
Bacterial Coinfection and Antibiotic Resistance Profiles among Hospitalised COVID-19 Patients

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Cohort
2.3. Collection of Specimens for Bacterial Investigation
2.4. Antibiotic Sensitivity Testing
2.5. Statistical Analysis
2.6. Ethics Statement
3. Results
3.1. Demographic Characteristics of the Study Cohort
3.2. Prevalence of Bacterial Coinfection in ICU and Non-ICU COVID-19 Patients
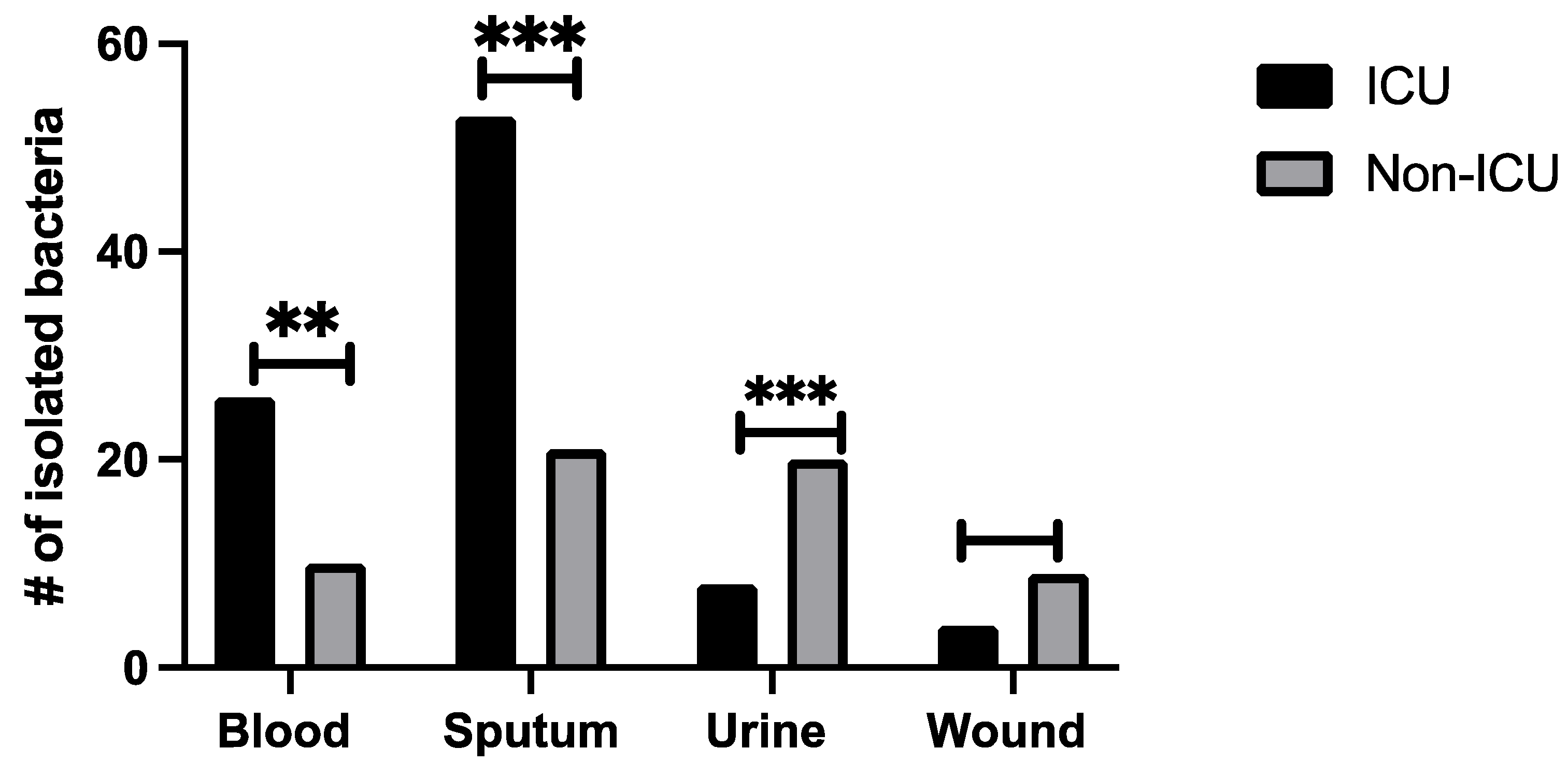
3.3. Identified Bacteria from Tested Specimens among ICU and Non-ICU COVID-19 Patients
3.4. Resistance Profiles of Detected Bacterial Isolates from ICU and Non-ICU Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MOH. COVID-19 Dashboard. Available online: https://covid19.moh.gov.sa/ (accessed on 27 March 2021).
