

Green Alternatives as Antimicrobial Agents in Mitigating Periodontal Diseases: A Narrative Review


Abstract
:1. Introduction
2. Methods
3. Periodontitis
4. Plant-Based Antimicrobials against Periodontitis
4.1. Acacia arabica (Babul)
4.2. Acacia nilotica
4.3. Allium sativum (Garlic)
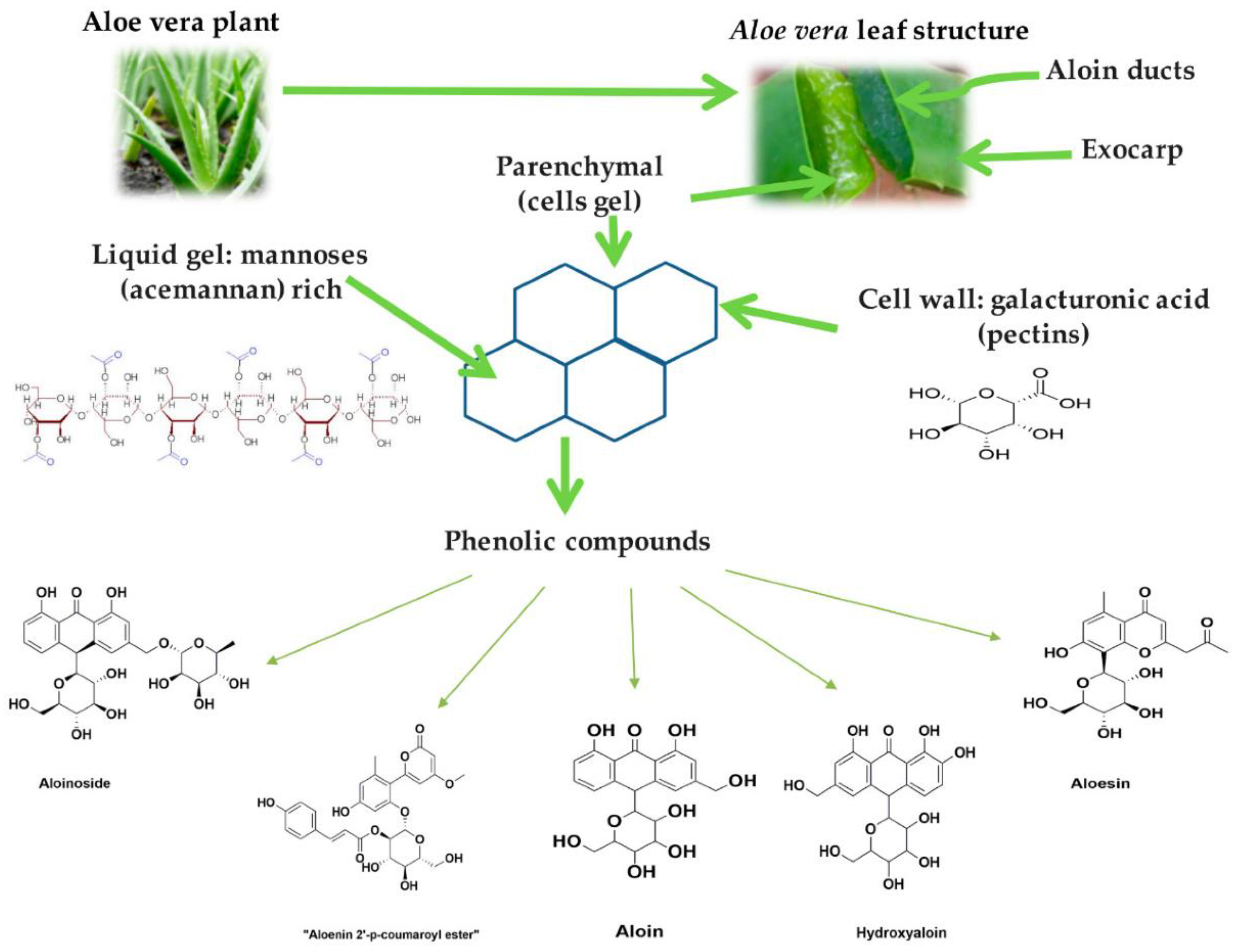
4.4. Aloe barbadensis Miller (Aloe Vera)
4.5. Amphipterygium adstringens
4.6. Azadirachta indica [109]
4.7. Berberis vulgaris
4.8. Camellia sinensis (Green Tea)
4.9. Cinnamomum zeylanicum (Ceylon Cinnamon)
4.10. Citrus sinensis
4.11. Coffea canephora (Coffee)
4.12. Copaifera pubiflora
4.13. Coptidis rhizoma
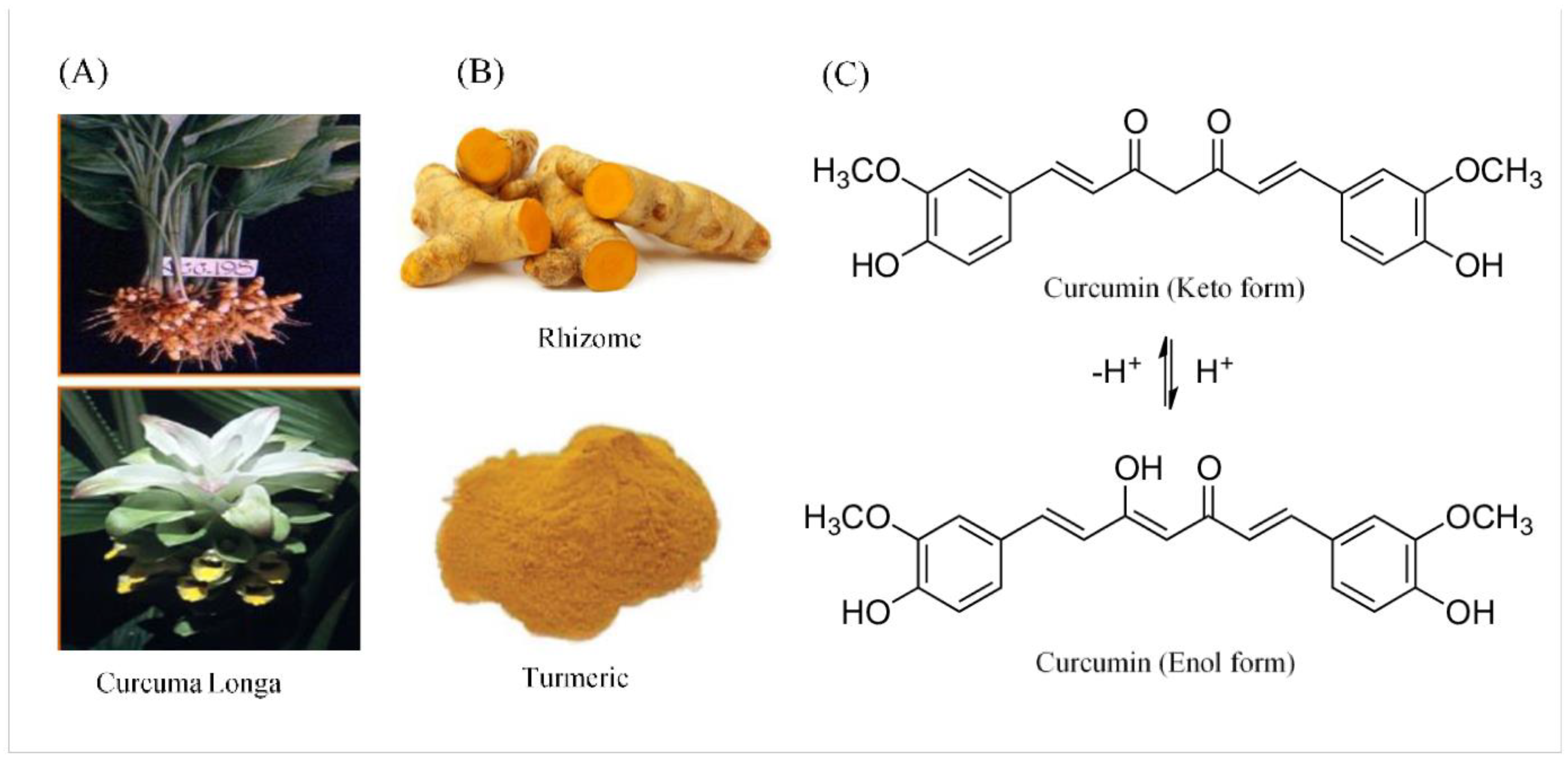
4.14. Curcuma longa (Turmeric)
4.15. Cymbopogon citratus (Lemongrass)
4.16. Eucalyptus globulus
4.17. Garcinia mangostana
4.18. Glycyrrhiza glabra and Glycyrrhiza uralensis (Chinese Licorice)
4.19. Hibiscus sabdariffa
4.20. Inula viscosa (False Yellowhead)
4.21. Juglans regia

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Natural Compound | Study Type | Samples Studied | Methods | Result(s)/Conclusion(s) | Ref./Year |
|---|---|---|---|---|---|
| Acacia nilotica | In vivo | Albino rabbits with ligature-induced periodontitis | G1: Distilled water G2: Positive control group G3: A. nilotica aqueous extract (dosage 300 mg/kg) G4: A. nilotica aqueous extract (dosage 500 mg/kg) G5: Amoxicillin (15 mg/kg) [CBC, ESR, serum creatinine, ALT, and AST were measured after 14 days] | A. nilotica extract significantly cured periodontitis to a great extent after 14 consecutive days of oral administration. | [292]/2019 |
| Allium sativum | In vitro | P. gingivalis, F. nucleatum, A. a. | Gs: An aqueous extract of Allium sativum [Disc diffusion technique, microspindle dilution method, and assessment of MIC and MBC were performed] | Allium sativum extract at 55.2% w/v produced inhibition zones of 17.3 ± 1.0, 30.3 ± 1.7, and 21.2 ± 2.3 mm with A. a, F. nucleatum, and P. gingivalis, respectively. MIC of 17.2, 1.1, and 4.3 mg/mL was obtained for A. a, F. nucleatum, and P. gingivalis, respectively. The MBC was 34.4, 1.1, and 8.6 mg/mL, respectively. Allium sativum aqueous extract may be a therapeutic alternative for treating periodontal disease based on the results obtained in this study. | [293]/2021 |
| In vitro | L. acidophilus, S. aureus, S. sanguis, S. mutans, S. salivarius | Gs: Allium sativum bulb [MIC and MBC were measured] | A. sativum bulbs are effective in treating periodontitis and dental caries. MBC value ranged from 60 ± 5 to 215 ± 7 mg/mL and MIC value ranged between 20 ± 2 and 120 ± 6 mg/mL. | [80]/2020 | |
| In vitro | P. gingivalis | G1: Aqueous garlic extract G2: 0.2% CHX [Groups were compared regarding MIC and MBC] | A significant difference was observed between G1 and G2 (0.29 ± 0.1 μL; p < 0.001) regarding the MIC (1.21 ± 0.37 μL) and MBC (1.44 ± 0.67 μL) against P. gingivalis. As compared to G1 (20.1 ± 1.4 mm), G2 (27.3 ± 1.8 mm) showed a significantly larger inhibitory zone against P. gingivalis (p < 0.000). Garlic extracts performed well as antimicrobial agents against P. gingivalis; however, they were not superior to CHX as antimicrobial agents. | [294]/2019 | |
| Aloe barbadensis Miller | In vitro | C. albicans, S. mutans, L. acidophilus, E. faecalis, P. intermedia, P. anaerobius | G1: Aloe vera tooth gel G2: Pepsodent toothpaste G3: Colgate toothpaste [Zone of inhibition was measure] | In preliminary tests, Aloe vera tooth gel and other toothpastes had similar antibacterial effects. S. mitis benefited from an enhanced antibacterial impact by Aloe vera tooth gel (p = 0.034). | [295]/2009 |
| Amphipterygium adstringens | In vitro | S. mutans, P. gingivalis, A. a, E. coli, C. albicans, C. dubliniensis | Gc: 0.12% CHX Gs: A methanolic extract of A. Adstringens [MIC, MBC, and total growth inhibition were measured] | All microbial strains tested with methane extracts of A. adstringens exhibited antimicrobial activity between 0.125 and 63 mg/mL. MIC of S. mutans was 0.125 mg/mL, and MBC was 0.31 mg/mL, making it the most sensitive strain. The MIC and MFC of Candida strains were 0.4 and 1.6 mg/mL, respectively. An MIC/MBC of 37 mg/mL was observed for both P. gingivalis and E. coli. With an inhibitory concentration of 63 mg/mL, A. a and E. coli also exhibited similar results. An MBC of 2.4 mg/L was found for chlorhexidine. | [296]/2015 |
| Azadirachta indica, Syzygium aroticum, and Cinnamomum zeylanicum | Ex vivo | Actinobacillus sp. | Gc: Tetracycline and azithromycin (30 mcg/mL) Gs: Neem, clove, and cinnamon in aqueous and acetone solvents (2%, 4%, 6%, 8%, and 10%) [Zone of inhibition was measured] | Actinobacillus sp. were inhibited at 10% concentration by aqueous extracts of clove and neem (24 and 22 mm, respectively). At the same concentration, aqueous cinnamon extracts displayed only a moderate inhibition zone (16 mm). Acetone extracts of neem and clove showed effective inhibition of Actinobacillus sp. (20 and 18 mm, respectively) compared with cinnamon, which showed a moderate inhibition zone (14 mm). Neem, clove, and cinnamon extracts could be used as an alternative treatment for chronic periodontitis. | [297]/2020 |
| Berberis vulgaris | In vivo | Rats with ligature-induced periodontitis | Gc: Cholisal gel Gs: A dental gel containing barberry extract. [Histopathology and ultrasound dopplerography were performed] | Periodontitis can be effectively treated with a dental gel containing 0.015 mg/g of barberry root extract. | [130]/2020 |
| Cinnamomum burmanii | In vitro | An A. a. or E. coli LPS-stimulated macrophage model | Gs: Cinnamon bark aqueous extract [Cytokine production, binding of LPS cells, and PPAR-γ binding were studied] | IL-6, TNF-α, and IL-8 secretion was reduced by the cinnamon fraction in a dose-dependent manner. A cinnamon fraction may have anti-inflammatory properties by reducing LPS binding to monocytes. A natural PPAR-γ ligand may exist in the cinnamon fraction as well. A cinnamon fraction has been shown to contain anti-inflammatory properties that can be used to treat periodontal disease due to its anti-inflammatory properties. | [298]/2021 |
| Cinnamomum zeylanicum | In vitro | P. gingivalis | Gs: Different concentrations of cinnamon with oil solvent (10, 50, 100, 250, 500, 750, and 1500 mg/mL) Gc: Amoxicillin, metronidazole, ciprofloxacin, amikacin, and gentamycin [MBC and MIC were evaluated] | Cinnamon at an MIC value of 750 mg/mL inhibited bacteria, while cinnamon at an MIC value of 1500 mg/mL killed them. The antibacterial activity was, however, much weaker than that of common antibiotics (p < 0.001). The antimicrobial activity of cinnamon against the pathogen P. gingivalis was demonstrated in patients with chronic periodontitis with deep pockets. | [299]/2018 |
| In vitro | A. a, F. nucleatum, P. gingivalis, S. salivarius, S. mitis, and S. mutans | Gs: EO from cinnamon tree bark + cinnamaldehyde [MIC was measured] | An MIC of 0.21–0.63 mg/mL was observed for cinnamon oil and 0.8–0.15 mg/mL for cinnamaldehyde against the tested bacteria. Changes in cell membranes were observed after two hours of exposure to the oil. Bacterial infections of the oral cavity can be prevented by cinnamon bark oil. | [300]/2013 | |
| Citrus sinensis | In vitro | P. gingivalis | Gs: Citrus sinensis [MIC, SI, and IC50 were measured] | Citrus sinensis exhibited low cytotoxicity and good antibacterial activity. It demonstrated an IC50 value of 512 μg/mL. | [155]/2020 |
| Coffea canephora | In vitro | P. gingivalis | Gs: Coffee extract and chlorogenic acid [The inhibitory effect, protease activity, and viability of P. gingivalis were evaluated] | Chlorogenic acid had an MIC of 4 mg/mL and an MBC of 16 mg/mL. When chlorogenic acid is applied above the MIC, the viability of P. gingivalis is inhibited for a longer period of time and the activity of the associated protease is significantly reduced. Different roast levels of coffee had no effect on the antibacterial activity of the extract. | [206]/2019 |
| Coptidis rhizoma | In vitro | A. naeslundii A. a, P. gingivalis, P. nigrescens, P. intermedia | Gs: C. rhizoma extract. [MIC and IC50 were measured] | MICs of 0.031–0.25 mg/mL inhibited the growth of the mentioned bacteria, while MICs of 0.5–2 mg/mL inhibited the growth of Lactobacillus and Streptococcus. C. rhizoma extract inhibited periodontopathogenic bacteria. Clinical application of these results may be possible for treating periodontal diseases. | [126]/2000 |
| Curcuma longa | In vivo | Rats with induced periodontitis | Gs: Curcumin-loaded nanoparticles | The μCT analysis demonstrated significant attenuation of NF-kB activation and p38 MAPK activity resulting from curcumin local administration. Inflammatory bone resorption, osteoclast counts, and inflammation infiltrates were significantly reduced. Experimental periodontal disease was effectively treated with curcumin-loaded nanoparticles. | [301]/2018 |
| In vivo | Wistar rats with ligature-induced periodontitis | G1: Placebo G2: Resveratrol G3: Curcumin G4: Resveratrol + curcumin [Morphometric analysis of bone loss was performed histologically; TNF-α, IL-4, IFN-γ, and IL-1β were studied] | As compared with the other groups, G1 showed greater bone loss than the other groups based on intergroup comparisons (p < 0.05). G2, G3, and G4 did not have different bone-loss values (p > 0.05). In G4, IL-1 β levels were lower than in G1 based on the immunoenzymatic assay of gingival tissue (p < 0.05). In comparison with G1, G2, and G3, G4 showed higher IL-4 values (p < 0.05). The levels concerning IFN-γ were only reduced by G2 (p < 0.05). Among the four groups, the TNF-α concentrations did not differ (p > 0.05). There was a reduction in alveolar bone loss due to resveratrol and curcumin. It was not found that these agents combined or synergized in any way. | [302]/2017 | |
| Cymbopogon citratus | In vitro | S. mutans, S. epidermidis, Lactobacillus | Gc: Tetracycline Gs: Lemongrass EO [Inhibition zone measurement] | The minimal inhibitory concentration of lemongrass EO was estimated to be 10 μL. A statistically significant zone of inhibition, and the antibacterial zone was more marked in Gs than Gc for S. mutans and S. epidermis (p < 0.001). Tetracycline had less antibacterial activity than lemongrass. Therefore, the herbal EO may be an adjunctive treatment for periodontitis or an alternative to tetracycline. | [303]/2019 |
| In vitro | A. naeslundii, P. gingivalis | Gs: Cymbopogon citratus EO [MIC was measured] | Based on the results, EO had MIC values of 0.44 and 0.22 mg/mL against A. naeslundii and P. gingivalis. Both reference strains and most clinical isolates, especially the tetracycline-resistant strains, are sensitive to Cymbopogon citratus EO. | [239]/2009 | |
| Eucalyptus globulus | In vitro | P. gingivalis, F. nucleatum, A. a | Gs: Eucalyptus globulus EOs [Their antioxidant capacity and MIC were measured] | In the analyzed oils, the antioxidant activity was weak, although the antibacterial activity was significant, especially against F. nucleatum (MIC = 1.14 mg/mL) and P. gingivalis (MIC = 0.28 mg/mL). A potential therapeutic application for E. globulus EOs may be periodontal disease treatment. | [304]/2015 |
| Garcinia mangostana | In vivo | Wistar rats with administered A. a | G1: Tetracycline gel (0.7%) G2: Mucoadhesive patch G2: An extract of mangosteen peel applied to a mucoadhesive patch [Histopathological examinations were performed to quantify osteoblasts and osteoclasts] | Osteoclasts and osteoblasts were significantly reduced in all groups by G3 (p < 0.05). Mangosteen peel extract inhibited osteoclasts and stimulated osteoblasts, thus preventing alveolar bone damage in periodontitis. | [305]/2021 |
| Glycyrrhiza uralensis | In vitro | P. gingivalis | Gs: Glycyrrhiza uralensis root extract [MIC and MBC were evaluated] | It was found that the licorice root extract had antimicrobial activity against P. gingivalis at an MIC value of 62.5 μg/mL and an MBC value of 25 μg/mL. Biofilms of P. gingivalis were also affected by licorice root extract. A potential therapeutic application of licorice root extract could be for periodontal disease. | [306]/2017 |
| In vivo | GCF samples from patients with mild–moderate periodontitis | G1: Doxycycline G2: Licorice G3: Placebo [MMP-8 concentration was measured] | There was a statistically significant difference between G1 and G2 and G3 in the mean MMP-8 concentrations (p < 0.001). A statistically significant difference was not detected between G2 and G1 in the mean MMP-8 concentration. Licorice extract is a powerful natural remedy for periodontitis and inflammation, as well as preventing MMPs from being released by the host cells. There were no side effects associated with the use of licorice extract. | [261]/2013 | |
| Glycyrrhiza glabra | In vitro | Pathogens responsible for plaque colonization and periodontitis | Gs: Glycyrrhiza uralensis bark extract [Zone of inhibition was measured] | A potential antibacterial effect was observed for G. glabra against primary plaque colonizers and periodontal pathogens (ZOI = 9.2 ± 1.09 and 10.6 ± 0.54 mm, respectively). Statistically, there was no significant difference between G. glabra and standard antibiotics for periodontal pathogens. | [307]/2016 |
| Juglans regia | In vitro | G. adiacens, S. sciuri, Kocuria spp. | Gc: Ciprofloxacin (5 μg/mL) + cefotaxime (30 μg/mL) Gs: Crude aqueous extracts from Juglans regia (100 mg/mL, 250 mg/mL, 500 mg/mL). [Measurement of zone of inhibition] | Compared to the other extracts, the 250 mg/mL extract was more effective. The extract showed the greatest impact on Kocuria spp. The extract’s active components increased biological activities, thus aiding in fighting bacterial infections. | [308]/2021 |
| In vitro | P. gingivalis | G1: Immature fruit ethanol extraction G2: Immature fruit methanol extraction G3: Woody parts ethanol extraction G4: Woody stems ethanol extraction G5: Woody stems methanol extraction [MIC, SI, and IC50 were measured] | The MIC and SI of the five extracts of J. regia studied were as follows: G5 (MIC 64 μg/mL, SI > 16), SI > 16), G4 (MIC 64 μg/mL, SI > 16), G3 (MIC 32 μg/mL, SI > 32), G2 (MIC 32 μg/mL, SI > 32), and G1 (MIC 64 μg/mL. | [155]/2020 | |
| In vitro | S. mutans, S. salivarius, S. sanguis, S. aureus | Gc(+): Erythromycin 15 μg + tetracycline 30 μg Gc(-): Water Gs: Aqueous and ethanolic extracts of Juglans regia bark [MIC was measured] | Aqueous and ethanolic extracts were found to be the most potent against S. sanguis and S. mutans, respectively. All strains of bacteria tested were significantly inhibited by the ethanolic extract. An antibacterial effect was not observed on S. mutans in the aqueous extract in comparison with the ethanolic extract. In comparison with the control, the aqueous extract significantly inhibited S. sanguis, S. salivarius, and S. aureus (p < 0.0001), In comparison with erythromycin, it did not affect S. mutans. The growth of oral bacteria was significantly inhibited by ethanolic and aqueous bark extracts of Juglans regia. | [290]/2013 | |
| Lippia sidoides | In vivo | Wistar rats with ligature-induced periodontitis | Gc(+): Diethylammonium diclofenac gel at 10 mg/g Gc(-): Saline gel Gs: Thymol gel [Histopathological analyses were performed] | Compared with a control of saline gel, Gs reduced histopathological lesions in gingival tissue and reduced myeloperoxidase activity (p < 0.05). | [309]/2016 |
| Manuka honey | In vitro In vivo | E. nodatum, S. mutans, C. rectus, S. sangiunis, A. a, P. gingivalis | In vitro section (G1: 0.2% CHX, G2: honey mouthwash, G3: saline) [MIC was measured] In vivo section: Plaque regrowth was simulated for four days. Four days after baseline, PI was measured | Among the six microorganisms tested, honey mouth rinses inhibited their growth effectively. All test species showed the lowest MICs with CHX rinses over honey and saline rinses. As a result of in vivo testing, CHX and honey rinses inhibited or reduced plaque formation. Testing showed honey to be antibacterial and antiplaque. | [310]/2012 |
| Myristica fragrans | In vitro | Ten tissue samples from patients with chronic periodontitis undergoing a flap surgery | Gc: Doxycycline Gs: Myristica fragrans [Zone of inhibition and antiprotease activity were measured] | Myristica fragrans, when added to the tissue sample, showed no zone of clearance compared to a significant zone of clearance of the tissue sample alone. Doxycycline demonstrated a small zone of clearance. Myristica fragrans possesses a better antiprotease activity as compared to doxycycline in vitro. | [311]/2016 |
| Myristica fragrans | In vitro | P. gingivalis | Gs: Myristica fragrans extract [Zone of inhibition was measured] | A 13.5 mm inhibitory zone was found in nutmeg extract. Myristica fragrans inhibited Porphyromonas gingivalis | [312]/2016 |
| In vitro | P. gingivalis | Gs: Isolated malabaricone C from nutmeg (Myristica fragrans) [MIC was measured] | Arg-gingipain was irreversibly inhibited by malabaricone C at 0.7 μg/mL, and P. gingivalis was selectively inhibited. | [313]/2014 | |
| Ocimum sanctum | In vitro | A. a, P. intermedia, P. gingivalis | Gc(+): Doxycycline Gc(-): Dimethyl formamide Gs: Ethanolic extract of Tulsi leaves (0.5%, 1%, 2%, 5%, and 10%) [Zone of inhibition was measured] | It was found that Tulsi extracts showed similar inhibition zones to doxycycline at concentrations of 5% and 10%, with similar antimicrobial activity against A. a (p > 0.05). However, P. gingivalis and P. intermedia resisted Tulsi extract, showing significantly smaller inhibition zones (p < 0.05). Due to its antimicrobial properties, Tulsi may be used as a complementary therapy to standard periodontal care. | [314]/2016 |
| In vivo | Wistar albino rats with ligature-induces periodontitis | G1: Control G2: Plain gel G3: 2% O. sanctum gel. [GI, PD, and morphometric analysis were performed] | Inhibition of edema by 2% Tulsi (O. sanctum) gel was 33.66% at 24 h. The GI and PD demonstrated statistical significance. No significant differences were found between the groups based on the morphometric analysis. Tulsi extract 2000 mg/kg was not found to have any toxic effects when administered orally. The O. sanctum gel was effective in treating experimental periodontitis. | [315]/2015 | |
| Pistacia atlantica Kurdica | In vitro In vivo | P. gingivalis Wistar rats | Gs: EO extracted from the gum of Pistacia atlantica Kurdica [MIC and MBC were measured; histological analyses were performed] | The experimental gel produced adequate wound healing and exhibited inhibitory and bactericidal activity against P. gingivalis. | [316]/2019 |
| Salvadora persica | In vitro | P. gingivalis and HSV-1 | Gs: Miswak raw extract [MIC, IC50, and MTT antiviral assays were measured] | An MIC of 62.5 μg/mL was determined against P. gingivalis. A therapeutic index of 11.3 μg/mL was observed against HSV-1. A concentration of 18.6 μg/mL was calculated as the IC50. A concentration of 210 μg/mL caused cytotoxicity in 50% of Vero cells. The SP films significantly inhibit P gingivalis and the HSV-1. | [317]/2020 |
| In vitro | S. mutans, S. mitis, Candida albicans, L. acidophilus, P. intermedia, and Peptostreptococcus | Gc(+): CHX Gc(-): Distilled water Gs: Aqueous and alcoholic extracts of SP (200 μg/mL and 400 μg/mL) [MIC was measured] | No significant results were obtained when Salvadora persica’s water extracts were tested, except for the minimum inhibitory effect against bacteria. Salvadora persica alcoholic extract exhibited relatively significant inhibitory effects. On all tested pathogens, alcoholic extract from SP showed antimicrobial activity. | [318]/2016 | |
| Satureja hortensis | In vitro | A. a, P. gingivalis, P. micra, T. forsythia, F. nucleatum, P. Intermedia, P. nigrescens | Gc: CHX Gs: Satureja hortensis EO [MIC and antibiofilm effects were measured] | All tested bacteria were inhibited by S. hortensis EO, despite its low MIC value. All strains of bacteria tested showed inhibition of proliferation at 0.125 µL/mL. In tests against periodontal bacteria, S. hortensis EO had limited antibiofilm activity (0.01 µL/mL), inhibiting only P. nigrescens biofilm formation. | [319]/2009 |
| Syzygium aromaticum | In vitro | A. a, F. nucleatum, and P. intermedia | G1: Hydro-ethanolic extracts G2: Delipidated hydro-ethanolic extracts G3: Fresh extract [MIC, MBC, and zone of inhibition were measured] | According to the MIC values, the tested organisms were antibacterial when tested at 6.25–25 mg/mL. On all bacteria subjected to the extract, the non-delipidated dry extract had a bactericidal effect. F. nucleatum was also shown to be bactericidal by delipidated extracts, as well as A. actinomycetemcomitans by fresh extracts. | [320]/2021 |
| In vitro | P. gingivalis | Gc(+): Tinidazole Gs: Syzygium aromaticum leaf essential oil (CLEO)-derived eugenol [MIC, MBC, CFU count, SEM, PI uptake, nucleic acid and protein leakage, biofilm quantification, and PCR were performed] | The amount of eugenol in CLEO, 90.84%, was found to have antibacterial activity against P. gingivalis at a concentration of 31.25 μM. The presence of eugenol at different concentrations inhibited the formation of biofilms and reduced the preformed ones of P. gingivalis. | [148]/2017 | |
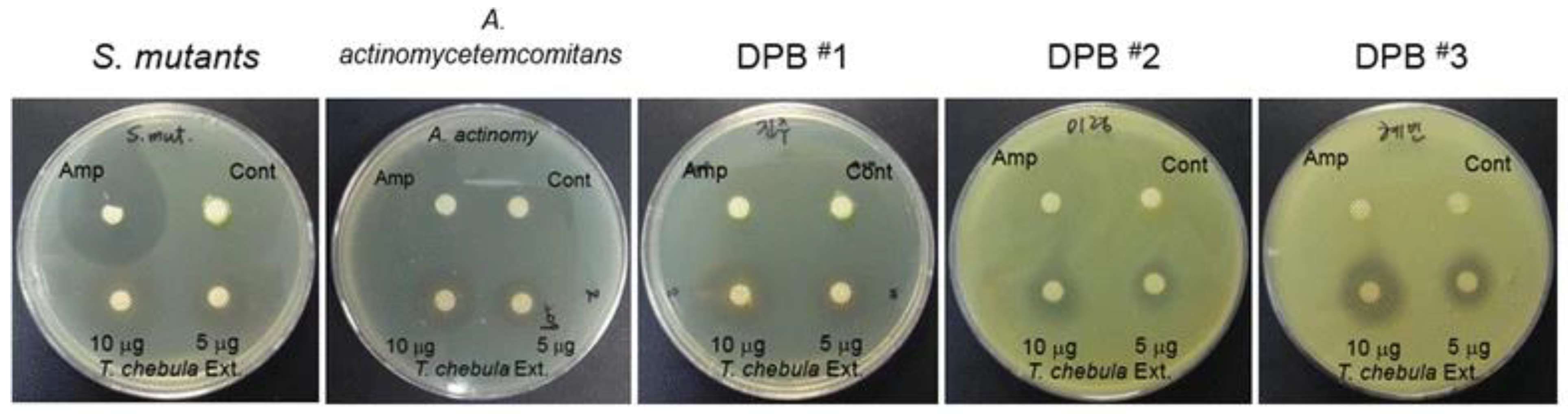
| Terminalia chebula | In vitro | S. mutans, A. a | Gc: Dimethyl sulfoxide (0.01%) Gs: Ethanol extract of Terminalia chebula (EETC) [MIC, susceptibility test, cytotoxicity assay, PGE2 assay, PCR, inflammation antibody array, protease array, ECM degradation, osteoclast formation, and pit formation were studied] | By inhibiting the growth of bacteria, EETC also inhibited the stimulation of PGE2, COX-2, and inflammatory cytokines. In the osteoblasts, EETC stimulated lipopolysaccharide derived from dental plaque to inhibit bone resorption and inhibit osteoclast formation. | [321]/2017 |
| Vaccinium macrocarpon | In vitro | P. gingivalis | Gc: Phosphate-buffered saline Gs: Cranberry juice concentrate prepared as a non-dialysable material [Growth, adherence properties, and biofilm formation of P. gingivalis were studied] | With cranberry concentrations exceeding 62.5 mg/mL, significant inhibition was observed (p < 0.05). With cranberry, P. gingivalis could not adhere effectively to collagen-, fibrinogen- or human serum-coated surfaces. Cranberry constituents may help prevent and treat periodontitis by preventing P. gingivalis from colonizing periodontal sites. | [322]/2006 |
| Vicia faba | In vitro | P. gingivalis | Gs: Vicia faba ethanolic and methanolic extracts [MIC, SI, and IC50 were measured] | Vicia faba exhibited low cytotoxicity and antibacterial activity. | [155]/2020 |
| Vitis vinifera | In vivo | Rats with ligature-induced periodontitis | G1: Laboratory diet G2: GSE for eight weeks G3: GSE for six weeks G4: GSE for two weeks [Histopathological studies were performed to determine ICN, CAL, OD, IL-10, and TGF-β] | GSE groups had lower ICN, higher CAL, and lower OD (p < 0.05). In the GSEs and GEs, IL-10 levels were higher (p < 0.05). In group B, periodontal ligament IL-10 levels were highest (p < 0.05). All groups had higher levels of TGF-ß in the gingival epithelium (p < 0.017). | [323]/2017 |
| Zingiber officinale | In vitro | P. gingivalis, P. endodontalis, P. intermedia | Gs: Ethanol and n-hexane extracts of ginger [MIC and MBC were measured] | The two alkylated gingerols, [10]-gingerol and [12]-gingerol, inhibited oral pathogen growth at MICs of 6–30 μg/mL. At an MBC range of 4–20 μg/mL, these ginger compounds also killed oral pathogens, but not 5-acetoxy-[6]-gingerol, galanolactone, or 3,5-diacetoxy-[6]-gingerdiol. | [324]/2008 |
