
Recent Trend of Antimicrobial Susceptibility among Mycoplasma pneumoniae Isolated from Japanese Children
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. M. pneumoniae Isolation
2.3. Antimicrobial Susceptibility Testing
2.4. Statistical Methods
3. Results
3.1. In Vitro Antimicrobial Activity
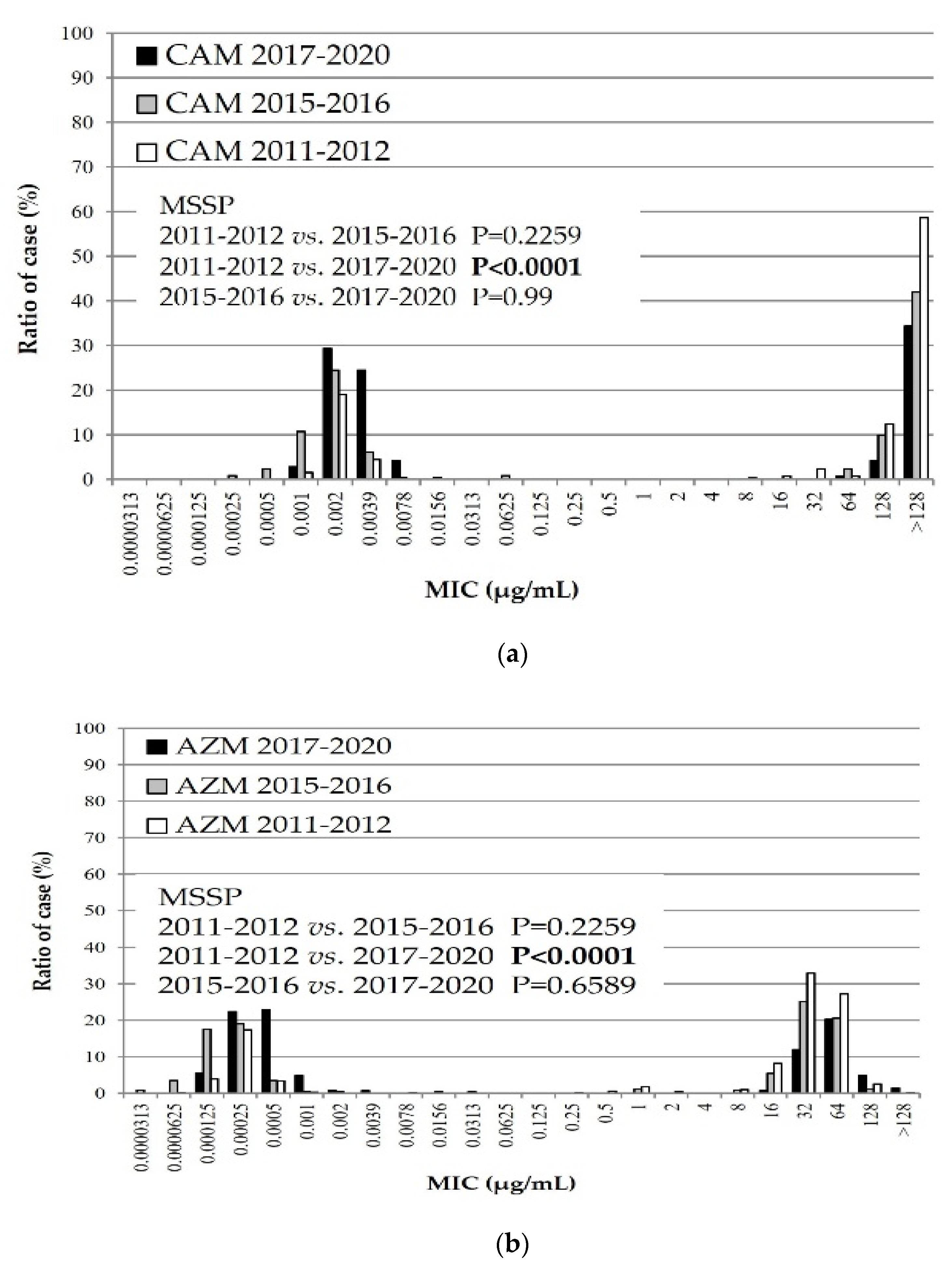
3.2. MIC Distribution of Macrolide Agents against M. pneumoniae Isolates during Three Time Periods
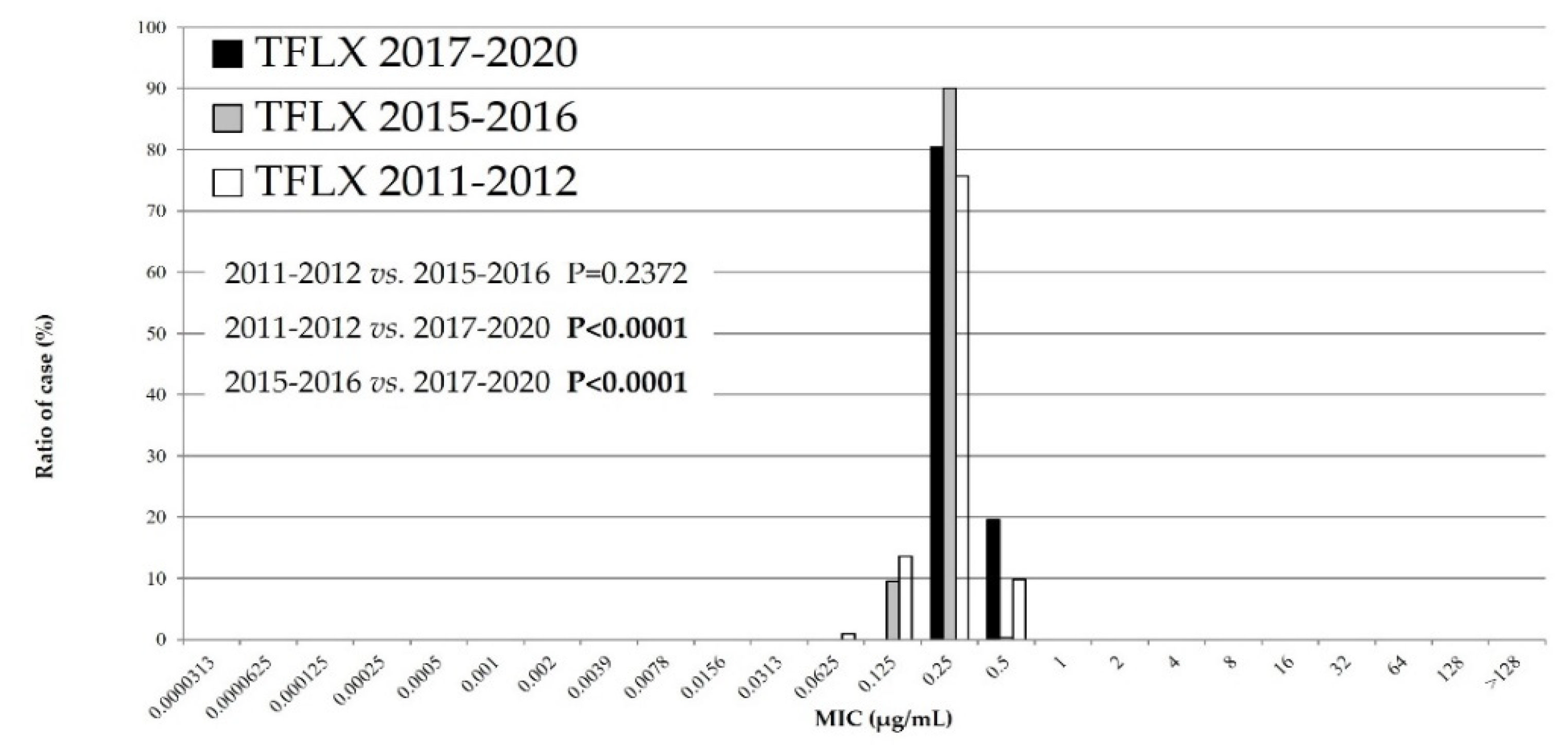
3.3. The MIC Distribution of TFLX against M. pneumoniae Isolates during Three Time Periods
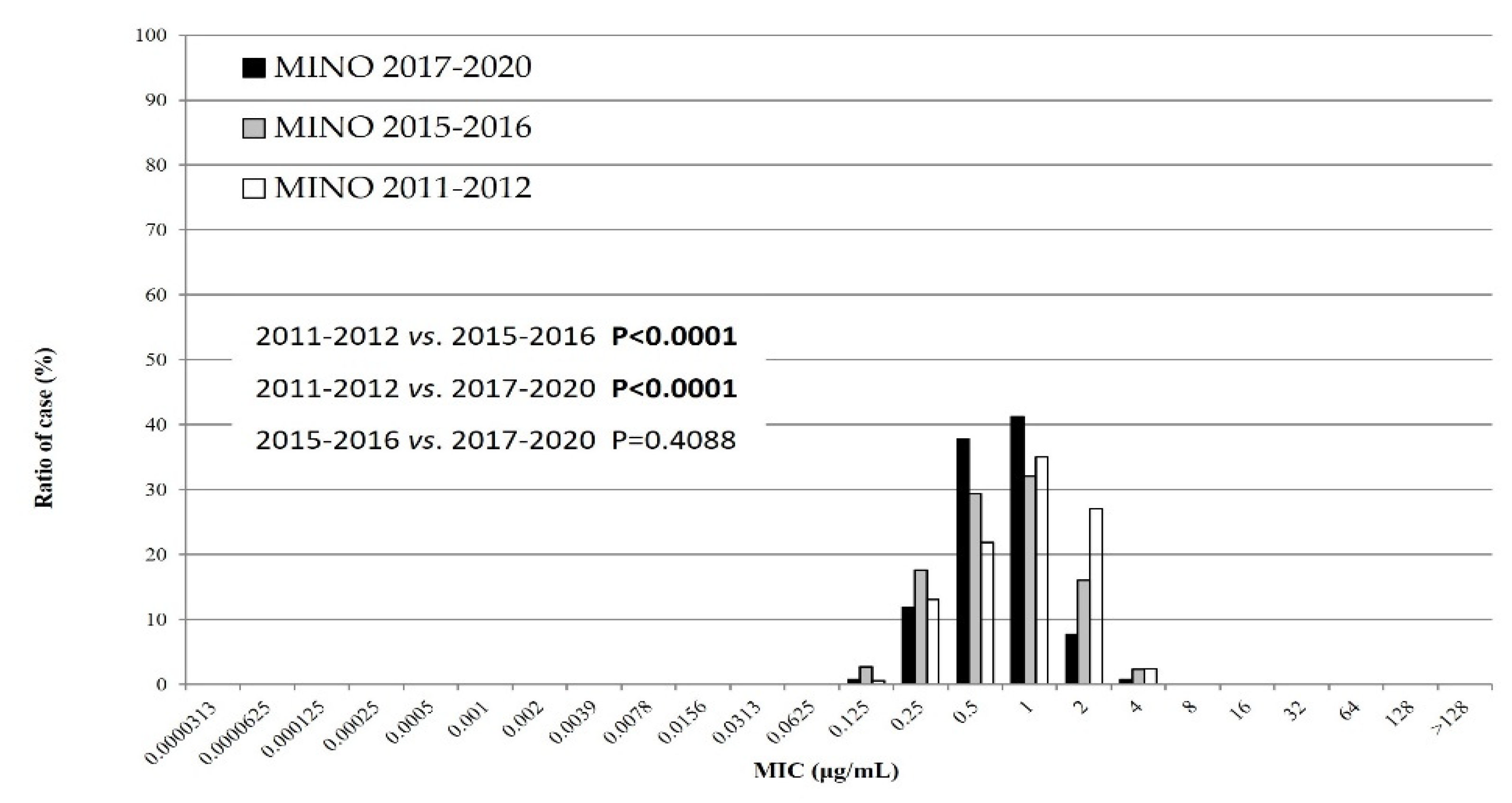
3.4. MIC Distribution of MINO against M. pneumoniae Isolates during Three Time Periods
4. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bradley, J.S.; Byington, C.L.; Shah, S.S.; Alverson, B.; Carter, E.R.; Harrison, C.; Kaplan, S.L.; Mace, S.E.; McCracken, G.H., Jr.; Moore, M.R.; et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: Clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2011, 53, 25–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.-H.; Tsai, C.-K.; Tsai, T.-A.; Wang, S.-C.; Lee, Y.-C.; Tsai, C.-M.; Liu, T.-Y.; Kuo, K.-C.; Chen, C.-C.; Yu, H.-R. Epidemiology and clinical manifestations of children with macrolide-resistant Mycoplasma pneumoniae pneumonia in Southern Taiwan. Pediatr. Neonatol. 2021, 62, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, N.; Namkoong, H.; Saito, F.; Ishizaki, M.; Yamazaki, M.; Mitamura, K. Epidemiology of macrolide-resistant Mycoplasma pneumoniae by age distribution in Japan. J. Infect. Chemother. 