
Factors Affecting the Intraluminal Therapy for Helicobacter pylori Infection


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.1.1. Intraluminal Triple Antibiotic Therapy
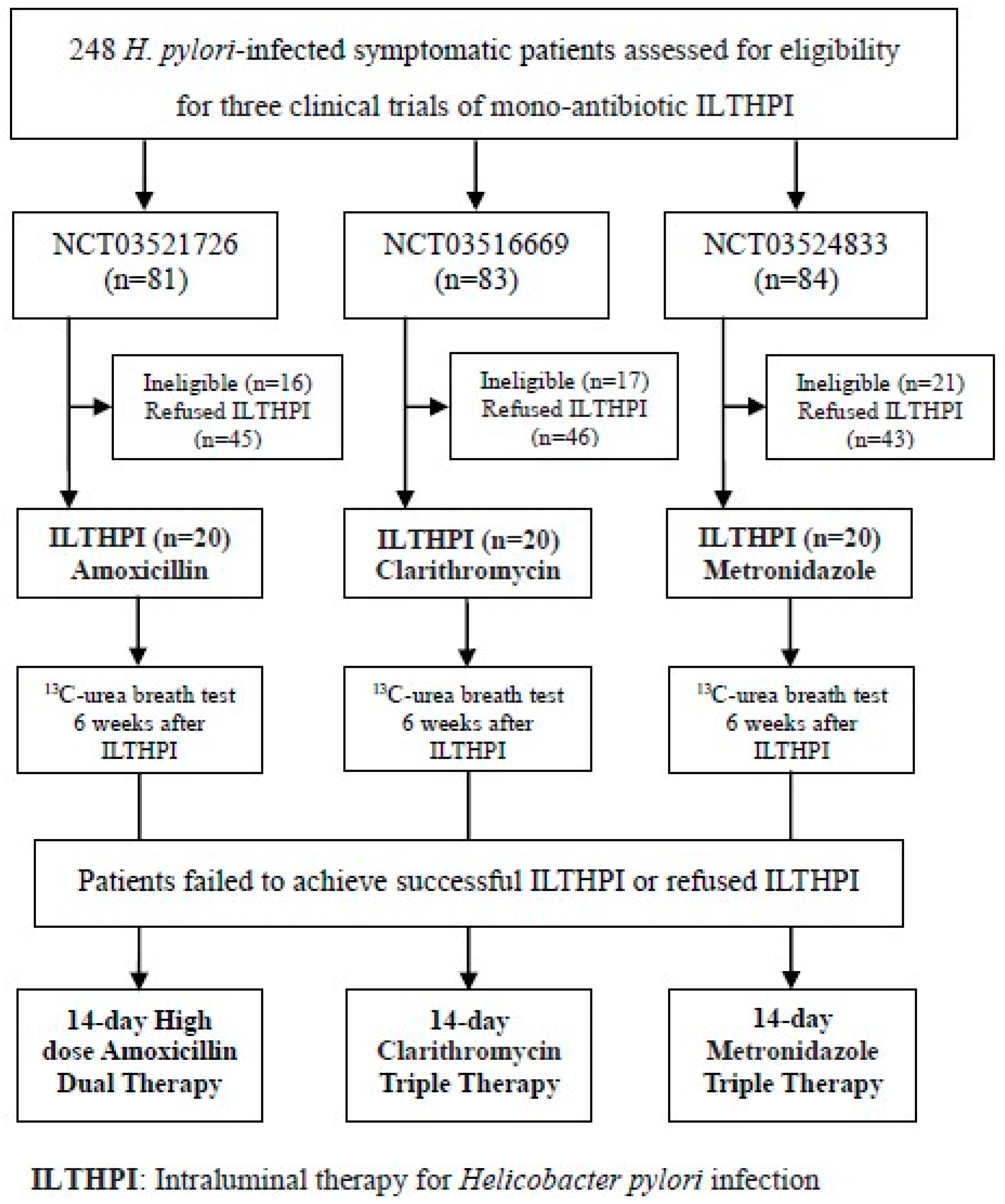
2.1.2. Intraluminal Mono-Antibiotic Therapy
2.2. Methods
2.2.1. Detection of Gastric Juice pH
2.2.2. Intraluminal Therapy for Helicobacter pylori Infection
2.2.3. Oral Antibiotic Therapy for Patients Failed ILTHPI
2.3. Statistical Analysis
3. Results
3.1. Factors Affecting the ILTHPI
3.2. Characteristics of H. pylori Infected Patients
3.3. The Efficacy and Adverse Event of ILTHPI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y. Global prevalence of Helicobacter pylori infection: Systematic review and meta-analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef] [PubMed]
- Plummer, M.; Franceschi, S.; Vignat, J.; Forman, D.; de Martel, C. Global burden of gastric cancer attributable to Helicobacter pylori. Int. J. Cancer 2015, 136, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-C.; Chiang, T.-H.; Chou, C.-K.; Tu, Y.-K.; Liao, W.-C.; Wu, M.-S.; Graham, D.Y. Association Between Helicobacter pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-analysis. Gastroenterology 2016, 150, 1113–1124.e5. [Google Scholar] [CrossRef] [Green Version]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2016, 43, 514–533. [Google Scholar] [CrossRef] [Green Version]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology 2016, 151, 51–69. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection—The Maastricht V/Florence Consensus Report. European Helicobacter and Microbiota Study Group and Consensus panel. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e17. [Google Scholar] [CrossRef] [Green Version]
- Liang, C.-M.; Tai, W.-C.; Hsu, P.-I.; Wu, D.-C.; Kuo, C.-H.; Tsay, F.-W.; Lee, C.-L.; Chen, K.-Y.; Chuah, S.-K. Trend of changes in antibiotic resistance in Helicobacter pylori from 2013 to 2019, a multicentre report from Taiwan. Ther. Adv. Gastroenterol. 2020, 13, 1756284820976990. [Google Scholar] [CrossRef]
- WHO Publishes List of Bacteria for Which New Antibiotics Are Urgently Needed. Available online: https://www.who.int/news-room/detail/27-022017 (accessed on 12 December 2021).
- Liou, T.-C.; Liao, P.-H.; Lin, Y.-C.; Chu, C.-H.; Shih, S.-C. Intraluminal therapy for Helicobacter pylori infection. J. Gastroenterol. Hepatol. 2019, 34, 1337–1343. [Google Scholar] [CrossRef]
- Wang, Y.-C.; Chen, Y.-P.; Ho, C.-Y.; Liu, T.-W.; Chu, C.-H.; Wang, H.-Y.; Liou, T.-C. The Impact of Gastric Juice pH on the Intraluminal Therapy for Helicobacter pylori Infection. J. Clin. Med. 2020, 9, 1852. [Google Scholar] [CrossRef] [PubMed]
