
Urinary Tract Infections and Associated Factors among Patients with Indwelling Urinary Catheters Attending Bugando Medical Centre a Tertiary Hospital in Northwestern Tanzania

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Duration and Settings
2.2. Study Population, Inclusion and Exclusion Criteria
2.3. Determination and Definition of Complications
2.4. Data and Sample Collection
2.5. Laboratory Procedures
2.5.1. Urine Culture
2.5.2. Antibiotics Susceptibility Testing and Phenotypic Detection of Extended Spectrum β-Lactamase Production in E. coli and Klebsiella spp.
2.6. Quality Control
2.7. Statistical Analysis
2.8. Ethical Considerations
3. Results
3.1. Socio-Demographic and Clinical Characteristics of Participants with Short-Term IUC (In-Patients) and Long-Term IUC (Out-Patients)
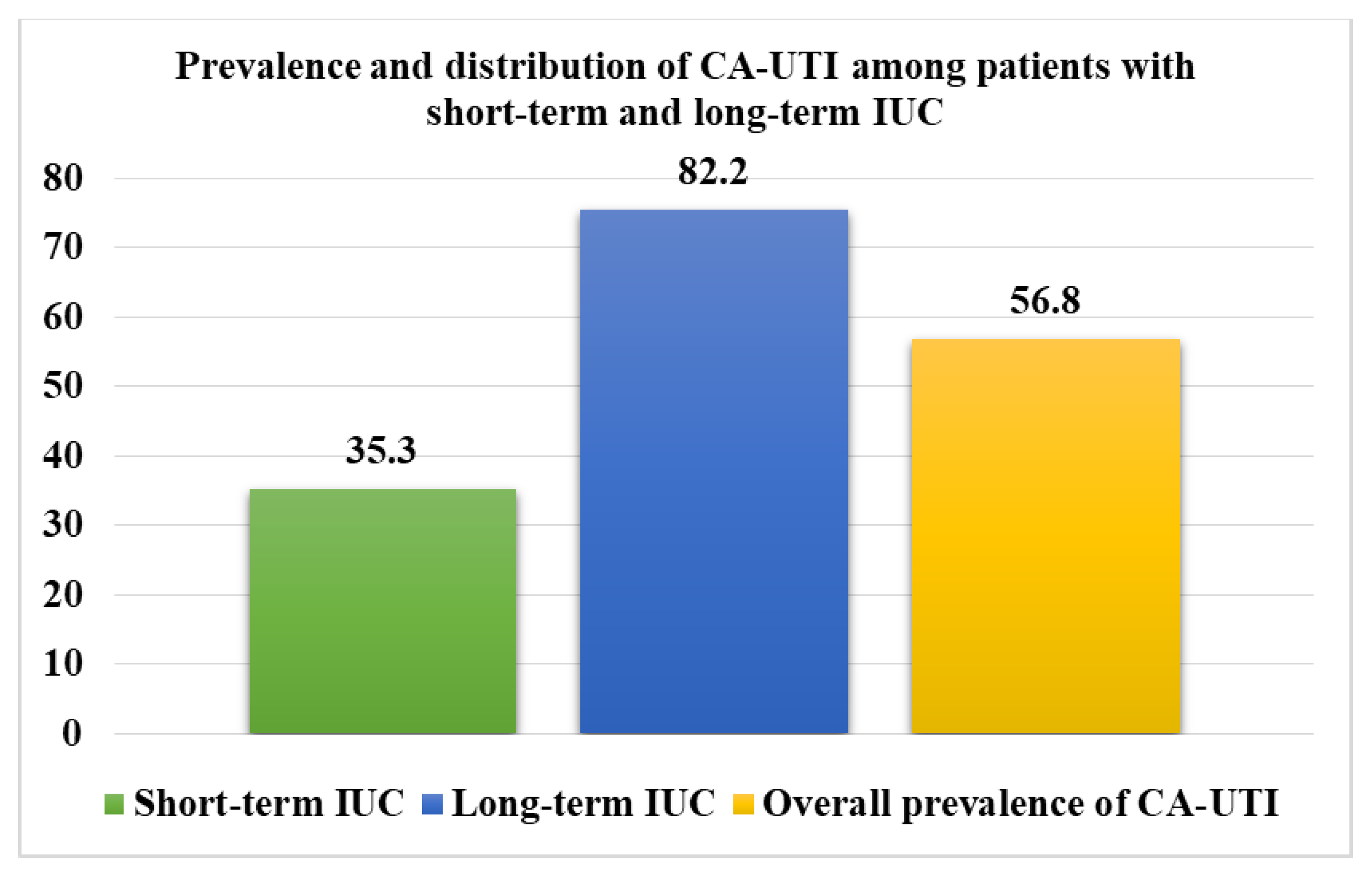
3.2. Prevalence and Pathogens Causing Catheter-Associated Urinary Tract Infection (CA-UTI) among Participants with Short-Term and Long-Term IUC
3.3. Percentages Resistance of Bacteria Causing CA-UTI among Patients with Short-Term and Long-Term IUC
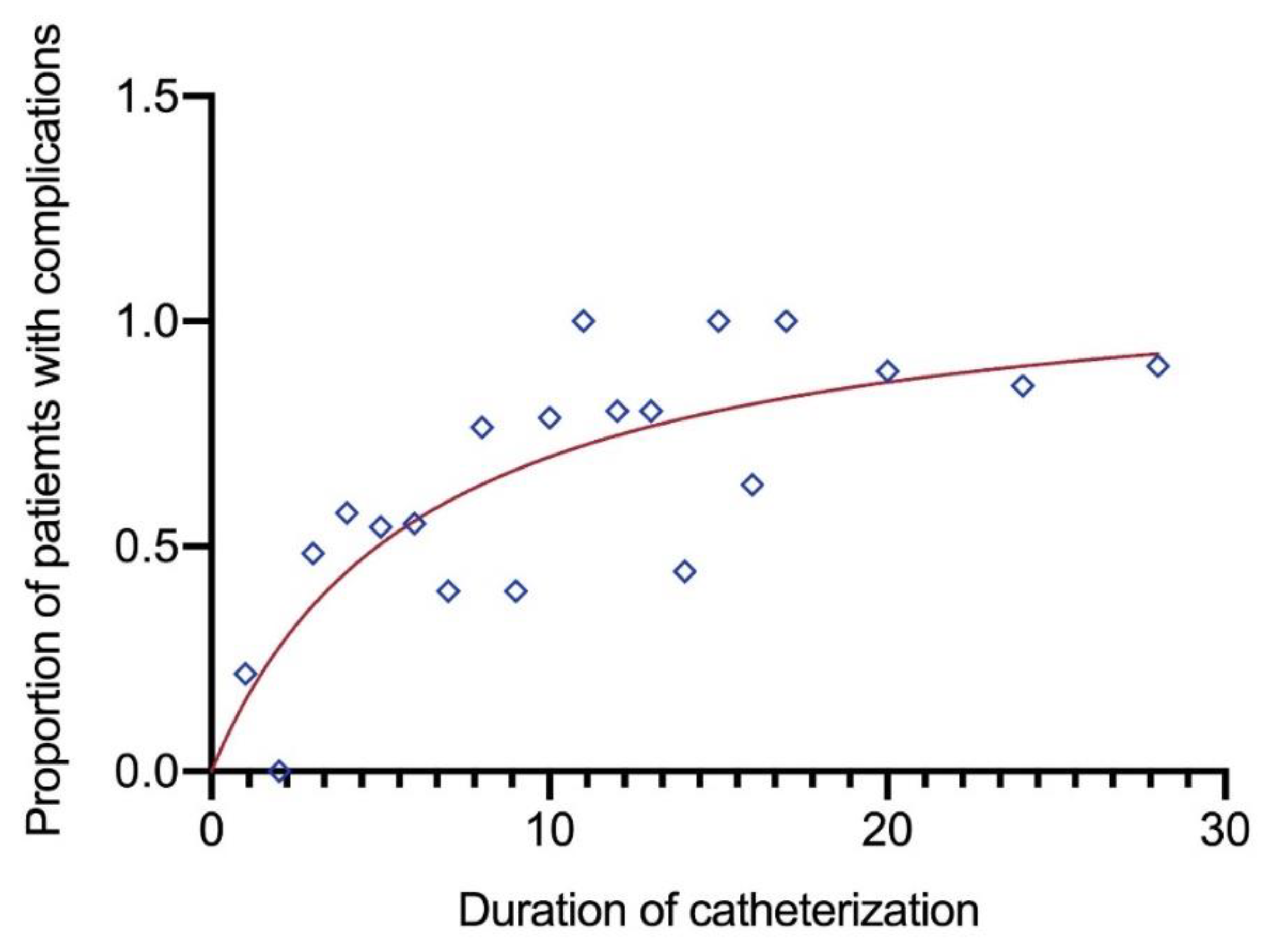
3.4. Factors Associated with Complications among Patients with Short-Term and Long-Term IUC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amaral, G.L.G.D.; Costa, K.M.D.M.; De Lima, C.M.F.; Domingues, T.A.M.; Barbosa, D.A.; Belasco, A.G.S. Quality of life and body image of patients with urinary disorders. Rev. Bras. Enferm. 2020, 73, e20190522. [Google Scholar] [CrossRef] [PubMed]
- Gould, C.V.; Umscheid, C.A.; Agarwal, R.K.; Kuntz, G.; Pegues, D.A. Healthcare Infection Control Practices Advisory Committee (HICPAC) Guideline for Prevention of Catheter-Associated Urinary Tract Infections 2009. Infect. Control Hosp. Epidemiol. 2010, 31, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Niël-Weise, B.S.; Broek, P.J.V.D.; da Silva, E.M.; A Silva, L. Urinary catheter policies for long-term bladder drainage. Cochrane Database Syst. Rev. 2012, 2012, CD004201. [Google Scholar] [CrossRef] [PubMed]
- Waskiewicz, A.; Alexis, O.; Cross, D. Supporting patients with long-term catheterisation to reduce risk of catheter-associated urinary tract infection. Br. J. Nurs. 2019, 28, S4–S17. [Google Scholar] [CrossRef] [PubMed]
- Tenney, J.; Hudson, N.; Alnifaidy, H.; Li, J.T.C.; Fung, K.H. Risk factors for aquiring multidrug-resistant organisms in urinary tract infections: A systematic literature review. Saudi Pharm. J. 2018, 26, 678–684. [Google Scholar] [CrossRef]
- Labib, M.; Spasojevic, N. Problem of Catheter Associated Urinary Tract Infections in Sub–Saharan Africa. In Recent Advances in the Field of Urinary Tract Infections; InTech: London, UK, 2013. [Google Scholar]
- Elvy, J.; Colville, A. Catheter associated urinary tract infection: What is it, what causes it and how can we prevent it? J. Infect. Prev. 2009, 10, 36–41. [Google Scholar] [CrossRef]
- Mshana, E.S.; Matee, M.; Rweyemamu, M. Antimicrobial resistance in human and animal pathogens in Zambia, Democratic Republic of Congo, Mozambique and Tanzania: An urgent need of a sustainable surveillance system. Ann. Clin. Microbiol. Antimicrob. 2013, 12, 28. [Google Scholar] [CrossRef] [Green Version]
