
Plasma Gut Microbe-Derived Metabolites Associated with Peripheral Artery Disease and Major Adverse Cardiac Events
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Variables
2.3. Endpoints
2.4. Detection and Quantification of Metabolites by High-Performance Liquid Chromatography–Tandem Mass Spectrometry (LC-MS/MS)
2.5. Statistical Analysis
3. Results
3.1. Study Population
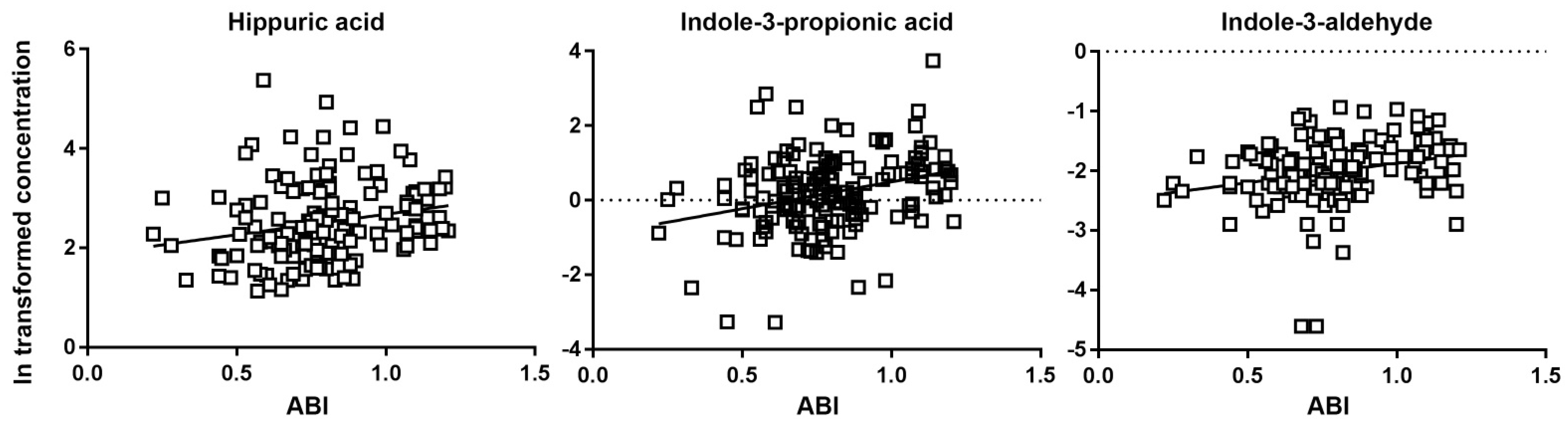
3.2. Correlation between Metabolites and ABI
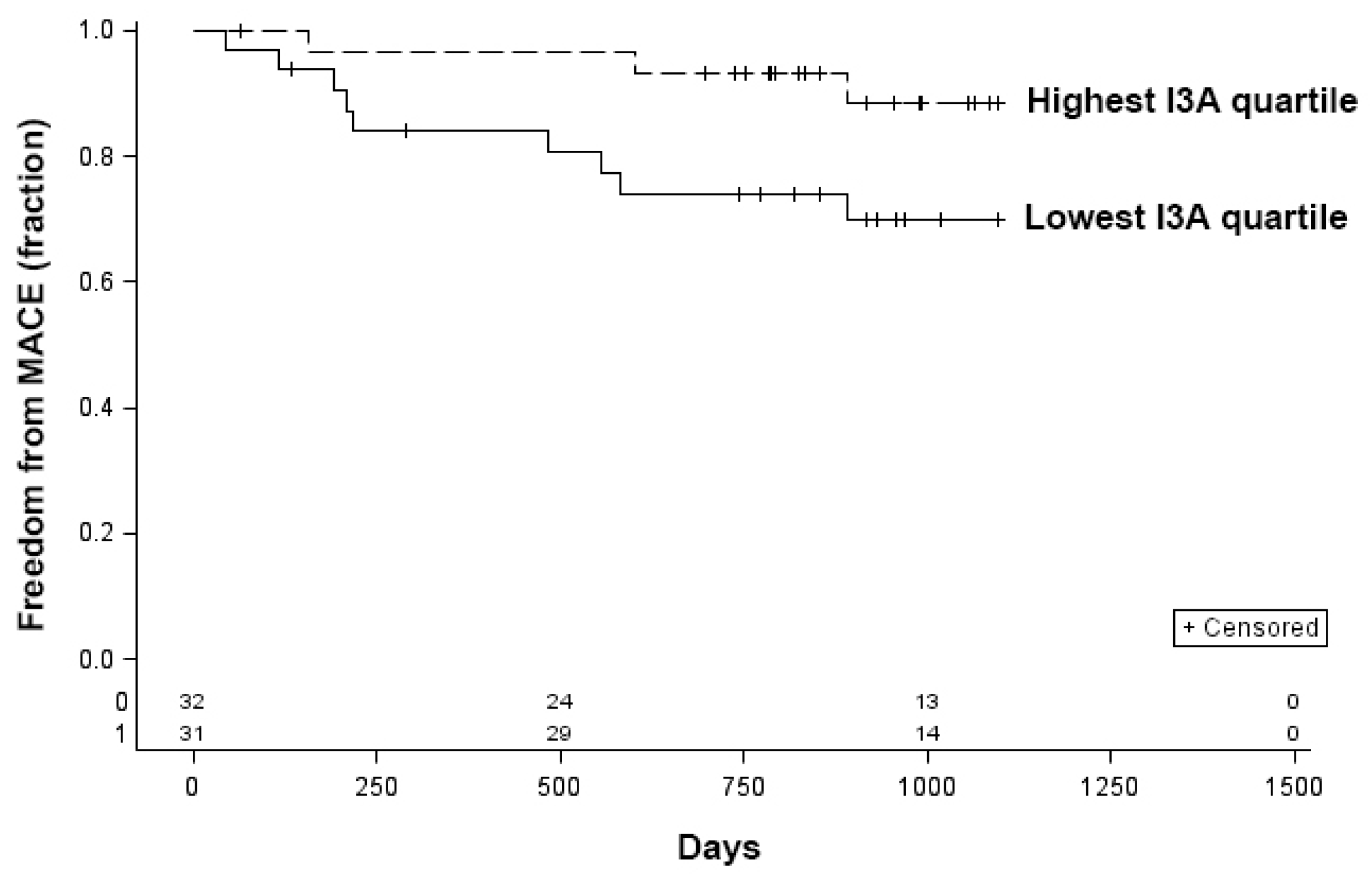
3.3. Relationship between Metabolites and MACE
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Stepankova, R.; Tonar, Z.; Bartova, J.; Nedorost, L.; Rossman, P.; Poledne, R.; Schwarzer, M.; Tlaskalova-Hogenova, H. Absence of Microbiota (Germ-Free Conditions) Accelerates the Atherosclerosis in ApoE-Deficient Mice Fed Standard Low Cholesterol Diet. J. Atheroscler. Thromb. 2010, 17, 796–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasahara, K.; Krautkramer, K.A.; Org, E.; Romano, K.A.; Kerby, R.L.; Vivas, E.I.; Mehrabian, M.; Denu, J.M.; Bäckhed, F.; Lusis, A.J.; et al. Interactions between Roseburia intestinalis and diet modulate atherogenesis in a murine model. Nat. Microbiol. 2018, 3, 1461–1471. [Google Scholar] [CrossRef]
- Tang, W.W.; Wang, Z.; Fan, Y.; Levison, B.; Hazen, J.E.; Donahue, L.M.; Wu, Y.; Hazen, S.L. Prognostic value of elevated levels of intestinal microbe-generated metabolite trimethylamine-N-oxide in patients with heart failure: Refining the gut hypothesis. J. Am. Coll. Cardiol. 2014, 64, 1908–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, W.H.W.; Wang, Z.; Levison, B.S.; Koeth, R.A.; Britt, E.B.; Fu, X.; Wu, Y.; Hazen, S.L. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N. Engl. J. Med. 2013, 368, 1575–1584. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; DuGar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.-M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senthong, V.; Wang, Z.; Fan, Y.; Wu, Y.; Hazen, S.L.; Tang, W.H.W. Trimethylamine N-Oxide and Mortality Risk in Patients With Peripheral Artery Disease. J. Am. Heart Assoc. 2016, 5, e004237. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, F.; Fåk, F.; Nookaew, I.; Tremaroli, V.; Fagerberg, B.; Petranovic, D.; Bäckhed, F.; Nielsen, J. Symptomatic atherosclerosis is associated with an altered gut metagenome. Nat. Commun. 2012, 3, 1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Q.; Gao, R.; Zhang, Y.; Pan, D.; Zhu, Y.; Zhang, X.; Yang, R.; Jiang, R.; Xu, Y.; Qin, H. Dysbiosis signatures of gut microbiota in coronary artery disease. Physiol. Genom. 2018, 50, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Chen, X.; Hu, X.; Niu, H.; Tian, R.; Wang, H.; Pang, H.; Jiang, L.; Qiu, B.; Chen, X.; et al. Alterations in the gut microbiome and metabolism with coronary artery disease severity. Microbiome 2019, 7, 68. [Google Scholar] [CrossRef] [Green Version]
- Tian, R.; Liu, H.; Feng, S.; Wang, H.; Wang, Y.; Wang, Y.; Liang, L.; Xu, H.; Xing, H.; Zhang, S. Gut microbiota dysbiosis in stable coronary artery disease combined with type 2 diabetes mellitus influences cardiovascular prognosis. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1454–1466. [Google Scholar] [CrossRef]
