
Evaluation of Plasma Lipocalin-2 as a Predictor of Etiology and Severity in Adult Patients with Community-Acquired Pneumonia
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Evaluation at Admission and Follow Up
2.3. LCN2 Quantification
2.4. Statistical Analysis
3. Results
3.1. Clinical and Microbiological Features of the Study Population
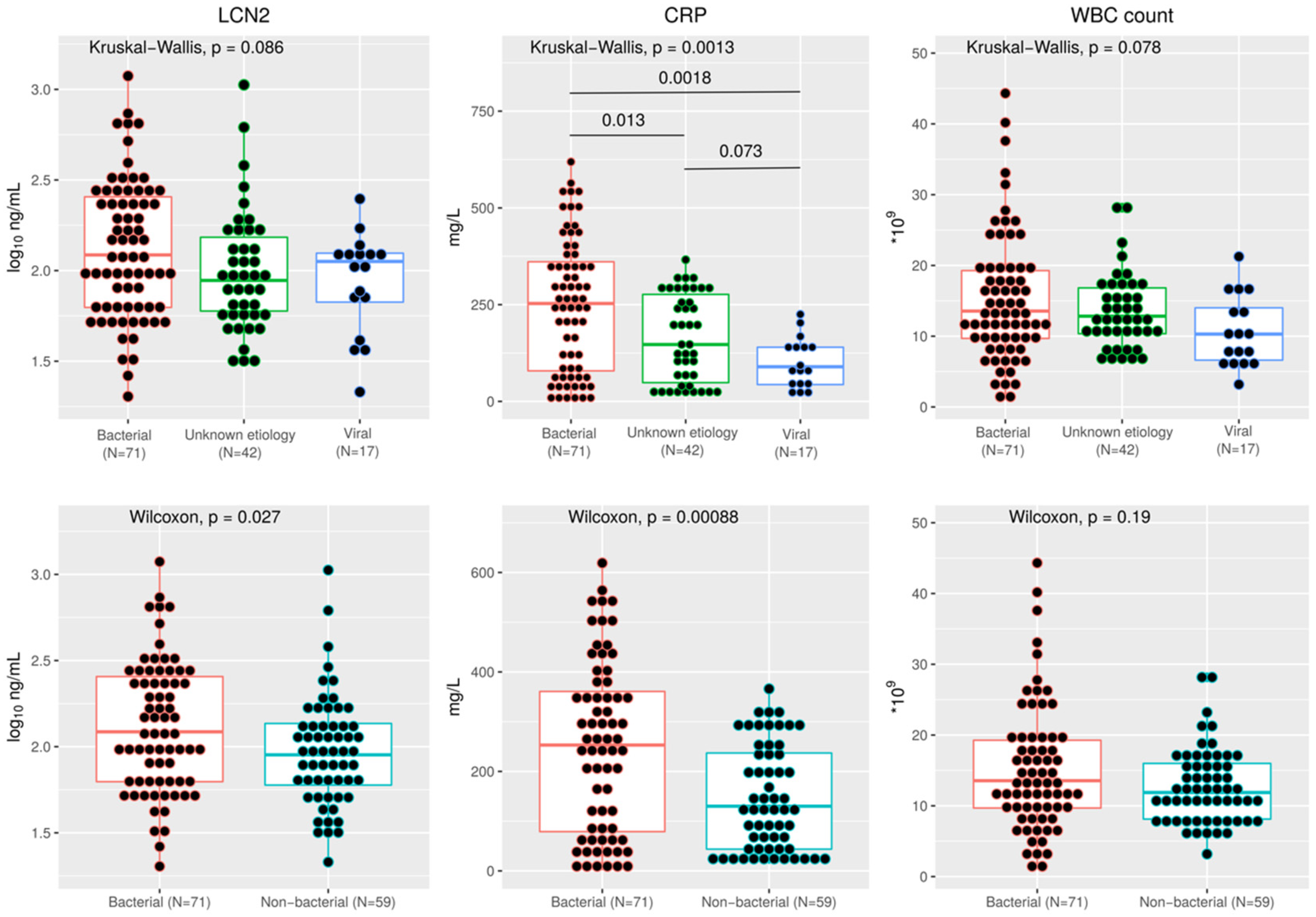
3.2. Plasma LCN2 and CAP Etiology
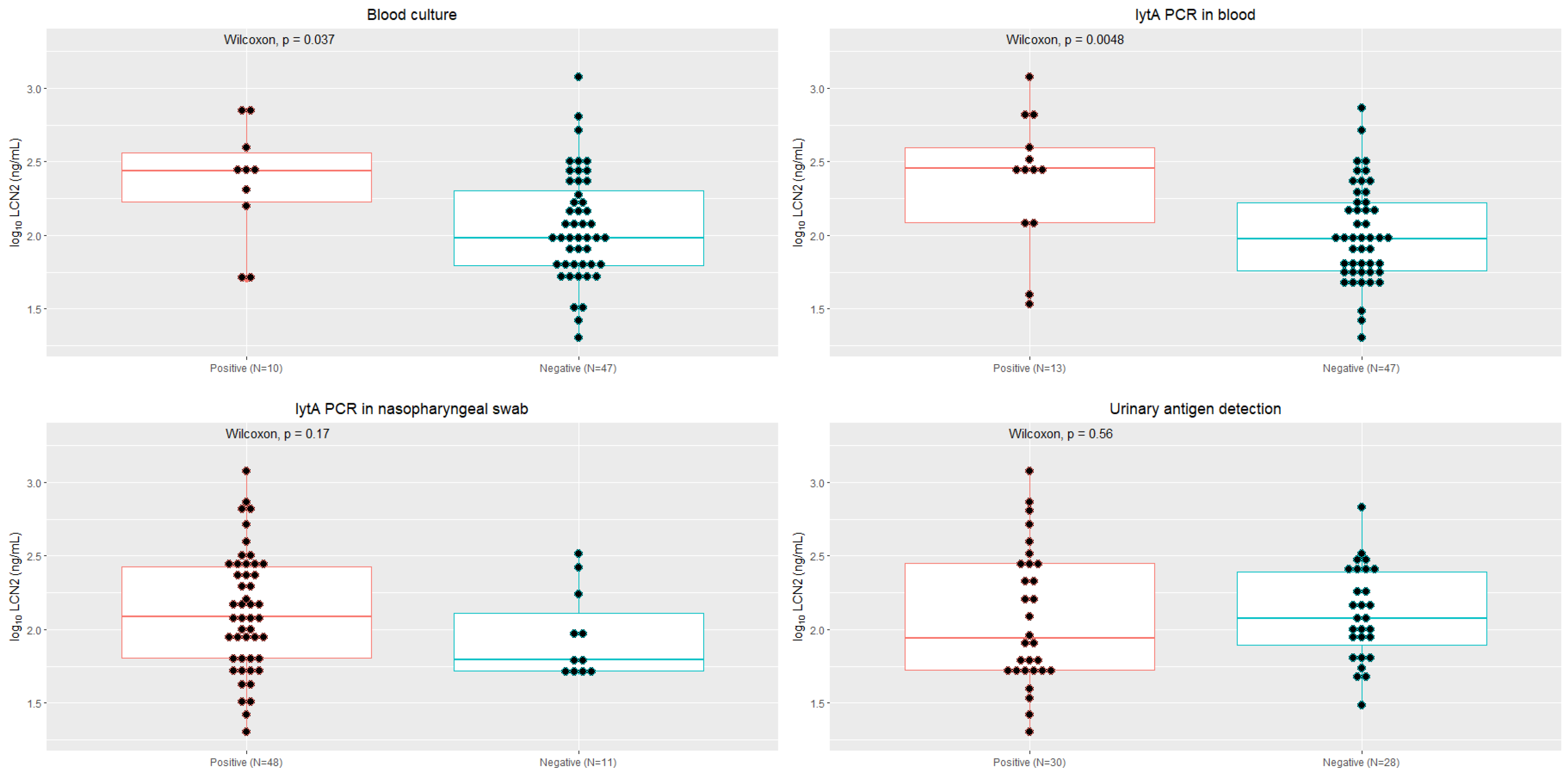
3.3. Plasma LCN2 and Pneumococcal Pneumonia
3.4. Plasma LCN2 as a Biomarker of Severity CAP
3.5. Plasma LCN2 and Clinical Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J. The Modern Diagnostic Approach to Community-Acquired Pneumonia in Adults. Semin. Respir. Crit. Care Med. 2016, 37, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Morley, D.; Torres, A.; Cillóniz, C.; Martin-Loeches, I. Predictors of treatment failure and clinical stability in patients with community acquired pneumonia. Ann. Transl. Med. 2017, 5, 443. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Jing, H.; Hongtao, P.; Furong, J.; Yuting, J.; Xu, S.; Venge, P. Distinction between bacterial and viral infections by serum measurement of human neutrophil lipocalin (HNL) and the impact of antibody selection. J. Immunol. Methods 2016, 432, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Venge, P. Human neutrophil lipocalin (HNL) as a biomarker of acute infections. Ups. J. Med. Sci. 2018, 123, 1–8. [Google Scholar] [CrossRef]
- Shaddock, E.J. How and when to use common biomarkers in community-acquired pneumonia. Pneumonia 2016, 8, 17. [Google Scholar] [CrossRef]
- Huang, H.; Ideh, R.C.; Gitau, E.; Thézénas, M.L.; Jallow, M.; Ebruke, B.; Chimah, O.; Oluwalana, C.; Karanja, H.; Mackenzie, G.; et al. Discovery and Validation of Biomarkers to Guide Clinical Management of Pneumonia in African Children. Clin. Infect. Dis. 2014, 58, 1707–1715. [Google Scholar] [CrossRef]
- Feldman, C.; Anderson, R. Pneumonia as a systemic illness. Curr. Opin. Pulm. Med. 2018, 24, 237–243. [Google Scholar] [CrossRef]