- Bagchi, I.; Jaitly, N.K.; Thombare, V. Microbiological Evaluation of Catheter Associated Urinary Tract Infection in a Tertiary Care Hospital. People 2015, 8, 23. [Google Scholar]
- Guneysel, O.; Onur, O.; Erdede, M.; Denizbasi, A. Trimethoprim/Sulfamethoxazole Resistance in Urinary Tract Infections. J. Emerg. Med. 2009, 36, 338–341. [Google Scholar] [CrossRef]
- Jayaprakash, C.; Bai, M.S. A Study of Bacterial Pathogens and Their Antibiotic Susceptibility Profile from Community-Acquired and Hospital-Acquired Urinary Tract Infections. J. Evol. Med. Dent. Sci. 2016, 5, 1400–1404. [Google Scholar] [CrossRef]
- Majumder, M.I.; Ahmed, T.; Ahmed, S.; Khan, A.R. Microbiology of Catheter Associated Urinary Tract Infection. In Microbiology of Urinary Tract Infections—Microbial Agents and Predisposing Factors; Sciyo: London, UK, 2019. [Google Scholar]
- Jacobsen, S.M.; Stickler, D.J.; Mobley, H.L.T.; Shirtliff, M.E. Complicated Catheter-Associated Urinary Tract Infections Due to Escherichia coli and Proteus mirabilis. Clin. Microbiol. Rev. 2008, 21, 26–59. [Google Scholar] [CrossRef] [Green Version]
- Juhász, J.; Ligeti, B.; Gajdács, M.; Makra, N.; Ostorházi, E.; Farkas, F.; Stercz, B.; Tóth, Á.; Domokos, J.; Pongor, S.; et al. Colonization Dynamics of Multidrug-Resistant Klebsiella pneumoniae Are Dictated by Microbiota-Cluster Group Behavior over Individual Antibiotic Susceptibility: A Metataxonomic Analysis. Antibiotics 2021, 10, 268. [Google Scholar] [CrossRef] [PubMed]
- Søgaard, M.; Heide-Jørgensen, U.; Vandenbroucke, J.P.; Schønheyder, H.C.; Vandenbroucke-Grauls, C. Risk factors for extend-ed-spectrum β-lactamase-producing Escherichia coli urinary tract infection in the community in Denmark: A case-control study. Clin. Microbiol. Infect. 2017, 23, 952–960. [Google Scholar] [CrossRef] [Green Version]
- Shiralizadeh, S.; Taghizadeh, S.; Asgharzadeh, M.; Shokouhi, B.; Gholizadeh, P.; Rahbar, M.; Kafil, H.S. Urinary tract infections: Raising problem in developing countries. Rev. Med. Microbiol. 2018, 29, 159–165. [Google Scholar] [CrossRef]
- Landi, F.; Cesari, M.; Onder, G.; Zamboni, V.; Barillaro, C.; Lattanzio, F.; Bernabei, R. Indwelling urethral catheter and mortality in frail elderly women living in community. Neurourol. Urodyn. 2004, 23, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Kralik, D.; Seymour, L.; Eastwood, S.; Koch, T. Managing the self: Living with an indwelling urinary catheter. J. Clin. Nurs. 2007, 16, 177–185. [Google Scholar] [CrossRef]
- Northwood, M. Adults experienced a long term indwelling urinary catheter as living with the forces of flowing water. Évid. Based Nurs. 2002, 5, 125. [Google Scholar] [CrossRef] [Green Version]
- Ndomba, A.L.M.; Laisser, R.M.; Kidenya, B.R.; Kohi, T.W.; Mwanga, J.R.; Mshana, S.E. Prevalence and indications of long-term indwelling urinary catheter among out-patients attending urology clinic at a tertiary hospital in Northwestern Tanzania. Afr. J. Urol. 2021, 27, 1–6. [Google Scholar] [CrossRef]
