

Increased Susceptibility for Thromboembolic Events versus High Bleeding Risk Associated with COVID-19
 , and
, and
Abstract
:1. Introduction
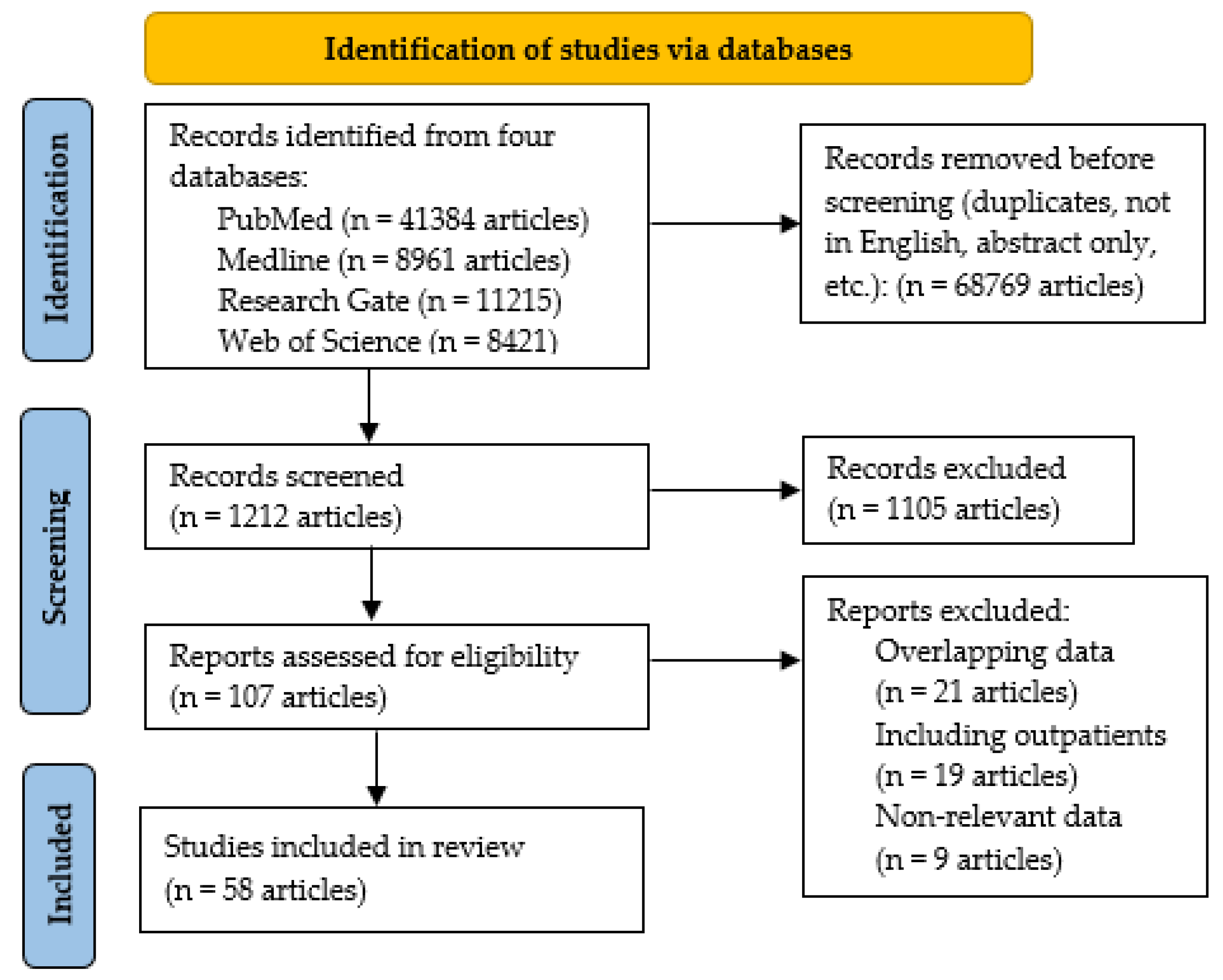
2. Materials and Methods
3. Results
3.1. Thrombotic Events in the Acute Phase of COVID-19

{kind=link}
{kind=link}
| Authors/Year | Study Type | No. of Studies/Patients | ICU | VTE | Prophylaxis AC | Comments |
|---|---|---|---|---|---|---|
| Lee et al./2022 [37] | Multicenter retrospective study | 3531 | ICU/ward | 6.68% | 88.55% | Increased hospitalization |
| Parks et al./2022 [38] | Multicenter cross-sectional study | 1121 | ICU/Ward | 8.8% | 86% | 2.1% AT; 4.1% major and 4.1% minor bleedings |
| Tamayo-Velasco et al./2022 [35] | Retrospective cohort study | 2894 | 10.85% ICU | 3.45% | 100% | 1.8% AT |
| Boyd et al./2022 [39] | Retrospective study | 128 | All ICU | 30% | 98.18% | Increased risk of VTE despite prophylaxis |
| Ontiveros et al./2022 [40] | Retrospective case series | 1/36 | 69% ICU | 1.8% (36 cases out of 2000) | 97.22% | Overall mortality was 55.6%. |
| Jimenez et al./2021 [10] | Meta-analysis | 47 out of 49 studies/18,093 | ICU/Ward | 17.3% | 100% | Bleedings prevalence 3.9% |
| Fontelo et al./2021 [11] | Meta-analysis | 19/2554 | ICU/Ward | 28% | 93.5% | Increased prevalence in ICU cases |
| Oba et al./2021 [41] | Retrospective single-center study | 1/516 | ICU/Ward | 4.26 | 100% | 3.8% AT |
| Munoz Rivas et al./2021 [28] | Retrospective single-center study | 1/1127 | Non-ICU | 6.1 | 100% | 1.6% AT |
| Perepu et al. [42] | Randomized control study | 176 | ICU/Ward | 13% | 100% | 2% major bleedings |
| Hasan et al./2020 [36] | Meta-analysis | 12/899 | ICU/Ward | 31% | 100% | High prevalence of VTE despite prophylaxis |
| Piazza et al./2020 [43] | Retrospective cohort study | 1/1114 | 15.26% ICU | 27% ICU 2.2% non-ICU | 89.4% | 2.6% AT |
| Bilaloglu et al./2020 [44] | Retrospective cohort study | 1/3334 | 24.86% (829 ICUpatients) | 6.2% | LMWH prophylaxis | 11.1% AT |
| Malas et al./2020 [6] | Meta-analysis | 42/8271 | ICU/Ward | 21% | Almost all patients | 2% AT; higher mortality |
| Fontana et al./2020 [34] | Meta-analysis | 11/1369 | 6 studies only ICU | General: 4.4–8.2%. ICU: 35.3% | ~100% | Higher prevalence in ICU, up to 53.8% |
| Chi et al./2020 [45] | Meta-analysis | 11/1981 | 5 studies only ICU, 6 studies only ward (10%-38% needed ICU) | 23.9% (11.9% DVT/11.9% PE) | 100% | VTE-30.4%-ICU 13% in ward. PE: 15.7% in ICU, 2.4% in non-ICU |
| Wang et al./2020 [46] | Meta-analysis | 28/4138 | Reported for 20 studies | 16% (all DVT) | Between 30 and 100% | 23% ICU vs. 5% in non-ICU; China 30%/13% in western countries |
| Potere et al./2020 [9] | Meta-analysis | 44/14.866 | 34% ICU | 34% in ICU; 15% non-ICU | Not Reported | Overall mortality 10% |
| Klok et al./2020 [47] | Cohort study | 184 | 100% ICU | 31% | 100% | AT 1.6% |
| Whyte and al./2020 [48] | Cohort study | 1477 | ICU/Ward | 27% | 100% | 5.4% PE non-ICU 16.7–47% ICU |
| Lodigiani et al./2020 [49] | Retrospective cohort study | 388 | ICU/Ward | 27.6% ICU 6.6% ward | 100% | 2.5% AT 2.1% bleeding |
| Trimaille et al./2020 [50] | Cohort study | 289 | Ward | 17% | 89.3% | Increased likelihood of ICU stay |
| Leonard-Lorant et al./2020 [51] | Retrospective cohort study | 1/1696 | 45.28% overall (75% of cases with VTE) | 30% (all PE) | 46.2% overall | Thorax angio-CT study |
| Wichmann et al./2020 [52] | Prospective autopsy cohort study | 1/12 | 41.66% (5 died after treatment in ICU) | 58% (7 cases had DVT and PE in 4) | Not Reported | DVT and PE were found at autopsy in 4 patients |