- Viasus, D.; Del Rio-Pertuz, G.; Simonetti, A.F.; Garcia-Vidal, C.; Acosta-Reyes, J.; Garavito, A.; Carratalà, J. Biomarkers for predicting short-term mortality in community-acquired pneumonia: A systematic review and meta-analysis. J. Infect. 2016, 72, 273–282. [Google Scholar] [CrossRef]
- Goetz, D.H.; Holmes, M.A.; Borregaard, N.; Bluhm, M.E.; Raymond, K.N.; Strong, R.K. The Neutrophil Lipocalin NGAL Is a Bacteriostatic Agent that Interferes with Siderophore-Mediated Iron Acquisition. Mol. Cell 2002, 10, 1033–1043. [Google Scholar] [CrossRef]
- Flower, D.R. The lipocalin protein family: Structure and function. Biochem. J. 1996, 318, 1–14. [Google Scholar] [CrossRef]
- Nasioudis, D.; Witkin, S.S. Neutrophil gelatinase-associated lipocalin and innate immune responses to bacterial infections. Med. Microbiol. Immunol. 2015, 204, 471–479. [Google Scholar] [CrossRef]
- Cowland, J.B.; Borregaard, N. Molecular Characterization and Pattern of Tissue Expression of the Gene for Neutrophil Gelatinase-Associated Lipocalin from Humans. Genomics 1997, 45, 17–23. [Google Scholar] [CrossRef]
- Venge, P.; Håkansson, L.D.; Garwicz, D.; Peterson, C.; Xu, S.; Pauksen, K. Human neutrophil lipocalin in fMLP-activated whole blood as a diagnostic means to distinguish between acute bacterial and viral infections. J. Immunol. Methods 2015, 424, 85–90. [Google Scholar] [CrossRef]
- Venge, P.; Douhan-Håkansson, L.; Garwicz, D.; Peterson, C.; Xu, S.; Pauksen, K. Human Neutrophil Lipocalin as a Superior Diagnostic Means To Distinguish between Acute Bacterial and Viral Infections. Clin. Vaccine Immunol. 2015, 22, 1025–1032. [Google Scholar] [CrossRef]
- Xu, S.Y.; Pauksen, K.; Venge, P. Serum measurements of human neutrophil lipocalin (HNL) discriminate between acute bacterial and viral infections. Scand. J. Clin. Lab. Investig. 1995, 55, 125–131. [Google Scholar] [CrossRef]
- Venge, P.; Eriksson, A.K.; Douhan-Håkansson, L.; Pauksen, K. Human neutrophil lipocalin in activated whole blood is a specific and rapid diagnostic biomarker of bacterial infections in the respiratory tract. Clin. Vaccine Immunol. 2017, 24, e00064-17. [Google Scholar] [CrossRef]