4.22. Lippia sidoides
4.23. Mangifera indica (Mango)
4.24. Manuka Honey
4.25. Matricaria aurea and Matricaria chamomilla
4.26. Morus alba (M. alba)
4.27. Myristica fragrans (Nutmeg)
4.28. Ocimum sanctum (Tulsi)
4.29. Pinus pinaster
4.30. Piper marginatum and Ilex guayusa
4.31. Pistacia lentiscus (Mastic Gum)
4.32. Psidium guajava (Guava)
4.33. Punica granatum (Pomegranate)
4.34. Rosmarinus officinalis
4.35. Salvadora persica (Miswak)
4.36. Satureja hortensis (Summer Savory)
4.37. Syzygium aromaticum (Clove)
4.38. Terminalia chebula
4.39. Vaccinium macrocarpon
4.40. Vicia faba
4.41. Vitis vinifera
4.42. Zanthoxylum armatum
4.43. Zingiber officinale
5. Constraints
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Petersen, P.E.; Baehni, P.C. Periodontal health and global public health. Periodontology 2000 2012, 60, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Flemmig, T.F. Periodontitis. Ann. Periodontol. 1999, 4, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Dye, B.A.; Wei, L.; Thornton-Evans, G.O.; Genco, R.J. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J. Dent. Res. 2012, 91, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe periodontitis in 1990–2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Bartold, P.M.; Van Dyke, T.E. Van Dyke, Periodontitis: A host-mediated disruption of microbial homeostasis. Unlearning learned concepts. Periodontology 2000 2013, 62, 203–217. [Google Scholar] [CrossRef]
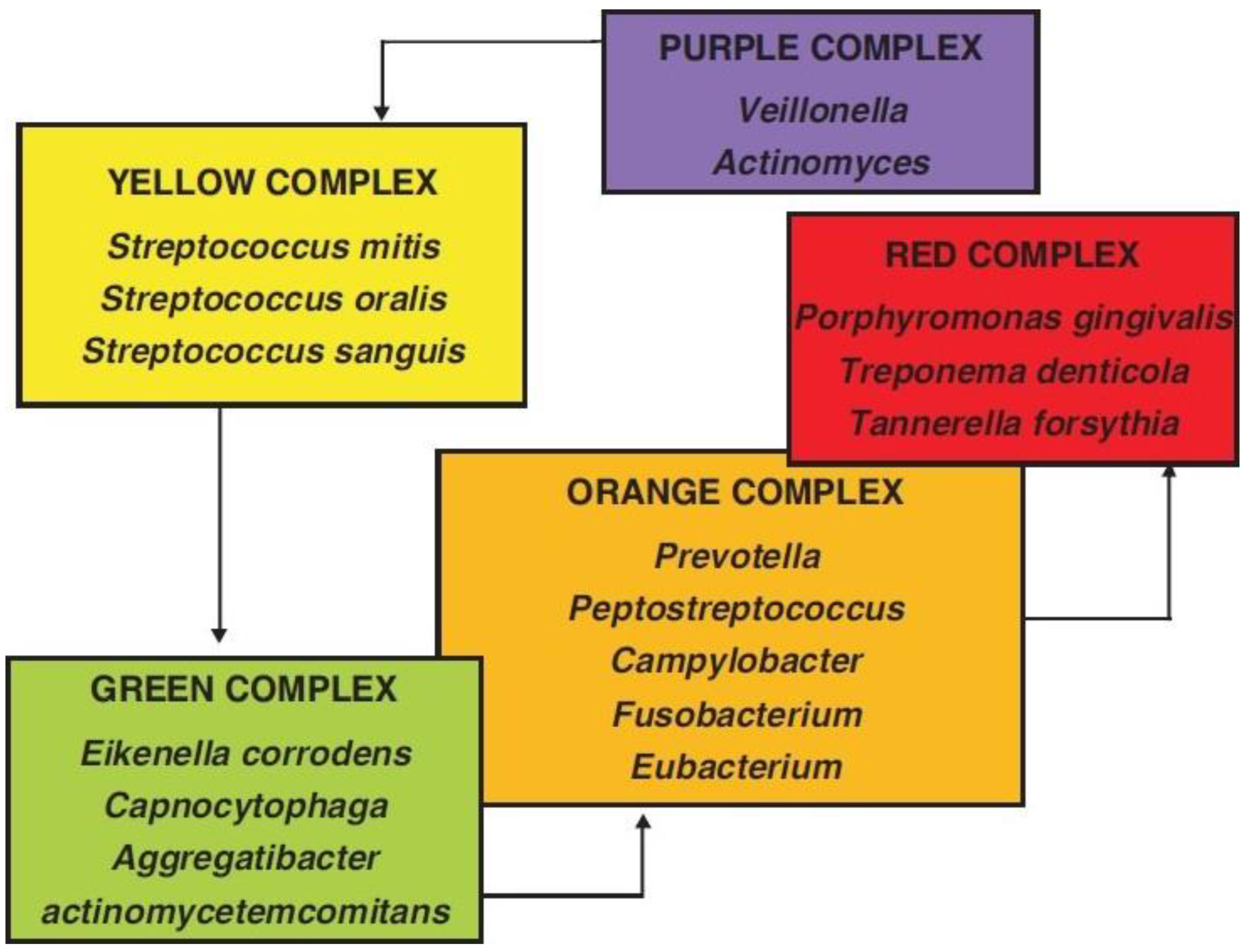
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Darveau, R.P. Periodontitis: A polymicrobial disruption of host homeostasis. Nat. Rev. Microbiol. 2010, 8, 481–490. [Google Scholar] [CrossRef]
- Boyd, R.L.; Leggott, P.; Quinn, R.; Buchanan, S.; Eakle, W.; Chambers, D. Effect of self-administered daily irrigation with 0.02% SnF2 on periodontal disease activity. J. Clin. Periodontol. 1985, 12, 420–431. [Google Scholar] [CrossRef]
- Listgarten, M.A.; Lindhe, J.; Hellden, L. Effect of tetracycline and/or scaling on human periodontal disease. Clinical, microbiological, and histological observations. J. Clin. Periodontol. 1978, 5, 246–271. [Google Scholar] [CrossRef]
- Slots, J. Subgingival microflora and periodontal disease. J. Clin. Periodontol. 1979, 6, 351–382. [Google Scholar] [CrossRef]
- Dzink, J.L.; Socransky, S.S.; Haffajee, A.D. The predominant cultivable microbiota of active and inactive lesions of destructive periodontal diseases. J. Clin. Periodontol. 1988, 15, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Wara-aswapati, N.; Pitiphat, W.; Chanchaimongkon, L.; Taweechaisupapong, S.; Boch, J.A.; Ishikawa, I. Red bacterial complex is associated with the severity of chronic periodontitis in a Thai population. Oral Dis. 2009, 15, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Newman, M.G.; Takei, H.; Klokkevold, P.R.; Carranza, F.A. Carranza’s Clinical Periodontology; Elsevier Health Sciences: London, UK, 2011. [Google Scholar]
- Chandki, R.; Banthia, P.; Banthia, R. Biofilms: A microbial home. J. Indian Soc. Periodontol. 2011, 15, 111–114. [Google Scholar] [PubMed]
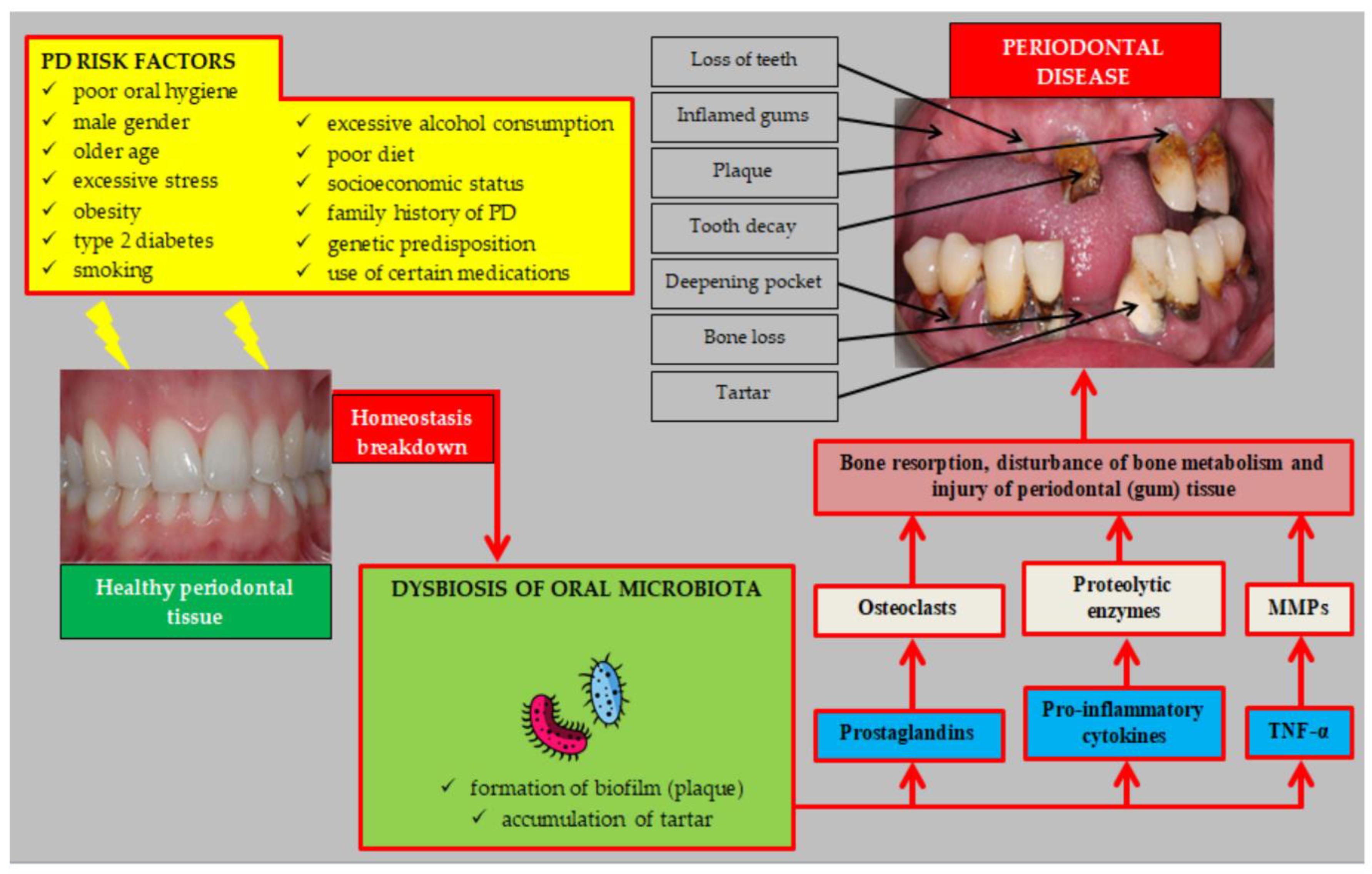
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontology 2000 2013, 62, 59–94. [Google Scholar] [PubMed]
- Lalla, E.; Papapanou, P.N. Diabetes mellitus and periodontitis: A tale of two common interrelated diseases. Nat. Rev. Endocrinol. 2011, 7, 738–748. [Google Scholar] [CrossRef]
- Kwon, T.; Lamster, I.B.; Levin, L. Current Concepts in the Management of Periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Czerniuk, M.R.; Surma, S.; Romańczyk, M.; Nowak, J.M.; Wojtowicz, A.; Filipiak, K.J. Unexpected Relationships: Periodontal Diseases: Atherosclerosis–Plaque Destabilization? From the Teeth to a Coronary Event. Biology 2022, 11, 272. [Google Scholar] [CrossRef]
- Spellberg, B.; Bartlett, J.G.; Gilbert, D.N. The future of antibiotics and resistance. N. Engl. J. Med. 2013, 368, 299–302. [Google Scholar] [CrossRef]
- Saquib, S.A.; AlQahtani, N.A.; Ahmad, I.; Kader, M.A.; Al Shahrani, S.S.; Asiri, E.A. Evaluation and Comparison of Antibacterial Efficacy of Herbal Extracts in Combination with Antibiotics on Periodontal pathobionts: An in vitro Microbiological Study. Antibiotics 2019, 8, 89. [Google Scholar] [CrossRef]
- Abdelmagyd, H.A.E.; Shetty, S.R.; Al-Ahmari, M.M.M. Herbal medicine as adjunct in periodontal therapies—A review of clinical trials in past decade. J. Oral Biol. Craniofac. Res. 2019, 9, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Fischer, R.G.; Lira, R., Jr.; Retamal-Valdes, B.; Figueiredo, L.C.; Malheiros, Z.; Stewart, B.; Feres, M. Periodontal disease and its impact on general health in Latin America. Section V: Treatment of periodontitis. Braz. Oral Res. 2020, 34 (Suppl. S1), e026. [Google Scholar] [CrossRef] [PubMed]
- Olsvik, B.; Tenover, F.C. Tetracycline resistance in periodontal pathogens. Clin. Infect. Dis. 1993, 16 (Suppl. S4), S310–S313. [Google Scholar] [CrossRef] [PubMed]
- Pajukanta, R. In vitro antimicrobial susceptibility of Porphyromonas gingivalis to azithromycin, a novel macrolide. Oral Microbiol. Immunol. 1993, 8, 325–326. [Google Scholar] [CrossRef] [PubMed]
- Slots, J. Selection of antimicrobial agents in periodontal therapy. J. Periodontal. Res. 2002, 37, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, G.G.; Locatelli, J.; Freitas, P.C.; Silva, G.L. Antibacterial activity of plant extracts and phytochemicals on antibiotic-resistant bacteria. Braz. J. Microbiol. 2000, 31, 247–256. [Google Scholar] [CrossRef]
- Rossiter, S.E.; Fletcher, M.H.; Wuest, W.M. Natural Products as Platforms to Overcome Antibiotic Resistance. Chem. Rev. 2017, 117, 12415–12474. [Google Scholar] [CrossRef]
- Pandita, V.; Patthi, B.; Singla, A.; Singh, S.; Malhi, R.; Vashishtha, V. Dentistry meets nature-role of herbs in periodontal care: A systematic review. J. Indian Assoc. Public Health Dent. 2014, 12, 148–156. [Google Scholar] [CrossRef]
- Kaur, A.; Kapoor, D.; Soni, N.; Gill, S. Phytodentistry—A boon. Arch. Dent. Med. Res. 2016, 2, 35–41. [Google Scholar]
- Anand, B. Herbal therapy in periodontics: A review. J. Res. Pharm. Sci. 2017, 3, 1–7. [Google Scholar]
- Khameneh, B.; Iranshahy, M.; Soheili, V.; Fazly Bazzaz, B.S. Review on plant antimicrobials: A mechanistic viewpoint. Antimicrob. Resist. Infect. Control 2019, 8, 118. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.N.; Zimmer, K.R.; Macedo, A.J.; Trentin, D.S. Plant Natural Products Targeting Bacterial Virulence Factors. Chem. Rev. 2016, 116, 9162–9236. [Google Scholar] [CrossRef] [PubMed]
- Gyllenhaal, C.; Kadushin, M.R.; Southavong, B.; Sydara, K.; Bouamanivong, S.; Xaiveu, M.; Xuan, L.T.; Hiep, N.T.; Hung, N.V.; Loc, P.K.; et al. Ethnobotanical approach versus random approach in the search for new bioactive compounds: Support of a hypothesis. Pharm. Biol. 2012, 50, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Cox, P.A.; Balick, M.J. The ethnobotanical approach to drug discovery. Sci. Am. 1994, 270, 82–87. [Google Scholar] [CrossRef]
- Barbieri, R.; Coppo, E.; Marchese, A.; Daglia, M.; Sobarzo-Sánchez, E.; Nabavi, S.F.; Nabavi, S.M. Phytochemicals for human disease: An update on plant-derived compounds antibacterial activity. Microbiol. Res. 2017, 196, 44–68. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, A.; Varghese, S.S.; Doraiswamy, J.N.; Malaiappan, S. Herbs as an antioxidant arsenal for periodontal diseases. J. Intercult. Ethnopharmacol. 2016, 5, 92–96. [Google Scholar] [CrossRef]
- Albandar, J.M.; Susin, C.; Hughes, F.J. Manifestations of systemic diseases and conditions that affect the periodontal attachment apparatus: Case definitions and diagnostic considerations. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S171–S189. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S162–S170. [Google Scholar] [CrossRef]
- José Luis, M.-C.; Viridiana Elizabeth, H.-R.; Oscar Eduardo, G.-H.; Francisca, C.-R.; María Isabel, C.-R.; Karla Mariana, C.-R.; Lizbeth, D.-A. Pathogenesis of Periodontal Disease, in Periodontal Disease; Nermin Mohammed Ahmed, Y., Ed.; IntechOpen: Rijeka, Croatia, 2019; Chapter 1. [Google Scholar]
- Hajishengallis, G.; Chavakis, T.; Lambris, J.D. Current understanding of periodontal disease pathogenesis and targets for host-modulation therapy. Periodontology 2000 2020, 84, 14–34. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Reis, E.S.; Mastellos, D.C.; Ricklin, D.; Lambris, J.D. Novel mechanisms and functions of complement. Nat. Immunol. 2017, 18, 1288–1298. [Google Scholar] [CrossRef]
- Tsukasaki, M. RANKL and osteoimmunology in periodontitis. J. Bone Miner. Metab. 2021, 39, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Belibasakis, G.N.; Bostanci, N. The RANKL-OPG system in clinical periodontology. J. Clin. Periodontol. 2012, 39, 239–248. [Google Scholar] [CrossRef] [PubMed]
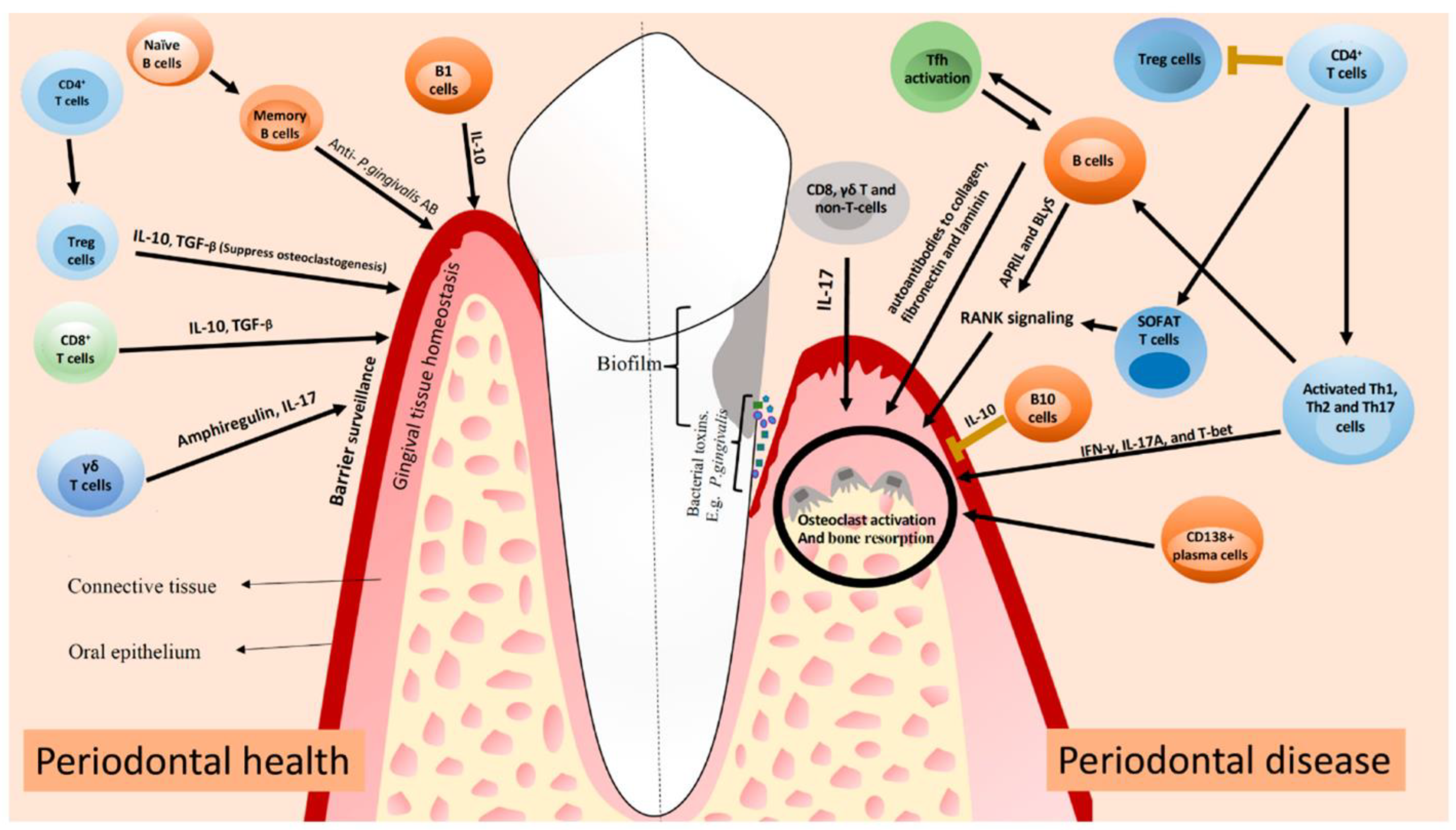
- Figueredo, C.; Lira, R., Jr.; Love, R. T and B Cells in Periodontal Disease: New Functions in A Complex Scenario. Int. J. Mol. Sci. 2019, 20, 3949. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N.; Chiang, N.; Van Dyke, T.E. Resolving inflammation: Dual anti-inflammatory and pro-resolution lipid mediators. Nat. Rev. Immunol. 2008, 8, 349–361. [Google Scholar] [CrossRef]
- Kourtzelis, I.; Mitroulis, I.; von Renesse, J.; Hajishengallis, G.; Chavakis, T. From leukocyte recruitment to resolution of inflammation: The cardinal role of integrins. J. Leukoc. Biol. 2017, 102, 677–683. [Google Scholar] [CrossRef]
- Gingivitis, P.I. Treatment of plaque-induced gingivitis, chronic periodontitis, and other clinical conditions. J. Periodontol. 2001, 72, 1790–1800. [Google Scholar]
- Walker, C.B. The acquisition of antibiotic resistance in the periodontal microflora. Periodontology 2000 1996, 10, 79–88. [Google Scholar] [CrossRef]
- Sanz, I.; Alonso, B.; Carasol, M.; Herrera, D.; Sanz, M. Nonsurgical treatment of periodontitis. J. Evid. Based Dent. Pract. 2012, 12 (Suppl. S3), 76–86. [Google Scholar] [CrossRef]
- Bonito, A.J.; Lux, L.; Lohr, K.N. Impact of local adjuncts to scaling and root planing in periodontal disease therapy: A systematic review. J. Periodontol. 2005, 76, 1227–1236. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Socransky, S.S. Introduction to microbial aspects of periodontal biofilm communities, development and treatment. Periodontology 2000 2006, 42, 7–12. [Google Scholar] [CrossRef]
- Chitme, H.R.; Chandra, M.; Kaushik, S. Studies on anti-diarrhoeal activity of Calotropis gigantea R. Br. in experimental animals. J. Pharm. Pharm. Sci. 2004, 7, 70–75. [Google Scholar] [PubMed]
- Kim, H.-S. Do not put too much value on conventional medicines. J. Ethnopharmacol. 2005, 100, 37–39. [Google Scholar] [CrossRef] [PubMed]
- Palombo, E.A. Traditional Medicinal Plant Extracts and Natural Products with Activity against Oral Bacteria: Potential Application in the Prevention and Treatment of Oral Diseases. Evid.-Based Complement. Altern. Med. 2011, 2011, 680354. [Google Scholar] [CrossRef] [PubMed]
- Singhal, R.; Agarwal, V.; Rastogi, P.; Khanna, R.; Tripathi, S. Efficacy of Acacia arabica gum as an adjunct to scaling and root planing in the treatment of chronic periodontitis: A randomized controlled clinical trial. Saudi Dent. J. 2018, 30, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Kirtikar, K.; Basu, B. Indian medicinal plan Leader road. Allahabad India 1984, 2, 1347–1348. [Google Scholar]
- Clark, D.; Gazi, M.; Cox, S.; Eley, B.; Tinsley, G. The effects of Acacia arabica gum on the in vitro growth and protease activities of periodontopathic bacteria. J. Clin. Periodontol. 1993, 20, 238–243. [Google Scholar] [CrossRef]
- Pradeep, A.; Agarwal, E.; Bajaj, P.; Naik, S.; Shanbhag, N.; Uma, S. Clinical and microbiologic effects of commercially available gel and powder containing Acacia arabica on gingivitis. Aust. Dent. J. 2012, 57, 312–318. [Google Scholar] [CrossRef]
- Pradeep, A.; Happy, D.; Garg, G. Short-term clinical effects of commercially available gel containing Acacia arabica: A randomized controlled clinical trial. Aust. Dent. J. 2010, 55, 65–69. [Google Scholar] [CrossRef]
- Mnisi, C.M.; Mlambo, V. Influence of harvesting site on chemical composition and potential protein value of Acacia erioloba, A. nilotica and Ziziphus mucronata leaves for ruminants. J. Anim. Physiol. Anim. Nutr. 2017, 101, 994–1003. [Google Scholar] [CrossRef]
- Kaur, K.; Michael, H.; Arora, S.; Härkönen, P.; Kumar, S. In vitro bioactivity-guided fractionation and characterization of polyphenolic inhibitory fractions from Acacia nilotica (L.) Willd. ex Del. J. Ethnopharmacol. 2005, 99, 353–360. [Google Scholar] [CrossRef]
- Singh, R.; Singh, B.; Singh, S.; Kumar, N.; Kumar, S.; Arora, S. Anti-free radical activities of kaempferol isolated from Acacia nilotica (L.) Willd. Ex. Del. Toxicol. In Vitro 2008, 22, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Al-Nour, M.Y.; Ibrahim, M.M.; Elsaman, T. Ellagic acid, Kaempferol, and Quercetin from Acacia nilotica: Promising combined drug with multiple mechanisms of action. Curr. Pharmacol. Rep. 2019, 5, 255–280. [Google Scholar] [CrossRef] [PubMed]
- Hussein, G.; Miyashiro, H.; Nakamura, N.; Hattori, M.; Kawahata, T.; Otake, T.; Kakiuchi, N.; Shimotohno, K. Inhibitory effects of Sudanese plant extracts on HIV-1 replication and HIV-1 protease. Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 1999, 13, 31–36. [Google Scholar] [CrossRef]
- Abd El Nabi, O.M.; Reisinger, E.C.; Reinthaler, F.F.; Still, F.; Eibel, U.; Krejs, G.J. Antimicrobial activity of Acacia nilotica (L.) Willd. ex Del. var. nilotica (Mimosaceae). J. Ethnopharmacol. 1992, 37, 77–79. [Google Scholar] [CrossRef]
- Maldini, M.; Montoro, P.; Hamed, A.I.; Mahalel, U.A.; Oleszek, W.; Stochmal, A.; Piacente, S. Strong antioxidant phenolics from Acacia nilotica: Profiling by ESI-MS and qualitative–quantitative determination by LC–ESI-MS. J. Pharm. Biomed. Anal. 2011, 56, 228–239. [Google Scholar] [CrossRef]
- Dafallah, A.A.; Al-Mustafa, Z. Investigation of the anti-inflammatory activity of Acacia nilotica and Hibiscus sabdariffa. Am. J. Chin. Med. 1996, 24, 263–269. [Google Scholar] [CrossRef]
- Muddathir, A.M.; Mohieldin, E.A.M.; Mitsunaga, T. In vitro activities of Acacia nilotica (L.) Delile bark fractions against Oral Bacteria, Glucosyltransferase and as antioxidant. BMC Complement. Med. Ther. 2020, 20, 360. [Google Scholar] [CrossRef]
- Block, E. The chemistry of garlic and onions. Sci. Am. 1985, 252, 114–119. [Google Scholar] [CrossRef]
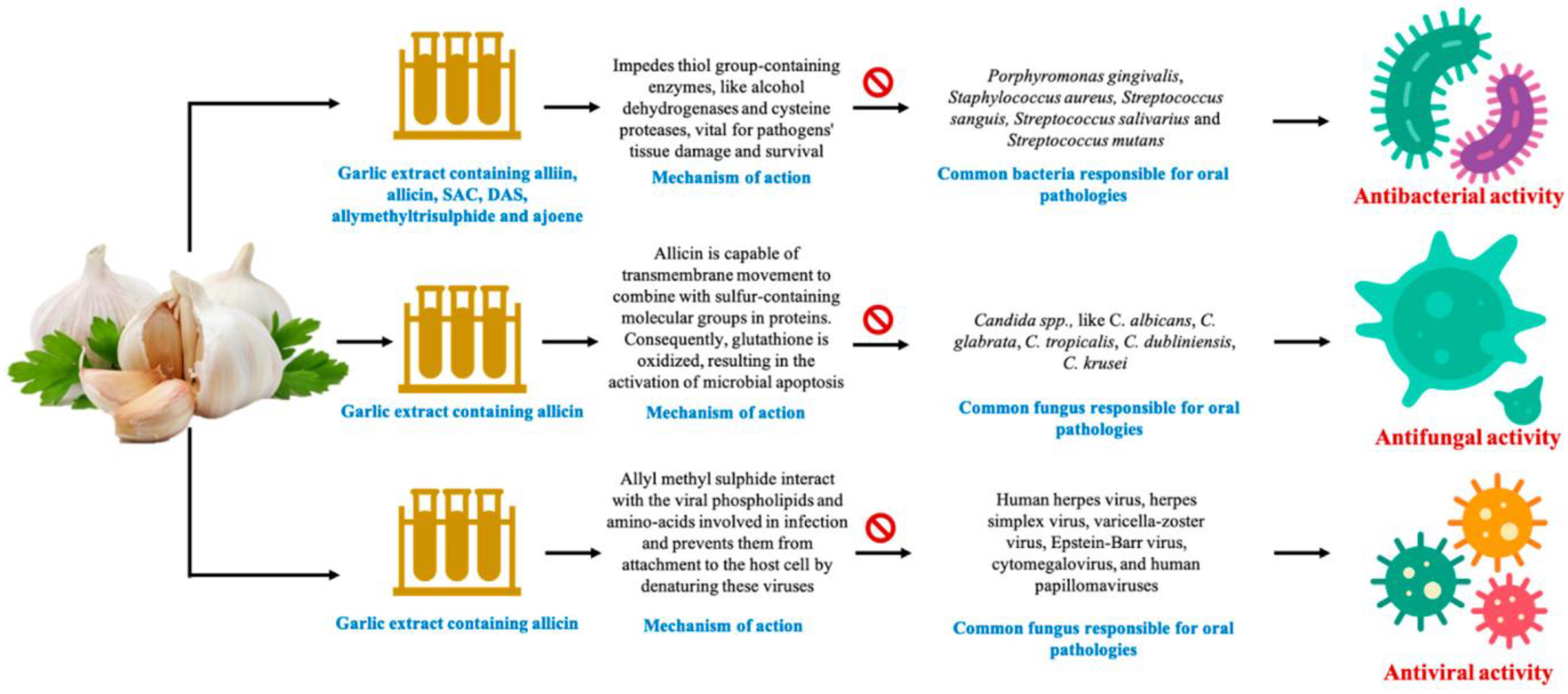
- Ankri, S.; Mirelman, D. Antimicrobial properties of allicin from garlic. Microbes Infect. 1999, 1, 125–129. [Google Scholar] [CrossRef]
- Ceccanti, C.; Rocchetti, G.; Lucini, L.; Giuberti, G.; Landi, M.; Biagiotti, S.; Guidi, L. Comparative phytochemical profile of the elephant garlic (Allium ampeloprasum var. holmense) and the common garlic (Allium sativum) from the Val di Chiana area (Tuscany, Italy) before and after in vitro gastrointestinal digestion. Food Chem. 2021, 338, 128011. [Google Scholar] [CrossRef]
- Harini, K.; Babu, S.; Ajila, V.; Hegde, S. Garlic: It’s role in oral and systemic health. Nitte Univ. J. Health Sci. 2013, 3, 17–22. [Google Scholar]
- Fenwick, G.R.; Hanley, A.B. The genus Allium—Part 1. Crit. Rev. Food Sci. Nutr. 1985, 22, 199–271. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.; Bernstein, Y.; Findler, M. Periodontal disease and its prevention, by traditional and new avenues (Review). Exp. Ther. Med. 2020, 19, 1504–1506. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.-W.; Chen, H.-W.; Sheen, L.-Y.; Lii, C.-K. Garlic: Health benefits and actions. BioMedicine 2012, 2, 17–29. [Google Scholar] [CrossRef]
- Ahmad, T.A.; El-Sayed, B.A.; El-Sayed, L.H. Development of immunization trials against Eimeria spp. Trials Vaccinol. 2016, 5, 38–47. [Google Scholar] [CrossRef]
- Sasi, M.; Kumar, S.; Kumar, M.; Thapa, S.; Prajapati, U.; Tak, Y.; Changan, S.; Saurabh, V.; Kumari, S.; Kumar, A.; et al. Garlic (Allium sativum L.) Bioactives and Its Role in Alleviating Oral Pathologies. Antioxidants 2021, 10, 1847. [Google Scholar] [CrossRef]
- Zini, A.; Mann, J.; Mazor, S.; Vered, Y. The Efficacy of Aged Garlic Extract on Gingivitis—A Randomized Clinical Trial. J. Clin. Dent. 2018, 29, 52–56. [Google Scholar]
- Bin, C.; Al-Dhabi, N.A.; Esmail, G.A.; Arokiyaraj, S.; Arasu, M.V. Potential effect of Allium sativum bulb for the treatment of biofilm forming clinical pathogens recovered from periodontal and dental caries. Saudi J. Biol. Sci. 2020, 27, 1428–1434. [Google Scholar] [CrossRef]
- Muniz, I.A.F.; Campos, D.E.S.; Shinkai, R.S.A.; Trindade, T.G.D.; Cosme-Trindade, D.C. Case report of oral mucosa garlic burn during COVID-19 pandemic outbreak and role of teledentistry to manage oral health in an older adult woman. Spec. Care Dent. 2021, 41, 639–643. [Google Scholar] [CrossRef]
- Ohtani, M.; Nishimura, T. The preventive and therapeutic application of garlic and other plant ingredients in the treatment of periodontal diseases. Exp. Ther. Med. 2020, 19, 1507–1510. [Google Scholar]
- Zini, A.; Mann, J.; Mazor, S.; Vered, Y. Beneficial effect of aged garlic extract on periodontitis: A randomized controlled double-blind clinical study. J. Clin. Biochem. Nutr. 2020, 67, 297–301. [Google Scholar] [PubMed]
- Shetty, S.; Thomas, B.; Shetty, V.; Bhandary, R.; Shetty, R.M. An in-vitro evaluation of the efficacy of garlic extract as an antimicrobial agent on periodontal pathogens: A microbiological study. Ayu 2013, 34, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Bhat, G.; Kudva, P.; Dodwad, V. Aloe vera: Nature’s soothing healer to periodontal disease. J. Indian Soc. Periodontol. 2011, 15, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.W.; Son, B.W.; Son, Y.S.; Park, Y.I.; Lee, S.K.; Chung, M.H. The wound-healing effect of a glycoprotein fraction isolated from aloe vera. Br. J. Dermatol. 2001, 145, 535–545. [Google Scholar] [CrossRef]
- Reynolds, T.; Dweck, A. Aloe vera leaf gel: A review update. J. Ethnopharmacol. 1999, 68, 3–37. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, K. Aloe Vera Heals: The Scientific Facts; Cancer Book House: Sydney, Australia, 1980. [Google Scholar]
- Budavari, S.; O’Neil, M.J.; Smith, A.; Heckelman, P.E. The Merck Index; Merck & Co., Inc.: Merck Rahway, NJ, USA, 1989; Volume 11. [Google Scholar]
- Vogler, B.K.; Ernst, E. Aloe vera: A systematic review of its clinical effectiveness. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 1999, 49, 823–828. [Google Scholar]
- Heggers, J.; Pineless, G.; Robson, M. Dermaide aloe aloe vera gel-comparison of the anti-microbial effects. J. Am. Med. Technol. 1979, 41, 293–294. [Google Scholar]
- Schleifer, K.H.; Kilpper-Bälz, R. Transfer of Streptococcus faecalis and Streptococcus faecium to the Genus Enterococcus nom. rev. as Enterococcus faecalis comb. nov. and Enterococcus faecium comb. nov. Int. J. Syst. Evol. Microbiol. 1984, 34, 31–34. [Google Scholar] [CrossRef]
- Grindlay, D.; Reynolds, T. The Aloe vera phenomenon: A review of the properties and modern uses of the leaf parenchyma gel. J. Ethnopharmacol. 1986, 16, 117–151. [Google Scholar] [CrossRef]
- Saoo, K.; Miki, H.; Ohmori, M.; Winters, W. Antiviral activity of aloe extracts against cytomegalovirus. Phytother. Res. 1996, 10, 348–350. [Google Scholar] [CrossRef]
- Hutter, J.A.; Salman, M.; Stavinoha, W.B.; Satsangi, N.; Williams, R.F.; Streeper, R.T.; Weintraub, S.T. Antiinflammatory C-glucosyl chromone from Aloe barbadensis. J. Nat. Prod. 1996, 59, 541–543. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Teradaira, R.; Beppu, H.; Obata, M.; Nagatsu, T.; Fujita, K. Properties and pharmacological activity of carboxypeptidase in Aloe arborescens Mill var. natalensis Berger. Phytother. Res. 1993, 7, S26–S29. [Google Scholar] [CrossRef]
- Tello, C.G.; Ford, P.; Iacopino, A. In vitro evaluation of complex carbohydrate denture adhesive formulations. Quintessence Int. 1998, 29, 585–593. [Google Scholar] [PubMed]
- Poor, M.R.; Hall, J.E.; Poor, A.S. Reduction in the incidence of alveolar osteitis in patients treated with the SaliCept patch, containing Acemannan hydrogel. J. Oral Maxillofac. Surg. 2002, 60, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Sudworth, R. The Use of Aloe Vera in Dentistry; Positive Health Publications Ltd.: Philadelphia, PA, USA, 2002. [Google Scholar]
- Chandrahas, B.; Jayakumar, A.; Naveen, A.; Butchibabu, K.; Reddy, P.K.; Muralikrishna, T. A randomized, double-blind clinical study to assess the antiplaque and antigingivitis efficacy of Aloe vera mouth rinse. J. Indian Soc. Periodontol. 2012, 16, 543. [Google Scholar]
- Namiranian, H.; Serino, G. The effect of a toothpaste containing aloe vera on established gingivitis. Swed. Dent. J. 2012, 36, 179–185. [Google Scholar]
- Tornero-Martínez, A.; Cruz-Ortiz, R.; Jaramillo-Flores, M.E.; Osorio-Díaz, P.; Ávila-Reyes, S.V.; Alvarado-Jasso, G.M.; Mora-Escobedo, R. In vitro Fermentation of Polysaccharides from Aloe vera and the Evaluation of Antioxidant Activity and Production of Short Chain Fatty Acids. Molecules 2019, 24, 3605. [Google Scholar] [CrossRef]
- Ajmera, N.; Chatterjee, A.; Goyal, V. Aloe vera: It’s effect on gingivitis. J. Indian Soc. Periodontol. 2013, 17, 435–438. [Google Scholar] [CrossRef]
- Cronquist, A.; Takhtadzhian, A.L. An Integrated System of Classification of Flowering Plants; Columbia University Press: New York City, NY, USA, 1981. [Google Scholar]
- Rivero-Cruz, B.E.; Esturau, N.; Sánchez-Nieto, S.; Romero, I.; Castillo-Juárez, I.; Rivero-Cruz, J.F. Isolation of the new anacardic acid 6-[16’Z-nonadecenyl]-salicylic acid and evaluation of its antimicrobial activity against Streptococcus mutans and Porphyromonas gingivalis. Nat. Prod. Res. 2011, 25, 1282–1287. [Google Scholar] [CrossRef]
- Sung, B.; Pandey, M.K.; Ahn, K.S.; Yi, T.; Chaturvedi, M.M.; Liu, M.; Aggarwal, B.B. Anacardic acid (6-nonadecyl salicylic acid), an inhibitor of histone acetyltransferase, suppresses expression of nuclear factor-kappaB-regulated gene products involved in cell survival, proliferation, invasion, and inflammation through inhibition of the inhibitory subunit of nuclear factor-kappaBalpha kinase, leading to potentiation of apoptosis. Blood 2008, 111, 4880–4891. [Google Scholar]
- Wu, Y.; He, L.; Zhang, L.; Chen, J.; Yi, Z.; Zhang, J.; Liu, M.; Pang, X. Anacardic acid (6-pentadecylsalicylic acid) inhibits tumor angiogenesis by targeting Src/FAK/Rho GTPases signaling pathway. J. Pharmacol. Exp. Ther. 2011, 339, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Robles-Zepeda, R.E.; Velázquez-Contreras, C.A.; Garibay-Escobar, A.; Gálvez-Ruiz, J.C.; Ruiz-Bustos, E. Antimicrobial activity of Northwestern Mexican plants against Helicobacter pylori. J. Med. Food. 2011, 14, 1280–1283. [Google Scholar] [CrossRef]
- Mandal, A.; Manohar, B.; Shetty, N.; Mathur, A.; Makhijani, B.; Sen, N. A Comparative Evaluation of Anti-Inflammatory and Antiplaque Efficacy of Citrus Sinesis Mouthwash and Chlorhexidine Mouthwash. J. Nepal. Soc. Periodontol. Oral Implantol. 2018, 2, 9–13. [Google Scholar] [CrossRef]
- Brahmachari, G. Neem—An omnipotent plant: A retrospection. Chembiochem 2004, 5, 408–421. [Google Scholar] [CrossRef]
- Prakash, D.; Suri, S.; Upadhyay, G.; Singh, B.N. Total phenol, antioxidant and free radical scavenging activities of some medicinal plants. Int. J. Food Sci. Nutr. 2007, 58, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Sakagami, H.; Oi, T.; Satoh, K. Prevention of oral diseases by polyphenols. In Vivo 1999, 13, 155–171. [Google Scholar] [PubMed]
- Alzoreky, N.; Nakahara, K. Antibacterial activity of extracts from some edible plants commonly consumed in Asia. Int. J. Food Microbiol. 2003, 80, 223–230. [Google Scholar] [CrossRef]
