
Small Intestinal Bacterial Overgrowth Is Associated with Poor Prognosis in Cirrhosis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
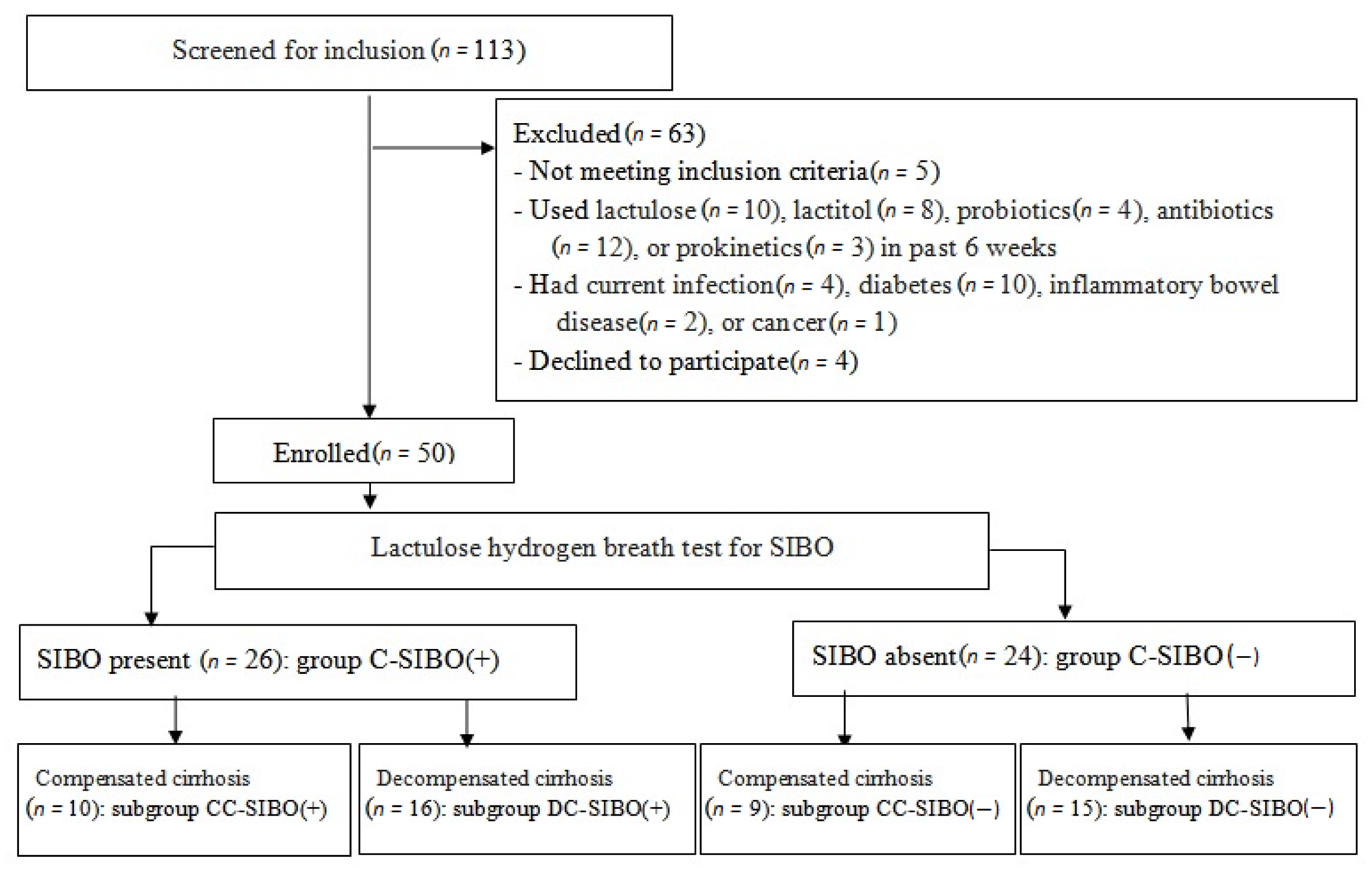
2.1. Participants
2.2. Diagnostic Workup
2.3. Follow-Up
2.4. Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fukui, H. Leaky Gut and Gut-Liver Axis in Liver Cirrhosis: Clinical Studies Update. Gut Liver 2021, 15, 666–676. [Google Scholar] [CrossRef] [PubMed]
- Gorham, J.; Gleeson, M. Cirrhosis and dysbiosis: New insights from next-generation sequencing. Hepatology 2016, 63, 336–338. [Google Scholar] [CrossRef] [PubMed]
- Maslennikov, R.; Pavlov, C.; Ivashkin, V. Small intestinal bacterial overgrowth in cirrhosis: Systematic review and meta-analysis. Hepatol. Int. 2018, 12, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, M.; Moreau, R.; Angeli, P.; Schnabl, B.; Arroyo, V. Mechanisms of decompensation and organ failure in cirrhosis: From peripheral arterial vasodilation to systemic inflammation hypothesis. J. Hepatol. 2015, 63, 1272–1284. [Google Scholar] [CrossRef] [PubMed]
- Maslennikov, R.; Pavlov, C.; Ivashkin, V. Is small intestinal bacterial overgrowth a cause of hyperdynamic circulation in cirrhosis? Turk. J. Gastroenterol. 2019, 30, 964–975. [Google Scholar] [CrossRef]
- Pugh, R.; Murraylyon, I.; Dawson, J. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. Am. J. Gastroenterol. 2017, 112, 775–784. [Google Scholar] [CrossRef] [Green Version]
- Ivashkin, V.T.; Maev, I.V.; Abdulganieva, D.I.; Alekseeva, O.P.; Alekseenko, S.A.; Zolnikova, O.Y.; Korochanskaya, N.V.; Medvedev, O.S.; Poluektova, E.A.; Simanenkov, V.I.; et al. Practical Recommendation of the Scientific Community for Human Microbiome Research (CHMR) and the Russian Gastroenterological Association (RGA) on Small Intestinal Bacterial Overgrowth in Adults. Russ. J. Gastroenterol. Hepatol. Coloproctology 2022, 32, 68–85. [Google Scholar] [CrossRef]
- Jin, M.; Kalainy, S.; Baskota, N.; Chiang, D.; Deehan, E.C.; McDougall, C.; Tandon, P.; Martínez, I.; Cervera, C.; Walter, J.; et al. Faecal microbiota from patients with cirrhosis has a low capacity to ferment non-digestible carbohydrates into short-chain fatty acids. Liver Int. 2019, 39, 1437–1447. [Google Scholar] [CrossRef]
- Zeng, Y.; Chen, S.; Fu, Y.; Wu, W.; Chen, T.; Chen, J.; Yang, B.; Ou, Q. Gut microbiota dysbiosis in patients with hepatitis B virus-induced chronic liver disease covering chronic hepatitis, liver cirrhosis and hepatocellular carcinoma. J. Viral Hepat. 2020, 27, 143–155. [Google Scholar] [CrossRef]