- Esposito, S.; Bianchini, S.; Gambino, M.; Madini, B.; Di Pietro, G.; Umbrello, G.; Presicce, M.L.; Ruggiero, L.; Terranova, L.; Principi, N. Measurement of lipocalin-2 and syndecan-4 levels to differentiate bacterial from viral infection in children with community-acquired pneumonia. BMC Pulm. Med. 2016, 16, 103. [Google Scholar] [CrossRef]
- Kim, J.W.; Hong, D.Y.; Lee, K.R.; Kim, S.Y.; Baek, K.J.; Park, S.O. Usefulness of plasma neutrophil gelatinase-associated lipocalin concentration for predicting the severity and mortality of patients with community-acquired pneumonia. Clin. Chim. Acta 2016, 462, 140–145. [Google Scholar] [CrossRef]
- Liu, C.; Wang, F.; Cui, L.; Zhou, J.; Xu, Z. Diagnostic value of serum neutrophil gelatinase-associated lipocalin, interleukin-6 and anti-citrullinated alpha-enolase peptide 1 for lower respiratory tract infections. Clin. Biochem. 2020, 75, 30–34. [Google Scholar] [CrossRef]
- Min, J.H.; Lee, H.; Chung, S.J.; Yeo, Y.; Park, T.S.; Park, D.W.; Moon, J.Y.; Kim, S.H.; Kim, T.H.; Sohn, J.W.Y.H. Neutrophil Gelatinase-Associated Lipocalin for Predicting Intensive Care Unit Admission and Mortality in Patients with Pneumonia. Tohoku J. Exp. Med. 2020, 250, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Yeh, Y.-H.; Chang, J.-L.; Hsiao, P.-C.; Tsao, S.M.; Lin, C.H.; Kao, S.J.; Chou, M.C.; Yang, S.F.; Chien, M.H. Circulating Level of Lipocalin 2 As a Predictor of Severity in Patients With Community-Acquired Pneumonia. J. Clin. Lab. Anal. 2013, 27, 253–260. [Google Scholar] [CrossRef]
- Naydenova, E.; Tsanas, A.; Howie, S.; Casals-Pascual, C.; De Vos, M. The power of data mining in diagnosis of childhood pneumonia. J. R. Soc. Interface 2016, 13, 20160266. [Google Scholar] [CrossRef] [PubMed]
- Sawatzky, J.; Soo, J.; Conroy, A.L.; Bhargava, R.; Namasopo, S.; Opoka, R.O.; Hawkes, M.T. Biomarkers of Systemic Inflammation in Ugandan Infants and Children Hospitalized With Respiratory Syncytial Virus Infection. Pediatr. Infect. Dis. J. 2019, 38, 854–859. [Google Scholar] [CrossRef]
