
Remdesivir Influence on SARS-CoV-2 RNA Viral Load Kinetics in Nasopharyngeal Swab Specimens of COVID-19 Hospitalized Patients: A Real-Life Experience

 , ,
, ,
Abstract
:1. Introduction
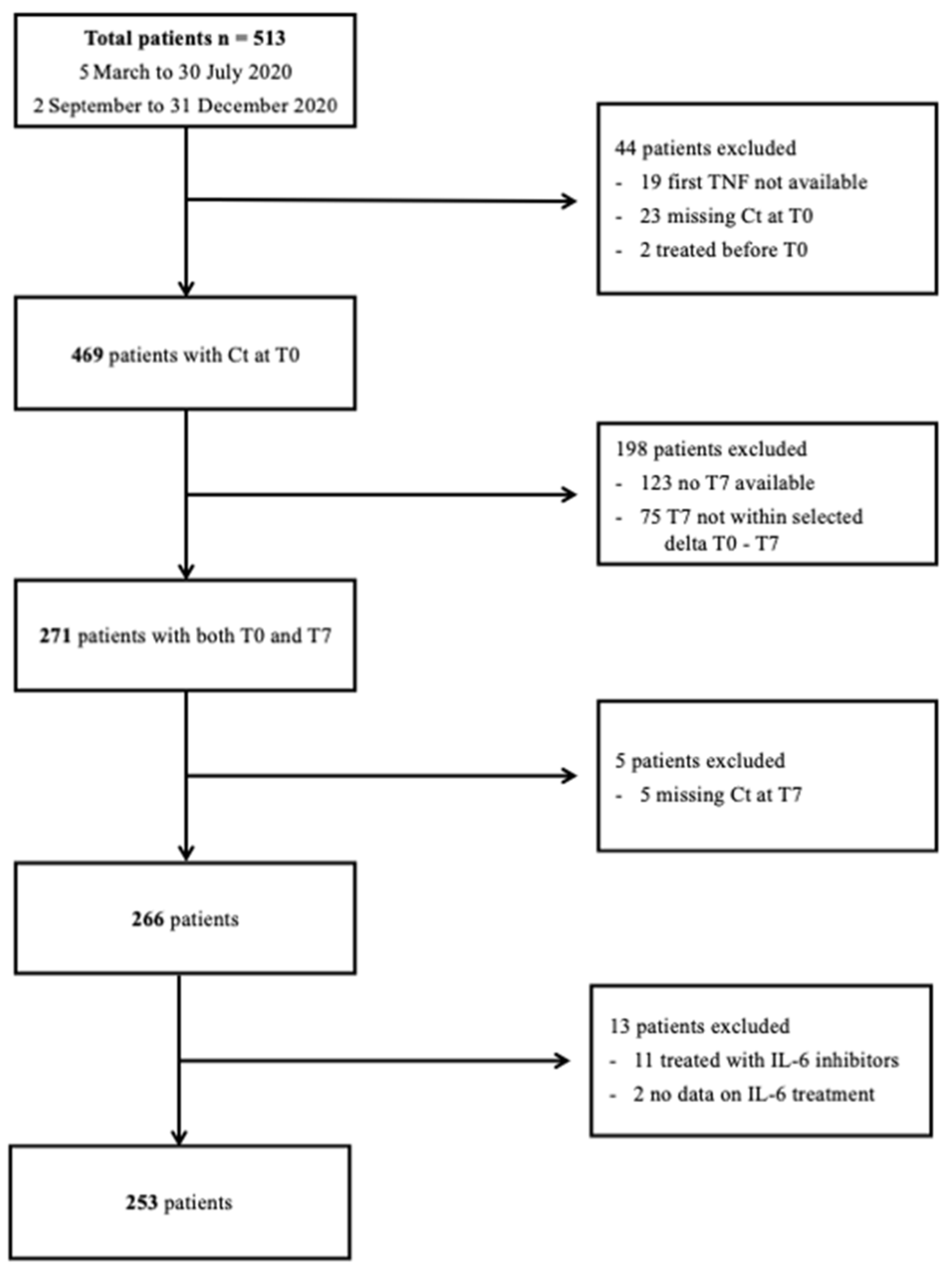
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Y.; Ye, D.; Liu, Q. Review of the 2019 Novel Coronavirus (SARS-CoV-2) Based on Current Evidence. Int. J. Antimicrob. Agents 2020, 55, 105948. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.-W.; Schmitz, J.E.; Persing, D.H.; Stratton, C.W. Laboratory Diagnosis of COVID-19: Current Issues and Challenges. J. Clin. Microbiol. 2020, 58, e00512-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, S.N.; Manissero, D.; Steele, V.R.; Pareja, J. A Systematic Review of the Clinical Utility of Cycle Threshold Values in the Context of COVID-19. Infect. Dis. Ther. 2020, 9, 573–586. [Google Scholar] [CrossRef] [PubMed]
- Hagman, K.; Hedenstierna, M.; Widaeus, J.; Arvidsson, E.; Hammas, B.; Grillner, L.; Jakobsson, J.; Gille-Johnson, P.; Ursing, J. Correlation of SARS-CoV-2 Nasopharyngeal CT Values With Viremia and Mortality in Adults Hospitalized With COVID-19. Open Forum Infect. Dis. 2022, 9, ofac463. [Google Scholar] [CrossRef] [PubMed]
- Kurzeder, L.; Jörres, R.A.; Unterweger, T.; Essmann, J.; Alter, P.; Kahnert, K.; Bauer, A.; Engelhardt, S.; Budweiser, S. A Simple Risk Score for Mortality Including the PCR Ct Value upon Admission in Patients Hospitalized Due to COVID-19. Infection 2022, 50, 1155–1163. [Google Scholar] [CrossRef]
- Dogan, L.; Allahverdiyeva, A.; Önel, M.; Meşe, S.; Saka Ersin, E.; Anaklı, İ.; Sarıkaya, Z.T.; Zengin, R.; Gucyetmez, B.; Yurtturan Uyar, N.; et al. Is SARS-CoV-2 Viral Load a Predictor of Mortality in COVID-19 Acute Respiratory Distress Syndrome Patients? J. Int. Med. Res. 2022, 50, 03000605221137443. [Google Scholar] [CrossRef]
- Gastine, S.; Pang, J.; Boshier, F.A.T.; Carter, S.J.; Lonsdale, D.O.; Cortina-Borja, M.; Hung, I.F.N.; Breuer, J.; Kloprogge, F.; Standing, J.F. Systematic Review and Patient-Level Meta-Analysis of SARS-CoV-2 Viral Dynamics to Model Response to Antiviral Therapies. Clin. Pharmacol. Ther. 2021, 110, 321–333. [Google Scholar] [CrossRef]
- Singh, T.U.; Parida, S.; Lingaraju, M.C.; Kesavan, M.; Kumar, D.; Singh, R.K. Drug Repurposing Approach to Fight COVID-19. Pharmacol. Rep. 2020, 72, 1479–1508. [Google Scholar] [CrossRef]