- Welden, L. Electronic Health Record: Driving Evidence-Based Catheter-Associated Urinary Tract Infections (CAUTI) Care Practices. OJIN Online J. Issues Nurs. 2013, 18, 50–59. [Google Scholar] [CrossRef]
- Zhu, Z.; Wang, Z.; Li, S.; Yuan, X. Antimicrobial strategies for urinary catheters. J. Biomed. Mater. Res. Part A 2019, 107, 445–467. [Google Scholar] [CrossRef]
- Vasudevan, R. Urinary Tract Infection: An Overview of the Infection and the Associated Risk Factors. J. Microbiol. Exp. 2014, 1, 42–54. [Google Scholar] [CrossRef]
- Prinjha, S. CA: Living with an indwelling urinary catheter. Eur. PMC 2013, 109, 12–14. [Google Scholar]
- Garibaldi, R.A.; Burke, J.P.; Dickman, M.L.; Smith, C.B. Factors Predisposing to Bacteriuria during Indwelling Urethral Catheterization. N. Engl. J. Med. 1974, 291, 215–219. [Google Scholar] [CrossRef]
- Willson, M.; Wilde, M.; Webb, M.-L.; Thompson, D.; Parker, D.; Harwood, J.; Callan, L.; Gray, M. Nursing Interventions to Reduce the Risk of Catheter-Associated Urinary Tract Infection. J. Wound Ostomy Cont. Nurs. 2009, 36, 137–154. [Google Scholar] [CrossRef] [Green Version]
- Gardner, A.; Mitchell, B.; Beckingham, W.; Fasugba, O. A point prevalence cross-sectional study of healthcare-associated urinary tract infections in six Australian hospitals. BMJ Open 2014, 4, e005099. [Google Scholar] [CrossRef] [Green Version]
- Geng, V.; Cobussen-Boekhorst, H.; Farrell, J.; Gea Sánchez, M.; Pearce, I.; Schwennesen, T.; Vahr, S.; Vandewinkel, C. Catheterisation. Indwelling Catheters in Adults. Urethral and Suprapubic. Evidence-Based Guidelines for Best Practice in Urological Health Care. European Association of Urology Nurses (EAUN): Arnhem, The Netherlands, 2012. [Google Scholar]
- Letica-Kriegel, A.S.; Salmasian, H.; Vawdrey, D.K.; Youngerman, B.; A Green, R.; Furuya, E.Y.; Calfee, D.P.; Perotte, R. Identifying the risk factors for catheter-associated urinary tract infections: A large cross-sectional study of six hospitals. BMJ Open 2019, 9, e022137. [Google Scholar] [CrossRef] [Green Version]
- Stickler, D.J.; Feneley, R.C.L. The encrustation and blockage of long-term indwelling bladder catheters: A way forward in prevention and control. Spinal Cord 2010, 48, 784–790. [Google Scholar] [CrossRef]
- Ikegami, Y.; Yoshida, K.; Imaizumi, T.; Isosu, T.; Kurosawa, S.; Murakawa, M. Life-threatening urethral hemorrhage after placement of a Foley catheter in a patient with uroseptic disseminated intravascular coagulation due to chronic urinary retention induced by untreated benign prostatic hyperplasia. Acute Med. Surg. 2016, 3, 407–410. [Google Scholar] [CrossRef] [Green Version]
- Ekwealor, P.A.; Ugwu, M.C.; Ezeobi, I.; Amalukwe, G.; Ugwu, B.C.; Okezie, U.; Stanley, C.; Esimone, C. Antimicrobial Evaluation of Bacterial Isolates from Urine Specimen of Patients with Complaints of Urinary Tract Infections in Awka, Nigeria. Int. J. Microbiol. 2016, 2016, 9740273. [Google Scholar] [CrossRef] [Green Version]
