
The Association of Toxoplasma gondii IgG Antibody and Chronic Kidney Disease Biomarkers


Abstract
:1. Introduction
1.1. Toxoplasma
1.2. Chronic Kidney Disease
1.3. Toxoplasma and CKD
2. Materials and Methods
2.1. Study Population
2.2. Exposure Variable: T. gondii
2.3. CKD biomarkers
2.3.1. First and Second Albumin-to-Creatinine Ratios
2.3.2. First and Second Albuminuria
2.3.3. Persistent Albuminuria
2.3.4. Serum Creatinine (Scr)
2.3.5. eGFR
2.3.6. CKD
- Stage 1: eGFR ≥ 90 mL/min/1.73 m2 and estimated persistent albuminuria;
- Stage 2: eGFR 60–89 mL/min/1.73 m2 and estimated persistent albuminuria;
- Stage 3: eGFR 30–59 mL/min/1.73 m2;
- Stage 4: eGFR 15–29 mL/min/1.73 m2;
- Stage 5: eGFR < 15mL/min/1.73 m2.
- Negative: Negative;
- Mild CKD: Stage 1 and 2;
- Moderate-to-Severe CKD: Stage 3, 4, and 5.
2.4. Covariates for Models Adjustment
2.5. Statistical Analysis
3. Results
3.1. Data Summary
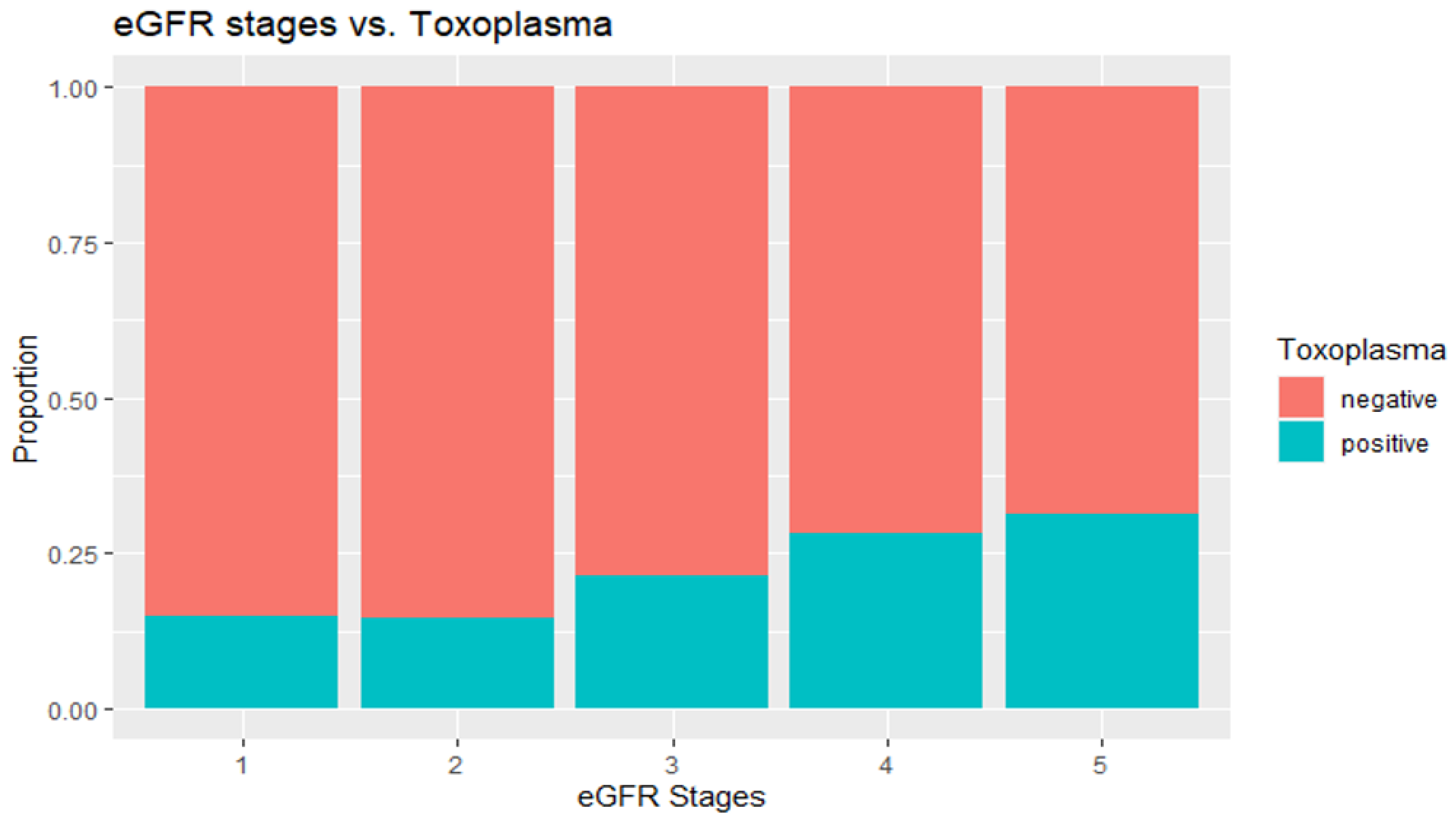
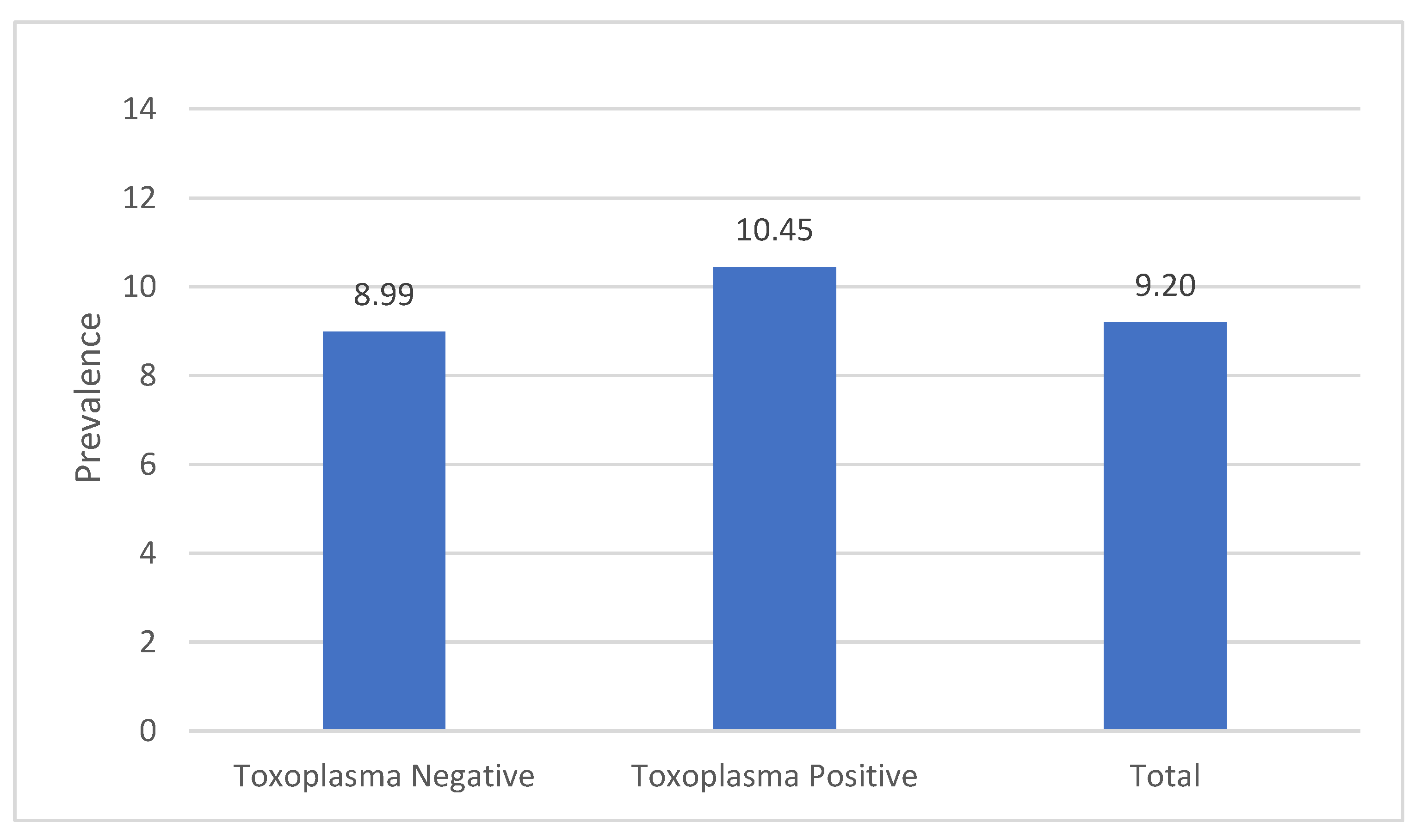
3.2. Association of Toxoplasma and CKD Biomarkers and CKD Status
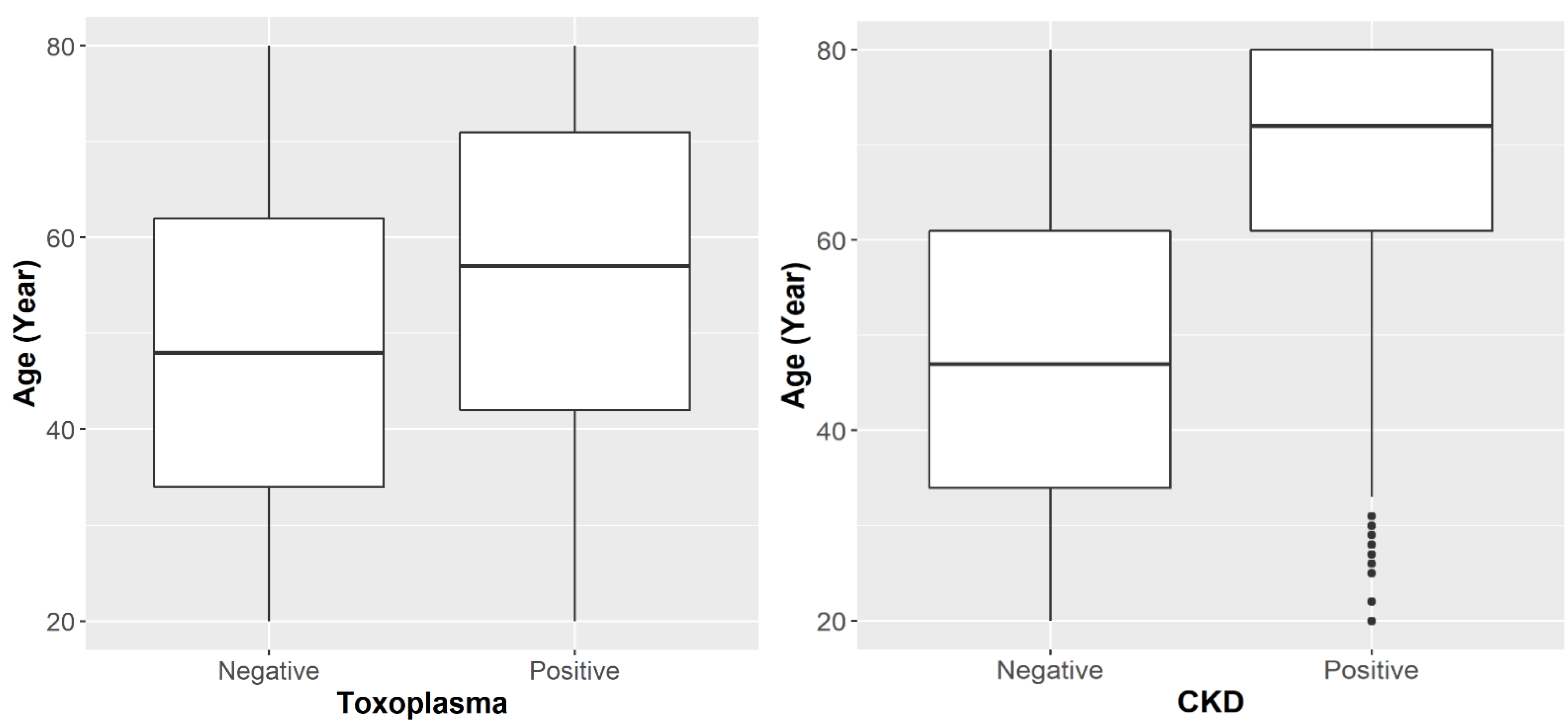
3.3. Age Factor
3.4. Association of Toxoplasma and CKD after Adjusting for Co-Variates
4. Discussion
4.1. Overview of Results and Implications
4.2. Implications of Findings
4.3. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, J.L.; Kruszon-Moran, D.; Elder, S.; Rivera, H.N.; Press, C.; Montoya, J.G.; McQuillan, G.M. PMC5929212; Toxoplasma gondii Infection in the United States, 2011–2014. Am. J. Trop. Med. Hyg. 2018, 98, 551–557. [Google Scholar] [CrossRef]