- SaiRam, M.; Ilavazhagan, G.; Sharma, S.; Dhanraj, S.; Suresh, B.; Parida, M.; Jana, A.; Devendra, K.; Selvamurthy, W. Anti-microbial activity of a new vaginal contraceptive NIM-76 from neem oil (Azadirachta indica). J. Ethnopharmacol. 2000, 71, 377–382. [Google Scholar] [CrossRef]
- Wolinsky, L.; Mania, S.; Nachnani, S.; Ling, S. The inhibiting effect of aqueous Azadirachta indica (Neem) extract upon bacterial properties influencing in vitro plaque formation. J. Dent. Res. 1996, 75, 816–822. [Google Scholar] [CrossRef]
- Vanka, A.; Tandon, S.; Rao, S.; Udupa, N.; Ramkumar, P. The effect of indigenous Neem Azadirachta indica [correction of (Adirachta indica)] mouth wash on Streptococcus mutans and lactobacilli growth. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2001, 12, 133–144. [Google Scholar]
- Dasgupta, T.; Banerjee, S.; Yadava, P.; Rao, A. Chemopreventive potential of Azadirachta indica (Neem) leaf extract in murine carcinogenesis model systems. J. Ethnopharmacol. 2004, 92, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Baral, R.; Chattopadhyay, U. Neem (Azadirachta indica) leaf mediated immune activation causes prophylactic growth inhibition of murine Ehrlich carcinoma and B16 melanoma. Int. Immunopharmacol. 2004, 4, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Raji, Y.; Ogunwande, I.A.; Osadebe, C.A.; John, G. Effects of Azadirachta indica extract on gastric ulceration and acid secretion in rats. J. Ethnopharmacol. 2004, 90, 167–170. [Google Scholar] [CrossRef]
- Bandyopadhyay, U.; Biswas, K.; Sengupta, A.; Moitra, P.; Dutta, P.; Sarkar, D.; Debnath, P.; Ganguly, C.K.; Banerjee, R.K. Clinical studies on the effect of Neem (Azadirachta indica) bark extract on gastric secretion and gastroduodenal ulcer. Life Sci. 2004, 75, 2867–2878. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.D.; Darout, I.A.; Skaug, N. Chewing sticks: Timeless natural toothbrushes for oral cleansing. J. Periodontal Res. 2001, 36, 275–284. [Google Scholar] [CrossRef]
- Prashant, G.; Chandu, G.; Murulikrishna, K.; Shafiulla, M. The effect of mango and neem extract on four organisms causing dental caries: Streptococcus mutans, Streptococcus salivavius, Streptococcus mitis, and Streptococcus sanguis: An in vitro study. Indian J. Dent. Res. 2007, 18, 148. [Google Scholar]
- Robinson, T. The Organic Constituents of Higher Plants, Diterjemahkan Oleh Padmawinata; Kosasih, P., Ed.; ITB: Bandung, Indonesia, 1995. [Google Scholar]
- Pai, M.R.; Acharya, L.D.; Udupa, N. Evaluation of antiplaque activity of Azadirachta indica leaf extract gel—A 6-week clinical study. J. Ethnopharmacol. 2004, 90, 99–103. [Google Scholar] [CrossRef]
- Schumacher, M.; Cerella, C.; Reuter, S.; Dicato, M.; Diederich, M. Anti-inflammatory, pro-apoptotic, and anti-proliferative effects of a methanolic neem (Azadirachta indica) leaf extract are mediated via modulation of the nuclear factor-κB pathway. Genes Nutr. 2011, 6, 149–160. [Google Scholar] [CrossRef]
- Hu, J.P.; Takahashi, N.; Yamada, T. Coptidis rhizoma inhibits growth and proteases of oral bacteria. Oral Dis. 2000, 6, 297–302. [Google Scholar] [CrossRef]
- Lamont, R.J.; Jenkinson, H.F. Life below the gum line: Pathogenic mechanisms of Porphyromonas gingivalis. Microbiol. Mol. Biol. Rev. 1998, 62, 1244–1263. [Google Scholar] [CrossRef]
- Pandit, N.; Changela, R.; Bali, D.; Tikoo, P.; Gugnani, S. Porphyromonas gingivalis: Its virulence and vaccine. J. Int. Clin. Dent. Res. Organ. 2015, 7, 51. [Google Scholar]
- Moeintaghavi, A.; Shabzendedar, M.; Parissay, I.; Makarem, A.; Orafaei, H.; Hosseinnezhad, M. Berberine gel in periodontal inflammation: Clinical and histological effects. J. Adv. Periodontol. Implant. Dent. 2012, 4, 7–11. [Google Scholar]
- Strusovskaya, A.; Poroysky, S.; Smirnov, A.; Firsova, I.; Sirotenko, V.; Kirichenko, L.; Strusovskaya, O. A study of the influence of barbaris root (Berberis vulgaris L., Berberidaceae) extract dental gel on the dynamics of the inflammatory process in periodontal tissues of rats on the model of induced gingivitis. In Proceedings of the AIP Conference Proceedings, Yekaterinburg, Russia, 13–16 November 2019. [Google Scholar]
- Passos, V.F.; Melo, M.A.S.d.; Lima, J.P.M.; Marçal, F.F.; Costa, C.A.G.d.A.; Rodrigues, L.K.A.; Santiago, S.L. Active compounds and derivatives of camellia sinensis responding to erosive attacks on dentin. Braz. Oral Res. 2018, 32, e40. [Google Scholar] [CrossRef] [PubMed]
- Kushiyama, M.; Shimazaki, Y.; Murakami, M.; Yamashita, Y. Relationship between intake of green tea and periodontal disease. J. Periodontol. 2009, 80, 372–377. [Google Scholar] [CrossRef]
- Koyama, Y.; Kuriyama, S.; Aida, J.; Sone, T.; Nakaya, N.; Ohmori-Matsuda, K.; Hozawa, A.; Tsuji, I. Association between green tea consumption and tooth loss: Cross-sectional results from the Ohsaki Cohort 2006 Study. Prev. Med. 2010, 50, 173–179. [Google Scholar] [CrossRef]
- Ide, R.; Fujino, Y.; Hoshiyama, Y.; Mizoue, T.; Kubo, T.; Pham, T.-M.; Shirane, K.; Tokui, N.; Sakata, K.; Tamakoshi, A. A prospective study of green tea consumption and oral cancer incidence in Japan. Ann. Epidemiol. 2007, 17, 821–826. [Google Scholar] [CrossRef]
- Mazur, M.; Ndokaj, A.; Jedlinski, M.; Ardan, R.; Bietolini, S.; Ottolenghi, L. Impact of Green Tea (Camellia Sinensis) on periodontitis and caries. Systematic review and meta-analysis. Jpn. Dent. Sci. Rev. 2021, 57, 1–11. [Google Scholar] [CrossRef]
- Wazaify, M.; Afifi, F.U.; El-Khateeb, M.; Ajlouni, K. Complementary and alternative medicine use among Jordanian patients with diabetes. Complement. Ther. Clin. Pract. 2011, 17, 71–75. [Google Scholar] [CrossRef]
- Yanakiev, S. Effects of Cinnamon (Cinnamomum spp.) in Dentistry: A Review. Molecules 2020, 25, 4184. [Google Scholar] [CrossRef]
- Kawatra, P.; Rajagopalan, R. Cinnamon: Mystic powers of a minute ingredient. Pharmacogn. Res. 2015, 7 (Suppl. S1), S1–S6. [Google Scholar] [CrossRef]
- Jayaprakasha, G.K.; Rao, L.J. Chemistry, biogenesis, and biological activities of Cinnamomum zeylanicum. Crit. Rev. Food Sci. Nutr. 2011, 51, 547–562. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Sun, J.; Ford, P. Differentiation of the four major species of cinnamons (C. burmannii, C. verum, C. cassia, and C. loureiroi) using a flow injection mass spectrometric (FIMS) fingerprinting method. J. Agric. Food Chem. 2014, 62, 2516–2521. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.L.; Walters, K.S.; Drake, D.R.; Dawson, D.V.; Blanchette, D.R.; Brogden, K.A.; Wertz, P.W. Oral mucosal lipids are antibacterial against Porphyromonas gingivalis, induce ultrastructural damage, and alter bacterial lipid and protein compositions. Int. J. Oral Sci. 2013, 5, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Mendes, S.J.F.; Sousa, F.I.A.B.; Pereira, D.M.S.; Ferro, T.A.F.; Pereira, I.C.P.; Silva, B.L.R.; Pinheiro, A.J.M.C.R.; Mouchrek, A.Q.S.; Monteiro-Neto, V.; Costa, S.K.P.; et al. Cinnamaldehyde modulates LPS-induced systemic inflammatory response syndrome through TRPA1-dependent and independent mechanisms. Int. Immunopharmacol. 2016, 34, 60–70. [Google Scholar] [CrossRef]
- Yang, X.Q.; Zheng, H.; Ye, Q.; Li, R.Y.; Chen, Y. Essential oil of Cinnamon exerts anti-cancer activity against head and neck squamous cell carcinoma via attenuating epidermal growth factor receptor—Tyrosine kinase. J. Buon 2015, 20, 1518–1525. [Google Scholar]
- Wang, Y.; Zhang, Y.; Shi, Y.Q.; Pan, X.H.; Lu, Y.H.; Cao, P. Antibacterial effects of cinnamon (Cinnamomum zeylanicum) bark essential oil on Porphyromonas gingivalis. Microb. Pathog. 2018, 116, 26–32. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, X.; Wang, Y.; Jiang, P.; Quek, S. Antibacterial activity and mechanism of cinnamon essential oil against Escherichia coli and Staphylococcus aureus. Food Control 2016, 59, 282–289. [Google Scholar] [CrossRef]
- Meng, X.; Li, D.; Zhou, D.; Wang, D.; Liu, Q.; Fan, S. Chemical composition, antibacterial activity and related mechanism of the essential oil from the leaves of Juniperus rigida Sieb. et Zucc against Klebsiella pneumoniae. J. Ethnopharmacol. 2016, 194, 698–705. [Google Scholar] [CrossRef]
- Chaieb, K.; Hajlaoui, H.; Zmantar, T.; Kahla-Nakbi, A.B.; Rouabhia, M.; Mahdouani, K.; Bakhrouf, A. The chemical composition and biological activity of clove essential oil, Eugenia caryophyllata (Syzigium aromaticum L. Myrtaceae): A short review. Phytother. Res. 2007, 21, 501–506. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Y.; Zhu, X.; Cao, P.; Wei, S.; Lu, Y. Antibacterial and antibiofilm activities of eugenol from essential oil of Syzygium aromaticum (L.) Merr. & L. M. Perry (clove) leaf against periodontal pathogen Porphyromonas gingivalis. Microb. Pathog. 2017, 113, 396–402. [Google Scholar]
- Bickers, D.; Calow, P.; Greim, H.; Hanifin, J.M.; Rogers, A.E.; Saurat, J.H.; Sipes, I.G.; Smith, R.L.; Tagami, H. A toxicologic and dermatologic assessment of cinnamyl alcohol, cinnamaldehyde and cinnamic acid when used as fragrance ingredients. Food Chem. Toxicol. 2005, 43, 799–836. [Google Scholar] [CrossRef] [PubMed]
- Cocchiara, J.; Letizia, C.S.; Lalko, J.; Lapczynski, A.; Api, A.M. Fragrance material review on cinnamaldehyde. Food Chem. Toxicol. 2005, 43, 867–923. [Google Scholar] [CrossRef] [PubMed]
- Hussain, K.A.; Tarakji, B.; Kandy, B.P.; John, J.; Mathews, J.; Ramphul, V.; Divakar, D.D. Antimicrobial effects of citrus sinensis peel extracts against periodontopathic bacteria: An in vitro study. Rocz. Panstw. Zakl. Hig. 2015, 66, 173–178. [Google Scholar] [PubMed]
- Lawal, D.; Bala, J.A.; Aliyu, S.Y.; Huguma, M.A. Phytochemical Screening and In Vitro Anti-Bacterial Studies of the Ethanolic Extract of Citrus Senensis (Linn.) Peel against some Clinical Bacterial Isolates. Int. J. Innov. Appl. Stud. 2013, 2, 138–145. [Google Scholar]
- Dubey, D.; Balamurugan, K.; Agrawal, R.; Verma, R.K.; Jain, R. Evalution of Antibacterial and Antioxidant Activity of Methanolic and Hydromethanolic Extract of Sweet Orange Peels. Recent Res. Sci. Technol. 2011, 3, 22–25. [Google Scholar]
- Jabuk, S.; Chabuck, A.; Adil, N.; Chabuck, G. In vitro and in vivo effect of three aqueous plant extract on pathogenicity of Klebsiella pneumonia isolated from patient with urinary tract infection. World J. Pharm. Res. 2014, 5, 160–179. [Google Scholar]
- Carrol, D.H.; Chassagne, F.; Dettweiler, M.; Quave, C.L. Antibacterial activity of plant species used for oral health against Porphyromonas gingivalis. PLoS ONE 2020, 15, e0239316. [Google Scholar] [CrossRef]
- Tangade, P.S.; Mathur, A.; Tirth, A.; Kabasi, S. Anti-gingivitis effects of Acacia arabica-containing toothpaste. Chin. J. Dent. Res. Off. J. Sci. Sect. Chin. Stomatol. Assoc. 2012, 15, 49–53. [Google Scholar]
- Sayar, F.; Farahmand, A.H.; Rezazadeh, M. Clinical Efficacy of Aloe Vera Toothpaste on Periodontal Parameters of Patients with Gingivitis—A Randomized, Controlled, Single-masked Clinical Trial. J. Contemp. Dent. Pract. 2021, 22, 242–247. [Google Scholar]
- Nazir, S.; Kumar, C. The Effect of Aloe Vera in Patient with Chronic Periodontitis. Pak. J. Med. Dent. 2019, 7, 5. [Google Scholar]
- Kanika, M. Efficacious Evaluation of Aloe Vera Tooth Gel and Commercially Available Tooth Gel on Patients with Gingivitis. J. Oral Health Dent. Sci. 2018, 2, 203. [Google Scholar]
- Vangipuram, S.; Jha, A.; Bhashyam, M. Comparative efficacy of aloe vera mouthwash and chlorhexidine on periodontal health: A randomized controlled trial. J. Clin. Exp. Dent. 2016, 8, e442–e447. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.A.; Malaiappan, S. The comparison of the antiplaque effect of aloe vera, chlorhexidine and placebo mouth washes on gingivitis patients. J. Pharm. Sci. Res. 2016, 8, 1295–1300. [Google Scholar]
- Yeturu, S.K.; Acharya, S.; Urala, A.S.; Pentapati, K.C. Effect of Aloe vera, chlorine dioxide, and chlorhexidine mouth rinses on plaque and gingivitis: A randomized controlled trial. J. Oral Biol. Craniofac. Res. 2016, 6, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Sargolzaie, N.; Rajabi, O.; Arab, H.; Esmaele, H.; Ehteshamfar, A. Comparative evaluation of Green Tea-Aloe Vera mouthwash and chlorhexidine 0.2% on gingival indices (A randomized clinical trial). J. Dent. Mater. Tech. 2016, 5, 31–35. [Google Scholar]
- Karim, B.; Bhaskar, D.J.; Agali, C.; Gupta, D.; Gupta, R.K.; Jain, A.; Kanwar, A. Effect of Aloe vera mouthwash on periodontal health: Triple blind randomized control trial. Oral Health Dent. Manag. 2014, 13, 14–19. [Google Scholar]
- Ashouri Moghaddam, A.; Radafshar, G.; Jahandideh, Y.; Kakaei, N. Clinical Evaluation of Effects of Local Application of Aloe vera Gel as an Adjunct to Scaling and Root Planning in Patients with Chronic Periodontitis. J. Dent. 2017, 18, 165–172. [Google Scholar]
- Makarem, A.; Asodeh, N.K.R. Efficacy of barberry aqueous extracts dental gel on control of plaque and gingivitis. Acta Med. Iran. 2007, 45, 91–94. [Google Scholar]
- Tripathi, P.; Blaggana, V.; Upadhyay, P.; Jindal, M.; Gupta, S.; Nishat, S. Antioxidant therapy (lycopene and green tea extract) in periodontal disease: A promising paradigm. J. Indian Soc. Periodontol. 2019, 23, 25–30. [Google Scholar]
- Taleghani, F.; Rezvani, G.; Birjandi, M.; Valizadeh, M. Impact of green tea intake on clinical improvement in chronic periodontitis: A randomized clinical trial. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 365–368. [Google Scholar] [CrossRef]
- Radafshar, G.; Ghotbizadeh, M.; Saadat, F.; Mirfarhadi, N. Effects of green tea (Camellia sinensis) mouthwash containing 1% tannin on dental plaque and chronic gingivitis: A double-blinded, randomized, controlled trial. J. Investig. Clin. Dent. 2017, 8, e12184. [Google Scholar] [CrossRef] [PubMed]
- Behfarnia, P.; Aslani, A.; Jamshidian, F.; Noohi, S. The Efficacy of Green Tea Chewing Gum on Gingival Inflammation. J. Dent. 2016, 17, 149–154. [Google Scholar]
- Sarin, S.; Marya, C.; Nagpal, R.; Oberoi, S.S.; Rekhi, A. Preliminary clinical evidence of the antiplaque, antigingivitis efficacy of a mouthwash containing 2% green tea—A randomised clinical trial. Oral Health Prev. Dent. 2015, 13, 197–203. [Google Scholar] [PubMed]
- Hambire, C.U.; Jawade, R.; Patil, A.; Wani, V.R.; Kulkarni, A.A.; Nehete, P.B. Comparing the antiplaque efficacy of 0.5% Camellia sinensis extract, 0.05% sodium fluoride, and 0.2% chlorhexidine gluconate mouthwash in children. J. Int. Soc. Prev. Community Dent. 2015, 5, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Jenabian, N.; Moghadamnia, A.A.; Karami, E.; Mir A, P.B. The effect of Camellia Sinensis (green tea) mouthwash on plaque-induced gingivitis: A single-blinded randomized controlled clinical trial. DARU J. Pharm. Sci. 2012, 20, 39. [Google Scholar] [CrossRef]
- Hattarki, S.; Pushpa, S.; Bhat, K. Evaluation of the efficacy of green tea catechins as an adjunct to scaling and root planing in the management of chronic periodontitis using PCR analysis: A clinical and microbiological study. J. Indian Soc. Periodontol. 2013, 17, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Hugar, S.S.; Patil, S.; Metgud, R.; Nanjwade, B.; Hugar, S.M. Influence of application of chlorhexidine gel and curcumin gel as an adjunct to scaling and root planing: A interventional study. J. Nat. Sci. Biol. Med. 2016, 7, 149. [Google Scholar] [CrossRef]
- Farjana, H.N.; Chandrasekaran, S.; Gita, B. Effect of oral curcuma gel in gingivitis management—A pilot study. J. Clin. Diagn. Res. JCDR 2014, 8, ZC08. [Google Scholar] [CrossRef]
- Mahendra, J.; Mahendra, L.; Svedha, P.; Cherukuri, S.; Romanos, G.E. Clinical and microbiological efficacy of 4% Garcinia mangostana L. pericarp gel as local drug delivery in the treatment of chronic periodontitis: A randomized, controlled clinical trial. J. Investig. Clin. Dent. 2017, 8, e12262. [Google Scholar] [CrossRef]
- Madan, S.; Kashyap, S.; Mathur, G. Glycyrrhiza glabra: An efficient medicinal plant for control of periodontitis—A randomized clinical trial. J. Int. Clin. Dent. Res. Organ. 2019, 11, 32–35. [Google Scholar] [CrossRef]
- Saimbi, C.; Shubh, N.; Kapoor, K.; Kaushal, S. Clinical effect of Juglans regia on developing dental plaque. J. Int. Clin. Dent. Res. Organ. 2009, 1, 1. [Google Scholar]
- Pereira, S.L.; Praxedes, Y.C.; Bastos, T.C.; Alencar, P.N.; da Costa, F.N. Clinical effect of a gel containing Lippia sidoides on plaque and gingivitis control. Eur. J. Dent. 2013, 7, 28–34. [Google Scholar] [PubMed]
- Botelho, M.A.; dos Santos, R.A.; Martins, J.G.; Carvalho, C.O.; Paz, M.C.; Azenha, C.; Ruela, R.S.; Queiroz, D.B.; Ruela, W.S.; Marinho, G.; et al. Comparative effect of an essential oil mouthrinse on plaque, gingivitis and salivary Streptococcus mutans levels: A double blind randomized study. Phytother. Res. 2009, 23, 1214–1219. [Google Scholar] [CrossRef]
- Bhat, S.S.; Hegde, K.S.; Mathew, C.; Bhat, S.V.; Shyamjith, M. Comparative evaluation of Mangifera indica leaf mouthwash with chlorhexidine on plaque accumulation, gingival inflammation, and salivary streptococcal growth. Indian. J. Dent. Res. 2017, 28, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Atwa, A.L.D.A.; AbuShahba, R.Y.; Mostafa, M.; Hashem, M.I. Effect of honey in preventing gingivitis and dental caries in patients undergoing orthodontic treatment. Saudi Dent. J. 2014, 26, 108–114. [Google Scholar] [CrossRef] [PubMed]
- English, H.K.P.; Pack, A.R.C.; Molan, P.C. The effects of manuka honey on plaque and gingivitis: A pilot study. J. Int. Acad. Periodontol. 2004, 6, 63–67. [Google Scholar]
- Agarwal, A.; Chaudhary, B. Clinical and microbiological effects of 1% Matricaria chamomilla mouth rinse on chronic periodontitis: A double-blind randomized placebo controlled trial. J. Indian Soc. Periodontol. 2020, 24, 354–361. [Google Scholar] [CrossRef]
- Goes, P.; Dutra, C.S.; Lisboa, M.R.; Gondim, D.V.; Leitão, R.; Brito, G.A.; Rego, R.O. Clinical efficacy of a 1% Matricaria chamomile L. mouthwash and 0.12% chlorhexidine for gingivitis control in patients undergoing orthodontic treatment with fixed appliances. J. Oral Sci. 2016, 58, 569–574. [Google Scholar] [CrossRef]
- Manohar Sharma, H.; Deepika, P.; Venkatesh, M.; Chandan, S.; Shashikumar, P. Efficacy of 3% Psidium guajava local drug delivery in the treatment of chronic periodontitis: A randomized controlled trial. J. Int. Oral Health 2021, 13, 17–23. [Google Scholar] [CrossRef]
- Dobayan, B.A.; Ayeid, F.a.A.; Guraid, I.A.; Bassiouny, G.; Nasser, S.A. The Effect of Punica Granatum Gel as An Adjunctive Therapy in Patients with chronic Periodontitis: A Clinical, Microbiological and histological Study. J. Am. Sci. 2019, 19, 12–15. [Google Scholar]
- Prakash, J.; Bhatnagar, V.; Nath, S.; Jacob Pulikkotil, S.; Prajapati, V. Effect of Punica granatum Extract Gel on Gingival Crevicular Fluid Levels of Interleukin-1β, Interleukin-8 and CCL28 Levels: Randomised Controlled Clinical Trial. J. Clin. Diagn. Res. 2017, 11, ZC12–ZC17. [Google Scholar] [CrossRef]
- Sedigh-Rahimabadi, M.; Fani, M.; Rostami-chijan, M.; Zarshenas, M.M.; Shams, M. A Traditional Mouthwash (Punica granatum var pleniflora) for Controlling Gingivitis of Diabetic Patients: A Double-Blind Randomized Controlled Clinical Trial. J. Evid.-Based Complement. Altern. Med. 2016, 22, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Azad, M.F.; Schwiertz, A.; Jentsch, H.F.R. Adjunctive use of essential oils following scaling and root planing—A randomized clinical trial. BMC Complement. Altern. Med. 2016, 16, 171. [Google Scholar] [CrossRef] [PubMed]
- Sabbagh, H.J.; AlGhamdi, K.S.; Mujalled, H.T.; Bagher, S.M. The effect of brushing with Salvadora persica (miswak) sticks on salivary Streptococcus mutans and plaque levels in children: A clinical trial. BMC Complement. Med. Ther. 2020, 20, 53. [Google Scholar] [CrossRef]
- Bahrololoomi, Z.; Sadat-Hashemi, A.; Hassan-Akhavan-Karbassi, M.; Khaksar, Y. Evaluating the additive effect of Persica and chlorhexidine mouthwashes on oral health status of children receiving chemotherapy for their hematomalignancy: A randomized clinical trial. J. Clin. Exp Dent. 2020, 12, e574–e580. [Google Scholar] [CrossRef]
- Varma, S.R.; Sherif, H.; Serafi, A.; Fanas, S.A.; Desai, V.; Abuhijleh, E.; Al Radaidah, A. The Antiplaque Efficacy of Two Herbal-Based Toothpastes: A Clinical Intervention. J. Int. Soc. Prev. Community Dent. 2018, 8, 21–27. [Google Scholar]
- Saha, S.; Mohammad, S.; Saha, S.; Samadi, F. Efficiency of traditional chewing stick (miswak) as an oral hygiene aid among Muslim school children in Lucknow: A cross-sectional study. J. Oral Biol. Craniofac. Res. 2012, 2, 176–180. [Google Scholar] [CrossRef]
- Gupta, D.; Gupta, R.; Bhaskar, D.; Gupta, V. Comparative Evaluation of Terminalia chebula Extract Mouthwash and Chlorhexidine Mouthwash on Plaque and Gingival Infl ammation—4-week Randomised Control Trial. Oral Health Prev. Dent. 2015, 13, 5–12. [Google Scholar]
- Gupta, D.; Bhaskar, D.J.; Gupta, R.K.; Karim, B.; Gupta, V.; Punia, H.; Batra, M.; Jain, A.; Agarwal, A.; Singh, P. Effect of Terminalia chebula extract and chlorhexidine on salivary pH and periodontal health: 2 weeks randomized control trial. Phytother. Res. 2014, 28, 992–998. [Google Scholar] [CrossRef]
- Esther, P.; Elanchezhiyan, S.; Daniel, R.; Meenalochani, T.; Pavithra, T.; Surya, D. Evaluation of clinical effificacy of Terminalia chebula inplaque-induced gingivitis: A randomized control trial. Indian J. Multidiscip. Dent. 2017, 7, 21–24. [Google Scholar] [CrossRef]
- Joët, T.; Salmona, J.; Laffargue, A.; Descroix, F.; Dussert, S. Use of the growing environment as a source of variation to identify the quantitative trait transcripts and modules of co-expressed genes that determine chlorogenic acid accumulation. Plant Cell Environ. 2010, 33, 1220–1233. [Google Scholar] [CrossRef] [PubMed]
- Higdon, J.V.; Frei, B. Coffee and health: A review of recent human research. Crit. Rev. Food Sci. Nutr. 2006, 46, 101–123. [Google Scholar] [CrossRef] [PubMed]
- Naveed, M.; Hejazi, V.; Abbas, M.; Kamboh, A.A.; Khan, G.J.; Shumzaid, M.; Ahmad, F.; Babazadeh, D.; FangFang, X.; Modarresi-Ghazani, F. Chlorogenic acid (CGA): A pharmacological review and call for further research. Biomed. Pharmacother. 2018, 97, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Bogdan, C.; Pop, A.; Iurian, S.M.; Benedec, D.; Moldovan, M.L. Research Advances in the Use of Bioactive Compounds from Vitis vinifera By-Products in Oral Care. Antioxidants 2020, 9, 502. [Google Scholar] [CrossRef] [PubMed]
- Bouayed, J.; Rammal, H.; Dicko, A.; Younos, C.; Soulimani, R. Chlorogenic acid, a polyphenol from Prunus domestica (Mirabelle), with coupled anxiolytic and antioxidant effects. J. Neurol. Sci. 2007, 262, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Chaube, S.; Swinyard, C.A. Teratological and toxicological studies of alkaloidal and phenolic compounds from Solanum tuberosum L. Toxicol. Appl. Pharmacol. 1976, 36, 227–237. [Google Scholar] [CrossRef]
- Yadav, M.; Kaushik, M.; Roshni, R.; Reddy, P.; Mehra, N.; Jain, V.; Rana, R. Effect of Green Coffee Bean Extract on Streptococcus mutans Count: A Randomised Control Trial. J. Clin. Diagn. Res. 2017, 11, Zc68–Zc71. [Google Scholar] [CrossRef]
- Tsou, S.-H.; Hu, S.-W.; Yang, J.-J.; Yan, M.; Lin, Y.-Y. Potential Oral Health Care Agent from Coffee Against Virulence Factor of Periodontitis. Nutrients 2019, 11, 2235. [Google Scholar] [CrossRef]
- Arruda, C.; Mejía, J.A.A.; Ribeiro, V.P.; Borges, C.H.G.; Martins, C.H.G.; Veneziani, R.C.S.; Ambrosio, S.R.; Bastos, J.K. Occurrence, chemical composition, biological activities and analytical methods on Copaifera genus—A review. Biomed. Pharmacother. 2019, 109, 1–20. [Google Scholar] [CrossRef]