- Gordon, C.J.; Tchesnokov, E.P.; Woolner, E.; Perry, J.K.; Feng, J.Y.; Porter, D.P.; Götte, M. Remdesivir Is a Direct-Acting Antiviral That Inhibits RNA-Dependent RNA Polymerase from Severe Acute Respiratory Syndrome Coronavirus 2 with High Potency. J. Biol. Chem. 2020, 295, 6785–6797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and Chloroquine Effectively Inhibit the Recently Emerged Novel Coronavirus (2019-NCoV) In Vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Paño-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 Living Guidelines: Drug Treatment and Clinical Management. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2022, 28, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Update to Living WHO Guideline on Drugs for Covid-19. BMJ 2022, 378, o1713. [CrossRef]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.-C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, ciaa478. [Google Scholar] [CrossRef]
- Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Izcovich, A.; Kum, E.; Pardo-Hernandez, H.; Rochwerg, B.; Lamontagne, F.; Han, M.A.; et al. Drug Treatments for Covid-19: Living Systematic Review and Network Meta-Analysis. BMJ 2020, 370, m2980. [Google Scholar] [CrossRef]
- Remdesivir and Three Other Drugs for Hospitalised Patients with COVID-19: Final Results of the WHO Solidarity Randomised Trial and Updated Meta-Analyses. Lancet 2022, 399, 1941–1953. [CrossRef]
- Russo, P.; Tacconelli, E.; Olimpieri, P.P.; Celant, S.; Colatrella, A.; Tomassini, L.; Palù, G. Mortality in SARS-CoV-2 Hospitalized Patients Treated with Remdesivir: A Nationwide, Registry-Based Study in Italy. Viruses 2022, 14, 1197. [Google Scholar] [CrossRef]
- Diaz, G.A.; Christensen, A.B.; Pusch, T.; Goulet, D.; Chang, S.-C.; Grunkemeier, G.L.; McKelvey, P.A.; Robicsek, A.; French, T.; Parsons, G.T.; et al. Remdesivir and Mortality in Patients With Coronavirus Disease 2019. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 74, 1812–1820. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in Adults with Severe COVID-19: A Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial. Lancet Lond. Engl. 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium; Pan, H.; Peto, R.; Henao-Restrepo, A.-M.; Preziosi, M.-P.; Sathiyamoorthy, V.; Abdool Karim, Q.; Alejandria, M.M.; Hernández García, C.; Kieny, M.