- Bazaid, A.S.; Aldarhami, A.; Binsaleh, N.K.; Sherwani, S.; Althomali, O.W. Knowledge and Practice of Personal Protective Measures during the COVID-19 Pandemic: A Cross-Sectional Study in Saudi Arabia. PLoS ONE 2020, 15, e0243695. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, M.C. Aerosol Transmission of SARS-CoV-2: Physical Principles and Implications. Front. Public Health 2020, 8, 590041. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, H.; McFarland, W.; Karamouzian, M.; Sharifi, H. COVID-19 among People Living with HIV: A Systematic Review. AIDS Behav. 2020, 25, 1–8. [Google Scholar] [CrossRef]
- Phua, J.; Weng, L.; Ling, L.; Egi, M.; Lim, C.-M.; Divatia, J.V.; Shrestha, B.R.; Arabi, Y.M.; Ng, J.; Gomersall, C.D.; et al. Intensive Care Management of Coronavirus Disease 2019 (COVID-19): Challenges and Recommendations. Lancet Respir. Med. 2020, 8, 506–517. [Google Scholar] [CrossRef]
- Dalton, K.R.; Rock, C.; Carroll, K.C.; Davis, M.F. One Health in Hospitals: How Understanding the Dynamics of People, Animals, and the Hospital Built-Environment Can Be Used to Better Inform Interventions for Antimicrobial-Resistant Gram-Positive Infections. Antimicrob. Resist. Infect. Control 2020, 9, 1–17. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, K.-H.; Chen, W.; Yu, Y.; Feng, S.-F. Epidemiology and Risk Factors for Nosocomial Infection in the Respiratory Intensive Care Unit of a Teaching Hospital in China: A Prospective Surveillance during 2013 and 2015. BMC Infect. Dis. 2019, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Díaz, J.M.L.; Mendoza-Olazarán, S.; Camacho-Ortiz, A.; Flores-Treviño, S.; Garza-González, E. One-Year Surveillance of ESKAPE Pathogens in an Intensive Care Unit of Monterrey, Mexico. Chemotherapy 2012, 58, 475–481. [Google Scholar] [CrossRef]
- Elabbadi, A.; Turpin, M.; Gerotziafas, G.T.; Teulier, M.; Voiriot, G.; Fartoukh, M. Bacterial Coinfection in Critically Ill COVID-19 Patients with Severe Pneumonia. Infection 2021, 49, 559–562. [Google Scholar] [CrossRef]
- Patel, A. Tackling Antimicrobial Resistance in the Shadow of COVID-19. Mbio 2021, 12, e0047321. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of Co-Infections and Superinfections in Hospitalized Patients with COVID-19: A Retrospective Cohort Study. Clin. Microbiol. Infect. 2020, 27, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and Outcomes of Co-Infection and Superinfection with SARS-CoV-2 and Other Pathogens: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef]
- Guleria, R.; Mohan, A.; Kulkarni, A.; Madan, K.; Hadda, V. Guidelines for Antibiotic Prescription in Intensive Care Unit. Indian J. Crit. Care Med. 2019, 23, 1–63. [Google Scholar] [CrossRef] [PubMed]
- Denny, S.; Rawson, T.M.; Hart, P.; Satta, G.; Abdulaal, A.; Hughes, S.; Gilchrist, M.; Mughal, N.; Moore, L.S.P. Bacteraemia Variation during the COVID-19 Pandemic; A Multi-Centre UK Secondary Care Ecological Analysis. BMC Infect. Dis. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Somily, A.; Babay, H.A.H.; Torchyan, A.A.; Sayyed, S.B.; Absar, M.; Al-Aqeel, R.; Binkhamis, A.K. Time-to-Detection of Bacteria and Yeast with the BACTEC FX Versus BacT/Alert Virtuo Blood Culture Systems. Ann. Saudi Med. 2018, 38, 194–199. [Google Scholar] [CrossRef]
- Ntirenganya, C.; Muvunyi, C.M.; Manzi, O.; Ogbuagu, O. High Prevalence of Antimicrobial Resistance among Common Bacterial Isolates in a Tertiary Healthcare Facility in Rwanda. Am. J. Trop. Med. Hyg. 2015, 92, 865–870. [Google Scholar] [CrossRef]