- Bardají, D.K.R.; da Silva, J.J.M.; Bianchi, T.C.; de Souza Eugênio, D.; de Oliveira, P.F.; Leandro, L.F.; Rogez, H.L.G.; Venezianni, R.C.S.; Ambrosio, S.R.; Tavares, D.C. Copaifera reticulata oleoresin: Chemical characterization and antibacterial properties against oral pathogens. Anaerobe 2016, 40, 18–27. [Google Scholar] [CrossRef]
- Abrão, F.; de Araújo Costa, L.D.; Alves, J.M.; Senedese, J.M.; de Castro, P.T.; Ambrósio, S.R.; Veneziani, R.C.S.; Bastos, J.K.; Tavares, D.C.; Martins, C.H.G. Copaifera langsdorffii oleoresin and its isolated compounds: Antibacterial effect and antiproliferative activity in cancer cell lines. BMC Complement. Altern. Med. 2015, 15, 443. [Google Scholar] [CrossRef] [PubMed]
- da S. Moraes, T.; Leandro, L.F.; de O. Silva, L.; Santiago, M.B.; Souza, A.B.; Furtado, R.A.; Tavares, D.C.; Veneziani, R.C.S.; Ambrósio, S.R.; Bastos, J.K. In vitro evaluation of Copaifera oblongifolia oleoresin against bacteria causing oral infections and assessment of its cytotoxic potential. Curr. Pharm. Biotechnol. 2016, 17, 894–904. [Google Scholar] [CrossRef] [PubMed]
- Borges, C.H.; Cruz, M.G.; Carneiro, L.J.; da Silva, J.J.; Bastos, J.K.; Tavares, D.C.; de Oliveira, P.F.; Rodrigues, V.; Veneziani, R.C.; Parreira, R.L. Copaifera duckei oleoresin and its main nonvolatile terpenes: In vitro schistosomicidal properties. Chem. Biodivers. 2016, 13, 1348–1356. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.M.; Senedese, J.M.; Leandro, L.F.; Castro, P.T.; Pereira, D.E.; Carneiro, L.J.; Ambrósio, S.R.; Bastos, J.K.; Tavares, D.C. Copaifera multijuga oleoresin and its constituent diterpene (−)-copalic acid: Genotoxicity and chemoprevention study. Mutat. Res./Genet. Toxicol. Environ. Mutagen. 2017, 819, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Abrão, F.; Alves, J.A.; Andrade, G.; De Oliveira, P.F.; Ambrósio, S.R.; Veneziani, R.; Tavares, D.C.; Bastos, J.K.; Martins, C.H. Antibacterial effect of Copaifera duckei Dwyer oleoresin and its main diterpenes against oral pathogens and their cytotoxic effect. Front. Microbiol. 2018, 9, 201. [Google Scholar] [CrossRef]
- Furtado, R.A.; de Oliveira, P.F.; Senedese, J.M.; Ozelin, S.D.; de Souza, L.D.R.; Leandro, L.F.; de Oliveira, W.L.; da Silva, J.J.M.; Oliveira, L.C.; Rogez, H. Assessment of genotoxic activity of oleoresins and leaves extracts of six Copaifera species for prediction of potential human risks. J. Ethnopharmacol. 2018, 221, 119–125. [Google Scholar] [CrossRef]
- De Souza, M.G.M.; Leandro, L.F.; da Silva Moraes, T.; Abrão, F.; Veneziani, R.C.S.; Ambrosio, S.R.; Martins, C.H.G. ent-Copalic acid antibacterial and anti-biofilm properties against Actinomyces naeslundii and Peptostreptococcus anaerobius. Anaerobe 2018, 52, 43–49. [Google Scholar] [CrossRef]
- Abrão, F.; Silva, T.S.; Moura, C.L.; Ambrósio, S.R.; Veneziani, R.C.S.; de Paiva, R.E.F.; Bastos, J.K.; Martins, C.H.G. Oleoresins and naturally occurring compounds of Copaifera genus as antibacterial and antivirulence agents against periodontal pathogens. Sci. Rep. 2021, 11, 4953. [Google Scholar] [CrossRef]
- Ivanovska, N.; Philipov, S. Study on the anti-inflammatory action of Berberis vulgaris root extract, alkaloid fractions and pure alkaloids. Int. J. Immunopharmacol. 1996, 18, 553–561. [Google Scholar] [CrossRef]
- Nakamoto, K.; Sadamori, S.; Hamada, T. Effects of crude drugs and berberine hydrochloride on the activities of fungi. J. Prosthet. Dent. 1990, 64, 691–694. [Google Scholar] [CrossRef]
- Tu, H.-P.; Fu, M.M.; Kuo, P.-J.; Chin, Y.-T.; Chiang, C.-Y.; Chung, C.-L.; Fu, E. Berberine’s effect on periodontal tissue degradation by matrix metalloproteinases: An in vitro and in vivo experiment. Phytomedicine 2013, 20, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Yu, Z.-H. Effect of berberine hydrochloride on the secretion of monocyte chemoattractant protein-1 from human periodontal ligament cells in vitro. Zhonghua Kou Qiang Yi Xue Za Zhi= Zhonghua Kouqiang Yixue Zazhi= Chin. J. Stomatol. 2012, 47, 610–613. [Google Scholar]
- Yucel-Lindberg, T.; Båge, T. Inflammatory mediators in the pathogenesis of periodontitis. Expert Rev. Mol. Med. 2013, 15, e7. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Jia, L.; Mo, L.; Yuan, S.; Zheng, X.; He, J.; Chen, V.; Guo, Q.; Zheng, L.; Yuan, Q. Berberine ameliorates periodontal bone loss by regulating gut microbiota. J. Dent. Res. 2019, 98, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Gu, L.; Ke, Y.; Gan, J.; Li, X. Berberine suppresses bone loss and inflammation in ligature-induced periodontitis through promotion of the G protein-coupled estrogen receptor-mediated inactivation of the p38MAPK/NF-κB pathway. Arch. Oral Biol. 2021, 122, 104992. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.L.; Wu, Y.R.; Song, F.F.; Gan, J.; Huang, L.Y.; Zhang, L.; Huang, C. Role of PCSK9 in the development of mouse periodontitis before and after treatment: A double-edged sword. J. Infect. Dis. 2018, 217, 667–680. [Google Scholar] [CrossRef] [PubMed]
- Kohli, K.; Ali, J.; Ansari, M.; Raheman, Z. Curcumin: A natural antiinflammatory agent. Indian J. Pharmacol. 2005, 37, 141. [Google Scholar] [CrossRef]
- Suhag, A.; Dixit, J.; Dhan, P. Role of curcumin as a subgingival irrigant: A pilot study. Periodontal Pract. Today 2007, 4, 115–121. [Google Scholar]
- Guimarães, M.R.; Coimbra, L.S.; de Aquino, S.G.; Spolidorio, L.C.; Kirkwood, K.L.; Rossa, C., Jr. Potent anti-inflammatory effects of systemically administered curcumin modulate periodontal disease in vivo. J. Periodontal Res. 2011, 46, 269–279. [Google Scholar] [CrossRef]
- Guimaraes-Stabili, M.R.; de Aquino, S.G.; de Almeida Curylofo, F.; Tasso, C.O.; Rocha, F.R.G.; de Medeiros, M.C.; de Pizzol, J.P.; Cerri, P.S.; Romito, G.A.; Rossa, C. Systemic administration of curcumin or piperine enhances the periodontal repair: A preliminary study in rats. Clin. Oral Investig. 2019, 23, 3297–3306. [Google Scholar] [CrossRef]
- Anuradha, B.; Bai, Y.D.; Sailaja, S.; Sudhakar, J.; Priyanka, M.; Deepika, V. Evaluation of anti-inflammatory effects of curcumin gel as an adjunct to scaling and root planing: A clinical study. J. Int. Oral Health JIOH 2015, 7, 90. [Google Scholar] [PubMed]
- Nagasri, M.; Madhulatha, M.; Musalaiah, S.; Kumar, P.A.; Krishna, C.M.; Kumar, P.M. Efficacy of curcumin as an adjunct to scaling and root planning in chronic periodontitis patients: A clinical and microbiological study. J. Pharm. Bioallied Sci. 2015, 7 (Suppl. S2), S554. [Google Scholar] [CrossRef] [PubMed]
- Ravishankar, P.; Kumar, Y.P.; Anila, E.; Chakraborty, P.; Malakar, M.; Mahalakshmi, R. Effect of local application of curcumin and ornidazole gel in chronic periodontitis patients. Int. J. Pharm. Investig. 2017, 7, 188. [Google Scholar] [CrossRef] [PubMed]
- Kandwal, A.; Mamgain, R.K.; Mamgain, P. Comparative evaluation of turmeric gel with 2% chlorhexidine gluconate gel for treatment of plaque induced gingivitis: A randomized controlled clinical trial. Ayu 2015, 36, 145. [Google Scholar] [CrossRef]
- Jacob, P.; Nath, S.; Sultan, O. Use of curcumin in periodontal inflammation. Interdiscip. J. Microinflamm. 2014, 1, 2. [Google Scholar]
- Borges, J.S.; Paranhos, L.R.; de Souza, G.L.; de Souza Matos, F.; de Macedo Bernardino, Í.; Moura, C.C.G.; Soares, P.B.F. Does systemic oral administration of curcumin effectively reduce alveolar bone loss associated with periodontal disease? A systematic review and meta-analysis of preclinical in vivo studies. J. Funct. Foods 2020, 75, 104226. [Google Scholar] [CrossRef]
- Nebrisi, E.E. Neuroprotective Activities of Curcumin in Parkinson’s Disease: A Review of the Literature. Int. J. Mol. Sci. 2021, 22, 11248. [Google Scholar] [CrossRef]
- Shah, G.; Shri, R.; Panchal, V.; Sharma, N.; Singh, B.; Mann, A.S. Scientific basis for the therapeutic use of Cymbopogon citratus, stapf (Lemon grass). J. Adv. Pharm. Technol. Res. 2011, 2, 3–8. [Google Scholar] [CrossRef]
- Crawford, M.; Hanson, S.W.; Koker, M.E. The structure of cymbopogone, a novel triterpenoid from lemongrass. Tetrahedron Lett. 1975, 16, 3099–3102. [Google Scholar] [CrossRef]
- Hammer, K.A.; Carson, C.F.; Riley, T.V. Antimicrobial activity of essential oils and other plant extracts. J. Appl. Microbiol. 1999, 86, 985–990. [Google Scholar] [CrossRef]
- Khongkhunthian, S.; Sookkhee, S.; Okonogi, S. Antimicrobial activities against periodontopathogens of essential oil from lemon grass (Cymbopogon citratus (DC.) Stapf.). CMU J. Nat. Sci. 2009, 8, 11–22. [Google Scholar]
- Susanto, S.; Oktavianti, T.; Wijaya, Y.; Wira, V.; Paramitta, V. Increased glutathione level in saliva of moderate gingivitis patients after lemongrass (cymbopogoncitratus) essential oil gargling. Asia Pac. Dent. Stud. J. 2010, 1, 45–52. [Google Scholar]
- Bruschi, M.L.; Jones, D.S.; Panzeri, H.; Gremião, M.P.; de Freitas, O.; Lara, E.H. Semisolid systems containing propolis for the treatment of periodontal disease: In vitro release kinetics, syringeability, rheological, textural, and mucoadhesive properties. J. Pharm. Sci. 2007, 96, 2074–2089. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, S.I.; Devi, K.; Khanam, S.; Zahra, N. Citral, a component of lemongrass oil inhibits the clastogenic effect of nickel chloride in mouse micronucleus test system. Pak. J. Pharm. Sci. 2006, 19, 108–113. [Google Scholar]
- Batish, D.R.; Singh, H.P.; Kohli, R.K.; Kaur, S. Eucalyptus essential oil as a natural pesticide. For. Ecol. Manag. 2008, 256, 2166–2174. [Google Scholar] [CrossRef]
- Topiar, M.; Sajfrtova, M.; Pavela, R.; Machalova, Z. Comparison of fractionation techniques of CO2 extracts from Eucalyptus globulus—Composition and insecticidal activity. J. Supercrit. Fluids 2015, 97, 202–210. [Google Scholar] [CrossRef]
- Nagata, H.; Inagaki, Y.; Yamamoto, Y.; Maeda, K.; Kataoka, K.; Osawa, K.; Shizukuishi, S. Inhibitory effects of macrocarpals on the biological activity of Porphyromonas gingivalis and other periodontopathic bacteria. Oral Microbiol. Immunol. 2006, 21, 159–163. [Google Scholar] [CrossRef]
- Osawa, K.; Yasuda, H.; Morita, H.; Takeya, K.; Itokawa, H. Macrocarpals H, I, and J from the Leaves of Eucalyptus globulus. J. Nat. Prod. 1996, 59, 823–827. [Google Scholar] [CrossRef]
- Nagata, H.; Inagaki, Y.; Tanaka, M.; Ojima, M.; Kataoka, K.; Kuboniwa, M.; Nishida, N.; Shimizu, K.; Osawa, K.; Shizukuishi, S. Effect of Eucalyptus Extract Chewing Gum on Periodontal Health: A Double-Masked, Randomized Trial. J. Periodontol. 2008, 79, 1378–1385. [Google Scholar] [CrossRef]
- Steinmetz, K.A.; Potter, J.D. Vegetables, fruit, and cancer prevention: A review. J. Am. Diet. Assoc. 1996, 96, 1027–1039. [Google Scholar] [CrossRef]
- Yang, J.; Liu, R.H.; Halim, L. Antioxidant and antiproliferative activities of common edible nut seeds. LWT Food Sci. Technol. 2009, 42, 1–8. [Google Scholar] [CrossRef]
- Obolskiy, D.; Pischel, I.; Siriwatanametanon, N.; Heinrich, M. Garcinia mangostana L.: A phytochemical and pharmacological review. Phytother. Res. 2009, 23, 1047–1065. [Google Scholar] [CrossRef] [PubMed]
- Suttirak, W.; Manurakchinakorn, S. In vitro antioxidant properties of mangosteen peel extract. J. Food Sci. Technol. 2014, 51, 3546–3558. [Google Scholar] [CrossRef] [PubMed]
- Shan, T.; Ma, Q.; Guo, K.; Liu, J.; Li, W.; Wang, F.; Wu, E. Xanthones from mangosteen extracts as natural chemopreventive agents: Potential anticancer drugs. Curr. Mol. Med. 2011, 11, 666–677. [Google Scholar] [CrossRef] [PubMed]
- Shankaranarayan, D.; Gopalakrishnan, C.; Kameswaran, L. Pharmacological profile of mangostin and its derivatives. Arch. Int. Pharmacodyn. Ther. 1979, 239, 257–269. [Google Scholar] [PubMed]
- Lim, Y.K.; Yoo, S.Y.; Jang, Y.Y.; Lee, B.C.; Lee, D.S.; Kook, J.-K. Anti-inflammatory and in vitro bone formation effects of Garcinia mangostana L. and propolis extracts. Food Sci. Biotechnol. 2020, 29, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Messier, C.; Epifano, F.; Genovese, S.; Grenier, D. Licorice and its potential beneficial effects in common oro-dental diseases. Oral Dis. 2012, 18, 32–39. [Google Scholar] [CrossRef]
- Tanabe, S.-i.; Desjardins, J.; Bergeron, C.; Gafner, S.; Villinski, J.R.; Grenier, D. Reduction of bacterial volatile sulfur compound production by licoricidin and licorisoflavan A from licorice. J. Breath Res. 2012, 6, 016006. [Google Scholar] [CrossRef]
- Wittschier, N.; Faller, G.; Beikler, T.; Stratmann, U.; Hensel, A. Polysaccharides from Glycyrrhiza glabra L. exert significant anti-adhesive effects against Helicobacter pylori and Porphyromonas gingivalis. Planta Med. 2006, 72, P_238. [Google Scholar] [CrossRef]
- Bodet, C.; La, V.D.; Gafner, S.; Bergeron, C.; Grenier, D. A licorice extract reduces lipopolysaccharide-induced proinflammatory cytokine secretion by macrophages and whole blood. J. Periodontol. 2008, 79, 1752–1761. [Google Scholar] [CrossRef]
- La, V.D.; Tanabe, S.i.; Bergeron, C.; Gafner, S.; Grenier, D. Modulation of matrix metalloproteinase and cytokine production by licorice isolates licoricidin and licorisoflavan A: Potential therapeutic approach for periodontitis. J. Periodontol. 2011, 82, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.; Grenier, D. Cranberry proanthocyanidins act in synergy with licochalcone A to reduce Porphyromonas gingivalis growth and virulence properties, and to suppress cytokine secretion by macrophages. J. Appl. Microbiol. 2012, 113, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Farhad, S.Z.; Aminzadeh, A.; Mafi, M.; Barekatain, M.; Naghney, M.; Ghafari, M.R. The effect of adjunctive low-dose doxycycline and licorice therapy on gingival crevicular fluid matrix metalloproteinase-8 levels in chronic periodontitis. Dent. Res. J. 2013, 10, 624. [Google Scholar]
- Segura-Carretero, A.; Puertas-Mejía, M.A.; Cortacero-Ramírez, S.; Beltrán, R.; Alonso-Villaverde, C.; Joven, J.; Dinelli, G.; Fernández-Gutiérrez, A. Selective extraction, separation, and identification of anthocyanins from Hibiscus sabdariffa L. using solid phase extraction-capillary electrophoresis-mass spectrometry (time-of-flight/ion trap). Electrophoresis 2008, 29, 2852–2861. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Medina, I.C.; Beltrán-Debón, R.; Molina, V.M.; Alonso-Villaverde, C.; Joven, J.; Menéndez, J.A.; Segura-Carretero, A.; Fernández-Gutiérrez, A. Direct characterization of aqueous extract of Hibiscus sabdariffa using HPLC with diode array detection coupled to ESI and ion trap MS. J. Sep. Sci. 2009, 32, 3441–3448. [Google Scholar] [CrossRef] [PubMed]
- Hirunpanich, V.; Utaipat, A.; Morales, N.P.; Bunyapraphatsara, N.; Sato, H.; Herunsalee, A.; Suthisisang, C. Antioxidant Effects of Aqueous Extracts from Dried Calyx of Hibiscus sabdariffa L INN.(Roselle) in Vitro Using Rat Low-Density Lipoprotein (LDL). Biol. Pharm. Bull. 2005, 28, 481–484. [Google Scholar] [CrossRef]
- Olaleye, M. Cytotoxicity and antibacterial activity of methanolic extract of Hibiscus sabdariffa. Antioxidant effect of Cysticus scoparius against carbon tetrachloride treated liver injury in rats. J. Ethonopharmacol. 2007, 109, 41–47. [Google Scholar]
- Da-Costa-Rocha, I.; Bonnlaender, B.; Sievers, H.; Pischel, I.; Heinrich, M. Hibiscus sabdariffa L.—A phytochemical and pharmacological review. Food Chem. 2014, 165, 424–443. [Google Scholar] [CrossRef]
- Jung, E.; Kim, Y.; Joo, N. Physicochemical properties and antimicrobial activity of Roselle (Hibiscus sabdariffa L.). J. Sci. Food Agric. 2013, 93, 3769–3776. [Google Scholar] [CrossRef]
- Chandra Shekar, B.R.; Nagarajappa, R.; Suma, S.; Thakur, R. Herbal extracts in oral health care—A review of the current scenario and its future needs. Pharmacogn. Rev. 2015, 9, 87–92. [Google Scholar] [CrossRef]
- Portillo-Torres, L.A.; Bernardino-Nicanor, A.; Gómez-Aldapa, C.A.; González-Montiel, S.; Rangel-Vargas, E.; Villagómez-Ibarra, J.R.; González-Cruz, L.; Cortés-López, H.; Castro-Rosas, J. Hibiscus Acid and Chromatographic Fractions from Hibiscus Sabdariffa Calyces: Antimicrobial Activity against Multidrug-Resistant Pathogenic Bacteria. Antibiotics 2019, 8, 218. [Google Scholar] [CrossRef] [PubMed]
- Baena-Santillán, E.S.; Piloni-Martini, J.; Santos-López, E.M.; Gómez-Aldapa, C.A.; Rangel-Vargas, E.; Castro-Rosas, J. Comparison of the Antimicrobial Activity of Hibiscus sabdariffa Calyx Extracts, Six Commercial Types of Mouthwashes, and Chlorhexidine on Oral Pathogenic Bacteria, and the Effect of Hibiscus sabdariffa Extracts and Chlorhexidine on Permeability of the Bacterial Membrane. J. Med. Food. 2021, 24, 67–76. [Google Scholar] [PubMed]
- Subhaswaraj, P.; Sowmya, M.; Bhavana, V.; Dyavaiah, M.; Siddhardha, B. Determination of antioxidant activity of Hibiscus sabdariffa and Croton caudatus in Saccharomyces cerevisiae model system. J. Food Sci. Technol. 2017, 54, 2728–2736. [Google Scholar] [CrossRef] [PubMed]
- Riaz, G.; Chopra, R. A review on phytochemistry and therapeutic uses of Hibiscus sabdariffa L. Biomed. Pharmacother. 2018, 102, 575–586. [Google Scholar] [CrossRef]
- Djeussi, D.E.; Noumedem, J.A.K.; Seukep, J.A.; Fankam, A.G.; Voukeng, I.K.; Tankeo, S.B.; Nkuete, A.H.L.; Kuete, V. Antibacterial activities of selected edible plants extracts against multidrug-resistant Gram-negative bacteria. BMC Complement. Altern. Med. 2013, 13, 164. [Google Scholar] [CrossRef]
- Shen, C.-Y.; Zhang, T.-T.; Zhang, W.-L.; Jiang, J.-G. Anti-inflammatory activities of essential oil isolated from the calyx of Hibiscus sabdariffa L. Food Funct. 2016, 7, 4451–4459. [Google Scholar] [CrossRef]
- Hassan, S.T.; Berchová, K.; Majerová, M.; Pokorná, M.; Švajdlenka, E. In vitro synergistic effect of Hibiscus sabdariffa aqueous extract in combination with standard antibiotics against Helicobacter pylori clinical isolates. Pharm. Biol. 2016, 54, 1736–1740. [Google Scholar] [CrossRef]
- Builders, P.F.; Kabele-Toge, B.; Builders, M.; Chindo, B.A.; Anwunobi, P.A.; Isimi, Y.C. Wound healing potential of formulated extract from Hibiscus sabdariffa calyx. Indian J. Pharm. Sci. 2013, 75, 45–52. [Google Scholar] [CrossRef]
- Omezzine, F.; Daami-Remadi, M.; Rinez, A.; Ladhari, A.; Haouala, R. In vitro assessment of Inula sporganic extracts for their antifungal activity against some pathogenic and antagonistic fungi. Afr. J. Microbiol. Res. 2011, 5, 3527–3531. [Google Scholar]
- Karygianni, L.; Cecere, M.; Skaltsounis, A.L.; Argyropoulou, A.; Hellwig, E.; Aligiannis, N.; Wittmer, A.; Al-Ahmad, A. High-Level Antimicrobial Efficacy of Representative Mediterranean Natural Plant Extracts against Oral Microorganisms. BioMed Res. Int. 2014, 2014, 839019. [Google Scholar] [CrossRef]
- Danino, O.; Gottlieb, H.E.; Grossman, S.; Bergman, M. Antioxidant activity of 1,3-dicaffeoylquinic acid isolated from Inula viscosa. Food Res. Int. 2009, 42, 1273–1280. [Google Scholar] [CrossRef]
- Hernández, V.; Recio, M.C.; Máñez, S.; Giner, R.M.; Ríos, J.-L. Effects of naturally occurring dihydroflavonols from Inula viscosa on inflammation and enzymes involved in the arachidonic acid metabolism. Life Sci. 2007, 81, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Andolfi, A.; Zermane, N.; Cimmino, A.; Avolio, F.; Boari, A.; Vurro, M.; Evidente, A. Inuloxins A–D, phytotoxic bi-and tri-cyclic sesquiterpene lactones produced by Inula viscosa: Potential for broomrapes and field dodder management. Phytochemistry 2013, 86, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Hertel, S.; Graffy, L.; Pötschke, S.; Basche, S.; Al-Ahmad, A.; Hoth-Hannig, W.; Hannig, M.; Hannig, C. Effect of Inula viscosa on the pellicle’s protective properties and initial bioadhesion in-situ. Arch. Oral Biol. 2016, 71, 87–96. [Google Scholar] [CrossRef]
- Kurz, H.; Karygianni, L.; Argyropoulou, A.; Hellwig, E.; Skaltsounis, A.L.; Wittmer, A.; Vach, K.; Al-Ahmad, A. Antimicrobial Effects of Inula viscosa Extract on the In Situ Initial Oral Biofilm. Nutrients 2021, 13, 4029. [Google Scholar] [CrossRef]
- Oğuz, H.; Gökdoğan, O.; Baran, M.; Oğuz, I. Potential of walnut (Juglans regia L.) nursery production and its economic importance in Turkey. In XXX International Horticultural Congress IHC2018: XIX Symposium on Horticultural Economics and Management, VII Symposium on 1258; ISHS: Fort Collins, CO, USA, 2018. [Google Scholar]
- Ribeiro, A.S.; Estanqueiro, M.; Oliveira, M.B.; Sousa Lobo, J.M. Main Benefits and Applicability of Plant Extracts in Skin Care Products. Cosmetics 2015, 2, 322–341. [Google Scholar] [CrossRef]
- Strelyaeva, A.V.; Lezhava, D.I.; Luferov, A.N.; Kuznetsov, R.M.; Bobkova, N.V.; Lazareva Yu, B.; Kostikova, E.N. Study of Quality Medicinal Plants Bark Walnuts and Extract from it. Pharmacogn. J. 2020, 12, 282–286. [Google Scholar] [CrossRef]
- Croitoru, A.; Ficai, D.; Craciun, L.; Ficai, A.; Andronescu, E. Evaluation and Exploitation of Bioactive Compounds of Walnut, Juglans regia. Curr. Pharm. Des. 2019, 25, 119–131. [Google Scholar] [CrossRef]
- Jahanban-Esfahlan, A.; Ostadrahimi, A.; Tabibiazar, M.; Amarowicz, R. A Comprehensive Review on the Chemical Constituents and Functional Uses of Walnut (Juglans spp.) Husk. Int. J. Mol. Sci. 2019, 20, 3920. [Google Scholar] [CrossRef]
- Alkhawajah, A.M. Studies on the antimicrobial activity of juglans regia. Am. J. Chin. Med. 1997, 25, 175–180. [Google Scholar] [CrossRef]
- Zakavi, F.; Golpasand Hagh, L.; Daraeighadikolaei, A.; Farajzadeh Sheikh, A.; Daraeighadikolaei, A.; Leilavi Shooshtari, Z. Antibacterial Effect of Juglans Regia Bark against Oral Pathologic Bacteria. Int. J. Dent. 2013, 2013, 854765. [Google Scholar] [CrossRef] [PubMed]
- Pandita, N.; Mantri, M.; Alice, V. Antiplaque Activity of Juglans Regia L. and Characterization of Juglone from Juglans Regia L. Am. J. Biochem. Biotechnol. 2011, 7, 29–31. [Google Scholar]
- Farooq, Z. Evaluation of the Acacia nilotica extract in periodontitis induced Albino rabbit. Int. J. e-Healthc. Inf. Syst. 2019, 6, 164–172. [Google Scholar]
- Ntep Ntep, D.; Bong, A.; Ngokwe, B.; Nokam Kamdem, G.S.; Hortense, G.; Charles, B. In Vitro Evaluation of the Efficacy of an Aqueous Extract of Allium Sativum as an Antibacterial Agent on Three Major Periodontal Pathogen. J. Oral Dent. Health Res. 2021, 3, 121. [Google Scholar]
- Alirezaei, S.; Godarzi, H.; Moezi Ghadim, N.; Maheri, A. Antimicrobial Activity of Aqueous Garlic Extract (Allium sativum) Against Porphyromonas gingivalis: An In-Vitro Study. J. Res. Dent. Maxillofac. Sci. 2019, 4, 17–22. [Google Scholar] [CrossRef]
- George, D.; Bhat, S.S.; Antony, B. Comparative evaluation of the antimicrobial efficacy of aloe vera tooth gel and two popular commercial toothpastes: An in vitro study. Gen. Dent. 2009, 57, 238–241. [Google Scholar]
- Rodriguez-Garcia, A.; Peixoto, I.T.A.; Verde-Star, M.J.; De la Torre-Zavala, S.; Aviles-Arnaut, H.; Ruiz, A.L.T.G. In Vitro Antimicrobial and Antiproliferative Activity of Amphipterygium adstringens. Evid.-Based Complement. Altern. Med. Ecam 2015, 2015, 175497. [Google Scholar] [CrossRef]
- Ambarish, S.S.; Anmol, G.K.; Bellad, A.S.; Krishna, K. In-vitroantibacterial activity of neem, clove, and cinnamon against Actinobacillus sp., isolatedfrom chronic periodontitis patients. Biomedicine 2020, 40, 214–219. [Google Scholar]
- Ben Lagha, A.; Azelmat, J.; Vaillancourt, K.; Grenier, D. A polyphenolic cinnamon fraction exhibits anti-inflammatory properties in a monocyte/macrophage model. PLoS ONE 2021, 16, e0244805. [Google Scholar] [CrossRef]
- Amoian, B. Assessment of Antibacterial Effect of Cinnamon on Growth of Porphyromons Gingivalis in Chronic Periodontitis Patients with Deep Pockets; Babol University of Medical Sciences: Babol, Iran, 2018. [Google Scholar]
- Zainal-Abidin, Z.; Mohd-Said, S.; Adibah, F.; Abdul Majid, F.; Aida, W.; Wan Mustapha, W.; Jantan, I. Anti-Bacterial Activity of Cinnamon Oil on Oral Pathogens. Open Conf. Proc. J. 2013, 4, 12–16. [Google Scholar] [CrossRef]