- Pérez, R.P.; Ortega, M.J.C.; Álvarez, J.A.; Baquero-Artigao, F.; Rico, J.C.S.; Zúñiga, R.V.; Campos, L.M.; Gallego, B.C.; Fernández, A.J.C.; Calvo, C.; et al. Recommendations on the diagnosis and treatment of urinary tract infection. An. Pediatría 2019, 90, 400.e1–400.e9. [Google Scholar] [CrossRef]
- CLSI. C: Performance Standards for Antimicrobial Susceptibility Testing; Clinical Lab Standards Institute: Wayne, PA, USA, 2016. [Google Scholar]
- Igawa, Y.; Wyndaele, J.-J.; Nishizawa, O. Catheterization: Possible complications and their prevention and treatment. Int. J. Urol. 2008, 15, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Mackay, W.G.; MacIntosh, T.; Kydd, A.; Fleming, A.; O’Kane, C.; Shepherd, A.; Hagen, S.; Williams, C.; Mundie, J.; Russell, C.; et al. Living with an indwelling urethral catheter in a community setting: Exploring triggers for unscheduled community nurse “out-of-hours” visits. J Clin Nurs. 2018, 27, 866–875. [Google Scholar] [CrossRef] [PubMed]
- Stöhrer, M.; Castro-Diaz, D.; Chartier-Kastler, E.; Kramer, G.; Mattiasson, A.; Wyndaele, J.J. Guidelines on neurogenic lower urinary tract dysfunction. Progrès en Urologie 2007, 17, 703–755. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, E.L. Catheter associated urinary tract infections. Antimicrob. Resist. Infect. Control 2014, 3, 23. [Google Scholar] [CrossRef] [Green Version]
- Amalaradjou, M.A.R.; Venkitanarayanan, K. Role of bacterial biofilms in catheter-associated urinary tract infections (CAUTI) and strategies for their control. Recent Adv. Field Urin. Tract Infect. 2013, 10, 1–32. [Google Scholar]
- Acker, N. Reducing the risk of infection in indwelling catheterisation. J. Community Nurs. 2014, 28, 28. [Google Scholar]
- Emr, K.; Ryan, R. Best practice for indwelling catheter in the home setting. Home Health Nurse J. Home Care Hosp. Prof. 2004, 22, 820–828. [Google Scholar]
- Dougnon, T.V.; Bankole, H.S.; Johnson, R.C.; Hounmanou, G.; Toure, I.; Houessou, C.; Boko, M.; Baba-Moussa, L. Catheter-associated urinary tract infections at a hospital in Zinvie, Benin (West Africa). Int. J. Infect. 2016, 3, e34141. [Google Scholar] [CrossRef]
- Feneley, R.C.L.; Hopley, I.B.; Wells, P.N.T. Urinary catheters: History, current status, adverse events and research agenda. J. Med Eng. Technol. 2015, 39, 459–470. [Google Scholar] [CrossRef] [Green Version]
- Vaidyanathan, S.; Ward, J.; Soni, B.M.; Hughes, P.; Oo, T. Persistent urine leakage around a suprapubic catheter: The experience of a person with chronic tetraplegia. Spinal Cord Ser. Cases 2018, 4, 31. [Google Scholar] [CrossRef] [Green Version]
- Wilde, M.H.; McMahon, J.M.; Crean, H.F.; Brasch, J. Exploring relationships of catheter-associated urinary tract infection and blockage in people with long-term indwelling urinary catheters. J. Clin. Nurs. 2017, 26, 2558–2571. [Google Scholar] [CrossRef] [PubMed]
- Podkovik, S.; Toor, H.; Gattupalli, M.; Kashyap, S.; Brazdzionis, J.; Patchana, T.; Bonda, S.; Wong, S.; Kang, C.; Mo, K. Prevalence of catheter-associated urinary tract infections in neurosurgical intensive care patients–the overdiagnosis of urinary tract infec-tions. Cureus 2019, 11, e5494–e5503. [Google Scholar] [PubMed] [Green Version]