- Bazaid, A.S.; Saeed, A.; Alrashidi, A.; Alrashidi, A.; Alshaghdali, K.; Hammam, S.A.; Alreshidi, T.; Alshammary, M.; Alarfaj, A.; Thallab, R.; et al. Antimicrobial Surveillance for Bacterial Uropathogens in Ha’il, Saudi Arabia: A Five-Year Multicenter Retrospective Study. Infect. Drug Resist. 2021, 14, 1455–1465. [Google Scholar] [CrossRef]
- Carroll, K.C.; Borek, A.P.; Burger, C.; Glanz, B.; Bhally, H.; Henciak, S.; Flayhart, D.C. Evaluation of the BD Phoenix Automated Microbiology System for Identification and Antimicrobial Susceptibility Testing of Staphylococci and Enterococci. J. Clin. Microbiol. 2006, 44, 2072–2077. [Google Scholar] [CrossRef] [Green Version]
- Patel, J.B. Performance Standards for Antimicrobial Susceptibility Testing; Clinical and Laboratory Standards Institute: Wayne, MI, USA, 2017. [Google Scholar]
- Ferguson, J.K.; Joseph, J.; Kangapu, S.; Zoleveke, H.; Townell, N.; Duke, T.; Manning, L.; Lavu, E. Quality Microbiological Diagnostics and Antimicrobial Susceptibility Testing, an Essential Component of Antimicrobial Resistance Surveillance and Control Efforts in Pacific Island Nations. West. Pac. Surveill. Response J. 2020, 11, 41–46. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report. Available online: https://covid19.who.int/ (accessed on 8 June 2021).
- Zhu, X.; Ge, Y.; Wu, T.; Zhao, K.; Chen, Y.; Wu, B.; Zhu, F.; Zhu, B.; Cui, L. Co-Infection with Respiratory Pathogens among COVID-2019 Cases. Virus Res. 2020, 285, 198005. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Dana, R.; Bannay, A.; Bourst, P.; Ziegler, C.; Losser, M.-R.; Gibot, S.; Levy, B.; Audibert, G.; Ziegler, O. Obesity and Mortality in Critically Ill COVID-19 Patients with Respiratory Failure. Int. J. Obes. 2021, 45, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Shafran, N.; Shafran, I.; Ben-Zvi, H.; Sofer, S.; Sheena, L.; Krause, I.; Shlomai, A.; Goldberg, E.; Sklan, E.H. Secondary Bacterial Infection in COVID-19 Patients Is a Stronger Predictor for Death Compared to Influenza Patients. Sci. Rep. 2021, 11, 12703. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult in patients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Piroth, L.; Cottenet, J.; Mariet, A.-S.; Bonniaud, P.; Blot, M.; Tubert-Bitter, P.; Quantin, C. Comparison of the Characteristics, Morbidity, and Mortality of COVID-19 and Seasonal Influenza: A Nationwide, Population-Based Retrospective Cohort Study. Lancet Respir. Med. 2021, 9, 251–259. [Google Scholar] [CrossRef]
- Yang, S.; Hua, M.; Liu, X.; Du, C.; Pu, L.; Xiang, P.; Wang, L.; Liu, J. Bacterial and Fungal Co-Infections among COVID-19 Patients in Intensive Care Unit. Microbes Infect. 2021, 23, 104806. [Google Scholar] [CrossRef] [PubMed]
- Moretti, M.; Van Laethem, J.; Minini, A.; Pierard, D.; Malbrain, M.L. Ventilator-Associated Bacterial Pneumonia in Coronavirus 2019 Disease, a Retrospective Monocentric Cohort Study. J. Infect. Chemother. 2021, 27, 826–833. [Google Scholar] [CrossRef]
- D’Humières, C.; Patrier, J.; Lortat-Jacob, B.; Tran-Dinh, A.; Chemali, L.; Maataoui, N.; Rondinaud, E.; Ruppé, E.; Burdet, C.; Ruckly, S.; et al. Two Original Observations Concerning Bacterial Infections in COVID-19 Patients Hospitalized in Intensive Care Units during the First Wave of the Epidemic in France. PLoS ONE 2021, 16, e0250728. [Google Scholar] [CrossRef]