-P.; et al. Repurposed Antiviral Drugs for Covid-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- Bermejo-Martin, J.F.; González-Rivera, M.; Almansa, R.; Micheloud, D.; Tedim, A.P.; Domínguez-Gil, M.; Resino, S.; Martín-Fernández, M.; Ryan Murua, P.; Pérez-García, F.; et al. Viral RNA Load in Plasma Is Associated with Critical Illness and a Dysregulated Host Response in COVID-19. Crit. Care 2020, 24, 691. [Google Scholar] [CrossRef]
- Regan, J.; Flynn, J.P.; Rosenthal, A.; Jordan, H.; Li, Y.; Chishti, R.; Giguel, F.; Corry, H.; Coxen, K.; Fajnzylber, J.; et al. Viral Load Kinetics of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospitalized Individuals With Coronavirus Disease 2019. Open Forum Infect. Dis. 2021, 8, ofab153. [Google Scholar] [CrossRef] [PubMed]
- Biancofiore, A.; Mirijello, A.; Puteo, M.A.; Di Viesti, M.P.; Labonia, M.; Copetti, M.; De Cosmo, S.; Lombardi, R. CSS-COVID-19 Group Remdesivir Significantly Reduces SARS-CoV-2 Viral Load on Nasopharyngeal Swabs in Hospitalized Patients with COVID-19: A Retrospective Case-Control Study. J. Med. Virol. 2022, 94, 2284–2289. [Google Scholar] [CrossRef] [PubMed]
- Joo, E.J.; Ko, J.H.; Kim, S.E.; Kang, S.J.; Baek, J.H.; Heo, E.Y.; Shi, H.J.; Eom, J.S.; Choe, P.G.; Bae, S.; et al. Clinical and Virologic Effectiveness of Remdesivir Treatment for Severe Coronavirus Disease 2019 (COVID-19) in Korea: A Nationwide Multicenter Retrospective Cohort Study. J. Korean Med. Sci. 2021, 36, e83. [Google Scholar] [CrossRef]
- Goldberg, E.; Ben Zvi, H.; Sheena, L.; Sofer, S.; Krause, I.; Sklan, E.H.; Shlomai, A. A Real-Life Setting Evaluation of the Effect of Remdesivir on Viral Load in COVID-19 Patients Admitted to a Large Tertiary Centre in Israel. Clin. Microbiol. Infect. 2021, 27, 917.e1–917.e4. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Crichton, M.L.; Goeminne, P.C.; Tuand, K.; Vandendriessche, T.; Tonia, T.; Roche, N.; Chalmers, J.D. The Impact of Therapeutics on Mortality in Hospitalised Patients with COVID-19: Systematic Review and Meta-Analyses Informing the European Respiratory Society Living Guideline. Eur. Respir. Rev. 2021, 30, 210171. [Google Scholar] [CrossRef]
- Living Guidance for Clinical Management of COVID-19. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-clinical-2021–2 (accessed on 26 February 2022).