| Authors/Year | Study Type | No. of Studies/Patients | ICU | AT | Prophylaxis | Commentary |
|---|---|---|---|---|---|---|
| Ilonzo et al./2021 [54] | Retrospective case series | 1/21 hospitalized | Not reported | 76.2% | 76.2% of patients on antiplatelet and 19.1% on AC before admission | all patients had an acute thrombotic event, 76.2% AT and 23.8% DVT |
| Mao et al./2020 [55] | Retrospective observational case series | 1/214 | Not reported | 5.7% | Not Reported | stroke was documented in 5.7%. |
| Bellosta et al./2020 [56] | Retrospective observational case series | 1/20 | Not reported | All patients included | 25% on chronic AC due to AF | 16.3% AT, significantly higher than pre-COVID |
| Perini et al./2020 [57] | Retrospective observational case series | 1/4 | Not reported | All patients included | LMWH prophylaxis | All patients despite thromboprophylaxis; 2 were young (53 and 37 years). |
| Oxley et al./2020 [58] | Retrospective observational case series | 1/5 | 2 patients | All patients included | Not clearly reported | All patients had ischemic stroke and were under 50 |
| Morassi et al./2020 [59] | Retrospective observational case series | 1/6 | 83% | All patients included | 3 patients (50%) | All patients developed stroke and 5 died |
3.2. Alterations of Hemostasis
3.3. Disseminated Intravascular Coagulopathy
3.4. Major Bleedings
| Authors/Year | Study Type | Number of Studies/Patients | ICU | Prevalence of Hemorrhagic Events | Thromboprophylaxis | Comments |
|---|---|---|---|---|---|---|
| Valeriani et al./2022 [70] | Meta-analysis | 9/5470 | ICU/Ward | 2.5% therapeutic 1.4% prophylaxis | 100% | VTE 2.9% high dose and 5.7% prophylaxis |
| Wang et al./2022 [8] | Retrospective single-center study | 138 | ICU/Ward | 4.3% Ward 26.7% in ICU | 100% | 16.67% VTE |
| Helmy et al./2022 [71] | Prospective observational study | 114 | ICU/Ward | 15.8% | 100% | 13.2% VTE, 4.4% AT |
| Trindade et al./2021 [68] | Multicenter cohort study | 11, 158 | ICU/Ward | 3% | Almost all | Gastrointestinal bleeding was associated with high mortality |
| Zellmer et al./2021 [69] | Retrospective multicenter cohort study | 5344 | ICU/non-ICU | 1.8% 4.5% in ICU | Almost all | Higher mortality |
| Al Raizah et al./2021 [72] | Multicenter study | 636 | ICU/Ward | 1.7% 9.4% in ICU | 90% | 1.8% VTE 2.2% AT |
| Halaby et al./2021 [73] | Retrospective cohort study | 443 | ICU | 18.2% | 100–76.2% therapeutic | Higher risk for therapeutic dose |
| Godier et al./2021 [74] | Retrospective study | 56 | All ICU | 18% | 100–75% therapeutic | 29% VTE |
| Boira et al./2021 [17] | Series of cases | 4 | ICU/Ward | All | All | Equal prevalence between genders |
| Al-Samkari et al./2020 [23] | Retrospective multicenter study | 400 | ICU/Ward | 7.6%/4.8% | All except one | 6% VTE 2.8% AT |
| Fraisse et al./2020 [75] | Monocenter retrospective study | 92 | ICU | 21% | All-prophylactic or therapeutic dose | 40% VTE in ICU patients |
| Nadkarni et al./2020 [60] | Prospective multicenter study | 153 of 4389 | Non-ICU | 5.6% | 65.1% prophylactic or therapeutic dose | 3% in subjects with therapeutic AC dose |
3.5. Hematomas
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19---11-march-2020 (accessed on 1 December 2020).
- Raoult, D.; Zumla, A.; Locatelli, F.; Ippolito, G.; Kroemer, G. Coronavirus Infections: Epidemiological, Clinical and Immunological Features and Hypotheses. Cell Stress 2020, 4, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.D.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef] [PubMed]
