Epidemiological Trends of Five Common Diarrhea-Associated Enteric Viruses Pre- and Post-Rotavirus Vaccine Introduction in Coastal Kenya

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Study Population Characteristics
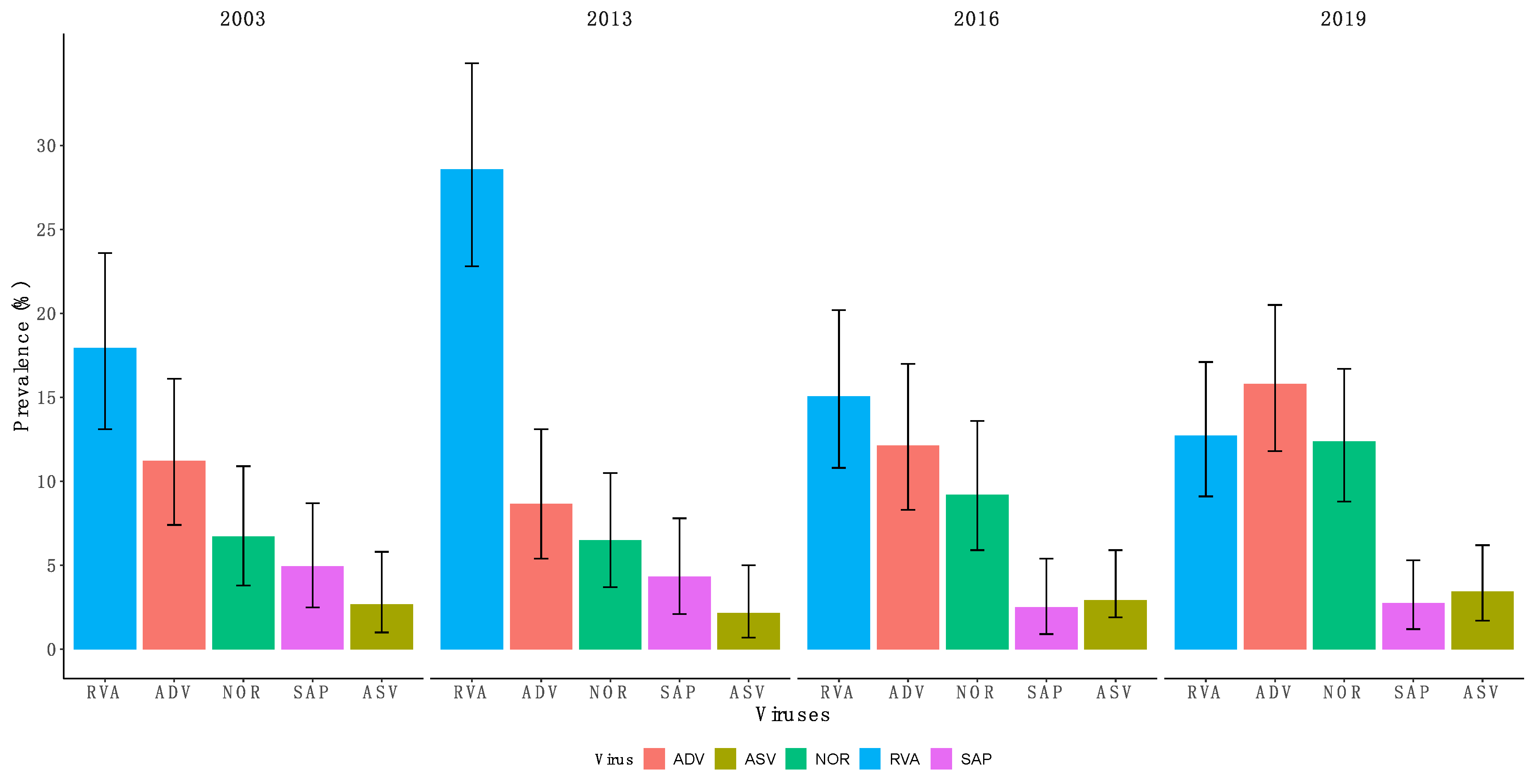