- Ahluwalia, V.; Betrapally, N.S.; Hylemon, P.B.; White, M.B.; Gillevet, P.M.; Unser, A.B.; Fagan, A.; Daita, K.; Heuman, D.M.; Zhou, H.; et al. Impaired Gut-Liver-Brain Axis in Patients with Cirrhosis. Sci. Rep. 2016, 6, 26800. [Google Scholar] [CrossRef]
- Kajihara, M.; Koido, S.; Kanai, T.; Ito, Z.; Matsumoto, Y.; Takakura, K.; Saruta, M.; Kato, K.; Odamaki, T.; Xiao, J.-Z.; et al. Characterisation of blood microbiota in patients with liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1577–1583. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Xie, Y.; Zhou, F.; Zhang, B.; Wu, J.; Yang, L.; Xu, S.; Stedtfeld, R.; Chen, Q.; Liu, J.; et al. Featured Gut Microbiomes Associated With the Progression of Chronic Hepatitis B Disease. Front. Microbiol. 2020, 11, 383. [Google Scholar] [CrossRef] [PubMed]
- Zheng, R.; Wang, G.; Pang, Z.; Ran, N.; Gu, Y.; Guan, X.; Yuan, Y.; Zuo, X.; Pan, H.; Zheng, J.; et al. Liver cirrhosis contributes to the disorder of gut microbiota in patients with hepatocellular carcinoma. Cancer Med. 2020, 9, 4232–4250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapidot, Y.; Amir, A.; Nosenko, R.; Uzan-Yulzari, A.; Veitsman, E.; Cohen-Ezra, O.; Davidov, Y.; Weiss, P.; Bradichevski, T.; Segev, S.; et al. Alterations in the Gut Microbiome in the Progression of Cirrhosis to Hepatocellular Carcinoma. mSystems 2020, 5, e00153-20. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Heuman, D.M.; Hylemon, P.B.; Sanyal, A.J.; White, M.B.; Monteith, P.; Noble, N.A.; Unser, A.B.; Daita, K.; Fisher, A.R.; et al. Altered profile of human gut microbiome is associated with cirrhosis and its complications. J. Hepatol. 2014, 60, 940–947. [Google Scholar] [CrossRef] [Green Version]
- Giannelli, V.; Digregorio, V.; Iebba, V.; Giusto, M.; Schippa, S.; Merli, M.; Thalheimer, U. Microbiota and the gut-liver axis: Bacterial translocation, inflammation and infection in cirrhosis. World J. Gastroenterol. 2014, 20, 16795–16810. [Google Scholar] [CrossRef]
- Kowalski, H.J.; Abelmann, W.H. The cardiac output at rest in Laennec’s cirrhosis. J. Clin. Investig. 1953, 32, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.F.; Dawson, A.M.; Sherlock, S. Circulatory changes in chronic liver disease. Am. J. Med. 1958, 24, 358–367. [Google Scholar] [CrossRef]