- Boix-Palop, L.; Obradors, M.; Xercavins, M.; Picó-Plana, E.; Canales, L.; Dietl, B.; Pérez, J.; Garau, J.; Calbo, E. Improvement of pneumococcal pneumonia diagnosis using quantitative real-time PCR targeting lytA in adult patients: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 138.e1–138.e7. [Google Scholar] [CrossRef] [PubMed]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A Prediction Rule to Identify Low-Risk Patients with Community-Acquired Pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Lim, W.S.; Van Der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Akaike, H. A new look at the statistical model identification. IEEE Trans. Autom. Control 1974, 19, 716–723. [Google Scholar] [CrossRef]
- Venge, P.; Xu, S. Diagnosis and Monitoring of Acute Infections with Emphasis on the Novel Biomarker Human Neutrophil Lipocalin. J. Appl. Lab. Med. 2019, 3, 664–674. [Google Scholar] [CrossRef]
- Haase, M.; Bellomo, R.; Devarajan, P.; Schlattmann, P.; Haase-Fielitz, A. Accuracy of Neutrophil Gelatinase-Associated Lipocalin (NGAL) in Diagnosis and Prognosis in Acute Kidney Injury: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2009, 54, 1012–1024. [Google Scholar] [CrossRef]
- Fang, C.; Wang, Z.; Dai, Y.; Chang, W.; Sun, L.; Ma, X. Serum human neutrophil lipocalin: An effective biomarker for diagnosing bacterial infections. Clin. Biochem. 2020, 75, 23–29. [Google Scholar] [CrossRef]
- Venge, P.; Eriksson, A.-K.; Holmgren, S.; Douhan-Håkansson, L.; Peterson, C.; Xu, S.; Eriksson, S.; Garwicz, D.; Larsson, A.; Pauksen, K. HNL (Human Neutrophil Lipocalin) and a multimarker approach to the distinction between bacterial and viral infections. J. Immunol. Methods 2019, 474, 112627. [Google Scholar] [CrossRef]
- Elkhidir, A.E.; Eltaher, H.B.; Mohamed, A.O. Association of lipocalin-2 level, glycemis status and obesity in type 2 diabetes mellitus. BMC Res. Notes 2017, 10, 285. [Google Scholar] [CrossRef]
- Maurizi, A.; Ponzetti, M.; Gautvik, K.M.; Reppe, S.; Teti, A.; Rucci, N. Lipocalin 2 serum levels correlate with age and bone turnover biomarkers in healthy subjects but not in postmenopausal osteoporotic women. Bone Rep. 2021, 14, 101059. [Google Scholar] [CrossRef]