- Hotez, P.J. Neglected infections of poverty in the United States of America. PLoS Negl. Trop. Dis. 2008, 2, e256. [Google Scholar] [CrossRef] [Green Version]
- Tamma, P. Toxoplasmosis. Pediatr. Rev 2007, 28, 470–471. [Google Scholar] [CrossRef]
- Khryanin, A.A.; Reshetnikov, O.V.; Kuvshinova, I.N. [Toxoplasmosis: Epidemiology, Diagnosis, Treatment]. Antibiot Khimioter 2015, 60, 16–21. [Google Scholar]
- Dubey, J.P.; Frenkel, J.K. Cyst-induced toxoplasmosis in cats. J. Protozool. 1972, 19, 155–177. [Google Scholar] [CrossRef]
- Ahmed, H.; Malik, A.; Arshad, M.; Mustafa, I.; Khan, M.R.; Afzal, M.S.; Ali, S.; Mobeen, M.; Simsek, S. Seroprevalence and Spatial Distribution of Toxoplasmosis in Sheep and Goats in North-Eastern Region of Pakistan. Korean J. Parasitol. 2016, 54, 439–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, A.J.; Gilbert, R.E.; Buffolano, W.; Zufferey, J.; Petersen, E.; Jenum, P.A.; Foulon, W.; Semprini, A.E.; Dunn, D.T. Sources of toxoplasma infection in pregnant women: European multicentre case-control study. European Research Network on Congenital Toxoplasmosis. BMJ 2000, 321, 142–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhopale, G.M. Pathogenesis of toxoplasmosis. Comp. Immunol. Microbiol. Infect. Dis. 2003, 26, 213–222. [Google Scholar] [CrossRef]