- de Boer, W.A.; Thys, J.C.; Borody, T.J.; Graham, D.Y.; O’Morain, C.O.; Tytgat, G.N.J. Proposal for use of a standard side effect scoring system in studies exploring Helicobacter pylori treatment regimens. Eur. J. Gastroenterol. Hepatol. 1996, 8, 641–643. [Google Scholar] [PubMed]
- Aziz, F.; Chakarobaty, A.; Liu, K.; Zhang, T.; Li, X.; Du, R.; Monts, J.; Xu, G.; Li, Y.; Bai, R.; et al. Gastric tumorigenesis induced by combining Helicobacter pylori infection and chronic alcohol through IL-10 inhibition. Carcinogenesis 2021, bgab114. [Google Scholar] [CrossRef] [PubMed]
- Aziz, F.; Xin, M.; Gao, Y.; Chakroborty, A.; Khan, I.; Monts, J.; Monson, K.; Bode, A.M.; Dong, Z. Induction and Prevention of Gastric Cancer with Combined Helicobacter Pylori and Capsaicin Administration and DFMO Treatment, Respectively. Cancers 2020, 12, 816. [Google Scholar] [CrossRef] [Green Version]
- Sheu, B.-S.; Wu, M.-S.; Chiu, C.-T.; Lo, J.-C.; Wu, D.-C.; Liou, J.-M.; Wu, C.-Y.; Cheng, H.-C.; Lee, Y.-C.; Hsu, P.-I.; et al. Consensus on the clinical management, screening-to-treat, and surveillance of Helicobacter pylori infection to improve gastric cancer control on a nationwide scale. Helicobacter 2017, 22, e12368. [Google Scholar] [CrossRef] [Green Version]
- Liou, J.-M.; Malfertheiner, P.; Lee, Y.-C.; Sheu, B.-S.; Sugano, K.; Cheng, H.-C.; Yeoh, K.G.; Hsu, P.-I.; Goh, K.-L.; Mahachai, V.; et al. Asian Pacific Alliance on Helicobacter and Microbiota (APAHAM). Screening and eradication of Helicobacter pylori for gastric cancer prevention: The Taipei global consensus. Gut 2020, 69, 2093–2112. [Google Scholar] [CrossRef]
- Gisbert, J.P. Empirical or susceptibility-guided treatment for Helicobacter pylori infection? A comprehensive review. Ther. Adv. Gastroenterol. 2020, 13, 1–16. [Google Scholar] [CrossRef]
- Liou, J.-M.; Chang, C.-Y.; Chen, M.-J.; Chen, C.-C.; Fang, Y.-J.; Lee, J.-Y.; Wu, J.-Y.; Luo, J.-C.; Liou, T.-C.; Chang, W.-H.; et al. The primary resistance of Helicobacter pylori in Taiwan after the national policy to restrict antibiotic consumption and its relation to virulence factors—A nationwide study. Taiwan Gastrointestinal Disease and Helicobacter Consortium. PLoS ONE 2015, 10, e0124199. [Google Scholar] [CrossRef]
- Khadangi, F.; Yassi, M.; Kerachian, M.A. Review: Diagnostic accuracy of PCR-based detection tests for Helicobacter pylori in stool samples. Helicobacter 2017, 22, e12444. [Google Scholar] [CrossRef]
- Graham, D.Y.; Lew, G.M.; Malaty, H.M.; Evans, D.G.; Evans, D.J.; Klein, P.D.; Alpert, L.C.; Genta, R.M. Factors influencing the eradication of Helicobacter pylori with triple therapy. Gastroenterology 1992, 102, 493–496. [Google Scholar] [CrossRef]