- Zambrano, L.M.G.; Brandao, D.A.; Rocha, F.R.G.; Marsiglio, R.P.; Longo, I.B.; Primo, F.L.; Tedesco, A.C.; Guimaraes-Stabili, M.R.; Rossa, C., Jr. Local administration of curcumin-loaded nanoparticles effectively inhibits inflammation and bone resorption associated with experimental periodontal disease. Sci. Rep. 2018, 8, 6652. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, M.; Pires, P.; Ribeiro, F.; Pimentel, S.; Casarin, R.; Cirano, F.; Tenenbaum, H.; Casati, M. Systemic treatment with resveratrol and/or curcumin reduces the progression of experimental periodontitis in rats. J. Periodontal Res. 2017, 52, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Paavai, I.; Vasugi, S.; Ayswarya, V.V.; Vanessa, R.; Veejai, C.; Arulpari, M.; Vineela Katam, R. Evaluation of Antibacterial Activity of Lemongrass Oil against Oral Clinical Isolates—An In vitro Study. Pharmacogn. J. 2019, 11, 1023–1028. [Google Scholar]
- Harkat-Madouri, L.; Asma, B.; Madani, K.; Said, Z.B.-O.S.; Rigou, P.; Grenier, D.; Allalou, H.; Remini, H.; Adjaoud, A.; Boulekbache-Makhlouf, L. Chemical composition, antibacterial and antioxidant activities of essential oil of Eucalyptus globulus from Algeria. Ind. Crops Prod. 2015, 78, 148–153. [Google Scholar] [CrossRef]
- Ridwan, R.D.; Yuliati, Y.; Sidarningsih, S.; Sholihah, F.M.; Aljunaid, M.; Lashari, D.M. A study of the mucoadhesive patches loaded with mangosteen peel extract in periodontitis. J. Taibah Univ. Med. Sci. 2021, 16, 864–869. [Google Scholar] [CrossRef]
- Suwannakul, S.; Chaibenjawong, P. Antibacterial Activities of Glycyrrhiza gabra Linn. (Licorice) Root Extract against Porphyromonas gingivalis rand Its Inhibitory Effects on Cysteine Proteases and Biofilms. J. Dent. Indones. 2017, 24, 85–92. [Google Scholar] [CrossRef]
- Sharma, H.; Yunus, G.; Mohapatra, A.; Kulshrestha, R.; Agrawal, R.; Kalra, M. Antimicrobial efficacy of three medicinal plants Glycyrrhiza glabra, Ficus religiosa, and Plantago major on inhibiting primary plaque colonizers and periodontal pathogens: An in vitro study. Indian J. Dent. Res. 2016, 27, 200–204. [Google Scholar] [CrossRef]
- Khawlah, A.S.; Sahar, M.J.; Najla Naji, C.; Alaa, S.J.A.-B. Efficacy of Bark (Juglans regia L.) Extracts Against Periodontitis Bacteria: An In Vitro Study. Indian J. Forensic Med. Toxicol. 2021, 15, 5492–5498. [Google Scholar]
- Botelho, M.A.; Barros, G.; Queiroz, D.B.; Carvalho, C.F.; Gouvea, J.; Patrus, L.; Bannet, M.; Patrus, D.; Rego, A.; Silva, I.; et al. Nanotechnology in Phytotherapy: Antiinflammatory Effect of a Nanostructured Thymol Gel from Lippia sidoides in Acute Periodontitis in Rats. Phytother. Res. 2016, 30, 152–159. [Google Scholar] [CrossRef]
- Aparna, S.; Srirangarajan, S.; Malgi, V.; Setlur, K.P.; Shashidhar, R.; Setty, S.; Thakur, S. A comparative evaluation of the antibacterial efficacy of honey in vitro and antiplaque efficacy in a 4-day plaque regrowth model in vivo: Preliminary results. J. Periodontol. 2012, 83, 1116–1121. [Google Scholar] [CrossRef]
- Jangid, K.; Bhargava, V.; Jayakumar, D. Anti-protease activity of Myristica fragrans compared to doxycycline on periodontal tissues: An ex-vivo study. Res. J. Pharm. Biol. Chem. Sci. 2016, 7, 984–988. [Google Scholar]
- Kaawoan, P.T.; Abidjulu, J.; Siagian, K.V. Uji daya hambat ekstrak buah pala (Myristica fragrans Houtt) terhadap bakteri penyebab periodontitis porphyromonas gingivalis secara in vitro. e-GiGi 2016, 4, 13504. [Google Scholar] [CrossRef]
- Shinohara, C.; Mori, S.; Ando, T.; Tsuji, T. Arg-Gingipain Inhibition and Anti-bacterial Activity Selective for Porphyromonas gingivalis by Malabaricone C. Biosci. Biotechnol. Biochem. 1999, 63, 1475–1477. [Google Scholar] [CrossRef] [PubMed]
- Mallikarjun, S.; Rao, A.; Rajesh, G.; Shenoy, R.; Pai, M. Antimicrobial efficacy of Tulsi leaf (Ocimum sanctum) extract on periodontal pathogens: An in vitro study. J. Indian Soc. Periodontol. 2016, 20, 145–150. [Google Scholar]
- Hosadurga, R.R.; Rao, S.N.; Edavanputhalath, R.; Jose, J.; Rompicharla, N.C.; Shakil, M.; Raju, S. Evaluation of the efficacy of 2% Ocimum sanctum gel in the treatment of experimental periodontitis. Int. J. Pharm. Investig. 2015, 5, 35–42. [Google Scholar] [CrossRef]
- Azeez, S.H.; Gaphor, S.M. Evaluation of antibacterial effect against Porphyromonas gingivalis and biocompatibility of essential oil extracted from the gum of Pistacia atlantica kurdica. BioMed Res. Int. 2019, 2019, 9195361. [Google Scholar] [CrossRef]
- Sekar, S.; Jacob, S.; Suthanthiran, T.K.; Dhasthaheer, S.; Vikraman, S.; Kaliappan, K. Characterization and Formulation of Miswak Film for the Treatment of Chronic Periodontitis: An In Vitro Study. J. Pharm. Bioallied. Sci. 2020, 12 (Suppl. S1), S199–S203. [Google Scholar] [CrossRef]
- Siddeeqh, S.; Parida, A.; Jose, M.; Pai, V. Estimation of Antimicrobial Properties of Aqueous and Alcoholic Extracts of Salvadora Persica (Miswak) on Oral Microbial Pathogens—An Invitro Study. J. Clin. Diagn. Res. 2016, 10, Fc13–Fc16. [Google Scholar] [CrossRef]
- Gursoy, U.K.; Gursoy, M.; Gursoy, O.V.; Cakmakci, L.; Könönen, E.; Uitto, V.J. Anti-biofilm properties of Satureja hortensis L. essential oil against periodontal pathogens. Anaerobe 2009, 15, 164–167. [Google Scholar] [CrossRef]
- Fotsing Kwetché, P.R.; Essama Eno Belinga, L.; Yawat Djogang, A.M.; Chamdjeu, V.T.; Agbor, M.A.; Tchoukoua, S.H.; Tekam, J.M. Antibacterial Potential of Hydro-Ethanolic Extracts from Syzygium Aromaticum (Myrtaceae) on Periodontal Bacteria. Health Sci. Dis. 2021, 22, 2530. [Google Scholar]
- Lee, J.; Nho, Y.H.; Yun, S.K.; Hwang, Y.S. Use of ethanol extracts of Terminalia chebula to prevent periodontal disease induced by dental plaque bacteria. BMC Complement. Altern. Med. 2017, 17, 113. [Google Scholar] [CrossRef] [PubMed]
- Labrecque, J.; Bodet, C.; Chandad, F.; Grenier, D. Effects of a high-molecular-weight cranberry fraction on growth, biofilm formation and adherence of Porphyromonas gingivalis. J. Antimicrob. Chemother. 2006, 58, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Özden, F.O.; Sakallioğlu, E.E.; Sakallioğlu, U.; Ayas, B.; Erişgin, Z. Effects of grape seed extract on periodontal disease: An experimental study in rats. J. Appl. Oral Sci. 2017, 25, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Bae, J.; Lee, D.S. Antibacterial activity of [10} gingerol and [12} gingerol isolated from ginger rhizome against periodontal bacteria. Phytother. Res. 2008, 22, 1446–1449. [Google Scholar] [CrossRef] [PubMed]
- Funari, C.S.; Gullo, F.P.; Napolitano, A.; Carneiro, R.L.; Mendes-Giannini, M.J.; Fusco-Almeida, A.M.; Piacente, S.; Pizza, C.; Silva, D.H. Chemical and antifungal investigations of six Lippia species (Verbenaceae) from Brazil. Food Chem. 2012, 135, 2086–2094. [Google Scholar] [CrossRef]
- Pinto Cda, P.; Rodrigues, V.D.; Pinto Fda, P.; Pinto Rda, P.; Uetanabaro, A.P.; Pinheiro, C.S.; Gadea, S.F.; Silva, T.R.; Lucchese, A.M. Antimicrobial activity of lippia species from the brazilian semiarid region traditionally used as antiseptic and anti-infective agents. Evid.-Based Complement. Altern. Med. 2013, 2013, 614501. [Google Scholar]
- Fontenelle, R.O.; Morais, S.M.; Brito, E.H.; Kerntopf, M.R.; Brilhante, R.S.; Cordeiro, R.A.; Tomé, A.R.; Queiroz, M.G.; Nascimento, N.R.; Sidrim, J.J.; et al. Chemical composition, toxicological aspects and antifungal activity of essential oil from Lippia sidoides Cham. J. Antimicrob. Chemother. 2007, 59, 934–940. [Google Scholar] [CrossRef]
- Gomes, G.A.; Monteiro, C.M.; Senra Tde, O.; Zeringota, V.; Calmon, F.; Matos Rda, S.; Daemon, E.; Gois, R.W.; Santiago, G.M.; de Carvalho, M.G. Chemical composition and acaricidal activity of essential oil from Lippia sidoides on larvae of Dermacentor nitens (Acari: Ixodidae) and larvae and engorged females of Rhipicephalus microplus (Acari: Ixodidae). Parasitol. Res. 2012, 111, 2423–2430. [Google Scholar] [CrossRef]
- Pascual, M.E.; Slowing, K.; Carretero, E.; Sánchez Mata, D.; Villar, A. Lippia: Traditional uses, chemistry and pharmacology: A review. J. Ethnopharmacol. 2001, 76, 201–214. [Google Scholar] [CrossRef]
- Botelho, M.A.; Bezerra Filho, J.G.; Correa, L.L.; Fonseca, S.G.; Montenegro, D.; Gapski, R.; Brito, G.A.; Heukelbach, J. Effect of a novel essential oil mouthrinse without alcohol on gingivitis: A double-blinded randomized controlled trial. J. Appl. Oral Sci. 2007, 15, 175–180. [Google Scholar] [CrossRef]
- Rodrigues, I.S.; Tavares, V.N.; Pereira, S.L.; Costa, F.N. Antiplaque and antigingivitis effect of Lippia Sidoides: A double-blind clinical study in humans. J. Appl. Oral Sci. 2009, 17, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Botelho, M.A.; Rao, V.S.; Carvalho, C.B.; Bezerra-Filho, J.G.; Fonseca, S.G.; Vale, M.L.; Montenegro, D.; Cunha, F.; Ribeiro, R.A.; Brito, G.A. Lippia sidoides and Myracrodruon urundeuva gel prevents alveolar bone resorption in experimental periodontitis in rats. J. Ethnopharmacol. 2007, 113, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Girão, V.C.; Nunes-Pinheiro, D.C.; Morais, S.M.; Sequeira, J.L.; Gioso, M.A. A clinical trial of the effect of a mouth-rinse prepared with Lippia sidoides Cham essential oil in dogs with mild gingival disease. Prev. Vet. Med. 2003, 59, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Gomes de Alencar-Araripe, M.; Sousa Nunes-Pinheiro, D.C.; Odebrecht Costa, B.; Sampaio Batista, L.; Silva Feitosa, M.; Gama de Almeida, G.K.; da Rocha Tomé, A.; Carneiro Girão, V. A Clinical Trial and Oral Wound Treated by Essential Oil of Lippia sidoides Mouthrinse in Horses. Acta Sci. Vet. 2014, 42, 1249. [Google Scholar]
- Coe, F.G.; Anderson, G.J. Screening of medicinal plants used by the Garífuna of eastern Nicaragua for bioactive compounds. J. Ethnopharmacol. 1996, 53, 29–50. [Google Scholar] [CrossRef] [PubMed]
- Andreu, G.P.; Delgado, R.; Velho, J.A.; Curti, C.; Vercesi, A.E. Iron complexing activity of mangiferin, a naturally occurring glucosylxanthone, inhibits mitochondrial lipid peroxidation induced by Fe2+-citrate. Eur. J. Pharmacol. 2005, 513, 47–55. [Google Scholar] [CrossRef]
- Leiro, J.M.; Alvarez, E.; Arranz, J.A.; Siso, I.G.; Orallo, F. In vitro effects of mangiferin on superoxide concentrations and expression of the inducible nitric oxide synthase, tumour necrosis factor-alpha and transforming growth factor-beta genes. Biochem. Pharmacol. 2003, 65, 1361–1371. [Google Scholar] [CrossRef]
- Li, H.; Miyahara, T.; Tezuka, Y.; Namba, T.; Nemoto, N.; Tonami, S.; Seto, H.; Tada, T.; Kadota, S. The effect of Kampo formulae on bone resorption in vitro and in vivo. I. Active constituents of Tsu-kan-gan. Biol. Pharm. Bull. 1998, 21, 1322–1326. [Google Scholar] [CrossRef]
- Bairy, I.; Reeja, S.; Siddharth; Rao, P.S.; Bhat, M.; Shivananda, P.G. Evaluation of antibacterial activity of Mangifera indica on anaerobic dental microglora based on in vivo studies. Indian J. Pathol. Microbiol. 2002, 45, 307–310. [Google Scholar]
- Israili, Z.H. Antimicrobial properties of honey. Am. J. Ther. 2014, 21, 304–323. [Google Scholar] [CrossRef]
- Schneider, M.; Coyle, S.; Warnock, M.; Gow, I.; Fyfe, L. Anti-microbial activity and composition of manuka and portobello honey. Phytother. Res. 2013, 27, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Al-Waili, N.; Salom, K.; Al-Ghamdi, A.A. Honey for wound healing, ulcers, and burns; data supporting its use in clinical practice. TheScientificWorldJournal 2011, 11, 766–787. [Google Scholar] [CrossRef] [PubMed]
- Al-Waili, N.; Al-Ghamdi, A.; Ansari, M.; Al-Attar, Y.; Osman, A.; Salom, K. Differences in composition of honey samples and their impact on the antimicrobial activities against drug multiresistant bacteria and pathogenic fungi. Arch. Med. Res. 2013, 44, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Jull, A.B.; Cullum, N.; Dumville, J.C.; Westby, M.J.; Deshpande, S.; Walker, N. Honey as a topical treatment for wounds. Cochrane Database Syst. Rev. 2015, 2015, CD005083. [Google Scholar] [CrossRef] [PubMed]
- Charalambous, M.; Raftopoulos, V.; Lambrinou, E.; Charalambous, A. The effectiveness of honey for the management of radiotherapy-induced oral mucositis in head and neck cancer patients: A systematic review of clinical trials. Eur. J. Integr. Med. 2013, 5, 217–225. [Google Scholar] [CrossRef]
- Alvarez-Suarez, J.M.; Gasparrini, M.; Forbes-Hernández, T.Y.; Mazzoni, L.; Giampieri, F. The composition and biological activity of honey: A focus on Manuka honey. Foods 2014, 3, 420–432. [Google Scholar] [CrossRef]
- Molan, P.C. The antibacterial activity of honey: 1. The nature of the antibacterial activity. Bee World 1992, 73, 5–28. [Google Scholar] [CrossRef]
- Allen, K.L.; Molan, P.C.; Reid, G.M. A survey of the antibacterial activity of some New Zealand honeys. J. Pharm. Pharmacol. 1991, 43, 817–822. [Google Scholar] [CrossRef]
- Cooper, R.; Molan, P.; Harding, K. The sensitivity to honey of Gram-positive cocci of clinical significance isolated from wounds. J. Appl. Microbiol. 2002, 93, 857–863. [Google Scholar] [CrossRef]
- Maddocks, S.E.; Lopez, M.S.; Rowlands, R.S.; Cooper, R.A. Manuka honey inhibits the development of Streptococcus pyogenes biofilms and causes reduced expression of two fibronectin binding proteins. Microbiology 2012, 158, 781–790. [Google Scholar] [CrossRef]
- Hammond, E.N.; Donkor, E.S.; Brown, C.A. Biofilm formation of Clostridium difficile and susceptibility to Manuka honey. BMC Complement. Altern. Med. 2014, 14, 329. [Google Scholar] [CrossRef] [PubMed]
- Badet, C.; Quero, F. The in vitro effect of manuka honeys on growth and adherence of oral bacteria. Anaerobe 2011, 17, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Schmidlin, P.R.; English, H.; Duncan, W.; Belibasakis, G.N.; Thurnheer, T. Antibacterial potential of Manuka honey against three oral bacteria in vitro. Swiss Dent. J. 2014, 124, 922–924. [Google Scholar] [PubMed]
- Haffajee, A.D. Microbial etiological agents of destructive periodontal diseases. Periodontology 2000 1994, 5, 78–111. [Google Scholar] [CrossRef] [PubMed]
- Slots, J.; Reynolds, H.S.; Genco, R.J. Actinobacillus actinomycetemcomitans in human periodontal disease: A cross-sectional microbiological investigation. Infect. Immun. 1980, 29, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.; Schäfer, G.; Kwieciński, J.; Atrott, J.; Henle, T.; Pfister, W. Honey—A potential agent against Porphyromonas gingivalis: An in vitro study. BMC Oral Health 2014, 14, 24. [Google Scholar] [CrossRef]
- Safii, S.H.; Tompkins, G.R.; Duncan, W.J. Periodontal Application of Manuka Honey: Antimicrobial and Demineralising Effects In Vitro. Int. J. Dent. 2017, 2017, 9874535. [Google Scholar] [CrossRef]
- Srivastava, J.K.; Shankar, E.; Gupta, S. Chamomile: A herbal medicine of the past with a bright future. Mol. Med. Rep. 2010, 3, 895–901. [Google Scholar]
- McKay, D.L.; Blumberg, J.B. A review of the bioactivity and potential health benefits of chamomile tea (Matricaria recutita L.). Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 2006, 20, 519–530. [Google Scholar] [CrossRef]
- Avallone, R.; Zanoli, P.; Puia, G.; Kleinschnitz, M.; Schreier, P.; Baraldi, M. Pharmacological profile of apigenin, a flavonoid isolated from Matricaria chamomilla. Biochem. Pharmacol. 2000, 59, 1387–1394. [Google Scholar] [CrossRef]
- Srivastava, J.K.; Pandey, M.; Gupta, S. Chamomile, a novel and selective COX-2 inhibitor with anti-inflammatory activity. Life Sci. 2009, 85, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.D.; Marques, M.M.; Bussadori, S.K.; Martins, M.A.T.; Pavesi, V.C.S.; Mesquita-Ferrari, R.A.; Fernandes, K.P.S. Comparative analysis between Chamomilla recutita and corticosteroids on wound healing. An in vitro and in vivo study. Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 2009, 23, 274–278. [Google Scholar] [CrossRef]
- Pourabbas, R.; Delazar, A.; Chitsaz, M.T. The effect of German chamomile mouthwash on dental plaque and gingival inflammation. Iran. J. Pharm. Res. 2010, 105–109. [Google Scholar]
- Willershausen, B.; Kasaj, A.; Sculean, A.; Wehrbein, H. Influence of an Herbal Mouthwash on Inflammatory Changes of the Gingiva in Patients with Fixed Orthodontic Appliance. Periodontal Pract. Today 2004, 1, 255–262. [Google Scholar]
- Batista, A.L.A.; Lins, R.D.A.U.; de Souza Coelho, R.; do Nascimento Barbosa, D.; Belém, N.M.; Celestino, F.J.A. Clinical efficacy analysis of the mouth rinsing with pomegranate and chamomile plant extracts in the gingival bleeding reduction. Complement. Ther. Clin. Pract. 2014, 20, 93–98. [Google Scholar] [CrossRef]
- Tiemann, P.; Toelg, M.; Ramos F, M.H. Administration of Ratanhia-based herbal oral care products for the prophylaxis of oral mucositis in cancer chemotherapy patients: A clinical trial. Evid.-Based Complement. Altern. Med. 2007, 4, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Al-Mustafa, A.H.; Al-Thunibat, O.Y. Antioxidant activity of some Jordanian medicinal plants used traditionally for treatment of diabetes. Pak. J. Biol. Sci. 2008, 11, 351–358. [Google Scholar] [CrossRef]
- Siddiqui, N.A. Chemical constituents of essential oil from flowers of Matricaria aurea grown in Saudi Arabia. Indian J. Drugs 2014, 2, 164–168. [Google Scholar]
- Singh, O.; Khanam, Z.; Misra, N.; Srivastava, M.K. Chamomile (Matricaria chamomilla L.): An overview. Pharmacogn. Rev. 2011, 5, 82. [Google Scholar] [CrossRef]
- Ahmad, I.; Wahab, S.; Nisar, N.; Dera, A.A.; Alshahrani, M.Y.; Abullias, S.S.; Irfan, S.; Alam, M.M.; Srivastava, S. Evaluation of antibacterial properties of Matricaria aurea on clinical isolates of periodontitis patients with special reference to red complex bacteria. Saudi Pharm. J. SPJ Off. Publ. Saudi Pharm. Soc. 2020, 28, 1203–1209. [Google Scholar] [CrossRef]
- Chan, E.W.C.; Lye, P.-Y.; Wong, S.-K. Phytochemistry, pharmacology, and clinical trials of Morus alba. Chin. J. Nat. Med. 2016, 14, 17–30. [Google Scholar] [PubMed]
- Gunjal, S.; Ankola, A.; Bhat, K. In vitro antibacterial activity of ethanolic extract of Morus alba leaf against periodontal pathogens. Indian J. Dent. Res. 2015, 26, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Soonthornsit, N.; Pitaksutheepong, C.; Hemstapat, W.; Utaisincharoen, P.; Pitaksuteepong, T. In Vitro Anti-Inflammatory Activity of Morus alba L. Stem Extract in LPS-Stimulated RAW 264.7 Cells. Evid.-Based Complement. Altern. Med. 2017, 2017, 3928956. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.-G.; Matsuzaki, K.; Takamatsu, S.; Kitanaka, S. Inhibitory Effects of Constituents from Morus alba var. multicaulis on Differentiation of 3T3-L1 Cells and Nitric Oxide Production in RAW264.7 Cells. Molecules 2011, 16, 6010–6022. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, P.; Kumar, P.; Singh, V.K.; Singh, D.K. Biological effects of Myristica fragrans. Annu. Rev. Biomed. Sci. 2009, 11, 21–29. [Google Scholar]
- Yang, X.-W.; Huang, X.; Ahmat, M. New neolignan from seed of Myristica fragrans. Zhongguo Zhong Yao Za Zhi China J. Chin. Mater. Medica 2008, 33, 397–402. [Google Scholar]
- Chung, J.Y.; Choo, J.H.; Lee, M.H.; Hwang, J.K. Anticariogenic activity of macelignan isolated from Myristica fragrans (nutmeg) against Streptococcus mutans. Phytomedicine 2006, 13, 261–266. [Google Scholar] [CrossRef]
- Sonavane, G.S.; Sarveiya, V.P.; Kasture, V.S.; Kasture, S.B. Anxiogenic activity of Myristica fragrans seeds. Pharmacol. Biochem. Behav. 2002, 71, 239–244. [Google Scholar] [CrossRef]
- Hussain, S.; Rao, A. Chemopreventive action of mace (Myristica fragrans, Houtt) on methylcholanthrene-induced carcinogenesis in the uterine cervix in mice. Cancer Lett. 1991, 56, 231–234. [Google Scholar] [CrossRef]
- Ozaki, Y.; Soedigdo, S.; Wattimena, Y.R.; Suganda, A.G. Antiinflammatory effect of mace, aril of Myristica fragrans Houtt., and its active principles. Jpn. J. Pharmacol. 1989, 49, 155–163. [Google Scholar] [CrossRef]
- Narasimhan, B.; Dhake, A.S. Antibacterial principles from Myristica fragrans seeds. J. Med. Food 2006, 9, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Shafiei, Z.; Shuhairi, N.N.; Md Fazly Shah Yap, N.; Harry Sibungkil, C.-A.; Latip, J. Antibacterial Activity of Myristica fragrans against Oral Pathogens. Evid.-Based Complement. Altern. Med. Ecam 2012, 2012, 825362. [Google Scholar] [CrossRef] [PubMed]
- Miguel, M.G. Antioxidant and anti-inflammatory activities of essential oils: A short review. Molecules 2010, 15, 9252–9287. [Google Scholar] [CrossRef] [PubMed]
- Yoon, W.J.; Kim, S.S.; Oh, T.H.; Lee, N.H.; Hyun, C.G. Torreya nucifera Essential Oil Inhibits Skin Pathogen Growth and Lipopolysaccharide-Induced Inflammatory Effects. Int. J. Pharmacol. 2009, 5, 37–43. [Google Scholar] [CrossRef]
- Hart, P.H.; Brand, C.; Carson, C.F.; Riley, T.V.; Prager, R.H.; Finlay-Jones, J.J. Terpinen-4-ol, the main component of the essential oil of Melaleuca alternifolia (tea tree oil), suppresses inflammatory mediator production by activated human monocytes. Inflamm. Res. 2000, 49, 619–626. [Google Scholar] [CrossRef]
- Juhás, Š.; Bukovska, A.; Čikoš, Š.; Czikková, S.; Fabian, D.; Koppel, J. Anti-Inflammatory Effects of Rosmarinus officinalis Essential Oil in Mice. Acta Vet. Brno 2009, 78, 121–127. [Google Scholar] [CrossRef]
- Gomes, A.; Fernandes, E.; Lima, J.L.; Mira, L.; Corvo, M.L. Molecular mechanisms of anti-inflammatory activity mediated by flavonoids. Curr. Med. Chem. 2008, 15, 1586–1605. [Google Scholar] [CrossRef]
- Anggakusuma; Yanti; Hwang, J.-K. Effects of macelignan isolated from Myristica fragrans Houtt. on UVB-induced matrix metalloproteinase-9 and cyclooxygenase-2 in HaCaT cells. J. Dermatol. Sci. 2010, 57, 114–122. [Google Scholar] [CrossRef]
- Lee, K.E.; Mun, S.; Pyun, H.B.; Kim, M.S.; Hwang, J.K. Effects of macelignan isolated from Myristica fragrans (Nutmeg) on expression of matrix metalloproteinase-1 and type I procollagen in UVB-irradiated human skin fibroblasts. Biol. Pharm. Bull. 2012, 35, 1669–1675. [Google Scholar] [CrossRef]
- Sethi, J.; Sood, S.; Seth, S.; Talwar, A. Evaluation of hypoglycemic and antioxidant effect of Ocimum sanctum. Indian J. Clin. Biochem. 2004, 19, 152–155. [Google Scholar] [CrossRef]
- Devi, P.U.; Ganasoundari, A. Modulation of glutathione and antioxidant enzymes by Ocimum sanctum and its role in protection against radiation injury. Indian J. Exp. Biol. 1999, 37, 262–268. [Google Scholar] [PubMed]
- Sharma, P.; Kulshreshtha, S.; Sharma, A. Anti-cataract activity of Ocimum sanctum on experimental cataract. Indian J. Pharmacol. 1998, 30, 16. [Google Scholar]
- Agarwal, P.; Nagesh, L. Evaluation of the antimicrobial activity of various concentrations of Tulsi (Ocimum sanctum) extract against Streptococcus mutans: An in vitro study. Indian J. Dent. Res. 2010, 21, 357–359. [Google Scholar] [CrossRef]
- Kelm, M.A.; Nair, M.G.; Strasburg, G.M.; DeWitt, D.L. Antioxidant and cyclooxygenase inhibitory phenolic compounds from Ocimum sanctum Linn. Phytomedicine 2000, 7, 7–13. [Google Scholar] [CrossRef]
- Mondal, S.; Varma, S.; Bamola, V.D.; Naik, S.N.; Mirdha, B.R.; Padhi, M.M.; Mehta, N.; Mahapatra, S.C. Double-blinded randomized controlled trial for immunomodulatory effects of Tulsi (Ocimum sanctum Linn.) leaf extract on healthy volunteers. J. Ethnopharmacol. 2011, 136, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Prakash, P.; Gupta, N. Therapeutic uses of Ocimum sanctum Linn (Tulsi) with a note on eugenol and its pharmacological actions: A short review. Indian J. Physiol. Pharmacol. 2005, 49, 125–131. [Google Scholar] [PubMed]
- Rohdewald, P. A review of the French maritime pine bark extract (Pycnogenol), a herbal medication with a diverse clinical pharmacology. Int. J. Clin. Pharmacol. Ther. 2002, 40, 158–168. [Google Scholar] [CrossRef]