- Ansems, K.; Grundeis, F.; Dahms, K.; Mikolajewska, A.; Thieme, V.; Piechotta, V.; Metzendorf, M.-I.; Stegemann, M.; Benstoem, C.; Fichtner, F. Remdesivir for the Treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 8, CD014962. [Google Scholar] [CrossRef] [PubMed]
- Juul, S.; Nielsen, E.E.; Feinberg, J.; Siddiqui, F.; Jørgensen, C.K.; Barot, E.; Holgersson, J.; Nielsen, N.; Bentzer, P.; Veroniki, A.A.; et al. Interventions for Treatment of COVID-19: Second Edition of a Living Systematic Review with Meta-Analyses and Trial Sequential Analyses (The LIVING Project). PLoS ONE 2021, 16, e0248132. [Google Scholar] [CrossRef] [PubMed]
- Marrone, A.; Nevola, R.; Sellitto, A.; Cozzolino, D.; Romano, C.; Cuomo, G.; Aprea, C.; Schwartzbaum, M.X.P.; Ricozzi, C.; Imbriani, S.; et al. Remdesivir plus Dexamethasone versus Dexamethasone Alone for the Treatment of COVID-19 Patients Requiring Supplemental O2 Therapy: A Prospective Controlled Non-Randomized Study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, e403–e409. [Google Scholar] [CrossRef]
- Kouzy, R.; Abi Jaoude, J.; Garcia Garcia, C.J.; El Alam, M.B.; Taniguchi, C.M.; Ludmir, E.B. Characteristics of the Multiplicity of Randomized Clinical Trials for Coronavirus Disease 2019 Launched During the Pandemic. JAMA Netw. Open 2020, 3, e2015100. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Lau, K.T.K.; Au, I.C.H.; Xiong, X.; Lau, E.H.Y.; Cowling, B.J. Clinical Improvement, Outcomes, Antiviral Activity, and Costs Associated with Early Treatment with Remdesivir for Patients with COVID-19. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 74, 1450–1458. [Google Scholar] [CrossRef]
- Barratt-Due, A.; Olsen, I.C.; Nezvalova-Henriksen, K.; Kåsine, T.; Lund-Johansen, F.; Hoel, H.; Holten, A.R.; Tveita, A.; Mathiessen, A.; Haugli, M.; et al. Evaluation of the Effects of Remdesivir and Hydroxychloroquine on Viral Clearance in COVID-19. Ann. Intern. Med. 2021, 174, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Nasiri, M.J.; Haddadi, S.; Tahvildari, A.; Farsi, Y.; Arbabi, M.; Hasanzadeh, S.; Jamshidi, P.; Murthi, M.; Mirsaeidi, M. COVID-19 Clinical Characteristics, and Sex-Specific Risk of Mortality: Systematic Review and Meta-Analysis. Front. Med. 2020, 7, 459. [Google Scholar] [CrossRef]
- Hengeveld, P.J.; Khader, A.O.; de Bruin, L.H.A.; Geelen, I.G.P.; van Baalen, E.A.; Jansen, E.; Bouwer, N.I.; Balak, Ö.; Riedl, J.A.; Langerak, A.W.; et al. Blood Cell Counts and Lymphocyte Subsets of Patients Admitted during the COVID-19 Pandemic: A Prospective Cohort Study. Br. J. Haematol. 2020, 190, e201–e204. [Google Scholar] [CrossRef]
- He, Z.; Zhao, C.; Dong, Q.; Zhuang, H.; Song, S.; Peng, G.; Dwyer, D.E. Effects of Severe Acute Respiratory Syndrome (SARS) Coronavirus Infection on Peripheral Blood Lymphocytes and Their Subsets. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2005, 9, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Iannetta, M.; Buccisano, F.; Fraboni, D.; Malagnino, V.; Campogiani, L.; Teti, E.; Spalliera, I.; Rossi, B.; Di Lorenzo, A.; Palmieri, R.; et al. Baseline T-Lymphocyte Subset Absolute Counts Can Predict Both Outcome and Severity in SARS-CoV-2 Infected Patients: A Single Center Study. Sci. Rep. 2021, 11, 12762. [Google Scholar] [CrossRef] [PubMed]