- Albrich, W.C.; Madhi, S.A.; Adrian, P.V.; Van Niekerk, N.; Mareletsi, T.; Cutland, C.; Wong, M.; Khoosal, M.; Karstaedt, A.; Zhao, P.; et al. Use of a Rapid Test of Pneumococcal Colonization Density to Diagnose Pneumococcal Pneumonia. Clin. Infect Dis. 2011, 54, 601–609. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Microorganism | N (%) |
|---|---|
| Bacterial CAP | 71 (54.6) |
| Streptococcus pneumoniae | 60 (46.2) |
| - S. pneumoniae co-infection * | 30 (23.1) |
| Mycoplasma pneumoniae | 2 (1.54) |
| Legionella pneumophila | 2 (1.54) |
| Chlamydophila pneumoniae + Human rhinovirus | 2 (1.54) |
| Streptococcus pyogenes | 1 (0.77) |
| Staphylococcus aureus + Influenza virus | 1 (0.77) |
| C. pneumoniae + Adenovirus | 1 (0.77) |
| Streptococcus viridans + Respiratory syncytial virus | 1 (0.77) |
| Legionella pneumophila + Adenovirus | 1 (0.77) |
| Unknown origin CAP | 42 (32.3) |
| Viral CAP | 17 (13.1) |
| Human rhinovirus | 5 (3.84) |
| Influenza virus | 3 (2.31) |
| Metapneumovirus | 2 (1.54) |
| Influenza virus + Adenovirus | 2 (1.54) |
| Coronavirus | 1 (0.77) |
| Parainfluenza virus | 1 (0.77) |
| Respiratory syncytial virus | 1 (0.77) |
| Adenovirus | 1 (0.77) |
| Human rhinovirus + Adenovirus | 1 (0.77) |
| Bacterial CAP (N = 71) | Unknown Origin CAP (N = 42) | Viral CAP (N = 17) | p | |
|---|---|---|---|---|
| Demographic data | ||||
| Age (years) | 68.0 (53.5–79.0) | 72.5 (59.0–82.0) | 82.0 (76.0–83.0) | 0.02 A |
| Gender, male | 50 (70.4) | 28 (66.7) | 6 (35.3) | 0.03 A |
| BMI (kg/m2) | 25.6 (22.3–29.1) | 26.9 (23.9–29.8) | 27.9 (22.7–30.8) | 0.3 |
| Caucasian race | 70 (98.6) | 41 (97.6) | 16 (94.1) | 0.3 |
| Current smoker | 18 (25.3) | 12 (28.6) | 0 | 0.03 A,C |
| Ex-smoker | 23 (32.4) | 17 (40.5) | 6 (35.3) | 0.7 |
| Comorbid conditions | ||||
| Charlson index ≥ 4 | 10 (14.1) | 4 (9.5) | 2 (11.8) | 0.9 |
| Chronic kidney disease | 8 (11.3) | 5 (9.5) | 3 (17.6) | 0.4 |
| Diabetes | 54 (76.1) | 33 (78.6) | 14 (82.4) | 0.62 |
| Immunosuppression 1 | 4 (5.6) | 0 | 2 (11.8) | 0.09 |
| Prior antibiotic treatment 2 | 9 (12.7) | 7 (16.7) | 4 (23.5) | 0.5 |
| Prehospital treatment 3 | 11 (15.5) | 4 (9.5) | 3 (17.6) | 0.6 |
