
Pathogen- and Type-Specific Changes in Invasive Bacterial Disease Epidemiology during the First Year of the COVID-19 Pandemic in The Netherlands


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Patient Information
2.2. Typing of Bacterial Isolates
2.3. Study Period and Patient Categories
2.4. Descriptive Analyses
3. Results
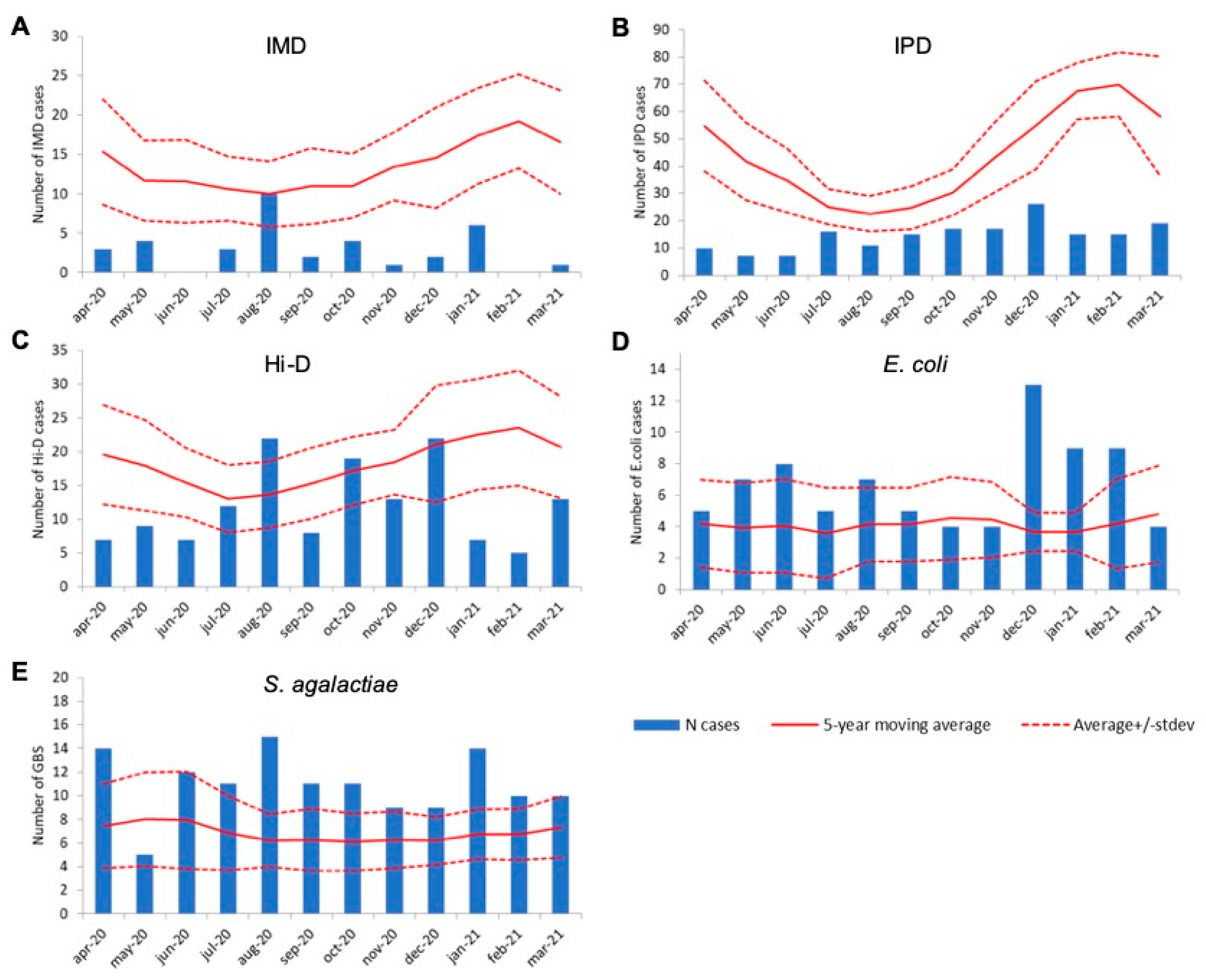
3.1. Decrease in Invasive Disease Cases Caused by Respiratory-Transmitted Pathogens in the First COVID-19 Year
3.2. Age-Specific Effects on Epidemiology of Invasive Disease
3.3. Serogroup-Specific Changes in Invasive Meningococcal Disease Cases
3.4. Serotype-Specific Changes in Invasive Pneumococcal Disease Cases
3.5. Serotype-Specific Changes in H. influenzae Invasive Disease
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koelman, D.L.H.; van Kassel, M.N.; Bijlsma, M.W.; Brouwer, M.C.; van de Beek, D.; van der Ende, A. Changing Epidemiology of Bacterial Meningitis Since Introduction of Conjugate Vaccines: 3 Decades of National Meningitis Surveillance in The Netherlands. Clin. Infect. Dis. 2021, 73, e1099–e1107. [Google Scholar] [CrossRef] [PubMed]
- Vestjens, S.M.; Sanders, E.A.; Vlaminckx, B.J.; de Melker, H.E.; van der Ende, A.; Knol, M.J. Twelve years of pneumococcal conjugate vaccination in the Netherlands: Impact on incidence and clinical outcomes of invasive pneumococcal disease. Vaccine 2019, 37, 6558–6565. [Google Scholar] [CrossRef] [PubMed]
- van Alphen, L.; Spanjaard, L.; van der Ende, A.; Schuurman, I.; Dankert, J. Effect of nationwide vaccination of 3-month-old infants in The Netherlands with conjugate Haemophilus influenzae type b vaccine: High efficacy and lack of herd immunity. J. Pediatr. 1997, 131, 869–873. [Google Scholar] [CrossRef] [Green Version]
- Bijlsma, M.W.; Bekker, V.; Brouwer, M.C.; Spanjaard, L.; van de Beek, D.; van der Ende, A. Epidemiology of invasive meningococcal disease in the Netherlands, 1960–2012: An analysis of national surveillance data. Lancet Infect. Dis. 2014, 14, 805–812. [Google Scholar] [CrossRef]
- Friesema, I.H.M.; Schotsborg, M.; Heck, M.E.O.C.; van Pelt, W. Risk factors for sporadic Shiga toxin-producing Escherichia coli O157 and non-O157 illness in The Netherlands, 2008–2012, using periodically surveyed controls. Epidemiol. Infect. 2014, 143, 1360–1367. [Google Scholar] [CrossRef] [Green Version]
- Cozorici, D.; Măciucă, R.-A.; Stancu, C.; Tihăuan, B.-M.; Uță, R.B.; Codrea, C.I.; Matache, R.; Pop, C.-E.; Wolff, R.; Fendrihan, S. Microbial Contamination and Survival Rate on Different Types of Banknotes. Int. J. Environ. Res. Public Health 2022, 19, 4310. [Google Scholar] [CrossRef]
- Berardi, A.; Spada, C.; Creti, R.; Auriti, C.; Gambini, L.; Rizzo, V.; Capretti, M.; Laforgia, N.; Papa, I.; Tarocco, A.; et al. Maternal Carriage in Late-Onset Group B Streptococcus Disease, Italy. Emerg. Infect. Dis. 2021, 27, 2279–2287. [Google Scholar] [CrossRef]