- Buetti, N.; Ruckly, S.; de Montmollin, E.; Reignier, J.; Terzi, N.; Cohen, Y.; Shiami, S.; Dupuis, C.; Timsit, J.-F. COVID-19 Increased the Risk of ICU-Acquired Bloodstream Infections: A Case–Cohort Study from the Multicentric OUTCOMEREA Network. Intensiv. Care Med. 2021, 47, 180–187. [Google Scholar] [CrossRef]
- Lai, C.-C.; Wang, C.-Y.; Hsueh, P.-R. Co-Infections among Patients with COVID-19: The Need for Combination Therapy with Non-Anti-SARS-CoV-2 Agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef]
- Silva, D.; Lima, C.; Magalhães, V.; Baltazar, L.; Peres, N.; Caligiorne, R.; Moura, A.; Fereguetti, T.; Martins, J.; Rabelo, L.; et al. Fungal and Bacterial Coinfections Increase Mortality of Severely Ill COVID-19 Patients. J. Hosp. Infect. 2021, 113, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Puzniak, L.; Finelli, L.; Yu, K.C.; Bauer, K.A.; Moise, P.; De Anda, C.; Vankeepuram, L.; Sepassi, A.; Gupta, V. A Multicenter Analysis of the Clinical Microbiology and Antimicrobial Usage in Hospitalized Patients in the US with or without COVID-19. BMC Infect. Dis. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Karataş, M.; Yaşar-Duman, M.; Tünger, A.; Çilli, F.; Aydemir, Ş.; Özenci, V. Secondary Bacterial Infections and Antimicrobial Resistance in COVID-19: Comparative Evaluation of Pre-Pandemic and Pandemic-Era, a Retrospective Single Center Study. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 1–8. [Google Scholar] [CrossRef]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; Doosti, Z.; Golzari, S.E. Evaluation of Bacterial Co-Infections of the Respiratory Tract in COVID-19 Patients Admitted to ICU. BMC Infect. Dis. 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Gavaruzzi, F.; Ceccarelli, G.; Borrazzo, C.; Oliva, A.; Alessandri, F.; Magnanimi, E.; Pugliese, F.; Venditti, M. Multidrug-Resistant Acinetobacter Baumannii Infections in COVID-19 Patients Hospitalized in Intensive Care Unit. Infection 2021, 50, 83–92. [Google Scholar] [CrossRef]
- Rangel, K.; Chagas, T.; De-Simone, S. Acinetobacter Baumannii Infections in Times of COVID-19 Pandemic. Pathogens 2021, 10, 1006. [Google Scholar] [CrossRef]
- Arteaga-Livias, K.; Pinzas-Acosta, K.; Perez-Abad, L.; Panduro-Correa, V.; Rabaan, A.A.; Pecho-Silva, S.; Dámaso-Mata, B. A Multidrug-Resistant Klebsiella Pneumoniae Outbreak in a Peruvian Hospital: Another Threat from the COVID-19 Pandemic. Infect. Control Hosp. Epidemiol. 2021, 43, 267–268. [Google Scholar] [CrossRef]
- Montrucchio, G.; Corcione, S.; Sales, G.; Curtoni, A.; De Rosa, F.; Brazzi, L. Carbapenem-Resistant Klebsiella Pneumoniae in ICU-Admitted COVID-19 Patients: Keep an Eye on the Ball. J. Glob. Antimicrob. Resist. 2020, 23, 398–400. [Google Scholar] [CrossRef]
- Copiz, M.M.M. The Gut Microbiota in Patients with COVID-19 and Obesity. FASEB J. 2021, 35. [Google Scholar] [CrossRef]
- García-Mena, J.; Corona-Cervantes, K.; Cuervo-Zanatta, D.; Benitez-Guerrero, T.; Vélez-Ixta, J.M.; Zavala-Torres, N.G.; Villalobos-Flores, L.E.; Hernández-Quiroz, F.; Perez-Cruz, C.; Murugesan, S.; et al. Gut Microbiota in a Population Highly Affected by Obesity and Type 2 Diabetes and Susceptibility to COVID-19. World J. Gastroenterol. 2021, 27, 7065–7079. [Google Scholar] [CrossRef]
- Sreenath, K.; Batra, P.; Vinayaraj, E.V.; Bhatia, R.; SaiKiran, K.; Singh, V.; Singh, S.; Verma, N.; Singh, U.B.; Mohan, A.; et al. Coinfections with Other Respiratory Pathogens among Patients with COVID-19. Microbiol. Spectr. 2021, 9, e0016321. [Google Scholar] [CrossRef] [PubMed]