- Byun, Y.H.I.; Jo, Y.J.; Kim, S.C.; Lee, J.S.; Shin, W.Y.; Park, Y.S.; Kim, S.H.; Lee, H.H.; Song, M.H. Clinical factors that predicts successful eradication of Helicobacter pylori. Korean J. Gastroenterol. 2006, 48, 172–179. [Google Scholar] [PubMed]
- Cai, W.Z.; Zhou, L.; Ren, W.; Deng, L.; Yu, M. Variables Influencing Outcome of Helicobacter pylori Eradication Therapy in South China. Helicobacter 2009, 14, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Tang, G.; Pan, L.; Zhu, H.; Zhou, S.; Wei, Z. Clinical factors associated with initial Helicobacter pylori eradication therapy: A retrospective study in China. Sci. Rep. 2020, 10, 15403. [Google Scholar] [CrossRef] [PubMed]
- Mamori, S.; Higashida, A.; Kawara, F.; Ohnishi, K.; Takeda, A.; Senda, E.; Ashida, C.; Yamada, H. Age-dependent eradication of Helicobacter pylori in Japanese patients. World J. Gastroenterol. 2010, 16, 4176–4179. [Google Scholar] [CrossRef] [PubMed]
- Sung, E.K.; Moo, I.P.; Seun, J.P.; Won, M.; Youn, J.C.; Ji, H.C.; Hye, J.K.; Ki, H.K.; Chang, H.Y.; Jae, H.K.; et al. Trends in Helicobacter pylori eradication rates by first-line triple therapy and related factors in eradication therapy. Korean J. Intern. Med. 2015, 30, 801–807. [Google Scholar]
- Osato, M.S.; Reddy, R.; Reddy, S.G.; Penland, R.L.; Malaty, H.M.; Graham, D.Y. Pattern of primary resistance of Helicobacter pylori to metronidazole or clarithromycin in the United States. Arch. Intern. Med. 2001, 161, 1217–1220. [Google Scholar] [CrossRef] [Green Version]
- Abdullahi, M.; Annibale, B.; Capoccia, D.; Tari, R.; Lahner, E.; Osborn, J.; Leonetti, F.; Severi, C. The Eradication of Helicobacter pylori is Affected by Body Mass Index (BMI). Obes. Surg. 2008, 18, 1450–1454. [Google Scholar] [CrossRef]
- Nam, S.J.; Park, S.C.; Lee, S.H.; Choi, D.W.; Lee, S.J.; Bang, C.S.; Baik, G.H.; Park, J.K. Helicobacter pylori eradication in patients with type 2 diabetes mellitus: Multicenter prospective observational study. SAGE Open Med. 2019, 7, 1–7. [Google Scholar] [CrossRef]
- Arslan, E.; Atilgan, H.; Yavaşoğlu, I. The prevalence of Helicobacter pylori in obese subjects. Eur. J. Intern. Med. 2009, 20, 695–697. [Google Scholar] [CrossRef]
- Xu, X.; Li, W.; Qin, L.; Yang, W.; Yu, G.; Wei, Q. Relationship between Helicobacter pylori infection and obesity in Chinese adults: A systematic review with meta-analysis. PLoS ONE 2019, 14, e0221076. [Google Scholar] [CrossRef]
- Chen, L.W.; Kuo, S.F.; Chen, C.H.; Chien, C.H.; Lin, C.L.; Chien, R.N. A community-based study on the association between Helicobacter pylori Infection and obesity. Sci. Rep. 2018, 8, e10746. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki, S.; Sakamoto, H.; Hayashi, Y.; Shinozaki, K.; Lefor, A.K.; Yamamoto, H. Elevated Serum anti-Helicobacter pylori IgG Levels is a Predictor of Successful Eradication Therapy. J. Gastroenterol. Hepatol. Res. 2015, 4, 1797–1800. [Google Scholar] [CrossRef] [Green Version]