- Sibley, L.D.; Boothroyd, J.C. Virulent strains of Toxoplasma gondii comprise a single clonal lineage. Nature 1992, 359, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Harker, K.S.; Ueno, N.; Lodoen, M.B. Toxoplasma gondii dissemination: A parasite’s journey through the infected host. Parasite Immunol. 2015, 37, 141–149. [Google Scholar] [CrossRef]
- Xiao, J.; Yolken, R.H. PMC4361247; Strain hypothesis of Toxoplasma gondii infection on the outcome of human diseases. Acta Physiol. 2015, 213, 828–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortego, T.J.; Robey, B.; Morrison, D.; Chan, C. Toxoplasmic chorioretinitis and hepatic granulomas. Am. J. Gastroenterol. 1990, 85, 1418–1420. [Google Scholar]
- El-Sayed, N.M.; Ramadan, M.E.; Ramadan, M.E. Toxoplasma gondii Infection and Chronic Liver Diseases: Evidence of an Association. Trop. Med. Infect. Dis. 2016, 1, 7. [Google Scholar] [CrossRef] [PubMed]
- Babekir, A.; Mostafa, S.; Obeng-Gyasi, E.J.I.J.o.E.R.; Health, P. The Association of Toxoplasma gondii IgG and Cardiovascular Biomarkers. Int. J. Environ. Res. Public Health 2021, 18, 4908. [Google Scholar] [CrossRef]
- Brown, A.S. Prenatal infection as a risk factor for schizophrenia. Schizophr. Bull. 2006, 32, 200–202. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. (n.d.). Chronic kidney disease (CKD). National Institute of Diabetes and Digestive and Kidney Diseases. Available online: https://www.niddk.nih.gov/health-information/kidney-disease/chronic-kidney-disease-ckd (accessed on 20 November 2021).
