogens. J. Clin. Pharm. Ther. 2020, 45, 863–873. [Google Scholar] [CrossRef]
- Lowrence, R.C.; Ramakrishnan, A.; Sundaramoorthy, N.S.; Shyam, A.; Mohan, V.; Subbarao, H.M.V.; Ulaganathan, V.; Raman, T.; Solomon, A.; Nagarajan, S. Norfloxacin Salts of Carboxylic Acids Curtail Planktonic and Biofilm Mode of Growth in ESKAPE Pathogens. J. Appl. Microbiol. 2018, 124, 408–422. [Google Scholar] [CrossRef]
- Chatterjee, M.; Anju, C.P.; Biswas, L.; Anil Kumar, V.; Gopi Mohan, C.; Biswas, R. Antibiotic Resistance in Pseudomonas aeruginosa and Alternative Therapeutic Options. Int. J. Med. Microbiol. 2016, 306, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Lob, S.H.; Hackel, M.A.; Kazmierczak, K.M.; Young, K.; Motyl, M.R.; Karlowsky, J.A.; Sahm, D.F. In Vitro Activity of Imipenem-Relebactam against Gram-Negative ESKAPE Pathogens Isolated by Clinical Laboratories in the United States in 2015 (Results from the SMART Global Surveillance Program). Antimicrob. Agents Chemother. 2017, 61, e02209-16. [Google Scholar] [CrossRef] [Green Version]
- Papp-Wallace, K.M.; Zeiser, E.T.; Becka, S.A.; Park, S.; Wilson, B.M.; Winkler, M.L.; D’Souza, R.; Singh, I.; Sutton, G.; Fouts, D.E.; et al. Ceftazidime-Avibactam in Combination With Fosfomycin: A Novel Therapeutic Strategy Against Multidrug-Resistant Pseudomonas aeruginosa. J. Infect. Dis. 2019, 220, 666–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunz Coyne, A.J.; El Ghali, A.; Holger, D.; Rebold, N.; Rybak, M.J. Therapeutic Strategies for Emerging Multidrug-Resistant Pseudomonas aeruginosa. Infect Dis Ther. 2022, 11, 661–682. [Google Scholar] [CrossRef]
- Vasala, A.; Hytönen, V.P.; Laitinen, O.H. Modern Tools for Rapid Diagnostics of Antimicrobial Resistance. Front. Cell. Infect. Microbiol. 2020, 10, 308. [Google Scholar] [CrossRef]
- Lingas, E.C. Empiric Antibiotics in COVID 19: A Narrative Review. Cureus 2022, 14, e25596. [Google Scholar] [CrossRef]
- Rezasoltani, S.; Yadegar, A.; Hatami, B.; Asadzadeh Aghdaei, H.; Zali, M.R. Antimicrobial Resistance as a Hidden Menace Lurking Behind the COVID-19 Outbreak: The Global Impacts of Too Much Hygiene on AMR. Front. Microbiol. 2020, 11, 590683. [Google Scholar] [CrossRef] [PubMed]
- İpek, S.; Şahin, A.; Gungor, S.; Yurttutan, S.; Güllü, U.U.; Inal, S.; Demiray, Ş. Nosocomial Infections in Non-COVID-19 Pediatric Patients Prior to and During the Pandemic in a Pediatric Intensive Care Unit. Cureus 2022, 14, e21451. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, D.; Kollef, M. The Epidemiology and Pathogenesis and Treatment of Pseudomonas aeruginosa Infections: An Update. Drugs 2021, 81, 2117–2131. [Google Scholar] [CrossRef] [PubMed]
- Shallcross, L.J.; Howard, S.J.; Fowler, T.; Davies, S.C. Tackling the Threat of Antimicrobial Resistance: From Policy to Sustainable Action. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2015, 370, 20140082. [Google Scholar] [CrossRef]