- Marietta, M.; Ageno, W.; Artoni, A.; De Candia, E.; Gresele, P.; Marchetti, M.; Marcucci, R.; Tripodi, A. COVID-19 and Haemostasis: A Position Paper from Italian Society on Thrombosis and Haemostasis, SISET. Blood Transfus. 2020, 18, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Mazzolai, L.; Aboyans, V.; Ageno, W.; Agnelli, G.; Alatri, A.; Bauersachs, R.; Brekelmans, M.P.A.; Büller, H.R.; Elias, A.; Farge, D.; et al. Diagnosis and Management of Acute Deep Vein Thrombosis: A Joint Consensus Document from the European Society of Cardiology Working Groups of Aorta and Peripheral Vascular Diseases and Pulmonary Circulation and Right Ventricular Function. Eur. Heart J. 2018, 39, 4208–4218. [Google Scholar] [CrossRef]
- Malas, M.B.; Naazie, I.N.; Elsayed, N.; Mathlouthi, A.; Marmor, R.; Clary, B. Thromboembolism Risk of COVID-19 Is High and Associated with a Higher Risk of Mortality: A Systematic Review and Meta-Analysis. eClinicalMedicine 2020, 29–30, 100639. [Google Scholar] [CrossRef]
- CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis); Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; et al. High Risk of Thrombosis in Patients with Severe SARS-CoV-2 Infection: A Multicenter Prospective Cohort Study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Xu, J.; Wang, L.; Zhao, L.; Li, F.; Liu, J.; Zhang, L.; Li, Q.; Gu, J.; Liang, S.; Zhao, Q.; et al. Risk Assessment of Venous Thromboembolism and Bleeding in COVID-19 Patients. Clin. Respir. J. 2022, 16, 182–189. [Google Scholar]
- Potere, N.; Valeriani, E.; Candeloro, M.; Tana, M.; Porreca, E.; Abbate, A.; Spoto, S.; Rutjes, A.W.S.; Di Nisio, M. Acute Complications and Mortality in Hospitalized Patients with Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Crit. Care 2020, 24, 389. [Google Scholar] [CrossRef]
- Jiménez, D.; García-Sanchez, A.; Rali, P.; Muriel, A.; Bikdeli, B.; Ruiz-Artacho, P.; Le Mao, R.; Rodríguez, C.; Hunt, B.J.; Monreal, M. Incidence of VTE and Bleeding Among Hospitalized Patients With Coronavirus Disease 2019. Chest 2021, 159, 1182–1196. [Google Scholar] [CrossRef]
- Fontelo, P.; Bastola, M.M.; Zheng, Z.; Baik, S.H. A Review of Thromboembolic Events in Hospitalized COVID-19 Patients. Thromb. J. 2021, 19, 47. [Google Scholar] [CrossRef]
- Nopp, S.; Moik, F.; Jilma, B.; Pabinger, I.; Ay, C. Risk of Venous Thromboembolism in Patients with COVID-19: A Systematic Review and Meta-analysis. Res. Pr. Thromb. Haemost. 2020, 4, 1178–1191. [Google Scholar] [CrossRef] [PubMed]
- Ohn, M.H.; Ng, J.R.; Ohn, K.M.; Luen, N.P. Double-Edged Sword Effect of Anticoagulant in COVID-19 Infection. BMJ Case Rep. CP 2021, 14, e241955. [Google Scholar] [CrossRef]
- Atallah, B.; Sadik, Z.G.; Salem, N.; El Nekidy, W.S.; Almahmeed, W.; Park, W.M.; Cherfan, A.; Hamed, F.; Mallat, J. The Impact of Protocol-based High-intensity Pharmacological Thromboprophylaxis on Thrombotic Events in Critically Ill COVID-19 Patients. Anaesthesia 2021, 76, 327–335. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Haematology COVID-19 Coagulopathy: An Evolving Story. Lancet Haematol. 2020, 7, e425. [CrossRef]
- Becker, R.C. COVID-19 Update: COVID-19-Associated Coagulopathy. J Thromb Thrombolysis 2020, 50, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Boira, I.; Esteban, V.; Vañes, S.; Castelló, C.; Celis, C.; Chiner, E. Major Bleeding Complications in COVID-19 Patients. Cureus 2021, 13, e16816. [Google Scholar] [CrossRef]
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin. Appl. Thromb. Hemost. 2020, 26, 1–7. [Google Scholar] [CrossRef]
- Benazzi, D.; Antonicelli, V.; Presciuttini, B.; Foroni, E.; Bellini, M.; Smurra, A.; Bianco, C.; Amato, M. COVID-19 and Hemorrhagic Complications: Pectoral Hematoma. Ital. J. Emerg. Med. 2021, 10, 6–10. [Google Scholar] [CrossRef]