- Li, J.; Zhao, F.; Wang, Y.; Chen, J.; Tao, J.; Tian, G.; Wu, S.; Liu, W.; Cui, Q.; Geng, B.; et al. Gut microbiota dysbiosis contributes to the development of hypertension. Microbiome 2017, 5, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dan, X.; Mushi, Z.; Baili, W.; Han, L.; Enqi, W.; Huanhu, Z.; Shuchun, L. Differential Analysis of Hypertension-Associated Intestinal Microbiota. Int. J. Med. Sci. 2019, 16, 872–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.; Lulla, A.; Sioda, M.; Winglee, K.; Wu, M.C.; Jacobs, D.R., Jr.; Shikany, J.M.; Lloyd-Jones, D.M.; Launer, L.J.; Fodor, A.A.; et al. Gut Microbiota Composition and Blood Pressure. Hypertension 2019, 73, 998–1006. [Google Scholar] [CrossRef]
- Benakis, C.; Brea, D.; Caballero, S.; Faraco, G.; Moore, J.; Murphy, M.; Sita, G.; Racchumi, G.; Ling, L.; Pamer, E.G.; et al. Commensal microbiota affects ischemic stroke outcome by regulating intestinal gammadelta T cells. Nat. Med. 2016, 22, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Roth, S.; Llovera, G.; Sadler, R.; Garzetti, D.; Stecher, B.; Dichgans, M.; Liesz, A. Microbiota Dysbiosis Controls the Neuroinflammatory Response after Stroke. J. Neurosci. 2016, 36, 7428–7440. [Google Scholar] [CrossRef] [Green Version]
- Xia, G.-H.; You, C.; Gao, X.-X.; Zeng, X.-L.; Zhu, J.-J.; Xu, K.-Y.; Tan, C.-H.; Xu, R.-T.; Wu, Q.-H.; Zhou, H.-W.; et al. Stroke Dysbiosis Index (SDI) in Gut Microbiome Are Associated With Brain Injury and Prognosis of Stroke. Front. Neurol. 2019, 10, 397. [Google Scholar] [CrossRef]
- Xu, K.; Gao, X.; Xia, G.; Chen, M.; Zeng, N.; Wang, S.; You, C.; Tian, X.; Di, H.; Tang, W.; et al. Rapid gut dysbiosis induced by stroke exacerbates brain infarction in turn. Gut 2021, 70, 1486–1494. [Google Scholar] [CrossRef]
- Sun, W.; Du, D.; Fu, T.; Han, Y.; Li, P.; Ju, H. Alterations of the Gut Microbiota in Patients With Severe Chronic Heart Failure. Front. Microbiol. 2021, 12, 813289. [Google Scholar] [CrossRef]
- Organ, C.L.; Otsuka, H.; Bhushan, S.; Wang, Z.; Bradley, J.; Trivedi, R.; Polhemus, D.J.; Tang, W.W.; Wu, Y.; Hazen, S.L.; et al. Choline Diet and Its Gut Microbe-Derived Metabolite, Trimethylamine N-Oxide, Exacerbate Pressure Overload-Induced Heart Failure. Circ. Heart Fail. 2016, 9, e002314. [Google Scholar] [CrossRef] [Green Version]
- Cui, X.; Ye, L.; Li, J.; Jin, L.; Wang, W.; Li, S.; Bao, M.; Wu, S.; Li, L.; Geng, B.; et al. Metagenomic and metabolomic analyses unveil dysbiosis of gut microbiota in chronic heart failure patients. Sci. Rep. 2018, 8, 635. [Google Scholar] [CrossRef]
- Nicholson, J.K.; Holmes, E.; Wilson, I.D. Gut microorganisms, mammalian metabolism and personalized health care. Nat. Rev. Microbiol. 2005, 3, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Wikoff, W.R.; Anfora, A.T.; Liu, J.; Schultz, P.G.; Lesley, S.A.; Peters, E.C.; Siuzdak, G. Metabolomics analysis reveals large effects of gut microflora on mammalian blood metabolites. Proc. Natl. Acad. Sci. USA 2009, 106, 3698–3703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cason, C.A.; Dolan, K.T.; Sharma, G.; Tao, M.; Kulkarni, R.; Helenowski, I.B.; Doane, B.M.; Avram, M.J.; McDermott, M.M.; Chang, E.B.; et al. Plasma microbiome-modulated indole- and phenyl-derived metabolites associate with advanced atherosclerosis and postoperative outcomes. J. Vasc. Surg. 2017, 65, 1552–1562. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, R.B.; Baker, J.; Ernst, C.; Johnston, K.; Porter, J.M.; Ahn, S.; Jones, D.N. Recommended standards for reports dealing with lower extremity ischemia: Revised version. J. Vasc. Surg. 1997, 26, 517–538. [Google Scholar] [CrossRef] [Green Version]
- Grenon, S.M.; Owens, C.D.; Nosova, E.V.; Hughes-Fulford, M.; Alley, H.F.; Chong, K.; Perez, S.; Yen, P.K.; Boscardin, J.; Hellmann, J.; et al. Short-Term, High-Dose Fish Oil Supplementation Increases the Production of Omega-3 Fatty Acid-Derived Mediators in Patients with Peripheral Artery Disease (the OMEGA-PAD I Trial). J. Am. Heart Assoc. 2015, 4, e002034. [Google Scholar] [CrossRef] [Green Version]