- Karampatsas, K.; Davies, H.; Mynarek, M.; Andrews, N.; Heath, P.T.; Le Doare, K. Clinical Risk Factors Associated with Late-Onset Invasive Group B Streptococcal Disease: Systematic Review and Meta-analyses. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Knol, M.J.; Ruijs, W.L.; Antonise-Kamp, L.; De Melker, H.E.; Van Der Ende, A. Implementation of MenACWY vaccination because of ongoing increase in serogroup W invasive meningococcal disease, the Netherlands, 2018. Eurosurveillance 2018, 23, 18-00158. [Google Scholar] [CrossRef]
- Ohm, M.; Hahné, S.J.M.; van der Ende, A.; Sanders, E.A.M.; Berbers, G.A.M.; Ruijs, W.L.M.; van Sorge, N.M.; de Melker, H.E.; Knol, M.J. Vaccine Impact and Effectiveness of Meningococcal Serogroup ACWY Conjugate Vaccine Implementation in the Netherlands: A Nationwide Surveillance Study. Clin. Infect. Dis. 2021, ciab791. [Google Scholar] [CrossRef]
- Peckeu, L.; van der Ende, A.; de Melker, H.; Sanders, E.; Knol, M. Impact and effectiveness of the 10-valent pneumococcal conjugate vaccine on invasive pneumococcal disease among children under 5 years of age in the Netherlands. Vaccine 2021, 39, 431–437. [Google Scholar] [CrossRef]
- Schurink-van’t Klooster, T.M.; de Melker, H.E. The National Immunisation Programme in the Netherlands: Surveillance and Developments in 2019–2020; Rijksinstituut voor Volksgezondheid en Milieu RIVM: Utrecht, The Netherlands, 2020. [Google Scholar]
- Bijlsma, M.W.; Brouwer, M.C.; Spanjaard, L.; van de Beek, D.; Van Der Ende, A. A Decade of Herd Protection after Introduction of Meningococcal Serogroup C Conjugate Vaccination. Clin. Infect. Dis. 2014, 59, 1216–1221. [Google Scholar] [CrossRef] [Green Version]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Brueggemann, A.B.; Jansen van Rensburg, M.J.; Shaw, D.; McCarthy, N.D.; Jolley, K.A.; Maiden, M.C.J.; van der Linden, M.P.G.; Amin-Chowdhury, Z.; Bennett, D.E.; Borrow, R.; et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: A prospective analysis of surveillance data. Lancet Digit. Health 2021, 3, e360–e370. [Google Scholar] [CrossRef]
- Middeldorp, M.; van Lier, A.; van der Maas, N.; Veldhuijzen, I.; Freudenburg, W.; van Sorge, N.M.; Sanders, E.A.; Knol, M.J.; de Melker, H.E. Short term impact of the COVID-19 pandemic on incidence of vaccine preventable diseases and participation in routine infant vaccinations in the Netherlands in the period March-September 2020. Vaccine 2021, 39, 1039–1043. [Google Scholar] [CrossRef]
- Subbarao, S.; Campbell, H.; Ribeiro, S.; Clark, S.A.; Lucidarme, J.; Ramsay, M.; Borrow, R.; Ladhani, S. Invasive Meningococcal Disease, 2011–2020, and Impact of the COVID-19 Pandemic, England. Emerg. Infect. Dis. 2021, 27, 2495–2497. [Google Scholar] [CrossRef]