- Chronic Kidney Disease Initiative. Chronic Kidney Disease in the United States. 2021. Available online: https://www.cdc.gov/kidneydisease/publications-resources/ckd-national-facts.html (accessed on 20 November 2021).
- Yang, J.; He, W. Chronic Kidney Disease; Springer Singapore Pte. Limited: Singapore, 2019; Volume 66, pp. s03–s09. [Google Scholar]
- Tecklenborg, J.; Clayton, D.; Siebert, S.; Coley, S.M. The role of the immune system in kidney disease. Clin. Exp. Immunol. 2018, 192, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Kazancioğlu, R. Risk factors for chronic kidney disease: An update. Kidney Int. Suppl. 2013, 3, 368–371. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Diabetes and Digestive and Kidney Diseases. Albuminuria: Albumin in the Urine. 2021. Available online: https://www.niddk.nih.gov/health-information/kidney-disease/chronic-kidney-disease-ckd/tests-diagnosis/albuminuria-albumin-urine (accessed on 11 November 2021).
- Peralta, C.A.; Shlipak, M.G.; Judd, S.; Cushman, M.; McClellan, W.; Zakai, N.A.; Safford, M.M.; Zhang, X.; Muntner, P.; Warnock, D. Detection of Chronic Kidney Disease With Creatinine, Cystatin C, and Urine Albumin-to-Creatinine Ratio and Association With Progression to End-Stage Renal Disease and Mortality. JAMA J. Am. Med. Assoc. 2011, 305, 1545–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamb, E.J.; Levey, A.S.; Stevens, P.E. The Kidney Disease Improving Global Outcomes (KDIGO) Guideline Update for Chronic Kidney Disease: Evolution not Revolution. Clin. Chem. 2013, 59, 462–465. [Google Scholar] [CrossRef]
- American Kidney Fund (AKF). Stages of Chronic Kidney Disease (CKD). 2021. Available online: https://www.kidneyfund.org/kidney-disease/chronic-kidney-disease-ckd/stages-of-chronic-kidney-disease/ (accessed on 11 November 2021).
- National Health and Nutrition Examination Survey. NHANES 2009–2010: Standard Biochemistry Profile Data Documentation, Codebook, and Frequencies. 2014. Available online: https://wwwn.cdc.gov/nchs/nhanes/2009-2010/BIOPRO_F.htm (accessed on 11 November 2021).