- Boltin, D.; Levi, Z.; Perets, T.T.; Schmilovitz-Weiss, H.; Gingold-Belfer, R.; Dickman, R.; Dotan, I. Correlation between Quantitative 13C-Urea Breath Test and Helicobacter pylori Treatment Success in a Population-Based Cohort. Gastroenterol. Res. Pract. 2018, 13, e5439539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, K.; Cho, M.-J.; Oh, J.-H.; Lim, C.-H. Second-Line Bismuth-Containing Quadruple Therapy for Helicobacter pylori Infection: A 12-Year Study of Annual Eradication Rates. J. Clin. Med. 2021, 10, 3273. [Google Scholar] [CrossRef]
- Liao, P.-H.; Lin, Y.-C.; Chu, C.-H.; Shih, S.-C.; Liou, T.-C. Colonization of Helicobacter pylori in the gastric cardia: A comparison between the UFT300 and CLO tests. JGH Open 2018, 2, 93–96. [Google Scholar] [CrossRef]
- Lee, S.-Y. Helicobacter pylori Infection and the Kyoto Classification of Gastritis. Korean J. Helicobacter Up. Gastrointest. Res. 2019, 19, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, M.; Furuta, T.; Shirai, N.; Kodaira, C.; Nishino, M.; Ikuma, M.; Ishizaki, T.; Hishida, A. Evidence that the degree and duration of acid suppression are related to Helicobacter pylori eradication by triple therapy. Helicobacter 2007, 12, 317–323. [Google Scholar] [CrossRef]
- Erah, P.O.; Goddard, A.F.; Barrett, D.A.; Shaw, P.N.; Spiller, R.C. The stability of amoxycillin, clarithromycin and metronidazole in gastric juice: Relevance to the treatment of Helicobacter pylori infection. J. Antimicrob. Chemother. 1997, 39, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Marcus, E.A.; Inatomi, N.; Nagami, G.T.; Sachs, G.; Scott, D.R. The effects of varying acidity on Helicobacter pylori growth and the bactericidal efficacy of ampicillin. Aliment. Pharmacol. Ther. 2012, 36, 972–979. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.; Sheng, W.-H.; Liou, J.-M.; Wang, H.-P.; Wu, M.-S.; Lin, J.-T.; Chang, S.-C. Comparative in vitro antimicrobial susceptibility and synergistic activity of antimicrobial combinations against Helicobacter pylori isolates in Taiwan. J. Microbiol. Immunol. Infect. 2015, 48, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Hassan, I.J.; Stark, R.M.; Greenman, J.; Millar, M.R. Activities of beta-lactams and macrolides against Helicobacter pylori. Antimicrob. Agents Chemother. 1999, 43, 1387–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 33613, Amoxicillin. 2021. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Amoxicillin (accessed on 12 December 2021).