- Grenon, S.M.; Owens, C.D.; Alley, H.; Chong, K.; Yen, P.K.; Harris, W.; Hughes-Fulford, M.; Conte, M.S. n-3 Polyunsaturated fatty acids supplementation in peripheral artery disease: The OMEGA-PAD trial. Vasc. Med. 2013, 18, 263–274. [Google Scholar] [CrossRef]
- Schaller, M.S.; Ramirez, J.L.; Gasper, W.J.; Zahner, G.J.; Hills, N.K.; Grenon, S.M. Frailty is Associated with an Increased Risk of Major Adverse Cardiac Events in Patients with Stable Claudication. Ann. Vasc. Surg. 2018, 50, 38–45. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Drudi, L.M.; Schaller, M.S.; Hiramoto, J.; Gasper, W.; Harris, W.S.; Hills, N.K.; Grenon, S.M. Predictors of change in omega-3 index with fish oil supplementation in peripheral artery disease. J. Surg. Res. 2017, 210, 124–131. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.S.; Pottala, J.V.; Lacey, S.M.; Vasan, R.S.; Larson, M.G.; Robins, S.J. Clinical correlates and heritability of erythrocyte eicosapentaenoic and docosahexaenoic acid content in the Framingham Heart Study. Atherosclerosis 2012, 225, 425–431. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; White, H.D.; Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. J. Am. Coll. Cardiol. 2007, 50, 2173–2195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, T.W.; Darlington, L.G. Endogenous kynurenines as targets for drug discovery and development. Nat. Rev. Drug Discov. 2002, 1, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Fabsitz, R.R.; Sidawy, A.N.; Go, O.; Lee, E.T.; Welty, T.K.; Devereux, R.B.; Howard, B.V. Prevalence of peripheral arterial disease and associated risk factors in American Indians: The Strong Heart Study. Am. J. Epidemiol. 1999, 149, 330–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curb, J.D.; Masaki, K.; Rodriguez, B.L.; Abbott, R.D.; Burchfiel, C.M.; Chen, R.; Petrovitch, H.; Sharp, D.; Yano, K. Peripheral artery disease and cardiovascular risk factors in the elderly. The Honolulu Heart Program. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 1495–1500. [Google Scholar] [CrossRef]
- Murabito, J.M.; Evans, J.C.; Larson, M.G.; Nieto, K.; Levy, D.; Wilson, P.W.F. The ankle-brachial index in the elderly and risk of stroke, coronary disease, and death: The Framingham Study. Arch. Intern. Med. 2003, 163, 1939–1942. [Google Scholar] [CrossRef] [Green Version]
- Newman, A.B.; Shemanski, L.; Manolio, T.A.; Cushman, M.; Mittelmark, M.; Polak, J.F.; Powe, N.R.; Siscovick, D. Ankle-arm index as a predictor of cardiovascular disease and mortality in the Cardiovascular Health Study. The Cardiovascular Health Study Group. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 538–545. [Google Scholar] [CrossRef] [Green Version]
- Vogt, M.T.; Cauley, J.A.; Newman, A.B.; Kuller, L.H.; Hulley, S.B. Decreased ankle/arm blood pressure index and mortality in elderly women. JAMA 1993, 270, 465–469. [Google Scholar] [CrossRef]
- Vogt, M.T.; McKenna, M.; Anderson, S.J.; Wolfson, S.K.; Kuller, L.H. The relationship between ankle-arm index and mortality in older men and women. J. Am. Geriatr. Soc. 1993, 41, 523–530. [Google Scholar] [CrossRef]
- McDermott, M.M.; Ferrucci, L.; Simonsick, E.M.; Balfour, J.; Fried, L.; Ling, S.; Gibson, D.; Guralnik, J.M. The ankle brachial index and change in lower extremity functioning over time: The Women’s Health and Aging Study. J. Am. Geriatr. Soc. 2002, 50, 238–246. [Google Scholar] [CrossRef]