| Clinical features on presentation | ||||
| Time symptom onset—ED visit (hours) | 48 (24–108) | 84 (48–138) | 72 (48–96) | 0.1 |
| Fever (≥38 °C) | 35 (49.3) | 12 (28.6) | 6 (35.3) | 0.09 |
| Dyspnea | 50 (70.4) | 32 (76.2) | 12 (70.6) | 0.8 |
| Tachypnea (≥20 rpm) | 45 (69.2) | 24 (64.9) | 8 (61.5) | 0.8 |
| Cough | 63 (88.7) | 35 (83.3) | 16 (94.1) | 0.6 |
| Purulent sputum | 30 (42.3) | 19 (45.2) | 9 (52.9) | 0.8 |
| Pleuritical chest pain | 30 (42.3) | 10 (23.8) | 3 (17.6) | 0.05 |
| Septic shock | 16 (22.9) | 3 (7.1) | 2 (11.8) | 0.08 |
| Respiratory failure | 38 (55.1) | 23 (54.8) | 13 (76.5) | 0.3 |
| PaO2/FiO2 | 290 (257.5–345.5) | 300 (252–362) | 271 (243–300) | 0.1 |
| PSI ≥ 4 * | 38 (54.3) | 14 (33.3) | 11 (64.7) | 0.1 |
| CURB-65 score ≥ 3 * | 11 (15.7) | 7 (16.7) | 3 (17.6) | 0.6 |
| Laboratory findings * | ||||
| LCN2 (ng/mL) | 122.0 (62.6–255.3) | 88.2 (59.8–153.0) | 112.3 (67.0–124.8) | 0.08 |
| CRP (mg/L) | 253.0 (79.0–360.7) | 147.0 (48.5–276.5) | 89.5 (43.5–140.0) | 0.001 A,B |
| WBC count (×109/L) | 13.5 (9.7–19.3) | 12.8 (10.4–16.8) | 10.3 (6.6–14.0) | 0.08 |
| Lymphocytes count (×109/L) | 1.0 (0.7–1.4) | 1.2 (0.8–1.6) | 1.2 (0.7–1.7) | 0.4 |
| Evolution and Outcome | ||||
| Time to clinical stability (days) | 2 (1–4) | 2 (1–4) | 2 (1–3) | 0.6 |
| ICU admission | 7 (9.9) | 3 (7.1) | 1 (5.9) | 0.9 |
| Mechanical Ventilation | 3 (4.2) | 2 (4.8) | 1 (5.9) | 1 |
| Length of hospital stay (days) | 6.0 (4.0–8.8) | 5.5 (1.2–9.0) | 6.0 (5.0–9.0) | 0.7 |
| In-hospital mortality | 0 | 0 | 1 (5.9) | 0.1 |
| Biomarker | Cutoff Value | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | AUC (95% CI) | OR (95% CI) |
|---|---|---|---|---|---|---|---|
| Bacterial CAP (n = 71) | |||||||
| -LCN2 (ng/L) -CRP (mg/L) -WBC (mm3) | 138.9 204 13.5 | 77.9 61.8 50.7 | 47.8 71.2 62.7 | 72.3 71.2 61.4 | 55.4 61.8 52.1 | 0.62 (0.52–0.72) 0.67 (0.58–0.77) 0.57 (0.47–0.67) | 3.25 (1.50–7.04) 4.00 (1.89–8.42) 1.73 (0.85–3.51) |
| S. pneumoniae CAP (n = 60) | |||||||
| -LCN2 (ng/L) -CRP (mg/L) -WBC (mm3) | 138.9 204 13.5 | 43.4 62.1 52.5 | 70.0 66.7 62.3 | 55.3 61.0 54.4 | 59.0 67.6 60.6 | 0.54 (0.44–0.65) 0.64 (0.54–0.74) 0.57 (0.46–0.67) | 1.78 (0.87–3.68) 3.27 (1.58–6.79) 1.83 (0.90–3.71) |