- Tan, S.; Tompkins, L.S.; Amieva, M.R. Helicobacter pylori usurps cell polarity to turn the cell surface into a replicative niche. PLoS Pathog. 2009, 5, e1000407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 84029, Clarithromycin. 2021. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Clarithromycin (accessed on 12 December 2021).
- National Center for Biotechnology Information. PubChem Compound Summary for CID 4173, Metronidazole. 2021. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Metronidazole (accessed on 12 December 2021).
- Cao, X.; Bansil, R.; Bhaskar, K.R.; Turner, B.S.; Lamont, J.T.; Niu, N.; Afdhal, N.H. pH-dependent conformational change of gastric mucin leads to sol-gel transition. Biophys. J. 1999, 76, 1250–1258. [Google Scholar] [CrossRef] [Green Version]
- Celli, J.P.; Turner, B.S.; Afdhal, N.H.; Ewoldt, R.H.; McKinley, G.H.; Bansil, R.; Erramilli, S. Rheology of gastric mucin exhibits a pH-dependent sol-gel transition. Biomacromolecules 2007, 8, 1580–1586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, S.K.; Wang, Y.-Y.; Hanes, J. Mucus-penetrating nanoparticles for drug and gene delivery to mucosal tissues. Adv. Drug Deliv. Rev. 2009, 61, 158–171. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Factors | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value * | |
| Age (years) | 1.02 | 0.98, 1.07 | 0.282 | 1.03 | 0.97, 1.08 | 0.322 |
| Male (ref. Female) | 1.97 | 0.86, 4.49 | 0.107 | |||
| Body mass index | 1.15 | 1.03, 1.27 | 0.011 | 1.12 | 0.998, 1.27 | 0.055 |
| Serum HPIgG | 0.93 | 0.75, 1.16 | 0.534 | |||
| 13C-UBT (DOB) | 1.00 | 0.98, 1.03 | 0.689 | 1.00 | 0.98, 1.03 | 0.739 |
| Type 2 DM (ref. non-T2DM) | 1.24 | 0.45, 3.42 | 0.681 | 0.77 | 0.23, 2.63 | 0.680 |
| Dyslipidemia (ref. non-DL) | 1.29 | 0.50, 3.28 | 0.598 | |||
| eGFR | 0.99 | 0.97, 1.01 | 0.274 | |||
| Anemia (ref. non-Anemia) | 0.85 | 0.20, 3.62 | 0.827 | |||
| Smokers (ref. non-smokers) | 0.81 | 0.48, 1.39 | 0.450 | 1.14 | 0.61, 2.16 | 0.678 |
| Alcohol users | 0.76 | 0.39, 1.48 | 0.416 | |||
| Tea users | 0.88 | 0.68, 1.14 | 0.328 | |||
| Coffee users | 0.88 | 0.70, 1.12 | 0.307 | |||
| NSAID users | 0.73 | 0.28, 1.93 | 0.528 | |||
| Steroid users | 2.69 | 0.27, 26.8 | 0.400 | |||
| Statin users | 0.70 | 0.22, 2.28 | 0.559 | |||
| Gastric juice pH | 1.35 | 1.16, 1.58 | 0.0001 | 1.30 | 1.10, 1.54 | 0.002 |
| PUD (ref. non-PUD) | 0.59 | 0.24, 1.46 | 0.257 | 0.70 | 0.25, 1.96 | 0.495 |
| Carditis (ref. non-Carditis) | 1.54 | 0.68, 3.49 | 0.304 | |||
| Positive UFT300 of cardia | 1.95 | 0.66, 5.72 | 0.225 | |||
| Characteristics | Group A † | Group B † | Group C ‡ |
|---|---|---|---|
| (n = 60) | (n = 100) | (n = 134) | |
| Age (years, mean ± SD/range) * | 51.6 ± 11.7 (26–73) | 52.1 ± 10.3 (24–74) | 51.8 ± 11.5 (20–75) |
| Gender (M/F) * | 27/33 | 47/53 | 62/72 |