- Leisman, D.E.; Ronner, L.; Pinotti, R.; Taylor, M.D.; Sinha, P.; Calfee, C.S.; Hirayama, A.V.; Mastroiani, F.; Turtle, C.J.; Harhay, M.O.; et al. Cytokine Elevation in Severe and Critical COVID-19: A Rapid Systematic Review, Meta-Analysis, and Comparison with Other Inflammatory Syndromes. Lancet Respir. Med. 2020, 8, 1233–1244. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. HLH Across Speciality Collaboration, UK COVID-19: Consider Cytokine Storm Syndromes and Immunosuppression. Lancet Lond. Engl. 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Zhang, X.; Tan, Y.; Ling, Y.; Lu, G.; Liu, F.; Yi, Z.; Jia, X.; Wu, M.; Shi, B.; Xu, S.; et al. Viral and Host Factors Related to the Clinical Outcome of COVID-19. Nature 2020, 583, 437–440. [Google Scholar] [CrossRef]
- Simons, L.M.; Lorenzo-Redondo, R.; Gibson, M.; Kinch, S.L.; Vandervaart, J.P.; Reiser, N.L.; Eren, M.; Lux, E.; McNally, E.M.; Tambur, A.R.; et al. Assessment of Virological Contributions to COVID-19 Outcomes in a Longitudinal Cohort of Hospitalized Adults. Open Forum Infect. Dis. 2022, 9, ofac027. [Google Scholar] [CrossRef]
- Fajnzylber, J.; Regan, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Worrall, D.; Giguel, F.; Piechocka-Trocha, A.; Atyeo, C.; et al. SARS-CoV-2 Viral Load Is Associated with Increased Disease Severity and Mortality. Nat. Commun. 2020, 11, 5493. [Google Scholar] [CrossRef] [PubMed]
- Magleby, R.; Westblade, L.F.; Trzebucki, A.; Simon, M.S.; Rajan, M.; Park, J.; Goyal, P.; Safford, M.M.; Satlin, M.J. Impact of Severe Acute Respiratory Syndrome Coronavirus 2 Viral Load on Risk of Intubation and Mortality Among Hospitalized Patients With Coronavirus Disease 2019. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e4197–e4205. [Google Scholar] [CrossRef]
- Knudtzen, F.C.; Jensen, T.G.; Lindvig, S.O.; Rasmussen, L.D.; Madsen, L.W.; Hoegh, S.V.; Bek-Thomsen, M.; Laursen, C.B.; Nielsen, S.L.; Johansen, I.S. SARS-CoV-2 Viral Load as a Predictor for Disease Severity in Outpatients and Hospitalised Patients with COVID-19: A Prospective Cohort Study. PLoS ONE 2021, 16, e0258421. [Google Scholar] [CrossRef]
- Shlomai, A.; Ben-Zvi, H.; Glusman Bendersky, A.; Shafran, N.; Goldberg, E.; Sklan, E.H. Nasopharyngeal Viral Load Predicts Hypoxemia and Disease Outcome in Admitted COVID-19 Patients. Crit. Care 2020, 24, 539. [Google Scholar] [CrossRef]
- Abdulrahman, A.; Mallah, S.I.; Alqahtani, M. COVID-19 Viral Load Not Associated with Disease Severity: Findings from a Retrospective Cohort Study. BMC Infect. Dis. 2021, 21, 688. [Google Scholar] [CrossRef]
- Liu, Y.; Liao, W.; Wan, L.; Xiang, T.; Zhang, W. Correlation Between Relative Nasopharyngeal Virus RNA Load and Lymphocyte Count Disease Severity in Patients with COVID-19. Viral Immunol. 2021, 34, 330–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckland, M.S.; Galloway, J.B.; Fhogartaigh, C.N.; Meredith, L.; Provine, N.M.; Bloor, S.; Ogbe, A.; Zelek, W.M.; Smielewska, A.; Yakovleva, A.; et al. Treatment of COVID-19 with Remdesivir in the Absence of Humoral Immunity: A Case Report. Nat. Commun. 2020, 11, 6385. [Google Scholar] [CrossRef] [PubMed]