- Criqui, M.H.; Langer, R.D.; Fronek, A.; Feigelson, H.S.; Klauber, M.R.; McCann, T.J.; Browner, D. Mortality over a period of 10 years in patients with peripheral arterial disease. N. Engl. J. Med. 1992, 326, 381–386. [Google Scholar] [CrossRef]
- McDermott, M.M.; Liu, K.; Criqui, M.H.; Ruth, K.; Goff, D.; Saad, M.F.; Wu, C.; Homma, S.; Sharrett, A.R. Ankle-brachial index and subclinical cardiac and carotid disease: The multi-ethnic study of atherosclerosis. Am. J. Epidemiol. 2005, 162, 33–41. [Google Scholar] [CrossRef]
- Diehm, C.; Schuster, A.; Allenberg, J.R.; Darius, H.; Haberl, R.; Lange, S.; Pittrow, D.; von Stritzky, B.; Tepohl, G.; Trampisch, H.-J. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: Cross-sectional study. Atherosclerosis 2004, 172, 95–105. [Google Scholar] [CrossRef]
- Leng, G.C.; Lee, A.J.; Fowkers, F.G.R.; Whiteman, M.; Dunbar, J.; Housley, E.; Ruckley, C.V. Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. Int. J. Epidemiol. 1996, 25, 1172–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leng, G.C.; Fowkes, F.G.R.; Lee, A.J.; Dunbar, J.; Housley, E.; Ruckley, C.V. Use of ankle brachial pressure index to predict cardiovascular events and death: A cohort study. BMJ 1996, 313, 1440–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDermott, M.M.; Feinglass, J.; Slavensky, R.; Pearce, W.H. The ankle-brachial index as a predictor of survival in patients with peripheral vascular disease. J. Gen. Intern. Med. 1994, 9, 445–449. [Google Scholar] [CrossRef] [PubMed]
- McKenna, M.; Wolfson, S.; Kuller, L. The ratio of ankle and arm arterial pressure as an independent predictor of mortality. Atherosclerosis 1991, 87, 119–128. [Google Scholar] [CrossRef]
- Paeslack, N.; Mimmler, M.; Becker, S.; Gao, Z.; Khuu, M.P.; Mann, A.; Malinarich, F.; Regen, T.; Reinhardt, C. Microbiota-derived tryptophan metabolites in vascular inflammation and cardiovascular disease. Amino Acids 2022, 1–18. [Google Scholar] [CrossRef]
- Wang, X.; Fang, X.; Zhou, J.; Chen, Z.; Zhao, B.; Xiao, L.; Liu, A.; Li, Y.-S.J.; Shyy, J.Y.-J.; Guan, Y.; et al. Shear stress activation of nuclear receptor PXR in endothelial detoxification. Proc. Natl. Acad. Sci. USA 2013, 110, 13174–13179. [Google Scholar] [CrossRef] [Green Version]
- Hagedorn, K.A.; Cooke, C.L.; Falck, J.R.; Mitchell, B.F.; Davidge, S.T. Regulation of vascular tone during pregnancy: A novel role for the pregnane X receptor. Hypertension 2007, 49, 328–333. [Google Scholar] [CrossRef] [Green Version]
- Venu, V.K.P.; Saifeddine, M.; Mihara, K.; Tsai, Y.C.; Nieves, K.; Alston, L.; Mani, S.; McCoy, K.D.; Hollenberg, M.D.; Hirota, S.A. The pregnane X receptor and its microbiota-derived ligand indole 3-propionic acid regulate endothelium-dependent vasodilation. Am. J. Physiol. Endocrinol. Metab. 2019, 317, E350–E361. [Google Scholar] [CrossRef]
- de Mello, V.D.; Paananen, J.; Lindström, J.; Lankinen, M.A.; Shi, L.; Kuusisto, J.; Pihlajamäki, J.; Auriola, S.; Lehtonen, M.; Rolandsson, O.; et al. Indolepropionic acid and novel lipid metabolites are associated with a lower risk of type 2 diabetes in the Finnish Diabetes Prevention Study. Sci. Rep. 2017, 7, 46337. [Google Scholar] [CrossRef] [Green Version]
- Tuomainen, M.; Lindström, J.; Lehtonen, M.; Auriola, S.; Pihlajamäki, J.; Peltonen, M.; Tuomilehto, J.; Uusitupa, M.; De Mello, V.D.; Hanhineva, K. Associations of serum indolepropionic acid, a gut microbiota metabolite, with type 2 diabetes and low-grade inflammation in high-risk individuals. Nutr. Diabetes 2018, 8, 35. [Google Scholar] [CrossRef] [Green Version]