- Palumbo, D.; Guazzarotti, G.; De Cobelli, F. Spontaneous Major Hemorrhage in COVID-19 Patients: Another Brick in the Wall of SARS-CoV-2–Associated Coagulation Disorders? J. Vasc. Interv. Radiol. 2020, 31, 1494–1496. [Google Scholar] [CrossRef]
- Taleja, H.; Nair, V.V.; Yadav, S.; Venkatnarayanan, R.; Roy, N.; Rao, P. Spontaneous Hematomas in COVID-19 Patients on Low-Molecular-Weight Heparin. Dubai Med. J. 2021, 4, 285–290. [Google Scholar] [CrossRef]
- Manjili, R.H.; Zarei, M.; Habibi, M.; Manjili, M.H. COVID-19 as an Acute Inflammatory Disease. J. Immunol. 2020, 205, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and Coagulation: Bleeding and Thrombotic Manifestations of SARS-CoV-2 Infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider Cytokine Storm Syndromes and Immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Chan, N.C.; Weitz, J.I. COVID-19 Coagulopathy, Thrombosis, and Bleeding. Blood 2020, 136, 381–383. [Google Scholar] [CrossRef]
- Arévalos, V.; Ortega-Paz, L.; Rodríguez-Arias, J.J.; Calvo López, M.; Castrillo-Golvano, L.; Salazar-Rodríguez, A.; Sabaté-Tormos, M.; Spione, F.; Sabaté, M.; Brugaletta, S. Acute and Chronic Effects of COVID-19 on the Cardiovascular System. J. Cardiovasc. Dev. Dis. 2021, 8, 128. [Google Scholar] [CrossRef]
- Xiong, T.-Y.; Redwood, S.; Prendergast, B.; Chen, M. Coronaviruses and the Cardiovascular System: Acute and Long-Term Implications. Eur. Heart J. 2020, 41, 1798–1800. [Google Scholar] [CrossRef]
- Muñoz-Rivas, N.; Abad-Motos, A.; Mestre-Gómez, B.; Sierra-Hidalgo, F.; Cortina-Camarero, C.; Lorente-Ramos, R.M.; Torres-Rubio, P.; Arranz-García, P.; Franco-Moreno, A.I.; Gómez-Mariscal, E.; et al. Systemic Thrombosis in a Large Cohort of COVID-19 Patients despite Thromboprophylaxis: A Retrospective Study. Thromb. Res. 2021, 199, 132–142. [Google Scholar] [CrossRef]
- Zhai, Z.; Li, C.; Chen, Y.; Gerotziafas, G.; Zhang, Z.; Wan, J.; Liu, P.; Elalamy, I.; Wang, C.; On behalf of the Prevention Treatment of VTE Associated with COVID-19 Infection Consensus Statement Group. Prevention and Treatment of Venous Thromboembolism Associated with Coronavirus Disease 2019 Infection: A Consensus Statement before Guidelines. Thromb. Haemost. 2020, 120, 937–948. [Google Scholar] [CrossRef]
- Cuker, A.; Tseng, E.K.; Nieuwlaat, R.; Angchaisuksiri, P.; Blair, C.; Dane, K.; DeSancho, M.T.; Diuguid, D.L.; Griffin, D.O.; Kahn, S.R.; et al. American Society of Hematology Living Guidelines on the Use of Anticoagulation for Thromboprophylaxis in Patients with COVID-19: January 2022 Update on the Use of Therapeutic-Intensity Anticoagulation in Acutely Ill Patients. Blood Adv. 2022, online. [Google Scholar] [CrossRef]
- Lauzier, F.; Arnold, D.M.; Rabbat, C.; Heels-Ansdell, D.; Zarychanski, R.; Dodek, P.; Ashley, B.J.; Albert, M.; Khwaja, K.; Ostermann, M.; et al. Risk Factors and Impact of Major Bleeding in Critically Ill Patients Receiving Heparin Thromboprophylaxis. Intensive Care Med. 2013, 39, 2135–2143. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Connors, J.M.; Warkentin, T.E.; Thachil, J.; Levi, M. The Unique Characteristics of COVID-19 Coagulopathy. Crit. Care 2020, 24, 360. [Google Scholar] [CrossRef] [PubMed]
- Antithrombotic Therapy. Available online: https://www.covid19treatmentguidelines.nih.gov/therapies/antithrombotic-therapy/ (accessed on 26 July 2022).
- Fontana, P.; Casini, A.; Robert-Ebadi, H.; Glauser, F.; Righini, M.; Blondon, M. Venous Thromboembolism in COVID-19: Systematic Review of Reported Risks and Current Guidelines. Swiss Med Wkly. 2020, 150, w20301. [Google Scholar] [CrossRef] [PubMed]