- Ouchterlony, O. Antigen—Antibody Reactions in Gels. Acta Pathol. Microbiol. Scand. 1949, 26, 507–515. [Google Scholar] [CrossRef]
- Knol, M.J.; Hahné, S.J.M.; Lucidarme, J.; Campbell, H.; de Melker, H.E.; Gray, S.J.; Borrow, R.; Ladhani, S.N.; Ramsay, M.E.; van der Ende, A. Temporal associations between national outbreaks of meningococcal serogroup W and C disease in the Netherlands and England: An observational cohort study. Lancet Public Health 2017, 2, e473–e482. [Google Scholar] [CrossRef] [Green Version]
- Wagenvoort, G.H.; Sanders, E.A.; Vlaminckx, B.J.; Elberse, K.E.; de Melker, H.E.; van der Ende, A.; Knol, M.J. Invasive pneumococcal disease: Clinical outcomes and patient characteristics 2–6 years after introduction of 7-valent pneumococcal conjugate vaccine compared to the pre-vaccine period, the Netherlands. Vaccine 2016, 34, 1077–1085. [Google Scholar] [CrossRef]
- Joensen, K.G.; Tetzschner, A.M.; Iguchi, A.; Aarestrup, F.M.; Scheutz, F. Rapid and Easy In Silico Serotyping of Escherichia coli Isolates by Use of Whole-Genome Sequencing Data. J. Clin. Microbiol. 2015, 53, 2410–2426. [Google Scholar] [CrossRef] [Green Version]
- Trijbels-Smeulders, M.A.J.M.; Kimpen, J.L.L.; Kollée, L.A.A.; Bakkers, J.; Melchers, W.; Spanjaard, L.; Wannet, W.J.B.; Hoogkamp-Korstanje, M.A.A. Serotypes, genotypes, and antibiotic susceptibility profiles of group b streptococci causing neonatal sepsis and meningitis before and after introduction of antibiotic prophylaxis. Pediatr. Infect. Dis. J. 2006, 25, 945–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steens, A.; Stanoeva, K.R.; Knol, M.J.; Mariman, R.; de Melker, H.E.; van Sorge, N.M. Increase in invasive disease caused by Haemophilus influenzae b, the Netherlands, 2020 to 2021. Eurosurveillance 2021, 26, 2100956. [Google Scholar] [CrossRef] [PubMed]
- Bekker, V.; Bijlsma, M.W.; van de Beek, D.; Kuijpers, T.W.; van der Ende, A. Incidence of invasive group B streptococcal disease and pathogen genotype distribution in newborn babies in the Netherlands over 25 years: A nationwide surveillance study. Lancet Infect. Dis. 2014, 14, 1083–1089. [Google Scholar] [CrossRef]
- Jamrozy, D.; Bijlsma, M.W.; de Goffau, M.C.; van de Beek, D.; Kuijpers, T.W.; Parkhill, J.; van der Ende, A.; Bentley, S.D. Increasing incidence of group B streptococcus neonatal infections in the Netherlands is associated with clonal expansion of CC17 and CC23. Sci. Rep. 2020, 10, 9539. [Google Scholar] [CrossRef] [PubMed]
- Dirkx, K.K.; Mulder, B.; Post, A.S.; Rutten, M.H.; Swanink, C.M.; Wertheim, H.F.; Cremers, A.J. The drop in reported invasive pneumococcal disease among adults during the first COVID-19 wave in the Netherlands explained. Int. J. Infect. Dis. 2021, 111, 196–203. [Google Scholar] [CrossRef]