- Bolognesi, M.; Dipascoli, M.; Verardo, A.; Gatta, A. Splanchnic vasodilation and hyperdynamic circulatory syndrome in cirrhosis. World J. Gastroenterol. 2014, 20, 2555–2563. [Google Scholar] [CrossRef]
- Maslennikov, R.; Ivashkin, V.; Efremova, I.; Poluektova, E.; Kudryavtseva, A.; Krasnov, G. Gut dysbiosis and small intestinal bacterial overgrowth as independent forms of gut microbiota disorders in cirrhosis. World J. Gastroenterol. 2022, 28, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Bushyhead, D.; Quigley, E.M.M. Small Intestinal Bacterial Overgrowth-Pathophysiology and Its Implications for Definition and Management. Gastroenterology 2022, 163, 593–607. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, U.C.; Sachdeva, S.; Ghoshal, U.; Misra, A.; Puri, A.S.; Pratap, N.; Shah, A.; Rahman, M.M.; Gwee, K.A.; Tan, V.P.Y.; et al. Asian-Pacific consensus on small intestinal bacterial overgrowth in gastrointestinal disorders: An initiative of the Indian Neurogastroenterology and Motility Association. Indian J. Gastroenterol. 2022, 41, 483–507. [Google Scholar] [CrossRef]
- Skrzydło-Radomańska, B.; Cukrowska, B. How to Recognize and Treat Small Intestinal Bacterial Overgrowth? J. Clin. Med. 2022, 11, 6017. [Google Scholar] [CrossRef] [PubMed]
- Jun, D.W.; Kim, K.T.; Lee, O.Y.; Chae, J.D.; Son, B.K.; Kim, S.H.; Jo, Y.J.; Park, Y.S. Association between small intestinal bacterial overgrowth and peripheral bacterial DNA in cirrhotic patients. Dig. Dis. Sci. 2010, 55, 1465–1471. [Google Scholar] [CrossRef]
- Morencos, F.C.; De Las Heras Castaño, G.; Martín Ramos, L.; López Arias, M.J.; Ledesma, F.; Pons Romero, F. Small bowel bacterial overgrowth in patients with alcoholic cirrhosis. Dig Dis Sci. 1995, 40, 1252–1256. [Google Scholar] [CrossRef]
- Yang, C.Y.; Chang, C.S.; Chen, G.H. Small-intestinal bacterial overgrowth in patients with liver cirrhosis, diagnosed with glucose H2 or CH4 breath tests. Scand J. Gastroenterol. 1998, 33, 867–871. [Google Scholar]
- Pande, C.; Kumar, A.; Sarin, S.K. Small-intestinal bacterial overgrowth in cirrhosis is related to the severity of liver disease. Aliment. Pharmacol. Ther. 2009, 29, 1273–1281. [Google Scholar] [CrossRef]
- Lakshmi, C.P.; Ghoshal, U.C.; Kumar, S.; Goel, A.; Misra, A.; Mohindra, S.; Choudhuri, G. Frequency and factors associated with small intestinal bacterial overgrowth in patients with cirrhosis of the liver and extra hepatic portal venous obstruction. Dig. Dis. Sci. 2010, 55, 1142–1148. [Google Scholar] [CrossRef]