- Getliffe, K.; Newton, T. Catheter-associated urinary tract infection in primary and community health care. Age Ageing 2006, 35, 477–481. [Google Scholar] [CrossRef] [Green Version]
- Indwelling Urinary Catheter-Insertion and Ongoing Care. Available online: https://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/Indwelling_urinary_catheter_insertion_and_ongoing_care (accessed on 31 January 2022).
- Hedawoo, J.B.; Deshmukh, K.S. A Study to Determine the Prevalence of Catheter Associated Urinary Tract Infection in Surgical Wards and Recovery Room in a Tertiary Healthcare Centre in Central India. Int. J. Sci. Res. 2019, 8, 871–875. [Google Scholar]
- Petronio Petronio, G.; Cutuli, M.A.; Magnifico, I.; Venditti, N.; Pietrangelo, L.; Vergalito, F.; Pane, A.; Scapagnini, G.; Di Marco, R. In vitro and in vivo biological activity of berberine chloride against uropathogenic E. coli strains using Galleria mellonella as a host model. Molecules 2020, 25, 5010. [Google Scholar] [CrossRef] [PubMed]
- Marando, R.; Seni, J.; Mirambo, M.M.; Falgenhauer, L.; Moremi, N.; Mushi, M.; Kayange, N.; Manyama, F.; Imirzalioglu, C.; Chakraborty, T.; et al. Predictors of the extended-spectrum-beta lactamases producing Enterobacteriaceae neonatal sepsis at a tertiary hospital, Tanzania. Int. J. Med. Microbiol. 2018, 308, 803–811. [Google Scholar] [CrossRef]
- Silago, V.; Kovacs, D.; Msanga, D.R.; Seni, J.; Matthews, L.; Oravcová, K.; Zadoks, R.N.; Lupindu, A.M.; Hoza, A.S.; Mshana, S.E. Bacteremia in critical care units at Bugando Medical Centre, Mwanza, Tanzania: The role of colonization and contaminated cots and mothers’ hands in cross-transmission of multidrug resistant Gram-negative bacteria. Antimicrob. Resist. Infect. Control. 2020, 9, 1–14. [Google Scholar] [CrossRef]
- Gajdács, M.; Ábrók, M.; Lázár, A.; Burián, K. Comparative Epidemiology and Resistance Trends of Common Urinary Pathogens in a Tertiary-Care Hospital: A 10-Year Surveillance Study. Medicina 2019, 55, 356. [Google Scholar] [CrossRef] [Green Version]
- Warren, J.W. Catheter-associated urinary tract infections. Infect. Dis. Clin. N. Am. 1997, 11, 609–622. [Google Scholar] [CrossRef]
- Kader, A.A.; Angamuthu, K. Extended-spectrum beta-lactamases in urinary isolates of Escherichia coli, Klebsiella pneumoniae and other gram-negative bacteria in a hospital in Eastern Province, Saudi Arabia. Saudi Med. J. 2005, 26, 956–959. [Google Scholar]
- Maharjan, G.; Khadka, P.; Shilpakar, G.S.; Chapagain, G.; Dhungana, G. Catheter-Associated Urinary Tract Infection and Obstinate Biofilm Producers. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 7624857. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Out-Patients (N = 202), n (%) | In-Patients (N = 238), n (%) | p-Value |
|---|---|---|---|
| Median age [IQR] in years | 69 (61–77) | 46 (30–62) | <0.001 |
| Sex | |||
| Males | 194 (96.0) | 132 (55.5) | <0.001 |