- Castro, A.F.; Coresh, J. CKD surveillance using laboratory data from the population-based National Health and Nutrition Examination Survey (NHANES). Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2009, 53, 46. [Google Scholar] [CrossRef] [Green Version]
- Kibria, G.M.A.; Crispen, R. Prevalence and trends of chronic kidney disease and its risk factors among US adults: An analysis of NHANES 2003-18. Prev. Med. Rep. 2020, 20, 101193. [Google Scholar] [CrossRef]
- Vart, P.; Powe, N.R.; McCulloch, C.E.; Saran, R.; Gillespie, B.W.; Saydah, S.; Crews, D.C. National Trends in the Prevalence of Chronic Kidney Disease Among Racial/Ethnic and Socioeconomic Status Groups, 1988–2016. JAMA Netw. Open 2020, 3, e207932. [Google Scholar] [CrossRef]
- Saki, J.; Khademvatan, S.; Soltani, S.; Shahbazian, H. Detection of toxoplasmosis in patients with end-stage renal disease by enzyme-linked immunosorbent assay and polymerase chain reaction methods. Parasitol. Res. 2013, 112, 163–168. [Google Scholar] [CrossRef]
- Al-Khamesi, M.; Al-Sibahi, Z.; Alobaidy, L.; Hilal, Z. Studying of Kidney, Liver Functions and Some Blood Ions In Toxoplasmosis Patients. Al-Mustansiriyah J. Sci. 2016, 27, 43–46. [Google Scholar]
- Mohammadi Manesh, R.; Hosseini Safa, A.; Sharafi, S.M.; Jafari, R.; Bahadoran, M.; Yousefi, M.; Nasri, H.; Yousofi Darani, H. Parasites and chronic renal failure. J. Ren. Inj. Prev. 2014, 3, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Molan, A.-L. Prevalence of Toxoplasma gondii Infection in Hemodialysis Patients with Chronic Renal Failure and Risk Factors in Diyala Province, Iraq. Malysian J. Med. Health Sci. 2019, 15, 31–36. [Google Scholar]
- Kaminski, T.W.; Pawlak, K.; Karbowska, M.; Mysliwiec, M.; Grzegorzewski, W.; Kuna, J.; Pawlak, D. Association between uremic toxin-anthranilic acid and fibrinolytic system activity in predialysis patients at different stages of chronic kidney disease. Int. Urol. Nephrol. 2018, 50, 127–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripepi, G.; Jager, K.J.; Dekker, F.W.; Zoccali, C. Stratification for confounding–part 1: The Mantel-Haenszel formula. Nephron Clin. Pract. 2010, 116, c317–c321. [Google Scholar] [CrossRef]
- Ocak, S.; Duran, N.; Eskiocak, A.F.; Aytac, H. Anti-Toxoplasma gondii antibodies in hemodialysis patients receiving long-term hemodialysis therapy in Turkey. Saudi Med. J. 2005, 26, 1378–1382. [Google Scholar]
- Saadat, F.; Mahmoudi, M.R.; Rajabi, E.; Roshan, Z.A.; Shad, B.M.; Karanis, P. Seroepidemiology and associated risk factors of Toxoplasma gondii in hemodialysis patients. Acta Parasitol. 2020, 65, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Dincel, G.C.; Atmaca, H.T. Role of oxidative stress in the pathophysiology of Toxoplasma gondii infection. Int. J. Immunopathol. Pharmacol. 2016, 29, 226–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative stress: Harms and benefits for human health. Oxidative Med. Cell. Longev. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.; Mitra, N.; Kanetsky, P.A.; Devaney, J.; Wing, M.R.; Reilly, M.; Shah, V.O.; Balakrishnan, V.S.; Guzman, N.J.; Girndt, M. Association between albuminuria, kidney function, and inflammatory biomarker profile in CKD in CRIC. Clin. J. Am. Soc. Nephrol. 2012, 7, 1938–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Description | n | Weighted Percentage/Mean (SE) |
|---|---|---|---|
| T. gondii IgG antibody | <33 IU/mL (negative) | 3789 | 84.8 |
| ≥33 IU/mL (positive) | 903 | 15.2 | |
| Gender | Male | 2256 | 47.7 |
| Female | 2436 | 52.3 | |
| Age | 4692 | 47.9 (0.49) | |
| Age group | Younger (<45) | 1792 | 41.9 |