- Sepulcri, C.; Dentone, C.; Mikulska, M.; Bruzzone, B.; Lai, A.; Fenoglio, D.; Bozzano, F.; Bergna, A.; Parodi, A.; Altosole, T.; et al. The Longest Persistence of Viable SARS-CoV-2 With Recurrence of Viremia and Relapsing Symptomatic COVID-19 in an Immunocompromised Patient—A Case Study. Open Forum Infect. Dis. 2021, 8, ofab217. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Xie, G.; Lin, S.; Wang, R.; Yang, X.; et al. Viral Load Dynamics and Disease Severity in Patients Infected with SARS-CoV-2 in Zhejiang Province, China, January-March 2020: Retrospective Cohort Study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yan, L.-M.; Wan, L.; Xiang, T.-X.; Le, A.; Liu, J.-M.; Peiris, M.; Poon, L.L.M.; Zhang, W. Viral Dynamics in Mild and Severe Cases of COVID-19. Lancet Infect. Dis. 2020, 20, 656–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, B.N.; Feldmann, F.; Schwarz, B.; Meade-White, K.; Porter, D.P.; Schulz, J.; van Doremalen, N.; Leighton, I.; Yinda, C.K.; Pérez-Pérez, L.; et al. Clinical Benefit of Remdesivir in Rhesus Macaques Infected with SARS-CoV-2. Nature 2020, 585, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Colagrossi, L.; Antonello, M.; Renica, S.; Merli, M.; Matarazzo, E.; Travi, G.; Vecchi, M.; Colombo, J.; Muscatello, A.; Grasselli, G.; et al. SARS-CoV-2 RNA in Plasma Samples of COVID-19 Affected Individuals: A Cross-Sectional Proof-of-Concept Study. BMC Infect. Dis. 2021, 21, 184. [Google Scholar] [CrossRef]
- Lai, A.; Bergna, A.; Menzo, S.; Zehender, G.; Caucci, S.; Ghisetti, V.; Rizzo, F.; Maggi, F.; Cerutti, F.; Giurato, G.; et al. Circulating SARS-CoV-2 Variants in Italy, October 2020–March 2021. Virol. J. 2021, 18, 168. [Google Scholar] [CrossRef] [PubMed]
- Bozidis, P.; Tsaousi, E.T.; Kostoulas, C.; Sakaloglou, P.; Gouni, A.; Koumpouli, D.; Sakkas, H.; Georgiou, I.; Gartzonika, K. Unusual N Gene Dropout and Ct Value Shift in Commercial Multiplex PCR Assays Caused by Mutated SARS-CoV-2 Strain. Diagn. Basel Switz. 2022, 12, 973. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Overall Population (N = 253) | Remdesivir (R) (N = 123; 48.6%) | Protease Inhibitors (PI) (N = 67; 26.5%) | No Treatment (NT) (N = 63; 24.9%) | p | |
|---|---|---|---|---|---|
| Age: median (IQR) | 64 (53–77) | 67 (58.5–76.5) | 64 (51–81.5) | 55 (44.5–75.5) | 0.004 |
| Sex: M/F | 164/89 (64.8/35.2) | 89/34 (72.4/27.6) | 36/31 (53.7/46.3) | 39/24 (61.9/38.9) | 0.032 |
| Time from symptoms’ onset to T0 NPhS: median (IQR) * | 7 (3–10) | 7 (4–9.75) | 6 (2–10.50) | 6 (7.50–9.50) | 0.316 |
| Non-severe/severe | 150/103 (59.3/40.7) | 43/80 (35/65) | 53/14 (79.1/20.9) | 54/9 (85.7/14.3) | <0.001 |
| ICU admission | 19 (7.5) | 14 (11.4) | 5 (7.5) | 0 | 0.021 |
| Survivors/non-survivors | 217/36 (85.7/14.3) | 102/21 (82.9/17.1) | 58/9 (86.6/13.4) | 57/6 (90.5/9.5) | 0.369 |
| Corticosteroid treatment | 150 (59.3) | 119 (96.7) | 16 (23.9) | 15 (23.8) | <0.001 |
| Comorbidities | |||||
| Any | 216 (85.4) | 108 (87.8) | 55 (82.1) | 53 (84.1) | 0.538 |
| Obesity | 44 (17.4) | 31 (25.2) | 7 (10.4) | 6 (9.5) | 0.006 |
| Cardiovascular | 145 (57.3) | 81 (65.8) | 36 (53.7) | 28 (44.4) | 0.016 |