| NSAID ingestion * | 12 (20.0%) | 21 (21.0%) | 26 (19.4%) |
| Smoking * | 10 (16.7%) | 17 (17.0%) | 24 (17.9%) |
| Alcohol consumption * | 5 (8.3%) | 7 (7.0%) | 11 (8.2%) |
| Ingestion of tea * | 17 (28.3%) | 30 (30.0%) | 43 (32.1%) |
| Ingestion of coffee * | 25 (41.7%) | 39 (39.0%) | 52 (38.8%) |
| BMI (kg/m2, mean ± SD/range) * | 25.3 ± 4.6 | 25.9 ± 4.4 | 25.6 ± 4.5 |
| (17.7–39.8) | (17.5–36.5) | (17.4–38.5) | |
| Endoscopic Findings * | |||
| Normal | 10 (16.7%) | 15 (15.0%) | 18 (13.4%) |
| Gastritis | 50 (83.3%) | 85 (85.0%) | 116 (86.6%) |
| (antrum/corpus/cardia) | (23/41/32) | (39/66/57) | (54/84/74) |
| Peptic ulcer disease | 15 (25.0%) | 28 (28.0%) | 37 (27.6%) |
| Gastric Juice pH * | |||
| pH ≤ 3.5 | 27 (45.0%) | 46 (46.0%) | 62 (46.3%) |
| pH 4–5.5 | 4 (6.7%) | 9 (9.0%) | 13 (9.7%) |
| pH ≥ 6.0 | 29 (48.3%) | 45 (45.0%) | 59 (44.0%) |
| Medicaments | Patients Number (Lost to Follow Up) | Eradication Rate | Adverse Event |
|---|---|---|---|
| Mono-antibiotic | 60 (0) | 7/60 (11.7%) * | 1/60 (1.7%) ** |
| Amoxicillin | 20 | 2/20 (10%) | 0/20 (0%) |
| Clarithromycin | 20 | 1/20 (5%) | 0/20 (0%) |
| Metronidazole | 20 | 4/20 (20%) | 1/20 (5%) |
| Triple antibiotic | 100 (5) | 51/95 (53.7%) * | 6/100 (6%) ** |
| ILTHPI (Success No.) | Oral Antibiotic Therapy (No.) | Eradication Rate † (ITT = PP) | Overall Eradication Rate (ILTHPI Plus Oral Antibiotic Therapy) |
|---|---|---|---|
| Amoxicillin (2) | HDDT-14 (18) | 16/18 (88.9%) | 18/20 (90.0%) |
| Clarithromycin (1) | CTT-14 (19) | 18/19 (94.7%) | 19/20 (95.0%) |
| Metronidazole (4) | MTT-14 (16) | 12/16 (75.0%) | 16/20 (80.0%) |
| ILTHPI | Oral Antibiotic Therapy | Eradication Rate † (Failed ILTHPI) | ITT Eradication Rate (without ILTHPI) | PP Eradication Rate (without ILTHPI) |
|---|---|---|---|---|
| Amoxicillin | HDDT-14 * | 16/18 (88.9%) | 38/45 (84.4%) | 38/44 (86.4%) |
| Clarithromycin | CTT-14 * | 18/19 (94.7%) | 37/46 (80.4%) | 37/44 (84.1%) |
| Metronidazole | MTT-14 * | 12/16 (75.0%) | 31/43 (72.1%) | 31/42 (73.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, C.-Y.; Liu, T.-W.; Lin, Y.-S.; Chen, Y.-P.; Chen, M.-J.; Wang, H.-Y.; Liou, T.-C. Factors Affecting the Intraluminal Therapy for Helicobacter pylori Infection. Microorganisms 2022, 10, 415. https://doi.org/10.3390/microorganisms10020415
Ho C-Y, Liu T-W, Lin Y-S, Chen Y-P, Chen M-J, Wang H-Y, Liou T-C. Factors Affecting the Intraluminal Therapy for Helicobacter pylori Infection. Microorganisms. 2022; 10(2):415. https://doi.org/10.3390/microorganisms10020415
Chicago/Turabian StyleHo, Cheng-Yu, Ting-Wen Liu, Yang-Sheng Lin, Yen-Po Chen, Ming-Jen Chen, Horng-Yuan Wang, and Tai-Cherng Liou. 2022. "Factors Affecting the Intraluminal Therapy for Helicobacter pylori Infection" Microorganisms 10, no. 2: 415. https://doi.org/10.3390/microorganisms10020415