- Xue, H.; Chen, X.; Yu, C.; Deng, Y.; Zhang, Y.; Chen, S.; Chen, X.; Chen, K.; Yang, Y.; Ling, W. Gut Microbially Produced Indole-3-Propionic Acid Inhibits Atherosclerosis by Promoting Reverse Cholesterol Transport and Its Deficiency Is Causally Related to Atherosclerotic Cardiovascular Disease. Circ. Res. 2022, 131, 404–420. [Google Scholar] [CrossRef]
- Shivanna, S.; Kolandaivelu, K.; Shashar, M.; Belghasim, M.; Al-Rabadi, L.; Balcells, M.; Zhang, A.; Weinberg, J.; Francis, J.; Pollastri, M.; et al. The Aryl Hydrocarbon Receptor is a Critical Regulator of Tissue Factor Stability and an Antithrombotic Target in Uremia. J. Am. Soc. Nephrol. 2016, 27, 189–201. [Google Scholar] [CrossRef] [Green Version]
- Chitalia, V.C.; Shivanna, S.; Martorell, J.; Balcells, M.; Bosch, I.; Kolandaivelu, K.; Edelman, E. Uremic serum and solutes increase post-vascular interventional thrombotic risk through altered stability of smooth muscle cell tissue factor. Circulation 2013, 127, 365–376. [Google Scholar] [CrossRef]
- Tanaka, S.; Watanabe, H.; Nakano, T.; Imafuku, T.; Kato, H.; Tokumaru, K.; Arimura, N.; Enoki, Y.; Maeda, H.; Tanaka, M.; et al. Indoxyl Sulfate Contributes to Adipose Tissue Inflammation through the Activation of NADPH Oxidase. Toxins 2020, 12, 502. [Google Scholar] [CrossRef]
- Barreto, F.C.; Barreto, D.V.; Liabeuf, S.; Meert, N.; Glorieux, G.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A.; European Uremic Toxin Work Group (EUTox). Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1551–1558. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.-Y.; Chou, H.-H.; Huang, H.-L.; Hung, S.-C. Indoxyl Sulfate and Incident Peripheral Artery Disease in Hemodialysis Patients. Toxins 2020, 12, 696. [Google Scholar] [CrossRef]
- Zelante, T.; Iannitti, R.G.; Cunha, C.; De Luca, A.; Giovannini, G.; Pieraccini, G.; Zecchi, R.; D’Angelo, C.; Massi-Benedetti, C.; Fallarino, F.; et al. Tryptophan catabolites from microbiota engage aryl hydrocarbon receptor and balance mucosal reactivity via interleukin-22. Immunity 2013, 39, 372–385. [Google Scholar] [CrossRef] [Green Version]
- Alexeev, E.E.; Lanis, J.M.; Kao, D.J.; Campbell, E.L.; Kelly, C.J.; Battista, K.D.; Gerich, M.E.; Jenkins, B.R.; Walk, S.T.; Kominsky, D.J.; et al. Microbiota-Derived Indole Metabolites Promote Human and Murine Intestinal Homeostasis through Regulation of Interleukin-10 Receptor. Am. J. Pathol. 2018, 188, 1183–1194. [Google Scholar] [CrossRef]
- Swimm, A.; Giver, C.R.; DeFilipp, Z.; Rangaraju, S.; Sharma, A.; Antonova, A.U.; Sonowal, R.; Capaldo, C.; Powell, D.; Qayed, M.; et al. Indoles derived from intestinal microbiota act via type I interferon signaling to limit graft-versus-host disease. Blood 2018, 132, 2506–2519. [Google Scholar] [CrossRef] [Green Version]
- Langan, D.; Perkins, D.; Vogel, S.; Moudgil, K. Microbiota-Derived Metabolites, Indole-3-aldehyde and Indole-3-acetic Acid, Differentially Modulate Innate Cytokines and Stromal Remodeling Processes Associated with Autoimmune Arthritis. Int. J. Mol. Sci. 2021, 22, 2017. [Google Scholar] [CrossRef]
- Yoshida, R.; Imanishi, J.; Oku, T.; Kishida, T.; Hayaishi, O. Induction of pulmonary indoleamine 2,3-dioxygenase by interferon. Proc. Natl. Acad. Sci. USA 1981, 78, 129–132. [Google Scholar] [CrossRef] [Green Version]