| Diabetes | 61 (24.1) | 36 (29.3) | 13 (19.4) | 12 (19.1) | 0.175 |
| Endocrinologic | 32 (12.6) | 16 (13) | 9 (13.4) | 7 (11.1) | 0.911 |
| Cerebrovascular | 21 (8.3) | 14 (11.4) | 4 (5.9) | 3 (4.7) | 0.218 |
| Chronic viral hepatitis | 3 (1.2) | 1 (0.8) | 1 (1.5) | 1(1.5) | 0.867 |
| Pulmonary | 30 (11.8) | 18 (14.6) | 8 (11.9) | 4 (6.4) | 0.255 |
| Renal | 19 (7.5) | 3 (2.4) | 6 (8.9) | 10 (15.8) | 0.004 |
| Solid Tumor | 34 (13.4) | 18 (14.6) | 11 (16.4) | 5 (7.9) | 0.316 |
| Hematologic | 21 (8.3) | 11 (8.9) | 7 (10.4) | 3 (4.7) | 0.470 |
| Neurologic/Psychiatric | 43 (16.9) | 13 (10.6) | 15 (22.3) | 15 (23.8) | 0.029 |
| Rheumatologic | 17 (6.7) | 8 (6.5) | 3 (4.5) | 6 (9.5) | 0.513 |
| Other | 49 (19.3) | 19 (15.4) | 15 (22.3) | 15 (23.8) | 0.302 |
| Survivors (N = 217; 85.7%) | Non-Survivors (N = 36; 14.3%) | p | Corticosteroid (N = 150; 59.3%) | No Corticosteroid (N = 103; 40.7%) | p | |
|---|---|---|---|---|---|---|
| T0 NPh swab | ||||||
| Median Ct E | 26.87 (22.14–32.03) | 21.48 (17.27–26.75) | <0.001 | 26.74 (22.17–31.11) | 25.19 (19.07–33.15) | 0.364 |
| Median Ct N | 26.52 (21.94–31.62) | 21.55 (16.76–26.92) | <0.001 | 25.56 (21.48–30.45) | 26.71 (20.45–33.69) | 0.361 |
| Median Ct RdRP | 27.41 (22.68–32.46) | 22.25 (17.56–28.95) | 0.002 | 27.26 (22.62–32.05) | 26.39 (20.54–32.65) | 0.390 |
| T7 NPh swab | ||||||
| Median Ct E | 34.44 (29.26–45.00) | 25.20 (20.88–31.51) | <0.001 | 33.51 (28.44–37.90) | 34.14 (26.66–45.00) | 0.277 |
| Median Ct N | 33.34 (28.88–37.39) | 25.25 (21.21–31.13) | <0.001 | 32.07 (26.62–36.67) | 33.50 (27.71–38.17) | 0.129 |
| Median Ct RdRP | 34.98 (30.09–45.00) | 26.07 (21.60–31.56) | <0.001 | 33.82 (28.91–45.00) | 33.80 (27.69–45.00) | 0.842 |
| Viral decay (T7-T0) | ||||||
| Median ΔCt E | 7.29 (1.50–12.03) | 5.15 (−0.35–9.12) | 0.084 | 7.10 (2.44–10.47) | 7.79 (0.00–14.78) | 0.497 |
| Median ΔCt N | 6.60 (2.83–10.90) | 4.48 (−0.96–8.58) | 0.050 | 6.43 (2.80–10.18) | 5.98 (2.64–10.91) | 0.937 |
| Median ΔCt RdRP | 7.27 (2.67–11.98) | 5.00 (−1.53–8.43) | 0.018 | 6.95 (2.80–10.32) | 7.08 (0.93–13.51) | 0.817 |
| Median Ct E T0 | Median CT N T0 | Median Ct RdRP T0 | Median Delta Ct E | Median Delta CT N | Median Delta Ct RdRP | |
|---|---|---|---|---|---|---|
| Age | −0.060 p = 0.339 | −0.092 p = 0.143 | −0.063 p = 0.320 | −0.060 p = 0.344 | −0.075 p = 0.235 | −0.084 p = 0.185 |
| Comorbidity score | −0.095 p = 0.133 | −0.122 p = 0.053 | −0.090 p = 0.152 | −0.022 p = 0.731 | −0.042 p = 0.508 | −0.038 p = 0.542 |
| IL−6 | −0.132 p = 0.047 | −0.106 p = 0.112 | −0.131 p = 0.048 | 0.023 p = 0.726 | 0.010 p = 0.883 | −0.006 p = 0.923 |
| D-dimer | 0.170 p = 0.011 | 0.102 p = 0.127 | 0.161 p = 0.016 | −0.127 p = 0.057 | −0.025 p = 0.713 | −0.110 p = 0.100 |
| CRP | 0.063 p = 0.335 | 0.034 p = 0.602 | 0.081 p = 0.213 | −0.004 p = 0.952 | −0.0008 p = 0.990 | −0.014 p = 0.826 |
| Fibrinogen | 0.160 p = 0.016 | 0.150 p = 0.024 | 0.147 p = 0.027 | 0.036 p = 0.588 | 0.039 p = 0.555 | 0.055 p = 0.406 |
| Lymphocyte total count (T0) | 0.032 p = 0.620 | 0.084 p = 0.193 | 0.037 p = 0.570 | 0.128 p = 0.047 | 0.092 p = 0.153 | 0.108 p = 0.092 |
| Lymphocyte subpopulation (T0) | ||||||