- Janapatla, R.P.; Chen, C.-L.; Dudek, A.; Li, H.-C.; Yang, H.-P.; Su, L.-H.; Chiu, C.-H. Serotype transmission dynamics and reduced incidence of invasive pneumococcal disease caused by different serotypes after implementation of non-pharmaceutical interventions during COVID-19 pandemic. Eur. Respir. J. 2021, 58, 2100978. [Google Scholar] [CrossRef]
- Amin-Chowdhury, Z.; Collins, S.; Sheppard, C.; Litt, D.; Fry, N.K.; Andrews, N.; Ladhani, S.N. Characteristics of Invasive Pneumococcal Disease Caused by Emerging Serotypes After the Introduction of the 13-Valent Pneumococcal Conjugate Vaccine in England: A Prospective Observational Cohort Study, 2014–2018. Clin. Infect. Dis. 2020, 71, e235–e243. [Google Scholar] [CrossRef]
- Balsells, E.; Dagan, R.; Yildirim, I.; Gounder, P.P.; Steens, A.; Muñoz-Almagro, C.; Mameli, C.; Kandasamy, R.; Lavi, N.G.; Daprai, L.; et al. The relative invasive disease potential of Streptococcus pneumoniae among children after PCV introduction: A systematic review and meta-analysis. J. Infect. 2018, 77, 368–378. [Google Scholar] [CrossRef] [Green Version]
- Ladhani, S.N.; Collins, S.; Djennad, A.; Sheppard, C.L.; Borrow, R.; Fry, N.K.; Andrews, N.J.; Miller, E.; Ramsay, M.E. Rapid increase in non-vaccine serotypes causing invasive pneumococcal disease in England and Wales, 2000–2017: A prospective national observational cohort study. Lancet Infect. Dis. 2018, 18, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Hanquet, G.; Krizova, P.; Dalby, T.; Ladhani, S.N.; Nuorti, J.P.; Danis, K.; Mereckiene, J.; Knol, M.J.; Winje, B.A.; Ciruela, P.; et al. Serotype Replacement after Introduction of 10-Valent and 13-Valent Pneumococcal Conjugate Vaccines in 10 Countries, Europe. Emerg. Infect. Dis. 2022, 28, 137–138. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Hanage, W.P. Making sense of differences in pneumococcal serotype replacement. Lancet Infect. Dis. 2019, 19, e213–e220. [Google Scholar] [CrossRef]
- Garcia Quesada, M.; Yang, Y.; Bennett, J.C.; Hayford, K.; Zeger, S.L.; Feikin, D.R.; Peterson, M.E.; Cohen, A.L.; Almeida, S.C.; Ampofo, K.; et al. Serotype Distribution of Remaining Pneumococcal Meningitis in the Mature PCV10/13 Period: Findings from the PSERENADE Project. Microorganisms 2021, 9, 738. [Google Scholar] [CrossRef]
- Isturiz, R.; Sings, H.L.; Hilton, B.; Arguedas, A.; Reinert, R.-R.; Jodar, L. Streptococcus pneumoniae serotype 19A: Worldwide epidemiology. Expert Rev. Vaccines 2017, 16, 1007–1027. [Google Scholar] [CrossRef]
- Casanova, C.; Küffer, M.; Leib, S.L.; Hilty, M. Re-emergence of invasive pneumococcal disease (IPD) and increase of serotype 23B after easing of COVID-19 measures, Switzerland, 2021. Emerg. Microbes Infect. 2021, 10, 2202–2204. [Google Scholar] [CrossRef]