- Zhang, Y.; Feng, Y.; Cao, B.; Tian, Q. Effects of SIBO and rifaximin therapy on MHE caused by hepatic cirrhosis. Int. J. Clin. Exp. Med. 2015, 8, 2954–2957. [Google Scholar]
- Lunia, M.K.; Sharma, B.C.; Sachdeva, S. Small intestinal bacterial overgrowth and delayed orocecal transit time in patients with cirrhosis and low-grade hepatic encephalopathy. Hepatol. Int. 2013, 7, 268–273. [Google Scholar] [CrossRef]
- Gupta, A.; Dhiman, R.K.; Kumari, S.; Rana, S.; Agarwal, R.; Duseja, A.; Chawla, Y. Role of small intestinal bacterial overgrowth and delayed gastrointestinal transit time in cirrhotic patients with minimal hepatic encephalopathy. J. Hepatol. 2010, 53, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Nancey, S.; Moussata, D.; Roman, S.; Benmansour, H.; Claudel, S.; Flourié, B. A positive breath hydrogen test does not predict the occurrence of a spontaneous bacterial peritonitis in cirrhotic patients with ascites. Digestion 2009, 79, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.S.; Chen, G.H.; Lien, H.C.; Yeh, H.Z. Small intestine dysmotility and bacterial overgrowth in cirrhotic patients with spontaneous bacterial peritonitis. Hepatology 1998, 28, 1187–1190. [Google Scholar] [CrossRef]
- Chang, C.S.; Yang, S.S.; Kao, C.H.; Yeh, H.Z.; Chen, G.H. Small intestinal bacterial overgrowth versus antimicrobial capacity in patients with spontaneous bacterial peritonitis. Scand J. Gastroenterol. 2001, 36, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.M.; Steinbrückner, B.; Brinkmann, F.E.; Ditzen, A.K.; Schwacha, H.; Aponte, J.J.; Pelz, K.; Kist, M.; Blum, H.E. Small intestinal bacterial overgrowth in patients with cirrhosis: Prevalence and relation with spontaneous bacterial peritonitis. Am. J. Gastroenterol. 2001, 96, 2962–2967. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients with SIBO (n = 26) | Patients without SIBO (n = 24) | p * | |
|---|---|---|---|
| Age, years | 49 [39–59] | 52 [39–58] | 0.904 |
| Body mass index, kg/m2 | 24.6 [22.7–27.8] | 24.1 [22.5–26.8] | 0.636 |
| Men/women | 13/13 | 11/13 | 0.785 |
| Race (Caucasian/other) | 25/1 | 24/0 | 1.000 |
| Etiology of cirrhosis: alcohol | 9 | 9 | 1.000 |
| autoimmune | 2 | 9 | 0.016 |
| viral | 11 | 6 | 0.242 |
| cryptogenic | 4 | 0 | 0.111 |