- Packer, L.; Rimbach, G.; Virgili, F. Antioxidant activity and biologic properties of a procyanidin-rich extract from pine (Pinus maritima) bark, pycnogenol. Free Radic. Biol. Med. 1999, 27, 704–724. [Google Scholar] [CrossRef]
- Cho, K.J.; Yun, C.H.; Packer, L.; Chung, A.S. Inhibition mechanisms of bioflavonoids extracted from the bark of Pinus maritima on the expression of proinflammatory cytokines. Ann. N. Y. Acad. Sci. 2001, 928, 141–156. [Google Scholar] [CrossRef]
- Hosseini, S.; Pishnamazi, S.; Sadrzadeh, S.M.H.; Farid, F.; Farid, R.; Watson, R.R. Pycnogenol® in the Management of Asthma. J. Med. Food 2001, 4, 201–209. [Google Scholar] [CrossRef]
- Lau, B.H.; Riesen, S.K.; Truong, K.P.; Lau, E.W.; Rohdewald, P.; Barreta, R.A. Pycnogenol as an adjunct in the management of childhood asthma. J. Asthma 2004, 41, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Kimbrough, C.; Chun, M.; dela Roca, G.; Lau, B.H.S. Pycnogenol® chewing gum minimizes gingival bleeding and plaque formation. Phytomedicine 2002, 9, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Sequeda-Castañeda, L.; Célis, C.; Gutiérrez, S.; Gamboa, F. Piper marginatum jacq.(piperaceae): Phytochemical, therapeutic, botanical insecticidal and phytosanitary uses. Pharmacol. Online 2015, 3, 136–145. [Google Scholar]
- Delgado-Paredes, G.E.; Kato, M.J.; Vásquez-Dueñas, N.; Minchala-Patiño, J.; Rojas-Idrogo, C. Cultivo de tejidos de Piper sp. (Piperaceae): Propagación, organogénesis y conservación de germoplasma in vitro. Rev. Colomb. Biotecnol. 2012, 14, 49–60. [Google Scholar]
- Dueñas, J.F.; Jarrett, C.; Cummins, I.; Logan–Hines, E. Amazonian Guayusa (Ilex guayusa Loes.): A historical and ethnobotanical overview. Econ. Bot. 2016, 70, 85–91. [Google Scholar] [CrossRef]
- Gamboa, F.; Muñoz, C.-C.; Numpaque, G.; Sequeda-Castañeda, L.G.; Gutierrez, S.J.; Tellez, N. Antimicrobial activity of Piper marginatum Jacq and Ilex guayusa Loes on microorganisms associated with periodontal disease. Int. J. Microbiol. 2018, 2018, 4147383. [Google Scholar] [CrossRef]
- Barra, A.; Coroneo, V.; Dessi, S.; Cabras, P.; Angioni, A. Characterization of the volatile constituents in the essential oil of Pistacia lentiscus L. from different origins and its antifungal and antioxidant activity. J. Agric. Food Chem. 2007, 55, 7093–7098. [Google Scholar] [CrossRef]
- Di Rosa, A. Erbe e Piante Medicinali in Sardegna; La Nuova: Sassari, Italy, 2018. [Google Scholar]
- Sakagami, H.; Kishino, K.; Kobayashi, M.; Hashimoto, K.; Iida, S.; Shimetani, A.; Nakamura, Y.; Takahashi, K.; Ikarashi, T.; Fukamachi, H. Selective antibacterial and apoptosis-modulating activities of mastic. In Vivo 2009, 23, 215–223. [Google Scholar]
- Paraschos, S.; Mitakou, S.; Skaltsounis, A.-L. Chios gum mastic: A review of its biological activities. Curr. Med. Chem. 2012, 19, 2292–2302. [Google Scholar] [CrossRef]
- Paraschos, S.; Magiatis, P.; Mitakou, S.; Petraki, K.; Kalliaropoulos, A.; Maragkoudakis, P.; Mentis, A.; Sgouras, D.; Skaltsounis, A.-L. In vitro and in vivo activities of Chios mastic gum extracts and constituents against Helicobacter pylori. Antimicrob. Agents Chemother. 2007, 51, 551–559. [Google Scholar] [CrossRef]
- Sterer, N. Antimicrobial effect of mastic gum methanolic extract against Porphyromonas gingivalis. J. Med. Food 2006, 9, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Kamrani, Y.; Amanlou, M.; Esmaeelian, B.; Bidhendi, S.M.; SahebJamei, M. Inhibitory effects of a flavonoid-rich extract of Pistacia vera hull on growth and acid production of bacteria involved in dental plaque. Int. J. Pharmacol. 2007, 3, 219–226. [Google Scholar]
- Milia, E.; Usai, M.; Szotáková, B.; Elstnerová, M.; Králová, V.; D’Hallewin, G.; Spissu, Y.; Barberis, A.; Marchetti, M.; Bortone, A.; et al. The Pharmaceutical Ability of Pistacia lentiscus L. Leaves Essential Oil Against Periodontal Bacteria and Candida sand Its Anti-Inflammatory Potential. Antibiotics 2020, 9, 281. [Google Scholar] [CrossRef] [PubMed]
- Azeez, S.H.; Gaphor, S.M.; Sha, A.M.; Garib, B.T. Effect of Pistacia atlantica subskurdica Gum in Experimental Periodontitis Induced in Wistar Rats by Utilization of Osteoclastogenic Bone Markers. Molecules 2020, 25, 5819. [Google Scholar] [CrossRef]
- Joseph, B.; Priya, R. Phytochemical and biopharmaceutical aspects of Psidium guajava (L.) essential oil: A review. Res. J. Med. Plants 2011, 5, 432–442. [Google Scholar] [CrossRef]
- Rishika, D.; Sharma, R. An update of pharmacological activity of Psidium guajava in the management of various disorders. Int. J. Pharm. Sci. Res. 2012, 3, 3577. [Google Scholar]
- Prabu, G.; Gnanamani, A.; Sadulla, S. Guaijaverin—A plant flavonoid as potential antiplaque agent against Streptococcus mutans. J. Appl. Microbiol. 2006, 101, 487–495. [Google Scholar] [CrossRef]
- Ushimaru, P.I.; Silva, M.T.N.d.; Di Stasi, L.C.; Barbosa, L.; Fernandes, A., Jr. Antibacterial activity of medicinal plant extracts. Braz. J. Microbiol. 2007, 38, 717–719. [Google Scholar] [CrossRef]
- Joseph, B.; Priya, R.M.; Helen, P.M.; Sujatha, S. Bio-active compounds in essential oil and its effects of antimicrobial, cytotoxic activity from the Psidium guajava (L.) leaf. J. Adv. Biotechnol. 2010, 9, 10–14. [Google Scholar]
- Gashe, F.; Belete, A.; Gebre-Mariam, T. Evaluation of antimicrobial and anti-inflammatory activities and formulation studies on the leaf extracts of Psidium guajava L. Ethiop. Pharm. J. 2010, 28, 131–142. [Google Scholar]
- Tona, L.; Kambu, K.; Ntondele, D.; Cimanga, K. Antimicrobial activity of tannins. Filoterapia 1994, 65, 276–278. [Google Scholar]
- Shu, Y.; Liu, Y.; Li, L.; Feng, J.; Lou, B.; Zhou, X.; Wu, H. Antibacterial activity of quercetin on oral infectious pathogens. Afr. J. Microbiol. Res. 2011, 5, 5358–5361. [Google Scholar]
- Geoghegan, F.; Wong, R.; Rabie, A. Inhibitory effect of quercetin on periodontal pathogens in vitro. Phytother. Res. 2010, 24, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahim, S.; Almagboul, A.; Omer, M.; Elegami, A. Antimicrobial activity of Psidium guajava L. Fitoterapia 2002, 73, 713–715. [Google Scholar] [CrossRef] [PubMed]
- Limsong, J.; Benjavongkulchai, E.; Kuvatanasuchati, J. Inhibitory effect of some herbal extracts on adherence of Streptococcus mutans. J. Ethnopharmacol. 2004, 92, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Brötz-Oesterhelt, H.; Beyer, D.; Kroll, H.-P.; Endermann, R.; Ladel, C.; Schroeder, W.; Hinzen, B.; Raddatz, S.; Paulsen, H.; Henninger, K. Dysregulation of bacterial proteolytic machinery by a new class of antibiotics. Nat. Med. 2005, 11, 1082–1087. [Google Scholar] [CrossRef]
- Esimone, C.; Nworu, C.; Ekong, U.; Iroha, I.; Okolin, C. A case for the use of herbal extracts in oral hygiene: The efficacy of Psidium guajava-based mouthwash formulations. Res. J. Appl. Sci. 2007, 2, 1143–1149. [Google Scholar]
- Kraivaphan, V.; Boonyamanound, L.; Amornchat, C.; Trirantana, T.; Kraivaphan, P. The effect of a mouthrinse containing Psidium guajava leaf extract on gingivitis. J. Dent. Assoc. Thai 1991, 41, 323–328. [Google Scholar]
- Fathilah, A.; Sujata, R.; Norhanom, A.; Adenan, M. Antiproliferative activity of aqueous extract of Piper betle L. and Psidium guajava L. on KB and HeLa cell lines. J. Med. Plants Res. 2010, 4, 987–990. [Google Scholar]
- Kavimani, S.; Ilango, R.; Vertichelvan, T. Anti–Inflammatory activity of volatile oil of Psidium guajava. Anc. Sci. Life 1998, 17, 300. [Google Scholar]
- Kwamin, F.; Gref, R.; Haubek, D.; Johansson, A. Interactions of extracts from selected chewing stick sources with Aggregatibacter actinomycetemcomitans. BMC Res. Notes 2012, 5, 203. [Google Scholar] [CrossRef] [PubMed]
- Joyce, O.; Chinwe, N.; Kwaku, J.; Tabot, P. Psidium guajava’s effect on acute phase protein levels during acute inflammation. Am. J. Pharm.Tech. Res. 2012, 2, 424–433. [Google Scholar]
- Kaileh, M.; Berghe, W.V.; Boone, E.; Essawi, T.; Haegeman, G. Screening of indigenous Palestinian medicinal plants for potential anti-inflammatory and cytotoxic activity. J. Ethnopharmacol. 2007, 113, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Koide, M.; Kinugawa, S.; Takahashi, N.; Udagawa, N. Osteoclastic bone resorption induced by innate immune responses. Periodontology 2000 2010, 54, 235–246. [Google Scholar] [CrossRef]
- Choi, S.Y.; Hwang, J.H.; Park, S.Y.; Jin, Y.J.; Ko, H.C.; Moon, S.W.; Kim, S.J. Fermented guava leaf extract inhibits LPS-induced COX-2 and iNOS expression in Mouse macrophage cells by inhibition of transcription factor NF-κB. Phytother. Res. 2008, 22, 1030–1034. [Google Scholar] [CrossRef]
- Åsman, B.; Bergström, K. Expression of Fc-γ-RIII and fibronectin in peripheral neutrophils with increased response to Fc stimulation in patients with Juvenile periodontitis. Arch. Oral Biol. 1992, 37, 991–995. [Google Scholar] [CrossRef]
- Battino, M.; Bullon, P.; Wilson, M.; Newman, H. Oxidative injury and inflammatory periodontal diseases: The challenge of anti-oxidants to free radicals and reactive oxygen species. Crit. Rev. Oral Biol. Med. 1999, 10, 458–476. [Google Scholar] [CrossRef]
- Figuero, E.; Soory, M.; Cerero, R.; Bascones, A. Oxidant/antioxidant interactions of nicotine, Coenzyme Q10, Pycnogenol and phytoestrogens in oral periosteal fibroblasts and MG63 osteoblasts. Steroids 2006, 71, 1062–1072. [Google Scholar] [CrossRef]
- Carnelio, S.; Khan, S.A.; Rodrigues, G. Definite, probable or dubious: Antioxidants trilogy in clinical dentistry. Br. Dent. J. 2008, 204, 29–32. [Google Scholar] [CrossRef]
- Fasola, T.R.; Oloyede, G.K.; Aponjolosun, B.S. Chemical composition, toxicity and antioxidant activities of essential oils of stem bark of Nigerian species of guava (Psidium guajava Linn.). Excli J. 2011, 10, 34. [Google Scholar]
- Vyas, N.; Tailang, M.; Gavatia, N.P.; Gupta, B.K. Antioxidant potential of Psidium guajava Linn. Int. J. PharmTech Res. 2010, 2, 417–419. [Google Scholar]
- He, Q.; Venant, N. Antioxidant power of phytochemicals fromPsidium guajava leaf. J. Zhejiang Univ. Sci. A 2004, 5, 676–683. [Google Scholar]
- Dakappa, S.S.; Adhikari, R.; Timilsina, S.S.; Sajjekhan, S. A review on the medicinal plant Psidium guajava Linn. (Myrtaceae). J. Drug Deliv. Ther. 2013, 3. [Google Scholar] [CrossRef]
- Oguntibeju, O.O. The biochemical, physiological and therapeutic roles of ascorbic acid. Afr. J. Biotechnol. 2008, 7. [Google Scholar]
- Brown, L.; Jones, D. Handbook of Antioxidants; Marcel Dekker: New York, NY, USA, 1996. [Google Scholar]
- Fernandes, K.P.S.; Bussadori, S.K.; Marques, M.M.; Wadt, N.S.Y.; Bach, E.; Martins, M.D. Healing and cytotoxic effects of Psidium guajava (Myrtaceae) leaf extracts. Braz. J. Oral Sci. 2010, 9, 449–454. [Google Scholar]
- Kumar, P.; Ansari, S.H.; Ali, J. Herbal remedies for the treatment of periodontal disease—A patent review. Recent Pat. Drug Deliv. Formul. 2009, 3, 221–228. [Google Scholar]
- Chapple, I.L. Role of free radicals and antioxidants in the pathogenesis of the inflammatory periodontal diseases. Clin. Mol. Pathol. 1996, 49, M247. [Google Scholar] [CrossRef]
- Mittal, P.; Gupta, V.; Kaur, G.; Garg, A.K.; Singh, A. Phytochemistry and pharmacological activities of Psidium guajava. IJPSR 2010, 1, 9–19. [Google Scholar]
- Salgado, A.D.; Maia, J.L.; Pereira, S.L.; de Lemos, T.L.; Mota, O.M. Antiplaque and antigingivitis effects of a gel containing Punica granatum Linn extract: A double-blind clinical study in humans. J. Appl. Oral Sci. 2006, 14, 162–166. [Google Scholar] [CrossRef]
- Jurenka, J.S. Therapeutic applications of pomegranate (Punica granatum L.): A review. Altern. Med. Rev. 2008, 13, 128–144. [Google Scholar]
- Arun, N.; Singh, D. Punica granatum: A review on pharmacological and therapeutic properties. Int. J. Pharm. Sci. Res. 2012, 3, 1240. [Google Scholar]
- Pereira, J.; Pereira, M.; Higino, J.; Sampio, F.; Alves, P.; Araujo, C. Studies with the extract of the Punica granatum Linn. (Pomegranate): Antimicrobial effect “in vitro” and clinical evaluation of a toothpaste upon microorganisms of the oral biofilm. J. Dent. Sci. 2005, 20, 262–269. [Google Scholar]
- Teniente, S.L.; Flores-Gallegos, A.C.; Esparza-González, S.C.; Campos-Múzquiz, L.G.; Nery-Flores, S.D.; Rodríguez-Herrera, R. Anticancer Effect of Pomegranate Peel Polyphenols against Cervical Cancer. Antioxidants 2023, 12, 127. [Google Scholar] [CrossRef] [PubMed]
- Shukla, M.; Gupta, K.; Rasheed, Z.; Khan, K.A.; Haqqi, T.M. Bioavailable constituents/metabolites of pomegranate (Punica granatum L.) preferentially inhibit COX2 activity ex vivo and IL-1beta-induced PGE2 production in human chondrocytes in vitro. J. Inflamm. 2008, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.G.; Selvasubramanian, S.; Jayasundar, S. Immunomodulatory activity of Punica granatum in rabbits—A preliminary study. J. Ethnopharmacol. 2001, 78, 85–87. [Google Scholar] [CrossRef]
- Ishikawa, I. Host responses in periodontal diseases: A preview. Periodontology 2000 2007, 43, 9–13. [Google Scholar] [CrossRef]
- Bhadbhade, S.J.; Acharya, A.B.; Rodrigues, S.V.; Thakur, S.L. The antiplaque efficacy of pomegranate mouthrinse. Quintessence Int. 2011, 42, 29–36. [Google Scholar]
- Sastravaha, G.; Gassmann, G.; Sangtherapitikul, P.; Grimm, W.D. Adjunctive periodontal treatment with Centella asiatica and Punica granatum extracts in supportive periodontal therapy. J. Int. Acad. Periodontol. 2005, 7, 70–79. [Google Scholar]
- DiSilvestro, R.A.; DiSilvestro, D.J.; DiSilvestro, D.J. Pomegranate extract mouth rinsing effects on saliva measures relevant to gingivitis risk. Phytother. Res. 2009, 23, 1123–1127. [Google Scholar] [CrossRef]
- Nomura, Y.; Tamaki, Y.; Tanaka, T.; Arakawa, H.; Tsurumoto, A.; Kirimura, K.; Sato, T.; Hanada, N.; Kamoi, K. Screening of periodontitis with salivary enzyme tests. J. Oral Sci. 2006, 48, 177–183. [Google Scholar] [CrossRef]
- Närhi, T.O.; Tenovuo, J.; Ainamo, A.; Vilja, P. Antimicrobial factors, sialic acid, and protein concentration in whole saliva of the elderly. Eur. J. Oral Sci. 1994, 102, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Badria, F.A.; Zidan, O.A. Natural products for dental caries prevention. J. Med. Food 2004, 7, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Newman, M.G.; Carranza, F.A.; Takei, H.H.; Klokkevold, P.R. Carranza’s Clinical Periodontology; Elsevier Brasil: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Pereira, J.V.; Silva Filho, S.C.; LS, H.J. Antimicrobial activity of hyroalcoholic extract of Punica granatum Linn. on plaque forming microorganisms. Periodontics Rev. 2001, 12, 57–64. [Google Scholar]
- Pereira, J.V.; Pereira, M.S.V.; Sampaio, F.C.; Sampaio, M.C.C.; Alves, P.M.; Araújo, C.R.; Higino, J.S. In vitro antibacterial and antiadherence effect of the extract of the Punica granatum Linn. upon dental biofilm microrganisms. Rev. Bras. Farmacogn. 2006, 16, 88–93. [Google Scholar] [CrossRef]
- Menezes, S.M.; Cordeiro, L.N.; Viana, G.S. Punica granatum (pomegranate) extract is active against dental plaque. J. Herb. Pharmacother. 2006, 6, 79–92. [Google Scholar] [CrossRef]
- Somu, C.A.; Ravindra, S.; Ajith, S.; Ahamed, M.G. Efficacy of a herbal extract gel in the treatment of gingivitis: A clinical study. J. Ayurveda Integr. Med. 2012, 3, 85–90. [Google Scholar] [CrossRef]
- Mazumdar, M.; Chatterjee, A.; Majumdar, S.; Chandrika, M.; Patki, P. Evaluation of the safety and efficacy of complete care herbal toothpaste in controlling dental plaque, gingival bleeding and periodontal diseases. J. Homeop. Ayurv. Med. 2013, 2, 1000124. [Google Scholar]
- Dye, B.A.; Kruszon-Moran, D.; McQuillan, G. The relationship between periodontal disease attributes and Helicobacter pylori infection among adults in the United States. Am. J. Public Health 2002, 92, 1809–1815. [Google Scholar] [CrossRef]
- Umeda, M.; Kobayashi, H.; Takeuchi, Y.; Hayashi, J.; Morotome-Hayashi, Y.; Yano, K.; Aoki, A.; Ohkusa, T.; Ishikawa, I. High prevalence of Helicobacter pylori detected by PCR in the oral cavities of periodontitis patients. J. Periodontol. 2003, 74, 129–134. [Google Scholar] [CrossRef]
- Gebara, E.C.; Pannuti, C.; Faria, C.M.; Chehter, L.; Mayer, M.P.; Lima, L.A. Prevalence of Helicobacter pylori detected by polymerase chain reaction in the oral cavity of periodontitis patients. Oral Microbiol. Immunol. 2004, 19, 277–280. [Google Scholar] [CrossRef]
- Riggio, M.P.; Lennon, A. Identification by PCR of Helicobacter pylori in subgingival plaque of adult periodontitis patients. J. Med. Microbiol. 1999, 48, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Hajimahmoodi, M.; Shams-Ardakani, M.; Saniee, P.; Siavoshi, F.; Mehrabani, M.; Hosseinzadeh, H.; Foroumadi, P.; Safavi, M.; Khanavi, M.; Akbarzadeh, T.; et al. In vitro antibacterial activity of some Iranian medicinal plant extracts against Helicobacter pylori. Nat. Prod. Res. 2011, 25, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- El-Sherbini, G.T.; Shoukry, N.M. In vitro effect of pomegranate peel extract on Trichomonas tenax. Life Sci. J. 2012, 9, 791–797. [Google Scholar]
- Howell, A.B.; Dsouza, D.H. The pomegranate: Effects on bacteria and viruses that influence human health. Evid.-Based Complement. Altern. Med. 2013, 2013, 606212. [Google Scholar] [CrossRef] [PubMed]
- Bialonska, D.; Ramnani, P.; Kasimsetty, S.G.; Muntha, K.R.; Gibson, G.R.; Ferreira, D. The influence of pomegranate by-product and punicalagins on selected groups of human intestinal microbiota. Int. J. Food Microbiol. 2010, 140, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Stamatova, I.; Meurman, J.H. Probiotics and periodontal disease. Periodontology 2000 2009, 51, 141–151. [Google Scholar] [CrossRef]
- Stamatova, I.; Meurman, J.H. Probiotics: Health benefits in the mouth. Am. J. Dent. 2009, 22, 329–338. [Google Scholar]
- Twetman, S.; Derawi, B.; Keller, M.; Ekstrand, K.; Yucel-Lindberg, T.; Stecksen-Blicks, C. Short-term effect of chewing gums containing probiotic Lactobacillus reuteri on the levels of inflammatory mediators in gingival crevicular fluid. Acta Odontol. Scand. 2009, 67, 19–24. [Google Scholar] [CrossRef]
- Staab, B.; Eick, S.; Knöfler, G.; Jentsch, H. The influence of a probiotic milk drink on the development of gingivitis: A pilot study. J. Clin. Periodontol. 2009, 36, 850–856. [Google Scholar] [CrossRef]
- Braga, L.C.; Leite, A.A.; Xavier, K.G.; Takahashi, J.A.; Bemquerer, M.P.; Chartone-Souza, E.; Nascimento, A.M. Synergic interaction between pomegranate extract and antibiotics against Staphylococcus aureus. Can. J. Microbiol. 2005, 51, 541–547. [Google Scholar] [CrossRef]
- Dey, D.; Debnath, S.; Hazra, S.; Ghosh, S.; Ray, R.; Hazra, B. Pomegranate pericarp extract enhances the antibacterial activity of ciprofloxacin against extended-spectrum β-lactamase (ESBL) and metallo-β-lactamase (MBL) producing Gram-negative bacilli. Food Chem. Toxicol. 2012, 50, 4302–4309. [Google Scholar] [CrossRef]
- Begum, A.; Sandhya, S.; Shaffath Ali, S.; Vinod, K.R.; Reddy, S.; Banji, D. An in-depth review on the medicinal flora Rosmarinus officinalis (Lamiaceae). Acta Sci. Pol. Technol. Aliment. 2013, 12, 61–73. [Google Scholar] [PubMed]
- Satyal, P.; Jones, T.H.; Lopez, E.M.; McFeeters, R.L.; Ali, N.A.; Mansi, I.; Al-Kaf, A.G.; Setzer, W.N. Chemotypic Characterization and Biological Activity of Rosmarinus officinalis. Foods 2017, 6, 20. [Google Scholar] [CrossRef]
- Santoyo, S.; Cavero, S.; Jaime, L.; Ibañez, E.; Señoráns, F.J.; Reglero, G. Chemical composition and antimicrobial activity of Rosmarinus officinalis L. essential oil obtained via supercritical fluid extraction. J. Food Prot. 2005, 68, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Asai, M.; Jeon, S.K.; Iimura, T.; Yonezawa, T.; Cha, B.Y.; Woo, J.T.; Yamaguchi, A. Rosmarinic acid exerts an antiosteoporotic effect in the RANKL-induced mouse model of bone loss by promotion of osteoblastic differentiation and inhibition of osteoclastic differentiation. Mol. Nutr. Food Res. 2015, 59, 386–400. [Google Scholar] [CrossRef] [PubMed]
- Amir Alireza, R.G.; Afsaneh, R.; Seied Hosein, M.S.; Siamak, Y.; Afshin, K.; Zeinab, K.; Mahvash, M.J.; Amir Reza, R. Inhibitory activity of Salvadora persica extracts against oral bacterial strains associated with periodontitis: An in-vitro study. J. Oral Biol. Craniofac. Res. 2014, 4, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Khatak, M.; Khatak, S.; Siddqui, A.A.; Vasudeva, N.; Aggarwal, A.; Aggarwal, P. Salvadora persica. Pharm. Rev. 2010, 4, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Mansour, H.; Alsamadany, H.; Al-Hasawi, Z.M. Genetic diversity and genetic structure of Salvadora persica L., rare plant species in Rabigh province, Saudi Arabia: Implications for conservation. J. Taibah Univ. Sci. 2020, 14, 881–888. [Google Scholar] [CrossRef]
- Haque, M.M.; Alsareii, S.A. A review of the therapeutic effects of using miswak (Salvadora Persica) on oral health. Saudi Med. J. 2015, 36, 530–543. [Google Scholar] [CrossRef]
- Al Bratty, M.; Makeen, H.A.; Alhazmi, H.A.; Syame, S.M.; Abdalla, A.N.; Homeida, H.E.; Sultana, S.; Ahsan, W.; Khalid, A. Phytochemical, Cytotoxic, and Antimicrobial Evaluation of the Fruits of Miswak Plant, Salvadora persica L. J. Chem. 2020, 2020, 4521951. [Google Scholar] [CrossRef]
- Mohamed, S.A.; Khan, J.A. Antioxidant capacity of chewing stick miswak Salvadora persica. BMC Complement. Altern. Med. 2013, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.M.; Al Sahli, A.A.; Alaraidh, I.A.; Al-Homaidan, A.A.; Mostafa, E.M.; El-Gaaly, G.A. Assessment of antioxidant activities in roots of Miswak (Salvadora persica) plants grown at two different locations in Saudi Arabia. Saudi. J. Biol. Sci. 2015, 22, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Lebda, M.A.; El-Far, A.H.; Noreldin, A.E.; Elewa, Y.H.A.; Al Jaouni, S.K.; Mousa, S.A. Protective Effects of Miswak (Salvadora persica) against Experimentally Induced Gastric Ulcers in Rats. Oxid. Med. Cell. Longev. 2018, 2018, 6703296. [Google Scholar] [CrossRef] [PubMed]
- Nordin, A.; Bin Saim, A.; Ramli, R.; Abdul Hamid, A.; Mohd Nasri, N.W.; Bt Hj Idrus, R. Miswak and oral health: An evidence-based review. Saudi J. Biol. Sci. 2020, 27, 1801–1810. [Google Scholar] [CrossRef]
- Hosseini, M.; Vazirian, M.; Nomani, A.; Monsef-Esfahani, H. Evaluation of anti-inflammatory effect of Salvadora persica in IBD-induced rat. Res. J. Pharmacogn. 2017, 4, 27. [Google Scholar]
- Khalil, M.A.; El-Sabbagh, M.S.; El Naggar, E.B.; El-Erian, R.H. Antibacterial activity of Salvadora persica against oral pathogenic bacterial isolates. Niger. J. Clin. Pract. 2019, 22, 1378–1387. [Google Scholar] [CrossRef]
- Arshad, H.; Sami, M.A.; Sadaf, S.; Hassan, U. Salvadora persica mediated synthesis of silver nanoparticles and their antimicrobial efficacy. Sci. Rep. 2021, 11, 5996. [Google Scholar] [CrossRef]
- Abdulbaqi, H.R.; Himratul-Aznita, W.H.; Baharuddin, N.A. Evaluation of Salvadora persica L. and green tea anti-plaque effect: A randomized controlled crossover clinical trial. BMC Complement. Altern. Med. 2016, 16, 493. [Google Scholar] [CrossRef]
- Patel, P.V.; Shruthi, S.; Kumar, S. Clinical effect of miswak as an adjunct to tooth brushing on gingivitis. J. Indian Soc. Periodontol. 2012, 16, 84–88. [Google Scholar] [CrossRef]
- Aspalli, S.; Shetty, V.S.; Devarathnamma, M.V.; Nagappa, G.; Archana, D.; Parab, P. Evaluation of antiplaque and antigingivitis effect of herbal mouthwash in treatment of plaque induced gingivitis: A randomized, clinical trial. J. Indian Soc. Periodontol. 2014, 18, 48–52. [Google Scholar] [CrossRef]