- Munn, D.H.; Mellor, A.L. Indoleamine 2,3 dioxygenase and metabolic control of immune responses. Trends Immunol. 2013, 34, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, E.R.; Tuseth, N.; Eussen, S.J.; Ueland, P.M.; Strand, E.; Svingen, G.F.T.; Midttun, Ø.; Meyer, K.; Mellgren, G.; Ulvik, A.; et al. Associations of plasma kynurenines with risk of acute myocardial infarction in patients with stable angina pectoris. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Berg, M.; Polyzos, K.A.; Agardh, H.; Baumgartner, R.; Forteza, M.J.; Kareinen, I.; Gisterå, A.; Bottcher, G.; Hurt-Camejo, E.; Hansson, G.K.; et al. 3-Hydroxyanthralinic acid metabolism controls the hepatic SREBP/lipoprotein axis, inhibits inflammasome activation in macrophages, and decreases atherosclerosis in Ldlr-/- mice. Cardiovasc. Res. 2020, 116, 1948–1957. [Google Scholar] [CrossRef]
- Lees, H.J.; Swann, J.R.; Wilson, I.D.; Nicholson, J.K.; Holmes, E. Hippurate: The natural history of a mammalian-microbial cometabolite. J. Proteome Res. 2013, 12, 1527–1546. [Google Scholar] [CrossRef]
- Zhang, F.; Jia, Z.; Gao, P.; Kong, H.; Li, X.; Chen, J.; Yang, Q.; Yin, P.; Wang, J.; Lu, X.; et al. Metabonomics study of atherosclerosis rats by ultra fast liquid chromatography coupled with ion trap-time of flight mass spectrometry. Talanta 2009, 79, 836–844. [Google Scholar] [CrossRef]
- Calvani, R.; Miccheli, A.; Capuani, G.; Miccheli, A.T.; Puccetti, C.; Delfini, M.; Iaconelli, A.; Nanni, G.; Mingrone, G. Gut microbiome-derived metabolites characterize a peculiar obese urinary metabotype. Int. J. Obes. 2010, 34, 1095–1098. [Google Scholar] [CrossRef] [Green Version]
- Mulder, T.P.; Rietveld, A.G.; van Amelsvoort, J.M. Consumption of both black tea and green tea results in an increase in the excretion of hippuric acid into urine. Am. J. Clin. Nutr. 2005, 81 (Suppl. 1), 256S–260S. [Google Scholar] [CrossRef] [Green Version]
- McCullough, M.L.; Peterson, J.J.; Patel, R.; Jacques, P.F.; Shah, R.; Dwyer, J.T. Flavonoid intake and cardiovascular disease mortality in a prospective cohort of US adults. Am. J. Clin. Nutr. 2012, 95, 454–464. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Ouyang, Y.Y.; Liu, J.; Zhao, G. Flavonoid intake and risk of CVD: A systematic review and meta-analysis of prospective cohort studies. Br. J. Nutr. 2014, 111, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Peterson, J.J.; Dwyer, J.T.; Jacques, P.F.; McCullough, M.L. Associations between flavonoids and cardiovascular disease incidence or mortality in European and US populations. Nutr. Rev. 2012, 70, 491–508. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.; Loo, R.L.; Stamler, J.; Bictash, M.; Yap, I.K.S.; Chan, Q.; Ebbels, T.; De Iorio, M.; Brown, I.J.; Veselkov, K.A.; et al. Human metabolic phenotype diversity and its association with diet and blood pressure. Nature 2008, 453, 396–400. [Google Scholar] [CrossRef]
- Akira, K.; Masu, S.; Imachi, M.; Mitome, H.; Hashimoto, M.; Hashimoto, T. 1H NMR-based metabonomic analysis of urine from young spontaneously hypertensive rats. J. Pharm. Biomed. Anal. 2008, 46, 550–556. [Google Scholar] [CrossRef]
- Lee, T.-S.; Lu, T.-M.; Chen, C.-H.; Guo, B.; Hsu, C.-P. Hyperuricemia induces endothelial dysfunction and accelerates atherosclerosis by disturbing the asymmetric dimethylarginine/dimethylarginine dimethylaminotransferase 2 pathway. Redox Biol. 2021, 46, 102108. [Google Scholar] [CrossRef]
- Jalkanen, J.; Maksimow, M.; Hollmen, M.; Jalkanen, S.; Hakovirta, H. Compared to Intermittant Claudication Critical Limb Ischemia Is Associated with Elevated Levels of Cytokines. PLoS ONE 2016, 11, e0162353. [Google Scholar] [CrossRef] [Green Version]
- Gremmels, H.; Teraa, M.; De Jager, S.C.A.; Pasterkamp, G.; De Borst, G.J.; Verhaar, M.C. A Pro-Inflammatory Biomarker-Profile Predicts Amputation-Free Survival in Patients with Severe Limb Ischemia. Sci. Rep. 2019, 9, 10740. [Google Scholar] [CrossRef] [Green Version]