- Tamayo-Velasco, Á.; Bombín-Canal, C.; Cebeira, M.J.; Sánchez-De Prada, L.; Miramontes-González, J.P.; Martín-Fernández, M.; Peñarrubia-Ponce, M.J. Full Characterization of Thrombotic Events in All Hospitalized COVID-19 Patients in a Spanish Tertiary Hospital during the First 18 Months of the Pandemic. J. Clin. Med. 2022, 11, 3443. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.S.; Radford, S.; Kow, C.S.; Zaidi, S.T.R. Venous Thromboembolism in Critically Ill COVID-19 Patients Receiving Prophylactic or Therapeutic Anticoagulation: A Systematic Review and Meta-Analysis. J. Thromb. Thrombolysis 2020, 50, 814–821. [Google Scholar] [CrossRef]
- Lee, Y.; Jehangir, Q.; Li, P.; Gudimella, D.; Mahale, P.; Lin, C.-H.; Apala, D.R.; Krishnamoorthy, G.; Halabi, A.R.; Patel, K.; et al. Venous Thromboembolism in COVID-19 Patients and Prediction Model: A Multicenter Cohort Study. BMC Infect. Dis. 2022, 22, 462. [Google Scholar] [CrossRef]
- Parks, A.L.; Auerbach, A.D.; Schnipper, J.L.; Bertram, A.; Jeon, S.Y.; Boyle, B.; Fang, M.C.; Gadrey, S.M.; Siddiqui, Z.K.; Brotman, D.J.; et al. Venous Thromboembolism (VTE) Prevention and Diagnosis in COVID-19: Practice Patterns and Outcomes at 33 Hospitals. PLoS ONE 2022, 17, e0266944. [Google Scholar] [CrossRef]
- Boyd, S.; Martin-Loeches, I. The Incidence of Venous Thromboembolism in Critically Ill Patients with COVID-19 Compared with Critically Ill Non-COVID Patients. Ir. J. Med. Sci. 2021, 190, 1317–1320. [Google Scholar] [CrossRef]
- Ontiveros, N.; Becerril-Gaitan, A.; Llausas-Villarreal, A.; Gonzalez-Urquijo, M.; Paredes-Vazquez, J.G.; Martínez-Resendez, M.F.; Fabiani, M.A. Venous Thromboembolism in Hospitalized COVID-19 Patients Treated in a Single Academic Center in Mexico: A Case Series Study. Vasc. Endovasc. Surg. 2022, 56, 144–150. [Google Scholar] [CrossRef]
- Oba, S.; Hosoya, T.; Amamiya, M.; Mitsumura, T.; Kawata, D.; Sasaki, H.; Kamiya, M.; Yamamoto, A.; Ando, T.; Shimada, S.; et al. Arterial and Venous Thrombosis Complicated in COVID-19: A Retrospective Single Center Analysis in Japan. Front. Cardiovasc. Med. 2021, 8, 767074. [Google Scholar] [CrossRef]
- Perepu, U.S.; Chambers, I.; Wahab, A.; Ten Eyck, P.; Wu, C.; Dayal, S.; Sutamtewagul, G.; Bailey, S.R.; Rosenstein, L.J.; Lentz, S.R. Standard Prophylactic versus Intermediate Dose Enoxaparin in Adults with Severe COVID-19: A Multi-center, Open-label, Randomized Controlled Trial. J. Thromb. Haemost. 2021, 19, 2225–2234. [Google Scholar] [CrossRef]
- Piazza, G.; Campia, U.; Hurwitz, S.; Snyder, J.E.; Rizzo, S.M.; Pfeferman, M.B.; Morrison, R.B.; Leiva, O.; Fanikos, J.; Nauffal, V.; et al. Registry of Arterial and Venous Thromboembolic Complications in Patients With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2060–2072. [Google Scholar] [CrossRef] [PubMed]
- Bilaloglu, S.; Aphinyanaphongs, Y.; Jones, S.; Iturrate, E.; Hochman, J.; Berger, J.S. Thrombosis in Hospitalized Patients With COVID-19 in a New York City Health System. JAMA 2020, 324, 799–801. [Google Scholar] [CrossRef] [PubMed]