- Serrano, I.; Alhinho, B.; Cunha, E.; Tavares, L.; Trindade, A.; Oliveira, M. Bacteriostatic and Antibiofilm Efficacy of a Nisin Z Solution against Co-Cultures of Staphylococcus Aureus and Pseudomonas aeruginosa from Diabetic Foot Infections. Life 2023, 13, 504. [Google Scholar] [CrossRef]


{kind=link}
| (a) | ||||||
| Years | 2015 | 2016 | 2017 | 2018 | 2019 | Tot. |
| Sex | N. (%) | N. (%) | N. (%) | N. (%) | N. (%) | N. (%) |
| F | 104 (35.6%) | 143 (41.7%) | 143 (49.5%) | 147 (40.1%) | 175 (39.1%) | 712 (40.9%) |
| M | 188 (64.4%) | 200 (58.3%) | 146 (50.5%) | 220 (59.9%) | 273 (60.9%) | 1027 (59.1%) |
| Tot. for Year | 292 (100%) | 343 (100%) | 289 (100%) | 367 (100%) | 448 (100%) | 1739 (100%) |
| (b) | ||||||
| Years | 2020 | 2021 | 2022 | Tot. | ||
| Sex | N. (%) | N. (%) | N. (%) | N. (%) | ||
| F | 112 (31.55%) | 170 (35.8%) | 221 (44.3%) | 503 (38.5%) | ||
| M | 243 (68.5%) | 305 (64.2%) | 256 (53.7%) | 804 (61.5%) | ||
| Tot. for Year | 355 (100%) | 475 (100%) | 477 (100%) | 1307 (100%) | ||
| (a) | ||||||||||||
| Years | 2015–2019 | 2015 | 2016 | 2017 | 2018 | 2019 | ||||||
| Samples | Isolates n. | Isolates % | Isolates n. | Isolates % | Isolates n. | Isolates % | Isolates n. | Isolates % | Isolates n. | Isolates % | Isolates n. | Isolates % |
| Respiratory | 590 | 33.9% | 114 | 39.0% | 98 | 28.6% | 112 | 38.8% | 127 | 34.6% | 139 | 23.2% |
| Wound swabs | 375 | 21.6% | 58 | 19.9% | 73 | 21.3% | 60 | 20.8% | 80 | 21.3% | 104 | 31.0% |
| Urinary | 296 | 17.0% | 33 | 10.3% | 60 | 17.5% | 45 | 15.6% | 78 | 21.8% | 80 | 17.9% |
| Cultural swab | 210 | 12.1% | 30 | 11.3% | 46 | 13.4% | 33 | 11.4% | 37 | 10.1% | 64 | 14.3% |
| Blood and Liquor culture | 130 | 7.5% | 27 | 9.2% | 31 | 9.0% | 13 | 4.5% | 25 | 6.8% | 34 | 7.6% |
| Catheters | 65 | 3.7% | 16 | 5.5% | 16 | 4.7% | 13 | 4.5% | 10 | 2.7% | 10 | 3.1% |
| Vaginal swabs | 45 | 2.6% | 4 | 3.4% | 12 | 3.5% | 10 | 3.5% | 5 | 1.4% | 14 | 2.2% |
| Others | 28 | 1.6% | 10 | 1.4% | 7 | 2.0% | 3 | 1.0% | 5 | 1.4% | 3 | 0.7% |
| Tot. Isolates | 1739 | 100% | 292 | 100% | 343 | 100% | 289 | 100% | 367 | 100% | 448 | 100% |
| (b) | ||||||||||||
| Years | 2020–2022 | 2020 | 2021 | 2022 | ||||||||
| Samples | Isolates n. | Isolates % | Isolates n. | Isolates % | Isolates n. | Isolates % | Isolates n. | Isolates % | ||||
| Respiratory | 397 | 30.4% | 107 | 30.1% | 166 | 34.9% | 124 | 26.0% | ||||
| Urinary | 249 | 19.1% | 66 | 18.6% | 86 | 18.1% | 97 | 20.3% | ||||
| Wound swabs | 237 | 18.1% | 62 | 17.5% | 70 | 14.7% | 105 | 22.0% | ||||
| Cultural swab | 191 | 14.6% | 56 | 15.8% | 70 | 14.7% | 65 | 13.6% | ||||
| Blood and Liquor culture | 133 | 10.2% | 36 | 10.1% | 50 | 10.5% | 47 | 9.9% | ||||
| Others | 43 | 3.3% | 12 | 3.4% | 22 | 4.6% | 9 | 1.9% | ||||
| Catheters | 40 | 3.1% | 12 | 3.4% | 9 | 1.9% | 19 | 4.0% | ||||
| Vaginal swabs | 17 | 1.3% | 4 | 1.1% | 2 | 0.4% | 11 | 2.3% | ||||
| Tot. Isolates | 1307 | 100% | 355 | 100% | 475 | 100% | 477 | 100% | ||||
| (a) | ||||||||||||||
| Antibiotics | 2015 | 2016 | 2017 | 2018 | 2019 | Total Years | p-Value | p-Value Trend | ||||||
| R | N. Test | R | N. Test | R | N. Test | R | N. Test | R | N. Test | R | N. Test | |||