- Sartipy, F.; Sigvant, B.; Lundin, F.; Wahlberg, E. Ten Year Mortality in Different Peripheral Arterial Disease Stages: A Population Based Observational Study on Outcome. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Kumakura, H.; Kanai, H.; Hojo, Y.; Iwasaki, T.; Ichikawa, S. Long-term survival and fate of the leg in de novo intermittent claudication. Eur. Heart J. Qual. Care Clin. Outcomes 2017, 3, 208–215. [Google Scholar] [CrossRef]
- Brown, J.M.; Hazen, S.L. Microbial modulation of cardiovascular disease. Nat. Rev. Microbiol. 2018, 16, 171–181. [Google Scholar] [CrossRef]
- Sonnenburg, J.L.; Backhed, F. Diet-microbiota interactions as moderators of human metabolism. Nature 2016, 535, 56–64. [Google Scholar] [CrossRef]
- Willing, B.P.; Russell, S.L.; Finlay, B.B. Shifting the balance: Antibiotic effects on host-microbiota mutualism. Nat. Rev. Microbiol. 2011, 9, 233–243. [Google Scholar] [CrossRef]
- Maier, L.; Pruteanu, M.; Kuhn, M.; Zeller, G.; Telzerow, A.; Anderson, E.E.; Brochado, A.R.; Fernandez, K.C.; Dose, H.; Mori, H.; et al. Extensive impact of non-antibiotic drugs on human gut bacteria. Nature 2018, 555, 623–628. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Covariates N (%) or Median [Interquartile Range] | Control Cohort (N = 37) | Claudication (N = 119) | p Value |
|---|---|---|---|
| Age | 67 (60–74) | 68 (65–73) | 0.19 |
| Male sex | 32 (86.5) | 115 (96.6) | 0.02 |
| African-American | 7 (18.9) | 23 (19.3) | 0.54 |
| Body mass index (kg/m2) | 29.4 (26.1–31.3) | 27.8 (24.4–31.2) | 0.18 |
| Coronary artery disease | 0 | 47 (39.5) | <0.0001 |
| Prior coronary revascularization | 33 (75%) | ||
| Prior MACE | 0 | 46 (42.4) | <0.0001 |
| Hypertension | 25 (67.6) | 111 (93.3) | <0.0001 |
| Hyperlipidemia | 24 (64.9) | 100 (84) | <0.01 |
| Diabetes mellitus | 8 (21.6) | 41 (34.5) | 0.14 |
| Current/former smoker | 27 (75) | 119 (93.3) | 0.002 |
| Aspirin use | 19 (51.4) | 86 (72.3) | 0.02 |
| Statin use | 23 (62.2) | 95 (79.3) | 0.03 |
| ABI | 1.1 (1.1–1.2) | 0.73 (0.64–0.81) | <0.0001 |
| Total cholesterol, mg/dL | 170 (142.5–197) | 158 (127–182) | 0.10 |
| LDL cholesterol, mg/dL | 99 (79.5–124.5) | 82 (60–106) | 0.008 |
| HDL cholesterol, mg/dL | 43.5 (38–47.5) | 42 (35–55) | 0.89 |
| eGFR, mL/min/1.73 mm2 | 82 (66–107) | 70.5 (60.5–86.5) | 0.02 |
| hs-CRP, mg/mL | 3.3 (1.2–5.1) | 2.4 (1.5–6) | 0.82 |
| Rutherford classification | <0.0001 | ||
| 0 | 37 (100) | 4 (3.4) | |
| 1 | 0 | 38 (32.5) | |
| 2 | 0 | 34 (29.1) | |
| 3 | 0 | 41 (35.0) | |
| Metabolites, μmol | |||
| Indole derivatives | |||
| Serotonin | 1.3 (.52–2.4) | 0.96 (0.48–1.38) | 0.02 |
| KYN | 3.8 (2.9–5) | 2.3 (1.9–4.2) | 0.0001 |
| TRP | 0.076 (0.047–0.099) | 0.052 (0.038–0.076) | 0.005 |
| KYN/TRP ratio (x100) | 4975 (3717–6783) | 4935 (3949–6743) | 0.69 |
| IPA | 2.7 (1.7–4.1) | 1.07 (0.57–1.86) | <0.0001 |
| I3A | 0.21 (0.14–0.24) | 0.12 (0.10–0.16) | <0.0001 |
| IS | 1.3 (0.6–2.4) | 2.8 (1.8–4.9) | 0.002 |
| HAA | 0 | 0.31 (0.22–0.54) | <0.0001 |
| Phenyl derivatives | |||
| PCS | 0.23 (0.13–0.37) | 0.31 (0.19–0.51) | 0.07 |
| HA | 18.4 (11.7–24.2) | 9.4 (6.3–16.7) | <0.0001 |
| Cytokines, pg/mL | |||
| IL-6 | 0.85 (0.63–1.23) | 1.2 (0.93–1.81) | 0.02 |
| ICAM | 206 (172–300) | 246 (207–300) | 0.06 |
| TNF-α | 1.7 (1.3–2.0) | 1.98 (1.64–2.35) | 0.004 |
| Omega-3 index | 0.064 (0.050–0.072) | 0.046 (0.040–0.055) | <0.0001 |
| Metabolite | OR | 95% CI | p Value |
|---|---|---|---|
| ln serotonin | 0.69 | 0.45–1.1 | 0.1 |