| Females | 8 (4.0) | 106 (44.5) | |
| Residence | |||
| Outside Mwanza | 117 (57.9) | 119 (50) | 0.097 |
| Mwanza | 85 (42.1) | 119 (50) | |
| Marital status | |||
| Married | 187 (92.6) | 195 (81.3) | <0.001 |
| Single | 15 (7.4) | 43 (18.1) | |
| Occupation | |||
| Peasants | 136 (67.3) | 164 (68.9) | <0.001 |
| Retired | 29 (14.4) | 2 (0.8) | |
| Petty traders | 26 (12.9) | 64 (26.9) | |
| Civil servants | 11 (5.5) | 8 (3.4) | |
| Religion | |||
| Christians | 153 (75.7) | 202 (84.9) | 0.041 |
| Muslims | 26 (12.9) | 22 (9.2) | |
| Others | 23 (11.4) | 14 (6.0) | |
| Education | |||
| No formal education | 43 (21.3) | 17 (7.1) | <0.001 |
| Primary level | 116 (57.3) | 198 (83.2) | |
| Secondary level | 29 (14.4) | 18 (7.6) | |
| College and above | 14 (6.9) | 5 (2.1) | |
| Patient Characteristics | Out-Patients (N = 202), n (%) | In-Patients (N = 238), n (%) | p-Value |
|---|---|---|---|
| Type of catheter | |||
| Supra-pubic type | 82 (40.6) | 10 (4.2) | <0.001 |
| Urethral type | 120 (59.4) | 228 (95.8) | |
| Catheter size (FR) | |||
| 14 FR | 19 (9.4) | 70 (29.4) | <0.001 |
| 16 FR | 158 (78.2) | 149 (62.6) | |
| 18 FR | 15 (7.4) | 19 (8.0) | |
| 20 FR | 10 (5.0) | - | |
| Instructions for proper handling of catheters at home for out-patients | |||
| Given | 20 (9.9) | NA | NA |
| Not given | 182 (90.1) | NA | |
| Catheter change for out-patients | |||
| Changed | 123 (61.0) | NA | NA |
| Not changed | 79 (39.1) | NA | |
| Duration of catheter in situ (weeks) | |||
| 0–2 | 0 (0.00) | 238 (100) | <0.001 |
| 3–5 | 91 (45.1) | 0 (0.00) | |
| ≥6 | 111 (55.0) | 0 (0.00) | |
| Comorbidity | |||
| With comorbidity | 44 (21.8) | 48 (20.2) | 0.163 |
| No comorbidity | 158 (78.2) | 190 (79.8) | |
| Indications for catheterization | |||
| BPH | 122 (60.4) | 9 (3.8) | <0.001 |
| Urethral stricture | 37 (18.3) | 19 (8.0) | |
| Urine retention | 24 (11.9) | - | |
| Urinary incontinence | 13 (6.4) | 78 (32.8) | |
| CNS | 2 (0.9) | 24 (10.1) | |
| Fistula | - | 25 (10.5) | |
| Others | 29 (14.4) | 79 (33.2) | |
| Complications associated with IUC | |||
| CA-UTI | 108 (53.5) | 78 (32.7) | 0.005 |
| Leakage and CA-UTI | 25 (11.9) | 2 (0.8) | |
| Blockage and CA-UTI | 21 (10.4) | - | |
| Bleeding and CA-UTI | 12 (5.4) | 4 (1.7) | |
| Leakage of urine | 3 (1.5) | 4 (1.7) | |
| Blockage of catheter | 1 (0.5) | 1 (0.4) | |
| Bleeding | - | 1 (0.4) | |
| None | 34 (16.8) | 149 (62.6) | |
| Bacterial Species | AMP n (R%) | SXT n (R%) | CN n (R%) | CIP n (R%) | AMC n (R%) | CRO n (R%) | CAZ n (R%) | F n (R%) | MEM n (R%) | ESBL n (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive | p-Value | ||||||||||
| E. coli | |||||||||||
| Out-patients (55) | 52 (94.5) | 46 (83.6) | 20 (36.4) | 24 (43.6) | 41 (74.5) | 25 (45.5) | 27 (49.1) | 17 (30.9) | 14 (25.4) | 25 (45.5) | 0.6013 |
| In-patients (24) | 23 (95.8) | 21 (87.5) | 14 (58.3) | 16 (66.7) | 22 (91.7) | 12 (50.0) | 13 (54.2) | 11 (45.8) | 0 (0.0) | 12 (50.0) | |
| All (79) | 75 (94.6) | 67 (84.8) | 34 (43.0) | 40 (50.6) | 63 (79.7) | 37 (46.8) | 40 (50.6) | 28 (35.4) | 14 (17.7) | 37 (50.6) | - |