- Chi, G.; Lee, J.J.; Jamil, A.; Gunnam, V.; Najafi, H.; Memar Montazerin, S.; Shojaei, F.; Marszalek, J. Venous Thromboembolism among Hospitalized Patients with COVID-19 Undergoing Thromboprophylaxis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2489. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, L.; Yang, H.; Duan, G.; Wang, Y. Pooled Prevalence of Deep Vein Thrombosis among Coronavirus Disease 2019 Patients. Crit. Care 2020, 24, 466. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of Thrombotic Complications in Critically Ill ICU Patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Whyte, M.B.; Kelly, P.A.; Gonzalez, E.; Arya, R.; Roberts, L.N. Pulmonary Embolism in Hospitalised Patients with COVID-19. Thromb. Res. 2020, 195, 95–99. [Google Scholar] [CrossRef]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.-D.; Sacco, C.; Bertuzzi, A.; et al. Venous and Arterial Thromboembolic Complications in COVID-19 Patients Admitted to an Academic Hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Trimaille, A.; Curtiaud, A.; Marchandot, B.; Matsushita, K.; Sato, C.; Leonard-Lorant, I.; Sattler, L.; Grunebaum, L.; Ohana, M.; Von Hunolstein, J.-J.; et al. Venous Thromboembolism in Non-Critically Ill Patients with COVID-19 Infection. Thromb. Res. 2020, 193, 166–169. [Google Scholar] [CrossRef]
- Leonard-Lorant, I.; Delabranche, X.; Severac, F.; Helms, J.; Pauzet, C.; Collange, O.; Schneider, F.; Labani, A.; Bilbault, P.; Moliere, S.; et al. Acute Pulmonary Embolism in COVID-19 Patients on CT Angiography and Relationship to D-Dimer Levels. Radiology 2020, 296, E189–E191. [Google Scholar] [CrossRef]
- Wichmann, D.; Sperhake, J.-P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef]
- Marone, E.M.; Bonalumi, G.; Curci, R.; Arzini, A.; Chierico, S.; Marazzi, G.; Diaco, D.A.; Rossini, R.; Boschini, S.; Rinaldi, L.F. Characteristics of Venous Thromboembolism in COVID-19 Patients: A Multicenter Experience from Northern Italy. Ann. Vasc. Surg. 2020, 68, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Ilonzo, N.; Rao, A.; Safir, S.; Vouyouka, A.; Phair, J.; Baldwin, M.; Ting, W.; Soundararajan, K.; Han, D.; Tadros, R.; et al. Acute Thrombotic Manifestations of Coronavirus Disease 2019 Infection: Experience at a Large New York City Health Care System. J. Vasc. Surg. 2021, 73, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Bellosta, R.; Luzzani, L.; Natalini, G.; Pegorer, M.A.; Attisani, L.; Cossu, L.G.; Ferrandina, C.; Fossati, A.; Conti, E.; Bush, R.L.; et al. Acute Limb Ischemia in Patients with COVID-19 Pneumonia. J. Vasc. Surg. 2020, 72, 1864–1872. [Google Scholar] [CrossRef]
- Perini, P.; Nabulsi, B.; Massoni, C.B.; Azzarone, M.; Freyrie, A. Acute Limb Ischaemia in Two Young, Non-Atherosclerotic Patients with COVID-19. Lancet 2020, 395, 1546. [Google Scholar] [CrossRef]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-Vessel Stroke as a Presenting Feature of Covid-19 in the Young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef]
- Morassi, M.; Bagatto, D.; Cobelli, M.; D’Agostini, S.; Gigli, G.L.; Bnà, C.; Vogrig, A. Stroke in Patients with SARS-CoV-2 Infection: Case Series. J. Neurol. 2020, 267, 2185–2192. [Google Scholar] [CrossRef]
- Nadkarni, G.N.; Lala, A.; Bagiella, E.; Chang, H.L.; Moreno, P.R.; Pujadas, E.; Arvind, V.; Bose, S.; Charney, A.W.; Chen, M.D.; et al. Anticoagulation, Bleeding, Mortality, and Pathology in Hospitalized Patients With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 1815–1826. [Google Scholar] [CrossRef]
- Veyre, F.; Poulain-Veyre, C.; Esparcieux, A.; Monsarrat, N.; Aouifi, A.; Lapeze, J.; Chatelard, P. Femoral Arterial Thrombosis in a Young Adult after Nonsevere COVID-19. Ann. Vasc. Surg. 2020, 69, 85–88. [Google Scholar] [CrossRef]
- Cheung, S.; Quiwa, J.C.; Pillai, A.; Onwu, C.; Tharayil, Z.J.; Gupta, R. Superior Mesenteric Artery Thrombosis and Acute Intestinal Ischemia as a Consequence of COVID-19 Infection. Am. J. Case Rep. 2020, 21, e925753. [Google Scholar] [CrossRef]