| IPD (n = 10) | |||||||
| -LCN2 (ng/L) -CRP (mg/L) -WBC (mm3) | 204 318 17.0 | 70.0 80.0 60.0 | 79.1 83.2 73.7 | 22.6 29.6 16.7 | 96.8 97.9 95.5 | 0.74 (0.53–0.94) 0.82 (0.71–0.93) 0.56 (0.30–0.82) | 8.85 (2.13–36.8) 21.1 (4.14–107.7) 4.2 (1.11–15.9) |
| Viral CAP (n = 17) * | |||||||
| -LCN2 (ng/L) -CRP (mg/L) -WBC (mm3) | 98.1 88.2 12.8 | 58.8 58.8 35.3 | 48.7 30.9 48.6 | 14.7 11.6 9.5 | 88.7 82.9 83.1 | 0.41 (0.33–0.51) 0.29 (0.20–0.39) 0.33 (0.20–0.47) | 1.34 (0.48–3.81) 0.64 (0.22–1.82) 0.52 (0.18–1.49) |
| Bacterial CAP | CURB-65 ≥ 3 | PSI ≥ 4 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Univariate | ||||||
| Age (years) | 0.97 (0.95–0.99) | 0.03 | 1.04 (1.00–1.08) | 0.03 | 1.04 (1.02–1.07) | 0.001 |
| Gender, male | 0.57 (0.28–1.18) | 0.13 | 0.88 (0.33–2.38) | 0.81 | 0.54 (0.26–1.13) | 0.10 |
| Current smoker | 1.33 (0.58–3.05) | 0.50 | 0.30 (0.66–1.37) | 0.12 | 0.75 (0.33–1.71) | 0.49 |
| Charlson index ≥ 4 | 1.45 (0.49–4.25) | 0.50 | 7.69 (2.47–24.0) | <0.001 | 9.14 (1.98–42.1) | 0.005 |
| Renal failure | 0.94 (0.32–2.71) | 0.92 | 6.25 (1.96–19.9) | 0.002 | 18.6 (2.36–146.1) | 0.005 |
| Prehospital treatment | 1.36 (0.49–3.77) | 0.55 | 0.65 (1.96–19.9) | 0.59 | 0.39 (0.13–1.17) | 0.09 |
| Time from symptom onset to ED visit (days) | 0.85 (0.71–1.01) | 0.06 | 0.66 (0.48–0.90) | 0.009 | 0.72 (0.59–0.87) | 0.001 |
| Septic shock | 3.20 (1.09–9.35) | 0.03 | 8.02 (2.78–23.1) | <0.001 | 4.15 (1.42–12.2) | 0.009 |
| Respiratory failure | 0.80 (0.40–1.62) | 0.54 | 2.81 (0.96–8.21) | 0.06 | 7.02 (3.17–15.5) | <0.001 |
| LCN2 (10 ng/mL) | 1.02 (0.99–1.05) | 0.07 | 1.06 (1.03–1.09) | <0.001 | 1.04 (1.01–1.07) | 0.01 |
| CRP (mg/dL) | 1.05 (1.02–1.08) | <0.001 | 1.01 (0.98–1.04) | 0.42 | 1.01 (0.98–1.03) | 0.66 |
| Best predictive model | ||||||
| Age (years) | 0.97 (0.94–0.99) | 0.009 | 1.07 (1.02–1.13) | 0.008 | 1.04 (1.01–1.08) | 0.008 |
| Charlson index ≥ 4 | 6.77 (1.51–30.4) | 0.013 | 6.47 (1.03–40.8) | 0.047 | ||
| Time from symptom onset to ED visit (days) | 0.71 (0.57–0.88) | 0.002 | 0.70 (0.44–1.12) | 0.14 | 0.79 (0.63–0.99) | 0.047 |