2020, 27, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Akashi, Y.; Hayashi, D.; Suzuki, H.; Shiigai, M.; Kanemoto, K.; Notake, S.; Ishiodori, T.; Ishikawa, H.; Imai, H. Clinical features, and seasonal variations in the prevalence of macrolide-resistant Mycoplasma pneumoniae. J. Gen. Fam. Med. 2018, 19, 191–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, E.D.; Welsh, C.H. Fulminant Mycoplasma pneumoniae pneumonia. West. J. Med. 1995, 162, 133–142. [Google Scholar]
- Lanatai, M.M.; Wang, H.; Everhart Moore-Clingenpeel, M.; Ramilo, O.; Leber, A. Macrolide-Resistant Mycoplasma pneumoniae Infections in Children, Ohio, USA. Emerg. Infect. Dis. 2021, 27, 1588–1597. [Google Scholar] [CrossRef]
- Xiao, L.; Ratliff, A.E.; Crabb, D.M.; Mixon, E.; Qin, X.; Selvarangan, R.; Tang, Y.-W.; Zheng, X.; Bard, J.D.; Hong, T.; et al. Molecular Characterization of Mycoplasma pneumoniae Isolates in the United States from 2012 to 2018. J. Clin. Microbiol. 2020, 58, e00710-20. [Google Scholar] [CrossRef]
- Hung, H.-M.; Chuang, C.-H.; Chen, Y.-Y.; Liao, W.-C.; Li, S.-W.; Chang, I.Y.-F.; Chen, C.-H.; Li, T.-H.; Huang, Y.-Y.; Huang, Y.-C.; et al. Clonal spread of macrolide-resistant Mycoplasma pneumoniae sequence type-3 and type-17 with recombination on non-P1 adhesin among children in Taiwan. Clin. Microbiol. Infect. 2020, 27, 1169.e1–1169.e6. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, J.; Chen, W.; Shen, N.; Tao, Y.; Zhao, R.; Luo, L.; Li, B.; Cao, Q. Impact of viral coinfection and macrolide-resistant mycoplasma infection in children with refractory Mycoplasma pneumoniae pneumonia. BMC Infect. Dis. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Lee, J.K.; Choi, Y.Y.; Sohn, Y.J.; Kim, K.-M.; Kim, Y.K.; Han, M.S.; Park, J.Y.; Cho, E.Y.; Choi, J.H.; Choi, E.H. Persistent high macrolide resistance rate and increase of macrolide-resistant ST14 strains among Mycoplasma pneumoniae in South Korea, 2019–2020. J. Microbiol. Immunol. Infect. 2021, 55, 910–916. [Google Scholar] [CrossRef]
- Morozumi, M.; Tajima, T.; Sakuma, M.; Shouji, M.; Meguro, H.; Saito, K.; Iwata, S.; Ubukata, K. Sequence Type Changes Associated with Decreasing Macrolide-Resistant Mycoplasma pneumoniae, Japan. Emerg. Infect. Dis. 2020, 26, 2210–2213. [Google Scholar] [CrossRef]
- Nakamura, Y.; Oishi, T.; Kaneko, K.; Kenri, T.; Tanaka, T.; Wakabayashi, S.; Kono, M.; Ono, S.; Kato, A.; Kondo, E.; et al. Recent acute reduction in macrolide-resistant Mycoplasma pneumoniae infections among Japanese children. J. Infect. Chemother. 2020, 27, 271–276. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, J.; Lu, Z.; Chen, Y.; Huang, S.; Li, H.; Lin, S.; Yu, J.; Zeng, X.; Ji, C.; et al. Mycoplasma pneumoniae among Chinese Outpatient Children with Mild Respiratory Tract Infections during the Coronavirus Disease 2019 Pandemic. Microbiol. Spectr. 2022, 10, e0155021. [Google Scholar] [CrossRef] [PubMed]