- Shah, A.; Donovan, K.; McHugh, A.; Pandey, M.; Aaron, L.; Bradbury, C.A.; Stanworth, S.J.; Alikhan, R.; Von Kier, S.; Maher, K.; et al. Thrombotic and Haemorrhagic Complications in Critically Ill Patients with COVID-19: A Multicentre Observational Study. Crit. Care 2020, 24, 561. [Google Scholar] [CrossRef] [PubMed]
- Langer, F.; Kluge, S.; Klamroth, R.; Oldenburg, J. Coagulopathy in COVID-19 and Its Implication for Safe and Efficacious Thromboprophylaxis. Hamostaseologie 2020, 40, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation Parameters Are Associated with Poor Prognosis in Patients with Novel Coronavirus Pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Sanchis-Gomar, F.; Favaloro, E.J.; Lavie, C.J.; Henry, B.M. Coronavirus Disease 2019–Associated Coagulopathy. Mayo Clin. Proc. 2021, 96, 203–217. [Google Scholar] [CrossRef] [PubMed]
- Abate, V.; Casoria, A.; Rendina, D.; Muscariello, R.; Nuzzo, V.; Vargas, M.; Servillo, G.; Venetucci, P.; Conca, P.; Tufano, A.; et al. Spontaneous Muscle Hematoma in Patients with COVID-19: A Systematic Literature Review with Description of an Additional Case Series. Semin. Thromb. Hemost. 2021, 48, 100–108. [Google Scholar] [CrossRef]
- Trindade, A.J.; Izard, S.; Coppa, K.; Hirsch, J.S.; Lee, C.; Satapathy, S.K. Northwell COVID-19 Research Consortium Gastrointestinal Bleeding in Hospitalized COVID-19 Patients: A Propensity Score Matched Cohort Study. J. Intern. Med. 2021, 289, 887–894. [Google Scholar] [CrossRef]
- Zellmer, S.; Hanses, F.; Muzalyova, A.; Classen, J.; Braun, G.; Piepel, C.; Erber, J.; Pilgram, L.; Walter, L.; Göpel, S.; et al. Gastrointestinal Bleeding and Endoscopic Findings in Critically and Non-Critically Ill Patients with Corona Virus Disease 2019 (COVID-19): Results from Lean European Open Survey on SARS-CoV-2 (LEOSS) and COKA Registries. United Eur. Gastroenterol. J. 2021, 9, 1081–1090. [Google Scholar] [CrossRef]
- Valeriani, E.; Porfidia, A.; Ageno, W.; Spoto, S.; Pola, R.; Di Nisio, M. High-Dose versus Low-Dose Venous Thromboprophylaxis in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Intern. Emerg. Med. 2022, in press. [Google Scholar] [CrossRef]
- Helmy, M.A.; Milad, L.M.; Hasanin, A.; Elsayed, E.A.; Kamel, O.Y.; Mostafa, M.; Fathy, S.; Elsayad, M. Bleeding and Thrombotic Complications in Patients with Severe COVID-19: A Prospective Observational Study. Health Sci. Rep. 2022, 5, e736. [Google Scholar] [CrossRef]
- Al Raizah, A.; Al Askar, A.; Shaheen, N.; Aldosari, K.; Alnahdi, M.; Luhanga, M.; Alshuaibi, T.; Bajhmoum, W.; Alharbi, K.; Alsahari, G.; et al. High Rate of Bleeding and Arterial Thrombosis in COVID-19: Saudi Multicenter Study. Thromb. J. 2021, 19, 13. [Google Scholar] [CrossRef]
- Halaby, R.; Cuker, A.; Yui, J.; Matthews, A.; Ishaaya, E.; Traxler, E.; Domenico, C.; Cooper, T.; Tierney, A.; Niami, P.; et al. Bleeding Risk by Intensity of Anticoagulation in Critically Ill Patients with COVID-19: A Retrospective Cohort Study. J. Thromb. Haemost. 2021, 19, 1533–1545. [Google Scholar] [CrossRef] [PubMed]
- Godier, A.; Clausse, D.; Meslin, S.; Bazine, M.; Lang, E.; Huche, F.; Cholley, B.; Hamada, S.R. Major Bleeding Complications in Critically Ill Patients with COVID-19 Pneumonia. J. Thromb. Thrombolysis 2021, 52, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Fraissé, M.; Logre, E.; Pajot, O.; Mentec, H.; Plantefève, G.; Contou, D. Thrombotic and Hemorrhagic Events in Critically Ill COVID-19 Patients: A French Monocenter Retrospective Study. Crit. Care 2020, 24, 275. [Google Scholar] [CrossRef]
- Mattioli, M.; Benfaremo, D.; Fustini, E.; Gennarini, S. Atypical Spontaneous Hematomas in a Patient with Severe Coronavirus Disease 2019 (COVID-19). Semin. Thromb. Hemost. 2020, 46, 856–858. [Google Scholar] [CrossRef]