| CD3+ # | 0.042 p = 0.512 | 0.099 p = 0.120 | 0.051 p = 0.425 | 0.138 p = 0.029 | 0.124 p = 0.051 | 0.134 p = 0.034 |
| CD3 + CD4+ # | 0.046 p = 0.472 | 0.102 p = 0.109 | 0.056 p = 0.379 | 0.140 p = 0.027 | 0.147 p = 0.020 | 0.139 p = 0.028 |
| CD3 + CD8+ # | 0.034 p = 0.595 | 0.087 p = 0.171 | 0.036 p = 0.571 | 0.120 p = 0.058 | 0.094 p = 0.138 | 0.124 p = 0.050 |
| CD19+ # | 0.188 p = 0.003 | 0.198 p = 0.002 | 0.179 p = 0.005 | 0.001 p = 0.958 | 0.023 p = 0.713 | 0.016 p = 0.795 |
| CD3-CD16 + CD56+ # | −0.099 p = 0.118 | −0.053 p = 0.408 | −0.078 p = 0.223 | 0.049 p = 0.440 | 0.031 p = 0.628 | 0.028 p = 0.664 |
| CD4/CD8 ratio | 0.039 p = 0.544 | 0.023 p = 0.713 | 0.037 p = 0.563 | −0.005 p = 0.940 | 0.059 p = 0.352 | 0.007 p = 0.918 |
| All Patients (N= 253) | Remdesivir (R) (N = 123; 48.6%) | Protease Inhibitors (PI) (N = 67; 26.5%) | No Treatment (NT) (N = 63; 24.9%) | p | |
|---|---|---|---|---|---|
| T0 NPh swab | |||||
| Median Ct E | 26.34 (21.09–31.53) | 26.26 (22.12–30.3) | 27.52 (22.42–34.94) | 24.4 (18.62–34.54) | 0.159 |
| Median Ct N | 25.97 (21.30–30.83) | 24.81 (21.43–29.6) | 29.78 (24.95–34.49) | 23.49 (18.69–33.45) | <0.001 |
| Median Ct RdRP | 21.17 (21.97–32.20) | 27.07 (22.59–31.62) | 28.02 (23.88–32.72) | 25.88 (19.00–34.76) | 0.392 |
| T7 NPh swab | |||||
| Median Ct E | 33.73 (27.17–45.00) | 33.79 (29.12–37.7) | 45.00 (28.00–45.00) | 31.47 (23.895–45.00) | 0.078 |
| Median Ct N | 32.92 (27.01–37.09) | 32.01 (27.14–35.11) | 34.97 (30.47–39.04) | 30.72 (25.15–37.59) | 0.019 |
| Median Ct RdRP | 33.80 (28.49–45.00) | 34.31 (29.75–38.98) | 34.95 (29.46–45.00) | 32.88 (25.00–45.00) | 0.280 |
| Viral decay (T7-T0) | |||||
| Median Ct E | 7.25 (1.25–11.78) | 7.46 (3.71–10.61) | 7.53 (0.00–16.65) | 5.72 (0.00–10.52) | 0.357 |
| Median Ct N | 6.42 (2.65–10.43) | 6.51 (2.85–10.82) | 5.73 (2.20–10.23) | 6.60 (2.78–9.89) | 0.646 |
| Median Ct RdRP | 7.02 (2.16–11.26) | 7.66 (3.33–10.77) | 6.37 (0.93–15.14) | 5.91 (0.00–9.37) | 0.233 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campogiani, L.; Iannetta, M.; Di Lorenzo, A.; Zordan, M.; Pace, P.G.; Coppola, L.; Compagno, M.; Malagnino, V.; Teti, E.; Andreoni, M.; et al. Remdesivir Influence on SARS-CoV-2 RNA Viral Load Kinetics in Nasopharyngeal Swab Specimens of COVID-19 Hospitalized Patients: A Real-Life Experience. Microorganisms 2023, 11, 312. https://doi.org/10.3390/microorganisms11020312
Campogiani L, Iannetta M, Di Lorenzo A, Zordan M, Pace PG, Coppola L, Compagno M, Malagnino V, Teti E, Andreoni M, et al. Remdesivir Influence on SARS-CoV-2 RNA Viral Load Kinetics in Nasopharyngeal Swab Specimens of COVID-19 Hospitalized Patients: A Real-Life Experience. Microorganisms. 2023; 11(2):312. https://doi.org/10.3390/microorganisms11020312
Chicago/Turabian StyleCampogiani, Laura, Marco Iannetta, Andrea Di Lorenzo, Marta Zordan, Pier Giorgio Pace, Luigi Coppola, Mirko Compagno, Vincenzo Malagnino, Elisabetta Teti, Massimo Andreoni, and et al. 2023. "Remdesivir Influence on SARS-CoV-2 RNA Viral Load Kinetics in Nasopharyngeal Swab Specimens of COVID-19 Hospitalized Patients: A Real-Life Experience" Microorganisms 11, no. 2: 312. https://doi.org/10.3390/microorganisms11020312