- Perniciaro, S.R.; van der Linden, M.P.; Weinberger, D.M. Re-emergence of Invasive Pneumococcal Disease in Germany during the Spring and Summer of 2021. MedRxiv 2021. [Google Scholar] [CrossRef]
- Danino, D.; Ben-Shimol, S.; van der Beek, B.A.; Givon-Lavi, N.; Avni, Y.S.; Greenberg, D.; Weinberger, D.M.; Dagan, R. Decline in Pneumococcal Disease in Young Children During the Coronavirus Disease 2019 (COVID-19) Pandemic in Israel Associated with Suppression of Seasonal Respiratory Viruses, Despite Persistent Pneumococcal Carriage: A Prospective Cohort Study. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Cohen, R.; Ashman, M.; Taha, M.-K.; Varon, E.; Angoulvant, F.; Levy, C.; Ryback, A.; Ouldali, N.; Guiso, N.; Grimprel, E. Pediatric Infectious Disease Group (GPIP) position paper on the immune debt of the COVID-19 pandemic in childhood, how can we fill the immunity gap? Infect. Dis. Now 2021, 51, 418–423. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Serotype | Covered by Vaccine * | Average Annual Number (Range) of Cases, April 2015–March 2020 | Number of Cases in First COVID-19 Year (Range), April 2020–March 2021 | Decrease in COVID-19 versus Non-COVID-19 Year (%) |
|---|---|---|---|---|
| All serotypes | 531 (503–576) | 175 | 67% | |
| 8 | PPV23 | 126 (118–129) | 30 | 76% |
| 19A | PCV13 | 76 (73–83) | 38 | 50% |
| 3 | PCV13 | 46 (38–59) | 18 | 61% |
| 22F | PPV23 | 35 (27–39) | 11 | 68% |
| 9N | PPV23 | 28 (21–34) | 9 | 68% |
| 12F | PPV23 | 23 (19–27) | 4 | 82% |
| 7F | PCV10 | 21 (4–43) | 0 | 100% |
| 6C | NVT | 18 (16–22) | 15 | 16% |
| 33F | PPV23 | 16 (11–20) | 2 | 87% |
| 15A | NVT | 14 (12–15) | 2 | 86% |
| 23B | NVT | 13 (10–16) | 5 | 60% |
| 23A | NVT | 11 (6–15) | 4 | 64% |
| 1 | PCV10 | 11 (0–30) | 0 | 100% |
| 10A | PPV23 | 11 (8–14) | 4 | 62% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steens, A.; Knol, M.J.; Freudenburg-de Graaf, W.; de Melker, H.E.; van der Ende, A.; van Sorge, N.M. Pathogen- and Type-Specific Changes in Invasive Bacterial Disease Epidemiology during the First Year of the COVID-19 Pandemic in The Netherlands. Microorganisms 2022, 10, 972. https://doi.org/10.3390/microorganisms10050972
Steens A, Knol MJ, Freudenburg-de Graaf W, de Melker HE, van der Ende A, van Sorge NM. Pathogen- and Type-Specific Changes in Invasive Bacterial Disease Epidemiology during the First Year of the COVID-19 Pandemic in The Netherlands. Microorganisms. 2022; 10(5):972. https://doi.org/10.3390/microorganisms10050972
Chicago/Turabian StyleSteens, Anneke, Mirjam J. Knol, Wieke Freudenburg-de Graaf, Hester E. de Melker, Arie van der Ende, and Nina M. van Sorge. 2022. "Pathogen- and Type-Specific Changes in Invasive Bacterial Disease Epidemiology during the First Year of the COVID-19 Pandemic in The Netherlands" Microorganisms 10, no. 5: 972. https://doi.org/10.3390/microorganisms10050972