- Vos, C.G.; Gravendeel, J.; Keller, B.P.J.A. Three Cases of Spontaneous Major Bleeding in Patients with a COVID-19 Infection. Acta Chir. Belg. 2021, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Tudoran, C.; Tudoran, M.; Abu-Awwad, A.; Cut, T.G.; Voiță-Mekereș, F. Spontaneous Hematomas and Deep Vein Thrombosis during the Recovery from a SARS-CoV-2 Infection: Case Report and Literature Review. Medicina 2022, 58, 230. [Google Scholar] [CrossRef]
- Alvarenga Fernandes, D.; Satomi Yumioka, A.; Ranes de Menezes Filho, H. COVID-19 and Venous Thromboembolism: Part of a Multisystem Disease. Rev. Esp. Enferm. Dig. 2021, 113, 5. [Google Scholar] [CrossRef]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus Infections and Immune Responses. J. Med. Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef]
- Cryer, M.J.; Farhan, S.; Kaufmann, C.C.; Jäger, B.; Garg, A.; Krishnan, P.; Mehran, R.; Huber, K. Prothrombotic Milieu, Thrombotic Events and Prophylactic Anticoagulation in Hospitalized COVID-19 Positive Patients: A Review. Clin. Appl. Thromb. Hemost. 2022, 28, 1–14. [Google Scholar] [CrossRef]
- Lopes, R.D.; de Barros e Silva, P.G.M.; Furtado, R.H.M.; Macedo, A.V.S.; Ramacciotti, E.; Damini, L.P.; Bronhara, B.; Cavalcanti, A.B.; Rosa, R.G.; Azevedo, L.C.P.; et al. Randomized Clinical Trial to Evaluate a Routine Full Anticoagulation Strategy in Patients with Coronavirus Infection (SARS-CoV2) Admitted to Hospital: Rationale and Design of the ACTION (AntiCoagulaTlon COroNavirus)–Coalition IV Trial. Am. Heart J. 2021, 238, 1–11. [Google Scholar] [CrossRef]
- Overton, P.M.; Toshner, M.; Mulligan, C.; Vora, P.; Nikkho, S.; de Backer, J.; Lavon, B.R.; Klok, F.A. PVRI Innovative Drug Development Initiative Pulmonary Thromboembolic Events in COVID-19—A Systematic Literature Review. Pulm. Circ. 2022. accepted. [Google Scholar] [CrossRef] [PubMed]
- Muthiah, A.; Ohnigian, S.; Reagan, J.L.; Hsu, A. Thrombosis in COVID 2022: An Updated Narrative Review of Current Literature and Inpatient Management. R. I. Med. J. 2022, 105, 36–40. [Google Scholar]
- Dimakakos, E.; Gomatou, G.; Catalano, M.; Olinic, D.-M.; Spyropoulos, A.C.; Falanga, A.; Maraveyas, A.; Liew, A.; Schulman, S.; Belch, J.; et al. Thromboembolic Disease in Patients With Cancer and COVID-19: Risk Factors, Prevention and Practical Thromboprophylaxis Recommendations–State-of-the-Art. Anticancer Res. 2022, 42, 3261–3274. [Google Scholar] [CrossRef] [PubMed]
- Mani, A.; Ojha, V. Thromboembolism after COVID-19 Vaccination: A Systematic Review of Such Events in 286 Patients. Ann. Vasc. Surg. 2022, in press. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tudoran, C.; Velimirovici, D.E.; Berceanu-Vaduva, D.M.; Rada, M.; Voiţă-Mekeres, F.; Tudoran, M. Increased Susceptibility for Thromboembolic Events versus High Bleeding Risk Associated with COVID-19. Microorganisms 2022, 10, 1738. https://doi.org/10.3390/microorganisms10091738
Tudoran C, Velimirovici DE, Berceanu-Vaduva DM, Rada M, Voiţă-Mekeres F, Tudoran M. Increased Susceptibility for Thromboembolic Events versus High Bleeding Risk Associated with COVID-19. Microorganisms. 2022; 10(9):1738. https://doi.org/10.3390/microorganisms10091738
Chicago/Turabian StyleTudoran, Cristina, Dana Emilia Velimirovici, Delia Mira Berceanu-Vaduva, Maria Rada, Florica Voiţă-Mekeres, and Mariana Tudoran. 2022. "Increased Susceptibility for Thromboembolic Events versus High Bleeding Risk Associated with COVID-19" Microorganisms 10, no. 9: 1738. https://doi.org/10.3390/microorganisms10091738