- Rivaya, B.; Lluch, E.J.; Rivas, G.F.; Molinos, S.; Campos, R.; Hernández, M.M.; Matas, L. Macrolide resistance and molecular typing of Mycoplasma pneumoniae infections during a 4-year period in Spain. J. Antimicrob. Chemother. 2020, 75, 2752–2759. [Google Scholar] [CrossRef] [PubMed]
- Morozumi, M.; Takahashi, T.; Ubukata, K. Macrolide-resistant Mycoplasma pneumoniae: Characteristics of isolates and clinical aspects of community-acquired pneumonia. J. Infect. Chemother. 2010, 16, 78–86. [Google Scholar] [CrossRef]
- Miyashita, N.; Kawai, Y.; Yamaguchi, T.; Ouchi, K.; Oka, M.; Atypical Pathogen Study Group. Clinical potential of diagnostic methods for the rapid diagnosis of Mycoplasma pneumoniae pneumonia in adults. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 30, 439–446. [Google Scholar] [CrossRef]
- Waites, K.B.; Crabb, D.M.; Bing, X.; Duffy, L.B. In Vitro Susceptibilities to and Bactericidal Activities of Garenoxacin (BMS-284756) and Other Antimicrobial Agents against Human Mycoplasmas and Ureaplasmas. Antimicrob. Agents Chemother. 2003, 47, 161–165. [Google Scholar] [CrossRef] [Green Version]
- Committee of the Japanese Society of Mycoplasmology. Guiding Principles * for Treating Mycoplasma Pneumoniae Pneumonia; Japanese Society of Mycoplasmology: Tokyo, Japan, 2014; Available online: http://square.umin.ac.jp/jsm/Eng%20shisin.pdf (accessed on 13 November 2022).