- Palanisamy, N.; Vihari, N.; Meena, D.S.; Kumar, D.; Midha, N.; Tak, V.; Sharma, A.; Bohra, G.K.; Kothari, N.; Dutt, N.; et al. Clinical Profile of Bloodstream Infections in COVID-19 Patients: A Retrospective Cohort Study. BMC Infect. Dis. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, H. Bacterial Co-Infections and Antibiotic Resistance in Patients with COVID-19. GMS Hyg. Infect. Control 2020, 15, Doc35. [Google Scholar] [CrossRef] [PubMed]
- Saeed, N.K.; Al-Khawaja, S.; Alsalman, J.; Almusawi, S.; Albalooshi, N.A.; Al-Biltagi, M. Bacterial Co-Infection in Patients with SARS-CoV-2 in the Kingdom of Bahrain. World J. Virol. 2021, 10, 168–181. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, J.; Yang, Y.; Cai, P.; Cao, J.; Cai, X.; Zhang, Y. Etiology and Antimicrobial Resistance of Secondary Bacterial Infections in Patients Hospitalized with COVID-19 in Wuhan, China: A Retrospective Analysis. Antimicrob. Resist. Infect. Control 2020, 9, 1–7. [Google Scholar] [CrossRef]
- Silva, A.R.O.; Salgado, D.R.; Lopes, L.P.N.; Castanheira, D.; Emmerick, I.C.M.; Lima, E.C. Increased Use of Antibiotics in the Intensive Care Unit During Coronavirus Disease (COVID-19) Pandemic in a Brazilian Hospital. Front. Pharmacol. 2021, 12, 3615. [Google Scholar] [CrossRef]
- Said, K.B.; Alsolami, A.; Khalifa, A.M.; Khalil, N.A.; Moursi, S.; Osman, A.; Fahad, D.; Rakha, E.; Rashidi, M.; Moussa, S.; et al. A Multi-Point Surveillance for Antimicrobial Resistance Profiles among Clinical Isolates of Gram-Negative Bacteria Recovered from Major Ha’il Hospitals, Saudi Arabia. Microorganisms 2021, 9, 2024. [Google Scholar] [CrossRef]
- Polemis, M.; Mandilara, G.; Pappa, O.; Argyropoulou, A.; Perivolioti, E.; Koudoumnakis, N.; Pournaras, S.; Vasilakopoulou, A.; Vourli, S.; Katsifa, H.; et al. COVID-19 and Antimicrobial Resistance: Data from the Greek Electronic System for the Surveillance of Antimicrobial Resistance—WHONET-Greece (January 2018–March 2021). Life 2021, 11, 996. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ICU Patients (%) | Non-ICU Patients (%) | Total | |
|---|---|---|---|
| Gender | |||
| Male | 37 (62) | 22 (38) | 59 |
| Female | 28 (56) | 21 (44) | 49 |
| Age | |||
| 25–34 | - | 3 (100) | 3 |
| 35–44 | 4 (50) | 4 (50) | 8 |
| 45–54 | 9 (56) | 7 (44) | 16 |
| 55–64 | 13 (52) | 12 (48) | 25 |
| 65+ | 39 (70) | 17 (30) | 56 |
| BMI | |||
| Underweight (>18.5) | - | - | |
| Normal (18.8–29.5) | 36 (56) | 28 (43) | 64 |
| Obese (<30) | 29 (66) | 15 (34) | 44 |
| Underlining disease | |||
| Diabetic | 17 (63) | 10 (37) | 27 |
| Non-diabetic | 48 (59) | 33 (41) | 81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bazaid, A.S.; Barnawi, H.; Qanash, H.; Alsaif, G.; Aldarhami, A.; Gattan, H.; Alharbi, B.; Alrashidi, A.; Al-Soud, W.A.; Moussa, S.; et al. Bacterial Coinfection and Antibiotic Resistance Profiles among Hospitalised COVID-19 Patients. Microorganisms 2022, 10, 495. https://doi.org/10.3390/microorganisms10030495
Bazaid AS, Barnawi H, Qanash H, Alsaif G, Aldarhami A, Gattan H, Alharbi B, Alrashidi A, Al-Soud WA, Moussa S, et al. Bacterial Coinfection and Antibiotic Resistance Profiles among Hospitalised COVID-19 Patients. Microorganisms. 2022; 10(3):495. https://doi.org/10.3390/microorganisms10030495
Chicago/Turabian StyleBazaid, Abdulrahman S., Heba Barnawi, Husam Qanash, Ghaida Alsaif, Abdu Aldarhami, Hattan Gattan, Bandar Alharbi, Abdulaziz Alrashidi, Waleed Abu Al-Soud, Safia Moussa, and et al. 2022. "Bacterial Coinfection and Antibiotic Resistance Profiles among Hospitalised COVID-19 Patients" Microorganisms 10, no. 3: 495. https://doi.org/10.3390/microorganisms10030495