- Bhate, D.; Jain, S.; Kale, R.; Muglikar, S. The comparative effects of 0.12% chlorhexidine and herbal oral rinse on dental plaque-induced gingivitis: A randomized clinical trial. J. Indian Soc. Periodontol. 2015, 19, 393–395. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Agarwal, N.; Anup, N.; Manujunath, B.C.; Bhalla, A. Evaluating the anti-plaque efficacy of meswak (Salvadora persica) containing dentifrice: A triple blind controlled trial. J. Pharm. Bioallied Sci. 2012, 4, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, M.A.; Dodamani, A.S.; Karibasappa, G.; Khairnar, M.R.; Naik, R.G.; Jadhav, H.C. Comparative Evaluation of the Efficacy of Probiotic, Herbal and Chlorhexidine Mouthwash on Gingival Health: A Randomized Clinical Trial. J. Clin. Diagn. Res. 2017, 11, Zc13–Zc16. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K.A.; John, S.; Deepika, V.; Dwijendra, K.S.; Reddy, B.R.; Chincholi, S. Anti-Plaque Efficacy of Herbal and 0.2% Chlorhexidine Gluconate Mouthwash: A Comparative Study. J. Int. Oral Health 2015, 7, 98–102. [Google Scholar] [PubMed]
- Rezaei, S.; Rezaei, K.; Mahboubi, M.; Jarahzadeh, M.H.; Momeni, E.; Bagherinasab, M.; Targhi, M.G.; Memarzadeh, M.R. Comparison the efficacy of herbal mouthwash with chlorhexidine on gingival index of intubated patients in Intensive Care Unit. J. Indian Soc. Periodontol. 2016, 20, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Tadikonda, A.; Pentapati, K.C.; Urala, A.S.; Acharya, S. Anti-plaque and anti-gingivitis effect of Papain, Bromelain, Miswak and Neem containing dentifrice: A randomized controlled trial. J. Clin. Exp. Dent. 2017, 9, e649–e653. [Google Scholar] [CrossRef] [PubMed]
- Mekhemar, M.; Hassan, Y.; Dörfer, C. Nigella sativa and Thymoquinone: A Natural Blessing for Periodontal Therapy. Antioxidants 2020, 9, 1260. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef]
- Albabtain, R.; Azeem, M.; Wondimu, Z.; Lindberg, T.; Borg-Karlson, A.K.; Gustafsson, A. Investigations of a Possible Chemical Effect of Salvadora persica Chewing Sticks. Evid.-Based Complement. Altern. Med. 2017, 2017, 2576548. [Google Scholar] [CrossRef]
- Rafiei, M.; Kiani, F.; Sayehmiri, F.; Sayehmiri, K.; Sheikhi, A.; Zamanian Azodi, M. Study of Porphyromonas gingivalis in periodontal diseases: A systematic review and meta-analysis. Med. J. Islam. Repub. Iran 2017, 31, 62. [Google Scholar] [CrossRef]
- Al-Ayed, M.S.; Asaad, A.M.; Qureshi, M.A.; Attia, H.G.; AlMarrani, A.H. Antibacterial Activity of Salvadora persica L. (Miswak) Extracts against Multidrug Resistant Bacterial Clinical Isolates. Evid.-Based Complement. Altern. Med. 2016, 2016, 7083964. [Google Scholar] [CrossRef] [PubMed]
- Al-sieni, A.I. The antibacterial activity of traditionally used Salvadora persica L. (miswak) and Commiphora gileadensis (palsam) in Saudi Arabia. Afr. J. Tradit. Complement. Altern. Med. 2014, 11, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Abhary, M.; Al-Hazmi, A.-A. Antibacterial activity of Miswak (Salvadora persica L.) extracts on oral hygiene. J. Taibah Univ. Sci. 2016, 10, 513–520. [Google Scholar] [CrossRef]
- Mekhemar, M.; Geib, M.; Kumar, M.; Radha; Hassan, Y.; Dörfer, C. Salvadora persica: Nature’s Gift for Periodontal Health. Antioxidants 2021, 10, 712. [Google Scholar] [CrossRef] [PubMed]
- Faruk, E.M.; Nafea, O.E.; Fouad, H.; Ebrahim, U.F.A.; Hasan, R.A.A. Possible healing effects of Salvadora persica extract (MISWAK) and laser therapy in a rabbit model of a caustic-induced tongue ulcers: Histological, immunohistochemical and biochemical study. J. Mol. Histol. 2020, 51, 341–352. [Google Scholar] [CrossRef]
- Moezizadeh, M.; Javand, F.; Tabatabaei, F.S. Effects of extracts of Salvadora persica on proliferation and viability of human dental pulp stem cells. J. Conserv. Dent. 2015, 18, 315–320. [Google Scholar] [CrossRef]
- Khunkar, S.; Hariri, I.; Alsayed, E.; Linjawi, A.; Khunkar, S.; Islam, S.; Bakhsh, T.A.; Nakashima, S. Inhibitory effect of Salvadora persica extract (Miswak) on collagen degradation in demineralized dentin: In vitro study. J. Dent. Sci. 2021, 16, 208–213. [Google Scholar] [CrossRef]
- Xu, X.; Zheng, L.; Yuan, Q.; Zhen, G.; Crane, J.L.; Zhou, X.; Cao, X. Transforming growth factor-β in stem cells and tissue homeostasis. Bone Res. 2018, 6, 2. [Google Scholar] [CrossRef]
- Checchi, V.; Maravic, T.; Bellini, P.; Generali, L.; Consolo, U.; Breschi, L.; Mazzoni, A. The Role of Matrix Metalloproteinases in Periodontal Disease. Int. J. Environ. Res. Public Health 2020, 17, 4923. [Google Scholar] [CrossRef]
- Hamidpour, R.; Hamidpour, S.; Hamidpour, M.; Shahlari, M.; Sohraby, M. Summer savory: From the selection of traditional applications to the novel effect in relief, prevention, and treatment of a number of serious illnesses such as diabetes, cardiovascular disease, Alzheimer’s disease, and cancer. J. Tradit. Complement. Med. 2014, 4, 140–144. [Google Scholar] [CrossRef]
- Zheng, G.-Q.; Kenney, P.M.; Lam, L.K.T. Sesquiterpenes from clove (Eugenia caryophyllata) as potential anticarcinogenic agents. J. Nat. Prod. 1992, 55, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Wu, C.D. Compounds from Syzygium aromaticum possessing growth inhibitory activity against oral pathogens. J. Nat. Prod. 1996, 59, 987–990. [Google Scholar] [CrossRef] [PubMed]
- Kamatou, G.P.; Vermaak, I.; Viljoen, A.M. Eugenol—From the remote Maluku Islands to the international market place: A review of a remarkable and versatile molecule. Molecules 2012, 17, 6953–6981. [Google Scholar] [CrossRef] [PubMed]
- Pramod, K.; Ansari, S.H.; Ali, J. Eugenol: A natural compound with versatile pharmacological actions. Nat. Prod. Commun. 2010, 5, 1934578X1000501236. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Hung, S.L.; Pai, S.F.; Lee, Y.H.; Yang, S.F. Eugenol suppressed the expression of lipopolysaccharide-induced proinflammatory mediators in human macrophages. J. Endod. 2007, 33, 698–702. [Google Scholar] [CrossRef]
- Bachiega, T.F.; de Sousa, J.P.; Bastos, J.K.; Sforcin, J.M. Clove and eugenol in noncytotoxic concentrations exert immunomodulatory/anti-inflammatory action on cytokine production by murine macrophages. J. Pharm. Pharmacol. 2012, 64, 610–616. [Google Scholar] [CrossRef]
- Thompson, D.; Eling, T. Mechanism of inhibition of prostaglandin H synthase by eugenol and other phenolic peroxidase substrates. Mol. Pharmacol. 1989, 36, 809–817. [Google Scholar]
- Raghavenra, H.; Diwakr, B.T.; Lokesh, B.R.; Naidu, K.A. Eugenol—The active principle from cloves inhibits 5-lipoxygenase activity and leukotriene-C4 in human PMNL cells. Prostaglandins Leukot. Essent. Fat. Acids 2006, 74, 23–27. [Google Scholar] [CrossRef]
- Yadav, A.S.; Bhatnagar, D. Free radical scavenging activity, metal chelation and antioxidant power of some of the Indian spices. Biofactors 2007, 31, 219–227. [Google Scholar] [CrossRef]
- Jirovetz, L.; Buchbauer, G.; Stoilova, I.; Stoyanova, A.; Krastanov, A.; Schmidt, E. Chemical composition and antioxidant properties of clove leaf essential oil. J. Agric. Food Chem. 2006, 54, 6303–6307. [Google Scholar] [CrossRef]
- Yoshimura, M.; Ito, H.; Miyashita, K.; Hatano, T.; Taniguchi, S.; Amakura, Y.; Yoshida, T. Flavonol glucuronides and C-glucosidic ellagitannins from Melaleuca squarrosa. Phytochemistry 2008, 69, 3062–3069. [Google Scholar] [CrossRef] [PubMed]
- Karmakar, S.; Choudhury, M.; Das, A.S.; Maiti, A.; Majumdar, S.; Mitra, C. Clove (Syzygium aromaticum Linn) extract rich in eugenol and eugenol derivatives shows bone-preserving efficacy. Nat. Prod. Res. 2012, 26, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Jagtap, A.; Karkera, S. Potential of the aqueous extract of Terminalia chebula as an anticaries agent. J. Ethnopharmacol. 1999, 68, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Rathinamoorthy, R.; Thilagavathi, G. Terminalia chebula—Review on pharmacological and biochemical studies. Int. J. Pharm. Tech. Res. 2014, 6, 97–116. [Google Scholar]
- Bajaj, N.; Tandon, S. The effect of Triphala and Chlorhexidine mouthwash on dental plaque, gingival inflammation, and microbial growth. Int. J. Ayurveda Res. 2011, 2, 29–36. [Google Scholar] [CrossRef]
- Baliga, M.S.; Meera, S.; Mathai, B.; Rai, M.P.; Pawar, V.; Palatty, P.L. Scientific validation of the ethnomedicinal properties of the Ayurvedic drug Triphala: A review. Chin. J. Integr. Med. 2012, 18, 946–954. [Google Scholar] [CrossRef]
- Kumar, M.S.; Kirubanandan, S.; Sripriya, R.; Sehgal, P.K. Triphala promotes healing of infected full-thickness dermal wound. J. Surg. Res. 2008, 144, 94–101. [Google Scholar] [CrossRef]
- Prabhakar, J.; Senthilkumar, M.; Priya, M.S.; Mahalakshmi, K.; Sehgal, P.K.; Sukumaran, V.G. Evaluation of antimicrobial efficacy of herbal alternatives (Triphala and green tea polyphenols), MTAD, and 5% sodium hypochlorite against Enterococcus faecalis biofilm formed on tooth substrate: An in vitro study. J. Endod. 2010, 36, 83–86. [Google Scholar] [CrossRef]
- Naiktari, R.S.; Gaonkar, P.; Gurav, A.N.; Khiste, S.V. A randomized clinical trial to evaluate and compare the efficacy of triphala mouthwash with 0.2% chlorhexidine in hospitalized patients with periodontal diseases. J. Periodontal Implant. Sci. 2014, 44, 134–140. [Google Scholar] [CrossRef]
- Maurya, D.; Mittal, N.; Sharma, K.; Nath, G. Role of triphala in the management of Periodontal disease. Anc. Sci. Life 1997, 17, 120–127. [Google Scholar]
- Yamanaka-Okada, A.; Sato, E.; Kouchi, T.; Kimizuka, R.; Kato, T.; Okuda, K. Inhibitory effect of cranberry polyphenol on cariogenic bacteria. Bull. Tokyo Dent. Coll. 2008, 49, 107–112. [Google Scholar] [CrossRef]
- Bodet, C.; Chandad, F.; Grenier, D. Anti-inflammatory activity of a high-molecular-weight cranberry fraction on macrophages stimulated by lipopolysaccharides from periodontopathogens. J. Dent. Res. 2006, 85, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Bodet, C.; Chandad, F.; Grenier, D. Cranberry components inhibit interleukin-6, interleukin-8, and prostaglandin E2 production by lipopolysaccharide-activated gingival fibroblasts. Eur. J. Oral Sci. 2007, 115, 64–70. [Google Scholar] [CrossRef] [PubMed]
- La, V.; Howell, A.; Grenier, D. Cranberry proanthocyanidins inhibit MMP production and activity. J. Dent. Res. 2009, 88, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Tipton, D.A.; Babu, J.P.; Dabbous, M.K. Effects of cranberry components on human aggressive periodontitis gingival fibroblasts. J. Periodontal Res. 2013, 48, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, S.; Santos, J.; La, V.D.; Howell, A.B.; Grenier, D. A-type cranberry proanthocyanidins inhibit the RANKL-dependent differentiation and function of human osteoclasts. Molecules 2011, 16, 2365–2374. [Google Scholar] [CrossRef] [PubMed]
- Nawrot-Hadzik, I.; Matkowski, A.; Kubasiewicz-Ross, P.; Hadzik, J. Proanthocyanidins and Flavan-3-ols in the Prevention and Treatment of Periodontitis—Immunomodulatory Effects, Animal and Clinical Studies. Nutrients 2021, 13, 239. [Google Scholar] [CrossRef]
- Otegui, I.; Fernández-Quintela, A.; Diego, A.D.; Cid, C.; Macarulla, M.T.; Partearroyo, M.A. Properties of spray-dried and freeze-dried faba bean protein concentrates. Int. J. Food Sci. Technol. 1997, 32, 439–443. [Google Scholar] [CrossRef]
- Baginsky, C.; Peña-Neira, Á.; Cáceres, A.; Hernández, T.; Estrella, I.; Morales, H.; Pertuzé, R. Phenolic compound composition in immature seeds of fava bean (Vicia faba L.) varieties cultivated in Chile. J. Food Compos. Anal. 2013, 31, 1–6. [Google Scholar] [CrossRef]
- Liu, Y.; Wu, X.; Hou, W.; Li, P.; Sha, W.; Tian, Y. Structure and function of seed storage proteins in faba bean (Vicia faba L.). 3 Biotech 2017, 7, 74. [Google Scholar] [CrossRef]
- Warsame, A.O.; O’Sullivan, D.M.; Tosi, P. Seed Storage Proteins of Faba Bean (Vicia faba L): Current Status and Prospects for Genetic Improvement. J. Agric. Food Chem. 2018, 66, 12617–12626. [Google Scholar] [CrossRef] [PubMed]
- Arogundade, L.A.; Tshay, M.; Shumey, D.; Manazie, S. Effect of ionic strength and/or pH on Extractability and physico-functional characterization of broad bean (Vicia faba L.) Protein concentrate. Food Hydrocoll. 2006, 20, 1124–1134. [Google Scholar] [CrossRef]
- Mejri, F.; Selmi, S.; Martins, A.; Benkhoud, H.; Baati, T.; Chaabane, H.; Njim, L.; Serralheiro, M.L.M.; Rauter, A.P.; Hosni, K. Broad bean (Vicia faba L.) pods: A rich source of bioactive ingredients with antimicrobial, antioxidant, enzyme inhibitory, anti-diabetic and health-promoting properties. Food Funct. 2018, 9, 2051–2069. [Google Scholar] [CrossRef] [PubMed]
- Lewis, W.; Elvin-Lewis, M. Oral Hygiene, Medical Botany; John Willy and Sons: New York, NY, USA, 1977. [Google Scholar]
- Xia, E.-Q.; Deng, G.-F.; Guo, Y.-J.; Li, H.-B. Biological activities of polyphenols from grapes. Int. J. Mol. Sci. 2010, 11, 622–646. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Tsao, R. Dietary polyphenols, oxidative stress and antioxidant and anti-inflammatory effects. Curr. Opin. Food Sci. 2016, 8, 33–42. [Google Scholar] [CrossRef]
- Daglia, M. Polyphenols as antimicrobial agents. Curr. Opin. Biotechnol. 2012, 23, 174–181. [Google Scholar] [CrossRef]
- Esteban-Fernandez, A.; Zorraquin-Pena, I.; de Llano, D.G.; Bartolome, B.; Moreno-Arribas, M.V. The role of wine and food polyphenols in oral health. Trends Food Sci. Technol. 2017, 69, 118–130. [Google Scholar] [CrossRef]
- Pizzorno, J.E.; Murray, M.T.; Joiner-Bey, H. The Clinician’s Handbook of Natural Medicine E-Book; Elsevier Health Sciences: London, UK, 2016. [Google Scholar]
- Furiga, A.; Lonvaud-Funel, A.; Badet, C. In vitro study of antioxidant capacity and antibacterial activity on oral anaerobes of a grape seed extract. Food Chem. 2009, 113, 1037–1040. [Google Scholar] [CrossRef]
- Rizzo, A.; Bevilacqua, N.; Guida, L.; Annunziata, M.; Carratelli, C.R.; Paolillo, R. Effect of resveratrol and modulation of cytokine production on human periodontal ligament cells. Cytokine 2012, 60, 197–204. [Google Scholar] [CrossRef]
- Zare Javid, A.; Hormoznejad, R.; Yousefimanesh, H.A.; Zakerkish, M.; Haghighi-zadeh, M.H.; Dehghan, P.; Ravanbakhsh, M. The impact of resveratrol supplementation on blood glucose, insulin, insulin resistance, triglyceride, and periodontal markers in type 2 diabetic patients with chronic periodontitis. Phytother. Res. 2017, 31, 108–114. [Google Scholar] [CrossRef]
- Bonifait, L.; Grenier, D. Cranberry polyphenols: Potential benefits for dental caries and periodontal disease. J. (Can. Dent. Assoc.) 2010, 76, a130. [Google Scholar] [PubMed]
- Gewali, M.B.; Awale, S. Aspects of Traditional Medicine in Nepal; Institute of Natural Medicine University of Toyama: Toyama, Japan, 2008; pp. 140–142. [Google Scholar]
- Patiño, L.O.J.; Prieto, R.J.A.; Cuca, S.L.E. Zanthoxylum genus as potential source of bioactive compounds. Bioact. Compd. Phytomed. 2012, 10, 184–218. [Google Scholar]
- Ocheng, F.; Bwanga, F.; Joloba, M.; Borg-Karlson, A.-K.; Gustafsson, A.; Obua, C. Antibacterial activities of extracts from Ugandan medicinal plants used for oral care. J. Ethnopharmacol. 2014, 155, 852–855. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Prakash, S.; Radha; Kumari, N.; Pundir, A.; Punia, S.; Saurabh, V.; Choudhary, P.; Changan, S.; Dhumal, S.; et al. Beneficial Role of Antioxidant Secondary Metabolites from Medicinal Plants in Maintaining Oral Health. Antioxidants 2021, 10, 1061. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, H.M.; Kalsi, V. A review on medicinal properties of zanthoxylum armatum DC. Res. J. Pharm. Technol. 2018, 11, 2131–2138. [Google Scholar] [CrossRef]
- Negi, J.S.; Bisht, V.; Bhandari, A.; Bisht, R.; Kandari Negi, S. Major constituents, antioxidant and antibacterial activities of Zanthoxylum armatum DC. essential oil. Iran. J. Pharmacol. Ther. 2012, 11, 68. [Google Scholar]
- Abuajah, C.I.; Ogbonna, A.C.; Osuji, C.M. Functional components and medicinal properties of food: A review. J. Food Sci. Technol. 2015, 52, 2522–2529. [Google Scholar] [CrossRef]
- Shidfar, F.; Rajab, A.; Rahideh, T.; Khandouzi, N.; Hosseini, S.; Shidfar, S. The effect of ginger (Zingiber officinale) on glycemic markers in patients with type 2 diabetes. J. Complement. Integr. Med. 2015, 12, 165–170. [Google Scholar] [CrossRef]
- Srinivasan, K. Ginger rhizomes (Zingiber officinale): A spice with multiple health beneficial potentials. PharmaNutrition 2017, 5, 18–28. [Google Scholar] [CrossRef]
- Mahyari, S.; Mahyari, B.; Emami, S.A.; Malaekeh-Nikouei, B.; Jahanbakhsh, S.P.; Sahebkar, A.; Mohammadpour, A.H. Evaluation of the efficacy of a polyherbal mouthwash containing Zingiber officinale, Rosmarinus officinalis and Calendula officinalis extracts in patients with gingivitis: A randomized double-blind placebo-controlled trial. Complement. Ther. Clin. Pract. 2016, 22, 93–98. [Google Scholar] [CrossRef]
- Hassen, G.; Belete, G.; Carrera, K.G.; Iriowen, R.O.; Araya, H.; Alemu, T.; Solomon, N.; Bam, D.S.; Nicola, S.M.; Araya, M.E.; et al. Clinical Implications of Herbal Supplements in Conventional Medical Practice: A US Perspective. Cureus 2022, 14, e26893. [Google Scholar] [CrossRef] [PubMed]
- Ekor, M. The growing use of herbal medicines: Issues relating to adverse reactions and challenges in monitoring safety. Front. Pharmacol. 2014, 4, 177. [Google Scholar] [CrossRef] [PubMed]
- Del Prete, A.; Scalera, A.; Iadevaia, M.D.; Miranda, A.; Zulli, C.; Gaeta, L.; Tuccillo, C.; Federico, A.; Loguercio, C. Herbal Products: Benefits, Limits, and Applications in Chronic Liver Disease. Evid.-Based Complement. Altern. Med. 2012, 2012, 837939. [Google Scholar] [CrossRef] [PubMed]
- Stickel, F.; Patsenker, E.; Schuppan, D. Herbal hepatotoxicity. J. Hepatol. 2005, 43, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Abebe, W. Herbal medication: Potential for adverse interactions with analgesic drugs. J. Clin. Pharm. Ther. 2002, 27, 391–401. [Google Scholar] [CrossRef]















| Natural Compound | Study Type | Samples Studied | Methods | Result(s)/Conclusion(s) | Limitations | Ref./Year |
|---|---|---|---|---|---|---|
| Acacia arabica | RCT | Nc: 40 Ns: 40 [Patients with mild–moderate periodontitis] | Gc: SRP + placebo Gs: SRP + Acacia arabica [PD and CAL were compared at baseline and after 15 and 90 days] | Acacia arabica’s antiplaque and antigingivitis properties were significantly valuable (p < 0.05). A reduction in sites with moderate PD was observed more among Gs than Gc (p = 0.001). The treatment may be prescribed with SRP for mild to moderate chronic periodontitis. | 1. No assessment of bone defect fill. 2. Short follow-up period. | [56]/2018 |
| RCT | Nc: 30 Ns: 30 [Patients with gingivitis] | Gc: Regular toothpaste Gs: Toothpaste containing Acacia arabica [PI, GI, and BOP were compared at the baseline and after 28 days] | Gs showed statistically significantly better results regarding PI, GI, and BOP (p < 0.001). Gingivitis may be prevented with toothpaste that contains Acacia arabica. Using it daily can help improve oral health. | Not assessing the combination therapy using herbal toothpastes and mouthwashes. | [156]/2012 | |
| Allium sativum | RCT | Nc: 100 Ns: 100 [Patients with mild–moderate periodontitis] | Gc: Placebo tablets Gs: Tablets containing 300 mg of AGE powder [Subjects were examined at the start and 12 and 18 months post-op. GR and PD were measured] | The mean value of pocket depth was 1.06 ± 0.49 in comparison with the baseline value of 1.89 ± 0.74 (p < 0.001). The corresponding value was 1.50 ± 0.46 for the placebo group (p < 0.001). Periodontal disease can be prevented or improved with aged garlic extract. | Not determining the exact dosage, required duration of usage, or the principal mode of action. | [83]/2020 |
| Aloe barbadensis Miller | RCT | N1: 10 N2: 10 [Patients with gingivitis] | G1: First, Aloe vera toothpaste for 14 days, then fluoride toothpaste for another 14 days G2: First, fluoride toothpaste for 14 days, then Aloe vera toothpaste for another 14 days [PI and GI were assessed] | PI was 2.14 ± 1.3 at baseline and 1.84 ± 1.02 at 30 days (p < 0.098). GI was 0.62 ± 0.74 at baseline and 0.25 ± 0.46 at 30 days (p < 0.068). In comparison with fluoride toothpaste, Aloe vera toothpaste had similar effects on PI and GI, and it seems that it can be used as an alternative. | 1. Small sample size 2. Short follow-up period | [157]/2021 |
| RCT | Nc: 20 Ns: 20 [Patients with chronic periodontitis] | Gc: SRP Gs: SRP + Aloe vera gel [GI, PI, and PD were evaluated at baseline and after 15 and 30 days] | The mean reduction in GI: baseline day, 1.98 ± 0.10; 15 days, 1.6 ± 0.10; 30 days, 1.05 ± 0.10. After and before treatment measurements. Aloe vera treatment significantly reduced PI. The plaque index was meaningfully decreased from 2.15 ± 0.271 to 1.60 ± 0.34 after 30 days. Periodontitis significantly decreased in areas treated with Aloe vera gel. | 1. Small sample size 2. Short follow-up period | [158]/2019 | |
| RCT | Nc: 18 Ns: 18 [Healthy individuals] | Gc: Close-up tooth gel Gs: Aloe vera tooth gel [After 3 weeks, PI and GI were measured at baseline] | It was demonstrated that toothpaste containing Aloe vera significantly improved GI and PI; the results were similar to those achieved with tooth gel applied close up. | 1. Small sample size 2. Short follow-up period | [159]/2018 | |
| RCT | N1: 130 N2: 130 N3: 130 [Patients with PI > 1.9, and GI > 1.1] | G1: Aloe vera mouthwash G2: CHX mouthwash G3: Placebo [GI and PI were measured at baseline and after 15 and 30 days] | Compared to the CHX and Aloe vera groups, all parameters presented considerable reductions (p < 0.05). Neither Aloe vera nor CHX presented a significant difference (p < 0.05). Aloe vera and placebo and CHX and placebo had significantly different mean PI and GI scores (p < 0.000). | Short follow-up period | [160]/2016 | |
| RCT | N1: 30 N2: 30 N3: 30 [Healthy individuals] | G1: Aloe vera mouthwash G2: CHX mouthwash G3: Placebo (normal saline) [After 15 and 30 days, GI and PI were evaluated at baseline] | Both Aloe vera and CHX significantly reduced plaque and gingivitis. There was no statistically significant difference between groups (p > 0.05). CHX mouthwash can be replaced with Aloe vera as an affordable and suitable alternative. | 1. Small sample size 2. Short follow-up period | [161]/2016 | |
| RCT | N1: 30 N2: 30 N3: 30 [Patients with visible plaque and gingivitis in at least 30% of their teeth] | G1: Aloe vera mouthwash G2: Chlorine dioxide mouthwash G3: CHX mouthwash [GI and PI were evaluated at baseline and after 15 days] | At follow-up, all three groups had significantly lower plaque and gingival scores than at baseline (p < 0.001). In comparison with Aloe vera, CHX significantly reduced PI and GI (p < 0.05). | 1. Small sample size 2. Short follow-up period | [162]/2016 | |
| RCT | N1: 30 N2: 30 N3: 30 [Patients with periodontitis] | G1: 0.2% CHX mouthwash G2: Green tea–Aloe vera mouthwash G3: Distilled water [After 14 days, GI, BI, and PI were evaluated at baseline] | G1, G2, and G3 reduced the PI by 0.17 ± 0.14, 0.10 ± 0.08, and 0.02 ± 0.18, respectively (p = 0.008). Between G1 and G2 with G3 were a significant difference. BIs between these three groups were significantly different, with p = 0.001 between G2 and G1 with G3. Periodontal health was improved by green tea–Aloe vera mouthwash. This can lead to improved dental and oral health. | 1. Small sample size 2. Short follow-up period | [163]/2016 | |
| RCT | N1: 115 N2: 115 N3: 115 [Healthy individuals with baseline DMFT index of 2.5 to 5 and baseline PI > 1.5] | G1: Mouthwash containing Aloe vera G2: CHX mouthwash G3: Placebo mouthwash [After 15 and 30 days, GI and PI were evaluated at baseline and] | CHX and Aloe vera groups reduced plaque and gingivitis significantly, but there was no statistically significant difference (p > 0.05). The ability of Aloe vera to reduce periodontal indexes makes it an effective mouthwash. | Short follow-up period | [164]/2014 | |