| Klebsiella spp. | |||||||||||
| Out-patients (47) | 47 (100) | 38 (80.9) | 11 (23.4) | 13 (27.7) | 38 (80.8) | 19 (40.4) | 18 (38.3) | 20 (42.6) | 12 (25.5) | 18 (38.3) | 0.0766 |
| In-patients (29) | 29 (100) | 25 (86.2) | 13 (44.8) | 12 (41.4) | 23 (79.3) | 17 (58.6) | 15 (51.7) | 15 (51.7) | 0 (0.0) | 18 (62.1) | |
| All (76) | 76 (100) | 63 (82.9) | 24 (31.6) | 25 (32.9) | 61 (80.3) | 36 (47.4) | 33 (43.4) | 35 (46.1) | 12 (15.7) | 36 (47.4) | - |
| Other Gram-negative rods (GNR) | |||||||||||
| Out-patients (69) * | 46 (80.7) | 34 (59.6) | 14 (20.3) | 22 (31.9) | 56 (81.3) | 19 (33.3) | 23 (33.3) | 31 (44.9) | 19 (27.5) | NT | NA |
| In-patients (30) ** | 11 (52.4) | 9 (42.9) | 6 (20.0) | 9 (30.0) | 23 (76.4) | 7 (33.3) | 6 (20.0) | 9 (30.0) | 0 (0.0) | NT | NA |
| All GNR (99) *** | 57 (73.1) | 43 (55.1) | 20 (20.2) | 31 (31.3) | 79 (79.6) | 26 (33.3) | 29 (29.3) | 40 (40.4) | 19 (19.2) | NT | NA |
| Patients’ Characteristics | Patients with Long-Term IUC (Out-Patients) | Patients with Short-Term IUC (In-Patients) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Complications | Analysis | Complications | Analysis | ||||||
| YES n (%) | NO n (%) | OR [95%CI] | p-Value | YES n (%) | NO n (%) | OR [9 5%CI] | p-Value | ||
| Age in years | 69 (61–77) years | 168 (83.2) | 34 (16.8) | 0.99 [0.96–1.0] | 0.341 | NA | NA | NA | NA |
| 46 (30–62) years | NA | NA | NA | NA | 89 (37.4 | 149 (62.6) | 0.9 [0.98–1.0] | 0.309 | |
| Gender | Males | 162 (83.5) | 32 (16.5) | 1.0 | 0.533 | 38 (28.8) | 94 (71.2) | 1.0 | 0.002 |
| Females | 6 (75) | 2 (25.0) | 0.6 [0.1–3.1] | 51 (48.1) | 55 (51.9) | 2.3 [1.3–3.9] | |||
| Marital status | Single | 13 (86.7) | 2 (13.3) | 1.0 | 0.708 | 17 (39.5) | 26 (60.5) | 1.0 | 0.749 |
| Married | 155 (82.9) | 32 (17.1) | 0.7 [0.2–3.5] | 72 (36.9) | 123 (63.1) | 0.9 [0.5–1.8] | |||
| Education level | No formal education | 31 (72.1) | 12 (27.9) | 1.0 | 0.029 | 12 (70.6) | 5 (29.4) | 1.0 | 0.092 |
| Primary | 97 (83.6) | 19 (16.4) | 1.8 [1.1–3.1] | 68 (34.3) | 130 (65.7) | 0.6 [0.3–1.1] | |||
| Secondary | 28 (96.6) | 1 (3.5) | 8 (44.4) | 10 (55.6) | |||||
| College | 12 (85.7) | 2 (14.3) | 1 (20.0) | 4 (80.4) | |||||
| Comorbidity | HIV/AIDS | 3 (100) | 0 (0.00) | 1.0 | 0.757 | 2 (22.2) | 7 (77.8) | 1.0 | 0.408 |
| DM | 6 (100) | 0 (0.00) | 0.99 [0.99–1.0] | 1 (14.3) | 6 (85.7) | 0.9 [0.9–1.0] | |||
| HTN | 13 (81.3) | 3 (18.8) | 1 (8.3) | 11 (91.7) | |||||
| Anemia | 4 (66.7) | 2 (33.3) | 8 (47.1) | 9 (52.9) | |||||
| Others | 33 (84.6) | 6 (15.4) | 22 (57.9) | 16 (42.1) | |||||
| None | 109 (82.6) | 23 (17.4) | 55 (35.5) | 100 (64.5) | |||||
| Duration of catheter | <2 weeks | NA | NA | NA | NA | 89 (37.4) | 149 (62.6) | Collinearity | NA |
| 3–5 weeks | 71 (78.0) | 20 (22) | 1.0 | 0.080 | NA | NA | NA | NA | |
| ≥6 weeks | 97 (87.4) | 14 (12.6) | 1.9 [0.9–4.1] | NA | NA | NA | NA | ||
| Type of catheter | Urethral | 101 (84.2) | 19 (15.8) | 1.0 | 0.647 | 84 (36.8) | 144 (63.2) | 1.0 | 0.405 |
| Supra-pubic | 67 (81.7) | 15 (18.3) | 1.2 [0.6–2.5] | 5 (50.0) | 5 (50.0) | 0.6 [0.2–2.1] | |||