| Septic shock | 8.74 (1.77–43.3) | 0.008 | ||||
| Respiratory failure | 6.07 (2.44–15.1) | <0.001 | ||||
| LCN2 (10 ng/mL) | 1.01 (0.98–1.04) | 0.42 | 1.04 (1.01–1.09) | 0.029 | 1.04 (1.01–1.07) | 0.025 |
| CRP (mg/dL) | 1.06 (1.02–1.09) | 0.0001 | ||||
| CURB-65 | PSI | |||||||
|---|---|---|---|---|---|---|---|---|
| 0/1 | 2 | ≥3 | p | I/II/III | IV | V | p | |
| Number (%) | 71 (55.0) | 37 (28.7) | 21 (16.3) | 66 (51.2) | 44 (34.1) | 19 (14.7) | ||
| LCN2 (ng/mL) | 88.2 (53.5–144.4) | 115.0 (62.0–243.1) | 265.0 (138.8–380.2) | <0.001 * | 90.9 (54.1–159.6) | 107.4 (59.9–176.5) | 265.0 (120.3–352.4) | 0.001 * |
| CRP (mg/L) | 195.0 (67.8–297.8) | 143.0 (44.7–326.0) | 240.0 (85.5–312.2) | 0.44 | 193.0 (59.6–299.0) | 203.0 (76.1–326.0) | 93.0 (48.1–289.0) | 0.96 |
| WBC (×109/L) | 11.5 (8.5–16.1) | 12.8 (10.3–19.3) | 16.6 (10.9–23.2) | 0.02 | 12.7 (8.9–16.1) | 13.2 (9.3–19.3) | 13.8 (8.4–22.2) | 0.23 |
| Lymphocytes (×109/L) | 1.1 (0.7–1.5) | 1.0 (0.5–1.4) | 1.3 (0.8–1.7) | 0.42 | 1.1 (0.7–1.5) | 1.0 (0.7–1.6) | 1.2 (0.7–1.7) | 0.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boix-Palop, L.; Vergara, A.; Padilla, E.; Martínez, D.; Blanco, A.; Pérez, J.; Calbo, E.; Vila, J.; Casals-Pascual, C. Evaluation of Plasma Lipocalin-2 as a Predictor of Etiology and Severity in Adult Patients with Community-Acquired Pneumonia. Microorganisms 2023, 11, 1160. https://doi.org/10.3390/microorganisms11051160
Boix-Palop L, Vergara A, Padilla E, Martínez D, Blanco A, Pérez J, Calbo E, Vila J, Casals-Pascual C. Evaluation of Plasma Lipocalin-2 as a Predictor of Etiology and Severity in Adult Patients with Community-Acquired Pneumonia. Microorganisms. 2023; 11(5):1160. https://doi.org/10.3390/microorganisms11051160
Chicago/Turabian StyleBoix-Palop, Lucía, Andrea Vergara, Emma Padilla, Diego Martínez, Ana Blanco, Josefa Pérez, Esther Calbo, Jordi Vila, and Climent Casals-Pascual. 2023. "Evaluation of Plasma Lipocalin-2 as a Predictor of Etiology and Severity in Adult Patients with Community-Acquired Pneumonia" Microorganisms 11, no. 5: 1160. https://doi.org/10.3390/microorganisms11051160