| RCT | N1: 40 N2: 40 N3: 40 [Healthy individuals] | G1: 100% Aloe vera mouthwash G2: CHX mouthwash G3: Placebo mouthwash [At 7, 14, and 22 days, GI, BI, and PI were evaluated at baseline] | The PI, GI, and BI scores of G1 and G2 decreased statistically significantly after rinse regimens were initiated compared with G3. Aloe vera mouthwash significantly decreased gingivitis and plaque, but not as much as CHX. | 1. Canceling regular oral hygiene was an inconvenient and embarrassing prerequisite in this mouth rinse study. 2. Short follow-up period | [100]/2012 | |
| RCT | Nc: 20 Ns: 20 [Patients with chronic periodontitis] | Gc: SRP Gs: SRP + local administration of Aloe vera gel [GI, PI, and PD were measured at baseline and after 30 and 60 days] | There was no statistically significant difference between the control and experimental groups in PI in any of the three stages. Both groups treated with SRP combined with Aloe vera or SRP indicated substantial improvement in all 3 stages regarding GI and PD. As a result, Gs had significantly lower GI than the control group (p = 0.0001) and PD (p = 0.009). | 1. Small sample size 2. Short follow-up period | [165]/2017 | |
| Berberis vulgaris | RCT | N1: 25 N2: 10 N3: 10 [Patients were healthy dormitory students] | G1: Barberry gel G2: Placebo gel without an active ingredient G3: Colgate® antiplaque toothpaste [GI and PI were measured at baseline and after 21 days] | Between placebo and barberry gel groups, Colgate® and placebo groups, there were significant differences in PI and GI (p < 0.01). However, there was no statistically significant difference between barberry and Colgate® groups. By applying barberry dental gel, school-aged children can effectively control microbial plaque and gingivitis. | 1. Lack of randomization 2. Small sample size 3. Lack of blinding 4. Short follow-up period | [166]/2007 |
| Camellia sinensis | RCT | Nc: 15 Ns: 15 [Patients with generalized gingivitis] | Gc: Full-mouth prophylaxis Gs: Green tea extract and oral lycopene for 45 days + oral prophylaxis. [BI, salivary UA, and PI levels were measured at baseline and after 45 days] | After treatment, a comparison of the test and control groups revealed statistically significant results in BI (p ≤ 0.001), salivary UA levels (p ≤ 0.01), and PI (p ≤ 0.001). Gingivitis can be treated with lycopene and green tea extract as adjunctive prophylactic and therapeutic methods. | 1. Small sample size 2. Short follow-up period | [167]/2019 |
| RCT | Nc: 15 Ns: 15 [Patients with chronic periodontitis] | Gc: No intervention Gs: Green tea herbal [After six weeks, BI, PI, and PD were evaluated at baseline] | Before and after SRP, both groups presented significant reductions in PD and BI; the intervention group presented a greater reduction (p = 0.003 and 0.031, respectively). The effect of reducing PI between the two groups was not significant, despite being significant within each group (p = 0.135). According to this study, green tea herbal may effectively treat periodontal diseases and improve the benefits of phase I periodontal therapy. | 1. Lack of blinding 2. Small sample size 3. Lack of randomization 4. Short follow-up period | [168]/2018 | |
| RCT | Nc: 20 Ns: 20 [Patients with a gingival index ≥ 1] | Gc: 0.12% CHX mouthwash Gs: Green tea mouthwash with 1% tannin [BI, PI, GI, and staining were measured at baseline and after one and four weeks] | After 1 and 4 weeks, significant differences were detected between groups, but not between groups, in all indices (p < 0.0001). Significantly less tooth staining was observed with the test mouthwash than with the control mouthwash. An adjunct to mechanical plaque reduction could be 1% tannin green tea mouthwash. | 1. Small sample size 2. Observation bias (Hawthorne effect) 3. Short follow-up period | [169]/2017 | |
| RCT | Nc: 22 Ns: 23 [Patients with marginal gingivitis] | Gc: Placebo gum Gs: Chewing gum containing green tea [BI, PI, and salivary IL-1β were measured at baseline and after 7 and 21 days] | There was a significant impact of chewing gum on BI and PI (p < 0.001). BI and PI mean changes at different observation periods were significantly different between the two groups (p < 0.001). Chewing gum had a significant effect on IL-1 β (p < 0.001). A significant difference in mean IL-1 β changes within 1–21 days was not observed (p = 0.086). | 1. Small sample size 2. Short follow-up period | [170]/2016 | |
| RCT | Nc: 55 Ns: 55 [Patients with PI and GI of at least 1.5 and 1, respectively] | Gc: Placebo mouthwash Gs: Mouthwash containing 2% green tea [GI and PI were measured at baseline and after 28 days] | Between baseline and 28 days, mean GI and PI scores decreased significantly among the test group, but not in the control group (p < 0.05). GI scores in the test group (0.67 ± 0.22) were statistically significantly reduced as compared with the control group (0.05 ± 0.11), and PI scores (1.65 ± 0.68) were statistically significantly reduced as compared to the control group (0.45 ± 0.99). | 1. Short follow-up period 2. Small sample size | [171]/2015 | |
| RCT | N1: 20 N2: 20 N3: 20 [Patients were healthy dormitory students] | G1: 0.2% CHX G2: 0.05% sodium fluoride G3: 0.5% Camellia sinensis extract [Salivary pH, PI, GI, and OHI scores were measured at baseline and after one and two weeks] | The experimental groups showed a reduction in mean PI and GI over the 2-week trial period. In all groups, antiplaque effectiveness was highest in G3 (p < 0.05). G1 and G3 were more effective than sodium fluoride at cleaning gingiva (p < 0.05). As compared to G1, the salivary pH increased in G2 and G3. In G1 and G3, the improvement in oral hygiene was more apparent. Due to its minimal side effects and prophylactic benefits, Camellia sinensis can be utilized as an adjunct to oral self-care. | 1. Small sample size 2. Short follow-up period | [172]/2015 | |
| RCT | Nc: 25 Ns: 25 [Patients with chronic gingivitis] | Gc: Normal saline Gs: Mouthwash containing 5% green tea [After five weeks, GI, PI, and BI were measured at baseline] | The periodontal indices showed significant improvement throughout this study (p < 0.001). The changing alteration patterns of indices were contrasted between two groups (p < 0.05). Even though the mouthwash group showed a greater overall improvement, the differences did not reach statistical significance (p > 0.05, observed power for GI: 0.09, PI: 0.11, and BI: 0.07). Green tea mouthwash is effective and safe for treating inflammatory periodontal diseases. | 1. Short follow-up period 2. Small sample size | [173]/2012 | |
| RCT | Nc: 10 Ns: 10 [Patients with chronic periodontitis] | Gc: SRP Gs: SRP + green tea catechin application [GI, PI, and PD were measured at baseline and after one and five weeks. After subgingival plaque sampling, red-complex bacteria were studied via PCR] | Between baseline and 1 week and baseline and 5 weeks, both study and control groups showed significant differences in PD, GI, and PI and substantial reductions in red-complex organisms. (p < 0.001). PD, PI, and GI did not show statistically significant intergroup differences. In Gs, T. forsythus was significantly reduced at one week and five weeks and P. gingivalis was significantly reduced at one week compared to Gc. Chronic periodontitis can be effectively treated with green tea catechins in combination with SRP. | 1. Short follow-up period 2. Split-mouth design 3. Small sample size | [174]/2013 | |
| Citrus sinensis | RCT | Nc: 10 Ns: 10 [Patients with moderate-severe gingivitis] | Gc: 2% CHX mouthwash Gs: Citrus sinensis (4% ethanolic extract) mouthwash [GI, PI, and BI were measured at baseline and after 7 and 14 days] | A mouthwash containing citrus sinensis 4% reduced PI (p = 0.095) as well as a mouthwash containing CHX 0.2% and BI (p = 0.42). However, the extract was more efficient in lowering GI (p = 0.04). | 1. Lack of blinding 2. Small sample size 3. Lack of randomization 4. Short follow-up period | [109]/2018 |
| Curcuma longa | RCT | Nc: 15 Ns: 15 [Patients with chronic periodontitis] | Gc: SRP + CHX gel Gs: SRP + curcumin gel [After 30 and 45 days, GI, PI, BI, and PD were evaluated at baseline] | A significant difference in PI, PD, BI, and GI was found between Gs and Gc (p < 0.001). SRP can be administered with the control and experimental gel, but curcumin gel performed better than CHX gel in reducing periodontal pockets in mild to moderate cases. | 1. Short follow-up period 2. Lack of microbiological evaluations 3. Small sample size | [175]/2016 |
| Pilot Study | Ten patients with severe gingivitis | Curcuma gel was consumed orally by the subjects for 21 days; BI was measured after three weeks | Statistical significance was found in the results (p < 0.001). By reducing gingival inflammation, Curcuma longa extract gel was effective. | 1. Short follow-up period 2. Pilot study 3. Small sample size | [176]/2014 | |
| Garcinia mangostana | RCT | Nc: 25 Ns: 25 [Patients with generalized chronic periodontitis] | Gc: SRP + placebo gel Gs: mangostana gel + SRP [At baseline and after three months, PI, BI, PD, CAL, and red-complex bacteria were evaluated] | Between baseline and three months after the study began, Gs had significantly lower PD, CAL, BI, PI, and Treponema denticola values than the placebo group (p ≤ 0.05). | 1. Small sample size 2. Short follow-up period | [177]/2017 |
| Glycyrrhiza glabra | RCT | Nc: 52 Ns: 52 [Patients with mild–moderate periodontitis] | Gc: No intervention Gs: 10% G. glabra gum paint [GI, PD, and CAL were evaluated at baseline and after four weeks] | Patients in the study group showed significant improvements in their periodontal health. G. glabra prevented periodontal diseases. | 1. Small sample size 2. Short follow-up period | [178]/2019 |
| Juglans regia | RCT | N: 20 [Patients with mild gingivitis] | 2% and 3% ether extracts of Juglans regia, 2% and 3% petroleum extracts of Juglans regia, 2% water-soluble extract of Juglans regia, and propylene glycol vehicles were evaluated. [PI was measured at baseline and after three days] | There was 32.12% and 31.56% antiplaque activity in 2% and 3% ether fractions of Juglans regia, respectively. Inhibition of plaque was observed in 30.32% of cases with the 2% aqueous solution of Juglans regia, and in 17.62% and 19.45% of cases with the 2% and 3% petroleum ether fractions. A high level of statistical significance was found in all the findings. The researchers concluded that Juglans regia could be used as an adjunct to oral hygiene regimens since it displayed potent anti-plaque properties. | 1. Small sample size 2. Short follow-up period | [179]/2009 |
| Lippia sidoides | RCT | N1: 10 N2: 10 N3: 10 [Healthy individuals] | G1: Lippia sidoides EO G2: CHX G3: Placebo [PI and BI were measured at baseline and after three months] | In the test groups, plaque and gingivitis were significantly reduced (p < 0.05), Statistically, there was no significant differences (p > 0.05). Gel preparations containing Lippia sidoides essential oil were effective against plaque and gingivitis. | 1. Small sample size 2. Short follow-up period | [180]/2013 |
| RCT | Nc: 28 Ns: 27 [Patients with PI and GI of at least 1.5 and 1, respectively] | G1: CHX mouthwash G2: Lippia sidoides EO mouthwash [PI, BI, GI, and salivary S. mutans colony counts were measured at baseline and after 7 and 30 days] | Clinical and microbiological parameters were significantly reduced by both mouth rinses. Both groups showed no significant differences (p > 0.05). Both groups had considerable reductions in the number of colonies of S. mutans (p < 0.05). Although CHX treatment reduced more efficiently than L. sidoides, there was no statistical difference between the two groups, and both treatments reduced the bacteria equally (p = 0.3). The results of this study demonstrate that Lippia sidoides EO mouth rinses reduce gingival inflammation and microbial plaque. | 1. Small sample size 2. Short follow-up period | [181]/2009 | |
| Mangifera indica | RCT | Nc: 10 Ns: 10 [Healthy individuals] | Gc: CHX mouthwash Gs: Mango leaf mouthwash [After five days, PI, GI, and salivary S. mutans, S. mitis, and S. salivarius counts were evaluated at baseline] | Mango leaf and CHX mouthwashes significantly reduced the microbial count and improved gingival health and plaque control, with CHX showing a greater reduction in the microbial count and better plaque control. | 1. Small sample size 2. Short follow-up period | [182]/2017 |
| Manuka honey | RCT | N1: 7 N2: 7 N3: 6 [Orthodontic patients] | G1: Honey G2: 10% sucrose G3: 10% sorbitol [Plaque pH, bacterial count, and antibacterial properties of honey against S. mutans, L. acidophilus, and P. gingivalis were measured at baseline and after 2, 5, 10, 20, and 30 min] | As compared to sorbitol, honey and sucrose had significantly different plaque pH values (p ≤ 0.001). Honey was the only substance that significantly reduced pH after 30 min of exposure, despite sucrose, sorbitol, and honey significantly reducing bacteria recovery (p < 0.001). There was a significant decrease in the growth of all bacterial strains when honey was added (p ≤ 0.001). By applying honey topically, pH can be modified, bacteria counts can be reduced, and bacterial growth can be inhibited. | 1. No follow-up 2. Small sample size | [183]/2014 |
| Pilot study | Nc: 15 Ns: 15 [Healthy individuals] | Gc: Sugar-free chewing gum Gs: Manuka honey products [PI and GI were measured at baseline and after 21 days] | Manuka honey reduced plaque scores and bleeding sites (48% reduced to 17%; p = 0.001) statistically significantly compared to the control group. The results suggest that manuka honey may have therapeutic potential in treating gingivitis and periodontitis. | 1. Short follow-up period 2. Pilot study 3. Small sample size | [184]/2004 | |
| Matricaria chamomilla | RCT | N1: 25 N2: 25 N3: 25 [Patients with chronic periodontitis] | G1: SRP + placebo G2: 0.12% CHX + SRP G3: 1% Matricaria chamomilla mouthwash + SRP [PI, BI, GI, PD, CAL, GR, stain index, and microbial colony counts were measured at baseline and after six weeks and three months] | All parameters (except GR in the placebo group) changed significantly between baseline and three months. Compared to the placebo group, meditative mouth rinses containing chamomilla exhibited significant benefits. In comparison to baseline, the CHX rinse resulted in slightly higher improvements in both PD (3.68 mm vs. 3.36 mm) and CAL (3.00 mm vs. 2.72 mm) than CHX rinse. Non-surgical periodontal therapy for chronic periodontitis can use Matricaria chamomilla as an adjunct to CHX mouthwash. | 1. Small sample size 2. Short follow-up period | [185]/2020 |
| Pilot study | N1: 10 N2: 10 N3: 10 [Orthodontic patients with fixed appliances] | G1: Placebo G2: 0.12% CHX G3: 1% Matricaria chamomilla mouthwash [PI and BI were measured at baseline and after 15 days] | G1 exhibited increases in PI and BI (10.2% and 23.1%, respectively). The PI and BI levels in G3(−25.6% and −29.9%, respectively) and G2 (−39.9% and −32.0%, respectively) were considerably lower than those in the placebo group. Biofilm formation and BI were reduced in gingivitis patients. This was probably a result of Matricaria chamomilla’s anti-inflammatory and antimicrobial properties | 1. Short follow-up period 2. Pilot study 3. Small sample size | [186]/2016 | |
| Psidium guajava | RCT | N total: 15 patients (30 sites) Nc: 15 sites Ns: 15 sites [Patients with chronic periodontitis] | Gc: SRP Gs: 3% P. guajava gel [After one and three months, PI, GI, BI, PD, CAL, and colony counts of A. a and P. gingivalis were evaluated at baseline] | Clinical parameters improved significantly throughout the study. Three months after testing, site-specific indices, PD (2.74 ± 0.283), and CAL (2.8 ± 0.152) showed statistically significant reductions. A. a. (17.4 ± 0.026) and P. gingivalis (22.7 ± 1.225) colony counts were significantly reduced at one and three months in the test sites (p < 0.001). Local delivery of 3% P. guajava gel treated chronic periodontitis with clinical and microbiological parameter improvements. | 1. Short follow-up period 2. Small sample size 3. Split-mouth design | [187]/2021 |
| Punica granatum | RCT | N total: 10 patients (20 sites) Nc: 10 sites Ns: 10 sites [Patients with moderate–severe chronic periodontitis] | Gc: Placebo gel Gs: Punica granatum gel [after 15 days, PI, GI, and BI were measured at baseline] | After 15 days following gel application, mean BI, GI, and PI were significantly reduced. According to microbiological results, Punica granatum oral gel suppresses microbial growth. Test specimens revealed mild perivascular inflammation and increased collagen fibers, while controls showed dense inflammatory infiltration and collagen fiber destruction. In combination with SRP, Punica granatum gel reduced chronic periodontitis clinical symptoms. | 1. Small sample size 2. Short follow-up period | [188]/2019 |
| RCT | N1: 20 N2: 20 N3: 20 N4: 20 [Healthy individuals] | G1: Pomegranate extract gel G2: CHX gel G3: Ornidazole–CHX gel G4: Placebo gel [After 14 and 60 days, GI, PI, BOP, PD, and GCF levels of IL-8, IL-1β and chemokine ligand 28 were measured at baseline] | Inhibition of inflammatory cytokines and chemokines was observed in G1. G1 levels of IL-1β and IL-8 increased less than CCL28 levels (p = 0.003, 0.002), which remained unchanged from baseline (p = 0.15). G1 subjects showed a lower increase in BOP and GI (p = 0.01, 0.05) compared to other groups (p < 0.001) after 14 days. It was similar in terms of PI reduction between G1 and G3 gels (p = 0.96). For the treatment of gingivitis, PEG effectively reduced inflammatory markers. | 1. In an experimental gingivitis model, all products were tested, which may differ from the natural gingivitis model. 2. In order to avoid bias caused by variable host responses, a cross-over design would have been more appropriate. | [189]/2017 | |
| RCT | Nc: 40 Ns: 40 [Diabetic patients with gingivitis] | Gc: CHX 0.2% Gs: Punica granatum mouthwash [After 14 days, PI, GI, BI, and PD were measured at baseline] | Both interventions significantly improved gingival and plaque indices (p < 0.001 for all indices). Primary outcome measures showed no significant differences between Gc and Gs, except for GI, where Gs mouthwash had superiority over Gc after two weeks (p = 0.039). It is safe and effective to use Punica granatum mouthwash as an alternative to CHX for diabetic patients with gingivitis. | 1. Short follow-up period 2. Lack of a placebo group 3. Small sample size | [190]/2016 | |
| Rosmarinus officinalis | RCT | Nc: 23 Ns: 23 [Patients with moderate chronic periodontitis] | Gc: SRP + placebo Gs: SRP + EO mouth rinse [After three and six months, PD, CAL, BOP, and BI were evaluated at baseline; the subgingival plaque was sampled to evaluate principal periodontitis-associated bacteria] | A significant improvement in CAL was observed after 3 and 6 months compared to the control group (p < 0.001). Following SRP, adding essential oils to mouthwashes decreases subgingival bacterial levels and improves clinical outcomes. | Small sample size | [191]/2016 |
| Salvadora persica | RCT | Nc: 47 Ns: 47 [School students] | Gc: Fluoridated toothpaste + brushing Gs: SP sticks [Baseline, three-week, and 12-week PI measurements were conducted as well as saliva sampling] | Plaque scores decreased statistically significantly in both groups (p = 0.007 and p = 0.001, respectively). After three months, the number of subjects with abundant S. sanguinis increased from zero to six. | 1. Small sample size 2. Short follow-up period | [192]/2020 |
| RCT | N total: 44 [Pediatric patients receiving chemotherapy] | Gc: Normal saline Gs: Persica oral drops [Oral conditions were recorded at baseline and after 8 and 15 days] | A comparison of the severity of mucositis and oral health status of patients in both examination sessions did not reveal significant differences between treatment groups (p > 0.05). Mucositis, plaque accumulation, and gingival health improved statistically significantly in both treatment groups after 14 days following mouth rinse administration (p < 0.05). SP oral drops significantly improve plaque and gingival health | 1. Small sample size 2. Short follow-up period | [193]/2020 | |
| RCT | N1: 12 N2: 13 [Patients with grade two or three plaque score] | G1: Toothpaste with tea tree oil G2: Miswak-based toothpaste [PI was recorded at baseline and after 24 h of follow-up] | Both herbal-based toothpastes reduced plaque scores, but when compared with G1, G2 resulted in significantly lower plaque scores. | 1. Short follow-up period 2. Lack of gingival inflammation assessment 3. Small sample size | [194]/2018 | |
| Cross-sectional | N1: 115 N2: 93 N3: 79 | G1: SP sticks (Miswak) G2: Conventional toothpaste/toothbrush G3: SP sticks + toothbrush [GI, OHI, and PI were recorded] | G1 had a higher mean GI than G2, and G3 had a lower mean PI than G2. Between G1 and G2, the mean GI score was statistically significant (p = 0.001). Oral hygiene did not differ statistically significantly between groups. | Small sample size | [195]/2012 | |
| Terminalia chebula | RCT | N1: 30 N2: 30 N3: 30 [Healthy students] | G1: T. chebula mouthwash G2: CHX G3: Distilled water At baseline and after 15 and 30 days, PI and GI were evaluated] | At 15 and 30 days, PI and GI decreased significantly in G1 and G2 (p < 0.05). There was a significant reduction in G2, but not statistically significant in comparison to G1. The GI between G1 and G2 was not statistically significant (p = 0.837 for 15 days and p = 0.909 for 30 days) and PI (p = 0.592 at 15 days and p = 1.096 at 30 days). Using the T. chebula mouth rinse reduced dental plaque and gingivitis as effectively as CHX without the adverse effects of CHX. | 1. Small sample size 2. Short follow-up period | [196]/2015 |
| RCT | N1: 26 N2: 26 N3: 26 [Patients with PI > 1.5] | G1: 0.12% CHX G2: Terminalia chebula 10% mouthwash G3: Saline rinse [At baseline and after 7 and 14 days, PI and GI were evaluated] | Clinical parameters were significantly reduced in both G1 and G2 even though there were no significant differences between them (p > 0.05). Studies have shown that Terminalia chebula mouth rinses reduce microbial plaques and gingival inflammations, as well as neutralize salivary pH levels. | 1. Small sample size 2. Short follow-up period | [197]/2014 | |
| RCT | Nc: 40 Ns: 40 [Patients with chronic gingivitis] | Gc: Oral prophylaxis alone Gs: Oral prophylaxis + gingival massage with T. chebula powder [At baseline and after one month, PI, GI, and BI were measured] | Significant reductions in the PI, GI, and BI scores were observed after gum massage with T. chebula powder. Chronic gingivitis patients can benefit from T. chebula powder. | 1. Short follow-up period 2. No comparison with other studies 3. Small sample size | [198]/2017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mosaddad, S.A.; Hussain, A.; Tebyaniyan, H. Green Alternatives as Antimicrobial Agents in Mitigating Periodontal Diseases: A Narrative Review. Microorganisms 2023, 11, 1269. https://doi.org/10.3390/microorganisms11051269
Mosaddad SA, Hussain A, Tebyaniyan H. Green Alternatives as Antimicrobial Agents in Mitigating Periodontal Diseases: A Narrative Review. Microorganisms. 2023; 11(5):1269. https://doi.org/10.3390/microorganisms11051269
Chicago/Turabian StyleMosaddad, Seyed Ali, Ahmed Hussain, and Hamid Tebyaniyan. 2023. "Green Alternatives as Antimicrobial Agents in Mitigating Periodontal Diseases: A Narrative Review" Microorganisms 11, no. 5: 1269. https://doi.org/10.3390/microorganisms11051269