| Catheter size | 14 FR | 17 (89.5) | 2 (10.5) | 1.0 | 0.923 | 31 (44.3) | 39 (55.7) | 1.0 | 0.167 |
| 16 FR | 130 (82.3) | 28 (17.7) | 1.0 [0.5–1.8] | 52 (34.9) | 97 (65.1) | 0.7 [0.5–1.1] | |||
| 18 FR | 12 (80) | 3 (20) | 6 (31.6) | 13 (68.4) | |||||
| 20–26 FR | 9 (90.0) | 1 (10.0) | NA | NA | |||||
| Indication for catheterization | BPH | 98 (80.3) | 24 (19.7) | 1.0 | 0.539 | 2 (22.2) | 7 (77.8) | 1.0 | 0.145 |
| Urethral stricture | 33 (89.2) | 4 (10.8) | 1.1 [0.8–1.4] | 6 (31.6) | 13 (68.4) | 1.1 [0.9–1.3] | |||
| Urinary incontinence | 12 (92.3) | 1 (7.7) | 18 (23.1) | 60 (76.9) | |||||
| CNS/unconsciousness | 0 (0.00) | 1 (100) | 11 (39.3) | 17 (60.7) | |||||
| Fistula | - | - | 23 (92.0) | 2 (8.0) | |||||
| Others | 25 (86.2) | 4 (13.8) | 29 (36.7) | 50 (63.3) | |||||
| Instructions on living with catheter at home | Not given | 116 (63.7) | 66 (36.3) | 1.0 | 0.110 | NA | NA | NA | NA |
| Given | 11 (55.0) | 9 (45.0) | 0.5 [0.2–1.2] | NA | NA | NA | |||
| Residence | Mwanza | 72 (84.7) | 13 (15.3) | 1.0 | 0.619 | 29 (24.4) | 90 (75.6) | 1.0 | <0.001 |
| Outside Mwanza | 96 (82.0) | 21 (17.9) | 1.2 [0.6–2.6] | 60 (50.4) | 59 (49.6) | 0.3 [0.2–0.5] | |||
| Occupations | Retired | 23 (79.3) | 6 (20.7) | 1.0 | 0.399 | 1 (50.0) | 1 (50.0) | 1.0 | 0.539 |
| Peasants | 112 (82.4) | 24 (17.6) | 1.2 [0.8–2.0] | 63 (38.4) | 101 (61.6) | 0.9 [0.7–1.2] | |||
| Civil servants | 11 (100) | 0 (0.00) | 3 (37.5) | 5 (62.5) | |||||
| Petty traders | 22 (84.6) | 4 (15.4) | 22 (34.4) | 42 (65.6) | |||||
| Positioning of urine bags | Hanging freely | NA | NA | NA | NA | 45 (29.4) | 108 (70.6) | 1.0 | <0.001 |
| Not hanging freely | NA | NA | NA | 44 (51.8) | 41 (48.2) | 0.4 [0.2–0.8] | |||
| Wards | Medical | NA | NA | NA | NA | 10 (23.3) | 33 (76.7) | 1.0 | 0.644 |
| Surgical | NA | NA | NA | 65 (44.2) | 82 (55.8) | 1.1 [0.7–1.7] | |||
| Others | NA | NA | NA | 14 (29.2) | 34 (70.8) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndomba, A.L.M.; Laisser, R.M.; Silago, V.; Kidenya, B.R.; Mwanga, J.; Seni, J.; Mshana, S.E. Urinary Tract Infections and Associated Factors among Patients with Indwelling Urinary Catheters Attending Bugando Medical Centre a Tertiary Hospital in Northwestern Tanzania. Microorganisms 2022, 10, 473. https://doi.org/10.3390/microorganisms10020473
Ndomba ALM, Laisser RM, Silago V, Kidenya BR, Mwanga J, Seni J, Mshana SE. Urinary Tract Infections and Associated Factors among Patients with Indwelling Urinary Catheters Attending Bugando Medical Centre a Tertiary Hospital in Northwestern Tanzania. Microorganisms. 2022; 10(2):473. https://doi.org/10.3390/microorganisms10020473
Chicago/Turabian StyleNdomba, Asteria L. M., Rose M. Laisser, Vitus Silago, Benson R. Kidenya, Joseph Mwanga, Jeremiah Seni, and Stephen E. Mshana. 2022. "Urinary Tract Infections and Associated Factors among Patients with Indwelling Urinary Catheters Attending Bugando Medical Centre a Tertiary Hospital in Northwestern Tanzania" Microorganisms 10, no. 2: 473. https://doi.org/10.3390/microorganisms10020473