| Older (≥45) | 2900 | 58.1 | |
| Race/ethnicity | Mexican American | 874 | 8.4 |
| Other Hispanic | 483 | 4.8 | |
| Non-Hispanic White | 2337 | 70.4 | |
| Non-Hispanic Black | 754 | 9.9 | |
| Other Race | 244 | 6.5 | |
| Alcohol use | Yes | 694 | 15.6 |
| No | 3046 | 84.4 | |
| Smoking use | Every day | 767 | 35.9 |
| Some days | 169 | 6.0 | |
| Not at all | 1211 | 58.1 | |
| Marijuana/hashish use | Yes | 1440 | 58.0 |
| No | 1309 | 42.0 | |
| Cocaine/heroin/methamphetamine use | Yes | 611 | 18.5 |
| No | 2824 | 81.5 | |
| BMI | 4659 | 28.9 (0.14) | |
| Having diabetes | Yes | 550 | 8.4 |
| No | 4045 | 89.7 | |
| Borderline | 94 | 1.9 | |
| Kidney Biomarker | |||
| First albumin creatinine ratio | 4692 | 24.1(2.94) | |
| Second albumin creatinine ratio | 4692 | 16.0 (2.06) | |
| First albuminuria | Negative | 4183 | 92.0 |
| Microalbuminuria | 424 | 6.9 | |
| Macroalbuminuria | 85 | 1.1 | |
| Second albuminuria | Negative | 4383 | 95.3 |
| Microalbuminuria | 248 | 4.0 | |
| Macroalbuminuria | 61 | 0.7 | |
| Persistent albuminuria | Negative | 4437 | 96.5 |
| Positive | 255 | 3.5 | |
| eGFR | 4692 | 87.8 (0.74) | |
| eGFR stages | Stage 1 | 2150 | 43.2 |
| Stage 2 | 2089 | 49.2 | |
| Stage 3 | 413 | 7.1 | |
| Stage 4 | 29 | 0.4 | |
| Stage 5 | 11 | 0.1 | |
| CKD | Negative | 4070 | 90.0 |
| Positive | 622 | 10.0 | |
| CKD levels | Negative | 4070 | 90.0 |
| Mild | 169 | 2.4 | |
| Moderate-to-Severe | 453 | 7.6 | |
| CKD stages | Negative | 4070 | 90.0 |
| Stage 1 | 69 | 0.9 | |
| Stage 2 | 100 | 1.5 | |
| Stage 3 | 413 | 7.1 | |
| Stage 4 | 29 | 0.4 | |
| Stage 5 | 11 | 0.1 |
| Variable | Level | T. gondii Negative | T. gondii Positive | p-Value | ||
|---|---|---|---|---|---|---|
| n | Weighted Percentage or Mean (SE) | n | Weighted Percentage or Mean (SE) | |||
| First albumin-to-creatinine ratio | 3789 | 22.5 (3.56) | 903 | 32.9 (4.62) | 0.1222 | |
| Second albumin-to-creatinine ratio | 3789 | 14.4 (2.38) | 903 | 24.9 (3.91) | 0.0376 | |
| First albuminuria | Negative | 3389 | 85.1 | 794 | 14.9 | 0.0752 |
| Microalbuminuria | 336 | 83.5 | 88 | 16.5 | ||
| Macroalbuminuria | 64 | 74.1 | 21 | 25.9 | ||
| Second albuminuria | Negative | 3555 | 85.2 | 828 | 14.8 | 0.0005 |
| Microalbuminuria | 192 | 78.2 | 56 | 21.8 | ||
| Macroalbuminuria | 42 | 67.8 | 19 | 32.2 | ||
| Persistent albuminuria | Negative | 3594 | 76.9 | 843 | 23.1 | <0.0001 |
| Positive | 195 | 85.1 | 60 | 14.9 | ||
| eGFR | 3789 | 88.1 (0.76) | 903 | 86.2 (1.22) | 0.0913 | |
| eGFR stages | Stage 1 | 1758 | 85.2 | 392 | 14.8 | 0.0014 |
| Stage 2 | 1688 | 85.6 | 401 | 14.4 | ||
| Stage 3 | 317 | 78.7 | 96 | 21.3 | ||
| Stage 4 | 20 | 71.7 | 9 | 28.3 | ||
| Stage 5 | 6 | 68.8 | 5 | 31.2 | ||
| CKD | Negative | 3314 | 85.6 | 756 | 14.4 | 0.0001 |
| Positive | 475 | 77.9 | 147 | 22.1 | ||
| CKD levels | Negative | 3314 | 85.6 | 756 | 14.4 | <0.0001 |
| Mild | 132 | 76.9 | 37 | 23.1 | ||
| Moderate-to-Severe | 343 | 78.2 | 110 | 21.8 | ||
| CKD stages | Negative | 3314 | 85.6 | 756 | 14.4 | 0.0004 |
| Stage 1 | 58 | 79.8 | 11 | 20.2 | ||
| Stage 2 | 74 | 75.1 | 26 | 24.9 | ||
| Stage 3 | 317 | 78.7 | 96 | 21.3 | ||
| Stage 4 | 20 | 71.1 | 9 | 28.9 | ||
| Stage 5 | 6 | 68.8 | 5 | 31.2 | ||
| Toxoplasma IgG Antibody | Younger (<45 Year) | Older (≥45 Year) | ||||
|---|---|---|---|---|---|---|
| No CKD | CKD | Total | No CKD | CKD | Total | |
| Negative (n) | 1505 | 43 | 1548 | 1809 | 432 | 2241 |
| Positive (n) | 239 | 5 | 244 | 517 | 142 | 659 |
| Stratified risk ratio | RRyoung = 0.76 (95% CI: 0.33–1.76) | RRold = 1.11 (95% CI: 0.95–1.31) | ||||
| Unstratified risk ratio (RRcrude) = 1.27 (95% CI: 1.09–1.49) | ||||||