- Okubo, Y.; Michihata, N.; Morisaki, N.; Uda, K.; Miyairi, I.; Ogawa, Y.; Matsui, H.; Fushimi, K.; Yasunaga, H. Recent trends in practice patterns and impact of corticosteroid use on pediatric Mycoplasma pneumoniae -related respiratory infections. Respir. Investig. 2017, 56, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Morinaga, Y.; Suzuki, H.; Notake, S.; Mizusaka, T.; Uemura, K.; Otomo, S.; Oi, Y.; Ushiki, A.; Kawabata, N.; Kameyama, K.; et al. Evaluation of GENECUBE Mycoplasma for the detection of macrolide-resistant Mycoplasma pneumoniae. J. Med. Microbiol. 2020, 69, 1346–1350. [Google Scholar] [CrossRef]
- Kakiuchi, T.; Miyata, I.; Kimura, R.; Shimomura, G.; Shimomura, K.; Yamaguchi, S.; Yokoyama, T.; Ouchi, K.; Matsuo, M. Clinical Evaluation of a Novel Point-of-Care Assay To Detect Mycoplasma pneumoniae and Associated Macrolide-Resistant Mutations. J. Clin. Microbiol. 2021, 59, e0324520. [Google Scholar] [CrossRef]
- Ouchi, K.; Takayama, S.; Fujioka, Y.; Sunakawa, K.; Iwata, S. A phase III, randomized, open-label study on 15% tosufloxacin granules in pediatric Mycoplasma pneumoniae pneumonia. Jpn. J. Chemother. 2017, 65, 585–596. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Organism (Number of Strains) (n = 122) | Antimicrobial Agents | MIC (μg/mL) | ||||
|---|---|---|---|---|---|---|
| MIC Range | MIC50 | MIC90 | ||||
| Mycoplasma pneumoniae (122) | CAM | 0.001 | – | >128 | 0.0039 | >128 |
| AZM | 0.00012 | >128 | 0.0005 | 64 | ||
| TFLX | 0.25 | – | 0.5 | 0.25 | 0.5 | |
| MINO | 0.125 | – | 4 | 0.5 | 1 | |
| Macrolide-susceptible M. pneumoniae (76) | CAM | 0.0078 | – | 0.001 | 0.002 | 0.0039 |
| AZM | 0.00012 | 0.0039 | 0.0005 | 0.001 | ||
| TFLX | 0.25 | – | 0.5 | 0.25 | 0.5 | |
| MINO | 0.25 | – | 4 | 1 | 1 | |
| Macrolide-resistant M. pneumoniae (46) | CAM | 16 | – | >128 | >128 | >128 |
| AZM | 64 | >128 | 64 | 128 | ||
| TFLX | 0.25 | – | 0.5 | 0.25 | 0.25 | |
| MINO | 0.125 | – | 2 | 0.5 | 2 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oishi, T.; Yoshioka, D.; Nakano, T.; Ouchi, K. Recent Trend of Antimicrobial Susceptibility among Mycoplasma pneumoniae Isolated from Japanese Children. Microorganisms 2022, 10, 2428. https://doi.org/10.3390/microorganisms10122428
Oishi T, Yoshioka D, Nakano T, Ouchi K. Recent Trend of Antimicrobial Susceptibility among Mycoplasma pneumoniae Isolated from Japanese Children. Microorganisms. 2022; 10(12):2428. https://doi.org/10.3390/microorganisms10122428
Chicago/Turabian StyleOishi, Tomohiro, Daisuke Yoshioka, Takashi Nakano, and Kazunobu Ouchi. 2022. "Recent Trend of Antimicrobial Susceptibility among Mycoplasma pneumoniae Isolated from Japanese Children" Microorganisms 10, no. 12: 2428. https://doi.org/10.3390/microorganisms10122428