| ln KYN | 0.22 | 0.086–0.57 | 0.002 |
| ln TRP | 0.69 | 0.34–1.4 | 0.29 |
| ln KYN/TRP | 0.65 | 0.36–1.15 | 0.14 |
| ln HA | 0.42 | 0.24–0.72 | 0.002 |
| ln IPA | 0.36 | 0.21–0.61 | 0.0002 |
| ln IS | 1.8 | 1.11–3.00 | 0.02 |
| ln PCS | 1.1 | 0.72–1.72 | 0.63 |
| ln HAA | 4.44 | 2.6–7.5 | <0.0001 |
| ln I3A | 0.11 | 0.03–0.35 | 0.0002 |
| Variable | No MACE N = 111 (79.9%) | MACE N = 28 (20.1%) | p Value |
|---|---|---|---|
| Age | 67.4 (63.6–73.3) | 68.8 (64.4–75.8) | 0.35 |
| Male sex | 108 (97.3%) | 27 (96.4%) | 0.99 |
| African-American | 24 (21.6%) | 4 (14.3%) | 0.56 |
| Body mass index (kg/m2) | 28.6 (25.0–31.2) | 27.8 (24.6–32.6) | 0.99 |
| Past medical history | |||
| Coronary artery disease | 27 (24.3%) | 17 (60.7%) | 0.0002 |
| Prior coronary revascularization | 18 (66.7%) | 15 (88.2%) | 0.11 |
| Prior MACE | 29 (26.1%) | 17 (60.7%) | 0.0005 |
| Hypertension | 98 (88.3%) | 25 (89.3%) | 0.88 |
| Hyperlipidemia | 92 (82.3%) | 22 (78.6%) | 0.60 |
| Diabetes mellitus | 35 (31.5%) | 10 (35.7%) | 0.67 |
| Current/former smoker | 100 (90.9%) | 25 (89.3%) | 0.79 |
| Aspirin use | 76 (68.5%) | 20 (71.4%) | 0.76 |
| Statin use | 82 (73.9%) | 23 (82.1%) | 0.36 |
| ABI | 0.8 (0.7–1.0) | 0.7 (0.6–0.8) | 0.01 |
| Total cholesterol, mg/dL | 160 (136–185) | 156 (122–189.5) | 0.61 |
| LDL cholesterol, mg/dL | 83 (64–110) | 83 (57.5–108.5) | 0.53 |
| HDL cholesterol, mg/dL | 43 (36–54) | 45 (35.5–50.5) | 0.57 |
| eGFR, mL/min/1.73 mm2 | 73 (63–90) | 72 (60–93) | 0.76 |
| hs-CRP, mg/mL | 2.4 (1.3–5.1) | 3.4 (1.7–7.1) | 0.28 |
| Rutherford classification | 0.08 | ||
| 0 | 29 (26.4%) | 4 (14.3%) | |
| 1 | 30 (27.3%) | 4 (14.3%) | |
| 2 | 25 (22.7%) | 7 (25.0%) | |
| 3 | 26 (23.6%) | 13 (45.4%) | |
| Metabolites, μmol | |||
| Indole derivatives | |||
| Serotonin | 0.96 (0.40–1.49) | 1.14 (0.64–1.51) | 0.46 |
| KYN | 2.84 (2.02–4.57) | 2.89 (1.77–3.21) | 0.02 |
| TRP | 0.06 (0.04–0.09) | 0.04 (0.029–0.057) | 0.003 |
| KYN/TRP ratio (x100) | 4790 (3798–6491) | 4955 (4189–6892) | 0.30 |
| IPA | 1.15 (0.61–2.3) | 1.11 (0.63–1.77) | 0.65 |
| I3A | 0.14 (0.11–0.20) | 0.11 (0.096–0.16) | 0.02 |
| IS | 2.70 (1.55–4.56) | 3.03 (1.81–4.40) | 0.74 |
| HAA | 0.26 (0–0.44) | 0.28 (0.11–0.63) | 0.32 |
| Phenyl derivatives | |||
| PCS | 0.29 (0.17–0.47) | 0.32 (0.21–0.70) | 0.20 |
| HA | 11.0 (7.1–19.7) | 9.1 (5.3–16.8) | 0.12 |
| Cytokines, pg/mL | |||
| IL-6 | 1.1 (0.79–1.49) | 1.5 (1–2.4) | 0.03 |
| ICAM | 230 (196.4–280) | 272.9 (221.5–308.1) | 0.07 |
| TNF-α | 1.86 (1.45–2.24) | 2.05 (1.82–2.31) | 0.04 |
| Omega-3 index | 0.07 (0.06–0.08) | 0.05 (0.04–0.06) | 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, K.J.; Ramirez, J.L.; Kulkarni, R.; Harris, K.G.; Helenowski, I.; Xiong, L.; Ozaki, C.K.; Grenon, S.M. Plasma Gut Microbe-Derived Metabolites Associated with Peripheral Artery Disease and Major Adverse Cardiac Events. Microorganisms 2022, 10, 2065. https://doi.org/10.3390/microorganisms10102065
Ho KJ, Ramirez JL, Kulkarni R, Harris KG, Helenowski I, Xiong L, Ozaki CK, Grenon SM. Plasma Gut Microbe-Derived Metabolites Associated with Peripheral Artery Disease and Major Adverse Cardiac Events. Microorganisms. 2022; 10(10):2065. https://doi.org/10.3390/microorganisms10102065
Chicago/Turabian StyleHo, Karen J., Joel L. Ramirez, Rohan Kulkarni, Katharine G. Harris, Irene Helenowski, Liqun Xiong, C. Keith Ozaki, and S. Marlene Grenon. 2022. "Plasma Gut Microbe-Derived Metabolites Associated with Peripheral Artery Disease and Major Adverse Cardiac Events" Microorganisms 10, no. 10: 2065. https://doi.org/10.3390/microorganisms10102065