| Pooled estimate risk ratio (RRMH) = 1.09 (95% CI: 0.93–1.28) | ||||||
| Magnitude of Confounding = 17% | ||||||
| CKD | ||||
|---|---|---|---|---|
| Sample Size = 4659 | Odds Ratio | OR 95% Confidence Interval | p-Value | |
| Toxoplasma IgG antibody (Positive) | 1.40 | 1.06 | 1.84 | 0.0447 |
| Age | ||||
| Younger (<45) (reference) | ||||
| Older (≥45) | 8.89 | 6.31 | 12.51 | <0.0001 |
| Gender | ||||
| Male (reference) | ||||
| Female | 1.27 | 1.06 | 1.54 | 0.0352 |
| Race/ethnicity | ||||
| Mexican American (reference) | ||||
| Other Hispanic | 0.91 | 0.62 | 1.34 | 0.6524 |
| Non-Hispanic White | 1.09 | 0.76 | 1.55 | 0.6649 |
| Non-Hispanic Black | 0.93 | 0.59 | 1.49 | 0.7786 |
| Other Race | 0.90 | 0.42 | 1.95 | 0.8028 |
| BMI | 1.04 | 1.02 | 1.06 | 0.0059 |
| Constant | 0.01 | 0.00 | 0.01 | <0.0001 |
| AIC = 2697, Pseudo R-Square = 0.07 | ||||
| CKD | ||||
|---|---|---|---|---|
| Sample Size = 3722 | Odds Ratio | OR 95% Confidence Interval | p-Value | |
| Toxoplasma IgG antibody (Positive) | 1.27 | 0.97 | 1.64 | 0.1381 |
| Age | ||||
| Younger (<45) (reference) | ||||
| Older (≥45) | 8.59 | 5.48 | 13.47 | 0.0002 |
| Gender | ||||
| Male (reference) | ||||
| Female | 1.15 | 0.93 | 1.42 | 0.2487 |
| Race/ethnicity | ||||
| Mexican American (reference) | ||||
| Other Hispanic | 1.00 | 0.60 | 1.64 | 0.9873 |
| Non-Hispanic White | 1.19 | 0.88 | 1.62 | 0.2985 |
| Non-Hispanic Black | 0.95 | 0.57 | 1.55 | 0.8334 |
| Other Race | 0.79 | 0.35 | 1.79 | 0.5932 |
| Alcohol use (No) | 0.94 | 0.71 | 1.25 | 0.7102 |
| BMI | 1.04 | 1.01 | 1.06 | 0.0144 |
| Has Diabetes (No) | 0.40 | 0.27 | 0.61 | 0.0075 |
| Constant | 0.03 | 0.01 | 0.08 | 0.0009 |
| AIC = 2120, Pseudo R-Square = 0.08 | ||||
| CKD | ||||
|---|---|---|---|---|
| Sample Size = 3722 | Odds Ratio | OR 95% Confidence Interval | p-Value | |
| Toxoplasma IgG antibody (Positive) | 1.56 | 1.20 | 2.04 | 0.0168 |
| Gender | ||||
| Male (reference) | ||||
| Female | 1.18 | 0.98 | 1.43 | 0.1464 |
| Race/ethnicity | ||||
| Mexican American (reference) | ||||
| Other Hispanic | 0.97 | 0.59 | 1.63 | 0.9338 |
| Non-Hispanic White | 1.70 | 1.21 | 2.27 | 0.0196 |
| Non-Hispanic Black | 1.11 | 0.68 | 1.82 | 0.6845 |
| Other Race | 0.81 | 0.39 | 1.73 | 0.6046 |
| Alcohol use (No) | 0.89 | 0.67 | 1.17 | 0.4407 |
| BMI | 1.03 | 1.01 | 1.05 | 0.0219 |
| Has Diabetes (No) | 0.30 | 0.19 | 0.43 | 0.0078 |
| Constant | 0.24 | 0.10 | 0.54 | 0.0142 |
| AIC = 2299, Pseudo R-Square = 0.03 | ||||
| CKD | ||||
|---|---|---|---|---|
| Sample Size = 1885 | Odds Ratio | OR 95% Confidence Interval | p-Value | |
| Toxoplasma IgG antibody (Positive) | 1.81 | 1.26 | 2.60 | 0.0325 |
| Gender | ||||
| Male (reference) | ||||
| Female | 0.99 | 0.73 | 1.33 | 0.9525 |
| Race/ethnicity | ||||
| Mexican American (reference) | ||||
| Other Hispanic | 0.82 | 0.38 | 1.75 | 0.6348 |
| Non-Hispanic White | 1.46 | 0.88 | 2.44 | 0.2133 |
| Non-Hispanic Black | 1.45 | 0.83 | 2.56 | 0.2593 |
| Other Race | 0.53 | 0.17 | 1.68 | 0.3423 |
| Alcohol use (No) | 0.89 | 0.64 | 1.27 | 0.5732 |
| BMI | 1.02 | 1.01 | 1.04 | 0.0696 |
| Has Diabetes (No) | 0.30 | 0.19 | 0.51 | 0.0125 |
| Smoking use (No) Reference | ||||
| Smoking use (every day) | 0.93 | 0.49 | 1.76 | 0.8512 |
| Smoking use (some days) | 1.78 | 1.32 | 2.39 | 0.0187 |
| Constant | 0.24 | 0.10 | 0.54 | 0.1556 |
| AIC = 1142, Pseudo R-Square = 0.04 | ||||
| CKD | ||||
|---|---|---|---|---|
| Sample Size = 1551 | Odds Ratio | OR 95% Confidence Interval | p-Value | |
| Toxoplasma IgG antibody (Positive) | 0.75 | 0.36 | 1.56 | 0.5803 |
| Gender | ||||
| Male (reference) | ||||
| Female | 0.98 | 0.59 | 1.64 | 0.9589 |
| Race/ethnicity | ||||