| Child–Turcotte–Pugh score | 8 [6–10] | 8 [6–9] | 0.465 |
| Model for End-Stage Liver Disease score | 10.5 [7.4–13.5] | 9.2 [7.1–11.9] | 0.317 |
| Esophageal varices (present/absent) | 20/6 | 20/4 | 0.728 |
| Hepatic encephalopathy (overt/minimal/ absent) | 9/9/8 | 8/11/5 | 0.526 |
| Ascites (present/absent) | 18/8 | 10/14 | 0.086 |
| Serum albumin, g/L | 35 [30–40] | 36 [31–41] | 0.505 |
| Serum total bilirubin, μmol/L | 36.8 [27.9–55.2] | 36.6 [23.2–64.0] | 0.954 |
| Prothrombin index (Quick test), % | 57 [50–68] | 65 [55–71] | 0.146 |
| Creatinine, mg/dL | 0.74 [0.60–0.91] | 0.70 [0.64–0.87] | 0.949 |
| Red blood cells, cell/μL | 3.6 [2.6–5.1] | 4.0 [3.6–4.3] | 0.393 |
| White blood cells, cell/μL | 3.8 [3.4–4.2] | 4.0 [3.3–5.4] | 0.579 |
| Platelets, cell/μL | 78 [45–106] | 91 [62–112] | 0.136 |
| Erythrocyte sedimentation rate, mm/h | 12.5 [11–25] | 11.5 [7.0–26.0] | 1.000 |
| Splenic length, cm | 16.1 [14.2–19.9] | 14.7 [13.3–16.5] | 0.112 |
| Drug | Patients with SIBO (n = 26) | Patients without SIBO (n = 24) | p |
|---|---|---|---|
| Beta-blockers | 19.2% | 12.5% | 0.704 |
| Ornithine-aspartate | 15.4% | 16.7% | 1.000 |
| Diuretics | 53.8% | 37.5% | 0.272 |
| Ursodeoxycholic acid | 15.4% | 25.0% | 0.490 |
| Steroids | 7.7% | 25.0% | 0.132 |
| Antiviral drugs | 30.7% | 16.7% | 0.327 |
| Factor † | p ‡ | Hazard Ratio |
|---|---|---|
| Small intestinal bacterial overgrowth | 0.028 | 4.2 [1.2–14.9] |
| Esophageal varicese | 0.104 | |
| Ascites | 0.316 | |
| Hepatic encephalopathy | 0.336 | |
| Total bilirubin | 0.551 | |
| Albumen | 0.027 | 0.84 [0.72–0.98] |
| Prothrombin (quick test) | 0.540 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Efremova, I.; Maslennikov, R.; Alieva, A.; Poluektova, E.; Ivashkin, V. Small Intestinal Bacterial Overgrowth Is Associated with Poor Prognosis in Cirrhosis. Microorganisms 2023, 11, 1017. https://doi.org/10.3390/microorganisms11041017
Efremova I, Maslennikov R, Alieva A, Poluektova E, Ivashkin V. Small Intestinal Bacterial Overgrowth Is Associated with Poor Prognosis in Cirrhosis. Microorganisms. 2023; 11(4):1017. https://doi.org/10.3390/microorganisms11041017
Chicago/Turabian StyleEfremova, Irina, Roman Maslennikov, Aliya Alieva, Elena Poluektova, and Vladimir Ivashkin. 2023. "Small Intestinal Bacterial Overgrowth Is Associated with Poor Prognosis in Cirrhosis" Microorganisms 11, no. 4: 1017. https://doi.org/10.3390/microorganisms11041017