| Pip./taz. | 43.2% | 285 | 42.2% | 332 | 25.5% | 196 | 34.2% | 357 | 39.1% | 445 | 37.7% | 1615 | 0.001 | 0.11 |
| Ceftazidime | 38.0% | 292 | 33.7% | 344 | 43.1% | 283 | 29.9% | 365 | 30.8% | 448 | 34.4% | 1732 | 0.01 | 0.126 |
| Cefepime | 29.4% | 293 | 26.7% | 345 | 31.0% | 287 | 26.4% | 307 | 28.6% | 147 | 28.3% | 1379 | 0.69 | 0.794 |
| Imipenem | 34.6% | 286 | 39.0% | 341 | 39.0% | 282 | 29.4% | 306 | 26.6% | 143 | 34.6% | 1358 | 0.02 | 0.0221 |
| Amikacin | 17.2% | 285 | 20.4% | 319 | 25.3% | 273 | 12.4% | 354 | 13.5% | 415 | 17.2% | 1646 | <0.0001 | 0.089 |
| Gentamicin | 28.8% | 292 | 24.5% | 343 | 32.4% | 284 | 20.0% | 365 | 23.2% | 449 | 25.2% | 1733 | 0.00 | 0.0326 |
| Ciprofloxacin | 44.0% | 291 | 39.5% | 344 | 47.2% | 284 | 37.8% | 365 | 44.2% | 450 | 42.4% | 1734 | 0.09 | 0.931 |
| Levofloxacin | 53.3% | 15 | 53.3% | 30 | 52.9% | 34 | 62.1% | 29 | 40.7% | 54 | 50.6% | 162 | 0.01 | 0.312 |
| (b) | ||||||||||||||
| Antibiotics | 2020 | 2021 | 2022 | Total Years | p-Value | p-Value Trend | ||||||||
| I | R | N. Test | I | R | N. Test | I | R | N. Test | I | R | N. Test | |||
| Pip./taz. | 11.7% | 40.1% | 349 | 43.4% | 40.2% | 468 | 60.2% | 39.2% | 475 | 41.0% | 39.8% | 1292 | 0.0188 | 0.017 |
| Ceftazidime | 13.2% | 34.3% | 356 | 53.0% | 30.0% | 474 | 66.4% | 35.3% | 467 | 46.9% | 33.1% | 1297 | 0.0497 | 0.0143 |
| Cefepime | 9.7% | 27.8% | 299 | 55.5% | 24.7% | 474 | 70.3% | 28.5% | 478 | 50.2% | 26.9% | 1251 | 0.00249 | <0.001 |
| Imipenem | 5.7% | 30.3% | 300 | 48.6% | 32.8% | 475 | 66.3% | 33.7% | 478 | 45.1% | 32.6% | 1253 | <0.001 | <0.001 |
| Amikacin | 1.5% | 13.3% | 332 | 0.4% | 10.7% | 466 | 0.0% | 11.6% | 476 | 0.5% | 11.7% | 1274 | 0.553 | 0.278 |
| Tobramycin | 0% | 21.4% | 248 | 0.0% | 17.4% | 380 | 0.0% | 24.4% | 401 | 0.0% | 21.1% | 1029 | <0.001 | <0.001 |
| Ciprofloxacin | 13.2% | 41.6% | 356 | 48.7% | 36.1% | 474 | 60.5% | 39.1% | 478 | 43.3% | 38.7% | 1308 | 0.124 | 0.0422 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serretiello, E.; Manente, R.; Dell’Annunziata, F.; Folliero, V.; Iervolino, D.; Casolaro, V.; Perrella, A.; Santoro, E.; Galdiero, M.; Capunzo, M.; et al. Antimicrobial Resistance in Pseudomonas aeruginosa before and during the COVID-19 Pandemic. Microorganisms 2023, 11, 1918. https://doi.org/10.3390/microorganisms11081918
Serretiello E, Manente R, Dell’Annunziata F, Folliero V, Iervolino D, Casolaro V, Perrella A, Santoro E, Galdiero M, Capunzo M, et al. Antimicrobial Resistance in Pseudomonas aeruginosa before and during the COVID-19 Pandemic. Microorganisms. 2023; 11(8):1918. https://doi.org/10.3390/microorganisms11081918
Chicago/Turabian StyleSerretiello, Enrica, Roberta Manente, Federica Dell’Annunziata, Veronica Folliero, Domenico Iervolino, Vincenzo Casolaro, Alessandro Perrella, Emanuela Santoro, Massimiliano Galdiero, Mario Capunzo, and et al. 2023. "Antimicrobial Resistance in Pseudomonas aeruginosa before and during the COVID-19 Pandemic" Microorganisms 11, no. 8: 1918. https://doi.org/10.3390/microorganisms11081918