| Mexican American (reference) | ||||
| Other Hispanic | 1.42 | 0.76 | 2.66 | 0.4678 |
| Non-Hispanic White | 0.89 | 0.55 | 1.43 | 0.7176 |
| Non-Hispanic Black | 1.12 | 0.61 | 2.06 | 0.7702 |
| Other Race | 0.76 | 0.16 | 3.60 | 0.7890 |
| Alcohol use (No) | 0.55 | 0.29 | 1.06 | 0.3265 |
| BMI | 1.06 | 1.03 | 1.09 | 0.1617 |
| Marijuana/hashish use | 1.53 | 0.90 | 2.59 | 0.3589 |
| Cocaine/heroin/methamphetamine use | 0.74 | 0.41 | 1.34 | 0.0562 |
| Constant | 0.01 | 0.00 | 0.02 | 0.0676 |
| AIC = 416, Pseudo R-Square = 0.01 | ||||
| CKD Stages | ||||
|---|---|---|---|---|
| Sample Size = 4659 | Odds Ratio | OR 95% Confidence Interval | p-Value | |
| Toxoplasma IgG antibody (Positive) | 1.41 | 1.07 | 1.86 | 0.0424 |
| Age | ||||
| Younger (<45) (reference) | ||||
| Older (≥45) | 8.97 | 6.38 | 12.60 | <0.0001 |
| Gender | ||||
| Male (reference) | ||||
| Female | 1.32 | 1.10 | 1.60 | 0.0195 |
| Race/ethnicity | ||||
| Mexican American (reference) | ||||
| Other Hispanic | 0.95 | 0.65 | 1.40 | 0.8087 |
| Non-Hispanic White | 1.14 | 0.81 | 1.60 | 0.4615 |
| Non-Hispanic Black | 0.96 | 0.61 | 1.51 | 0.8650 |
| Other Race | 0.91 | 0.43 | 1.94 | 0.8250 |
| BMI | 1.04 | 1.01 | 1.06 | 0.0058 |
| Negative|Stage 1 | 0.13 | 0.02 | 0.69 | 0.0742 |
| Stage 1|Stage 2 | 0.15 | 0.08 | 0.26 | 0.0852 |
| Stage 2|Stage 3 | 0.18 | 0.13 | 0.27 | 0.1131 |
| Stage 3|Stage 4 | 3.68 | 3.13 | 4.32 | 0.2157 |
| Stage 4|Stage 5 | 18.25 | 12.39 | 26.86 | 0.0223 |
| CKD Levels | ||||
|---|---|---|---|---|
| Sample Size = 4659 | Odds Ratio | OR 95% Confidence Interval | p-Value | |
| Toxoplasma IgG antibody (Positive) | 1.23 | 0.93 | 1.63 | 0.1799 |
| Age | ||||
| Younger (<45) (reference) | ||||
| Older (≥45) | 2.94 | 2.17 | 3.97 | <0.0001 |
| Gender | ||||
| Male (reference) | ||||
| Female | 1.52 | 1.25 | 1.84 | 0.0027 |
| Race/ethnicity | ||||
| Mexican American (reference) | ||||
| Other Hispanic | 1.50 | 1.11 | 2.03 | 0.0297 |
| Non-Hispanic White | 2.25 | 1.79 | 2.83 | 0.0001 |
| Non-Hispanic Black | 0.96 | 0.61 | 1.51 | 0.8650 |
| Other Race | 1.53 | 1.10 | 2.12 | 0.8250 |
| BMI | 1.01 | 0.99 | 1.02 | 0.6051 |
| Mild|Negative | 0.10 | 0.06 | 0.16 | 0.0001 |
| Negative|Moderate-to-Severe | 76.14 | 70.78 | 81.90 | 0.0001 |
| CKD Levels | ||||
|---|---|---|---|---|
| Sample Size = 4659 | Odds Ratio | OR 95% Confidence Interval | p-Value | |
| Toxoplasma IgG antibody (Positive) | 1.42 | 1.07 | 1.90 | 0.0371 |
| Gender | ||||
| Male (reference) | ||||
| Female | 1.54 | 1.28 | 1.85 | 0.0011 |
| Race/ethnicity | ||||
| Mexican American (reference) | ||||
| Other Hispanic | 1.50 | 1.07 | 2.04 | 0.0417 |
| Non-Hispanic White | 2.78 | 2.16 | 3.58 | 0.0001 |
| Non-Hispanic Black | 1.34 | 0.86 | 2.12 | 0.2245 |
| Other Race | 1.53 | 1.10 | 2.12 | 0.8250 |
| BMI | 1.01 | 0.99 | 1.02 | 0.2861 |
| Mild|Negative | 0.08 | 0.05 | 0.14 | 0.0001 |
| Negative|Moderate-to-Severe | 50.53 | 47.75 | 53.48 | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babekir, A.; Mostafa, S.; Obeng-Gyasi, E. The Association of Toxoplasma gondii IgG Antibody and Chronic Kidney Disease Biomarkers. Microorganisms 2022, 10, 115. https://doi.org/10.3390/microorganisms10010115
Babekir A, Mostafa S, Obeng-Gyasi E. The Association of Toxoplasma gondii IgG Antibody and Chronic Kidney Disease Biomarkers. Microorganisms. 2022; 10(1):115. https://doi.org/10.3390/microorganisms10010115
Chicago/Turabian StyleBabekir, Amani, Sayed Mostafa, and Emmanuel Obeng-Gyasi. 2022. "The Association of Toxoplasma gondii IgG Antibody and Chronic Kidney Disease Biomarkers" Microorganisms 10, no. 1: 115. https://doi.org/10.3390/microorganisms10010115