2.2. Overall Virus Detection
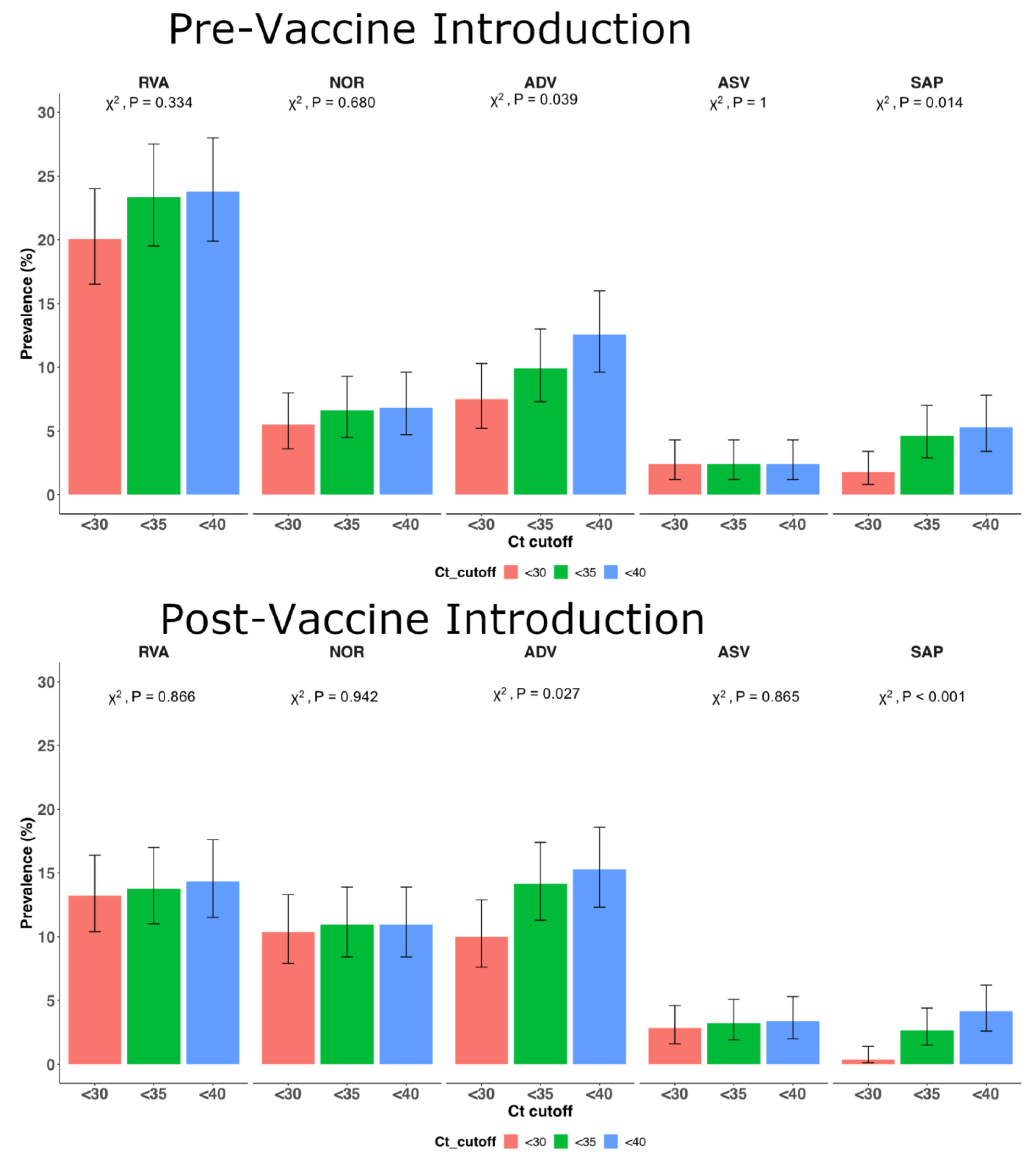
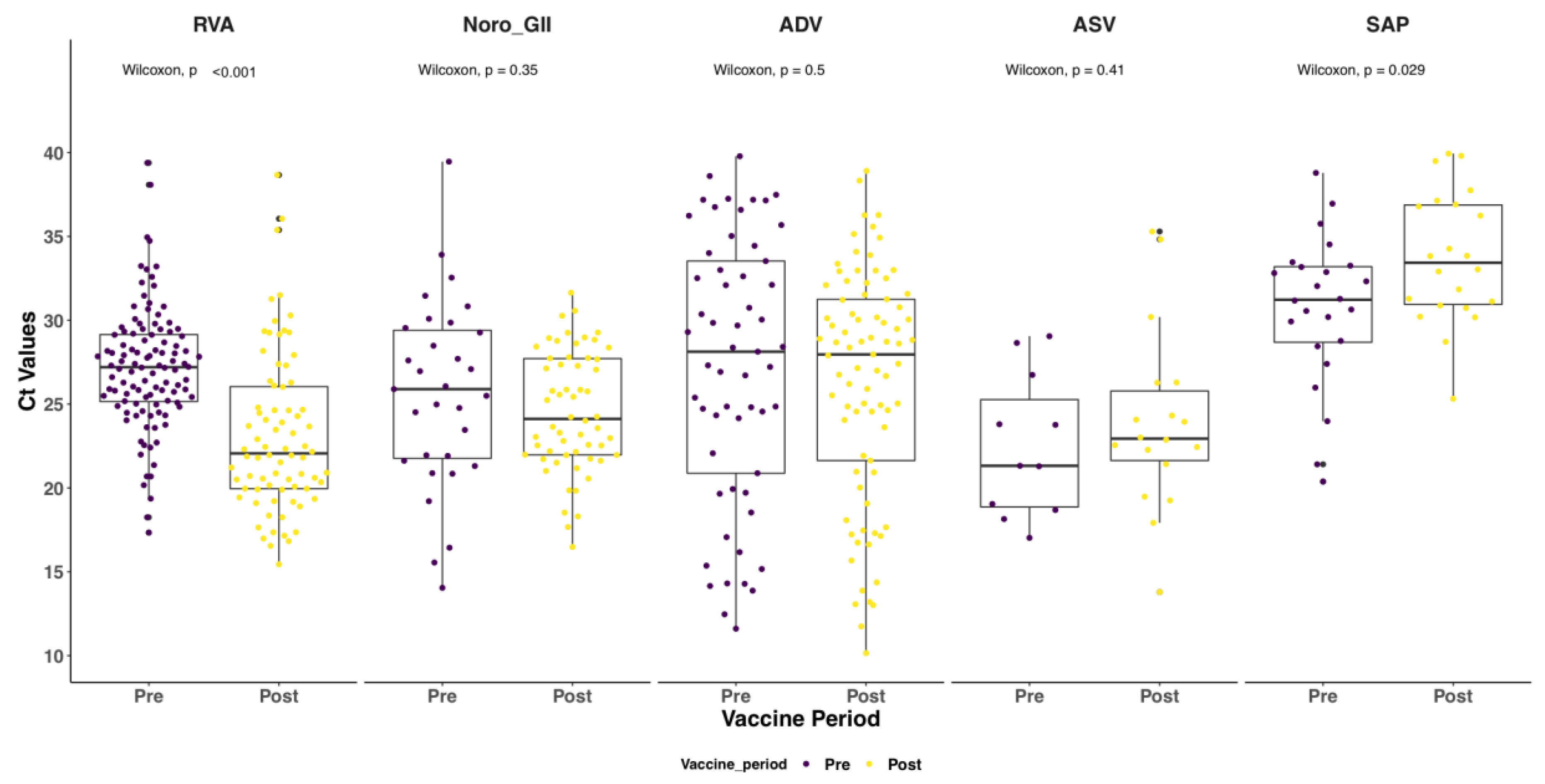
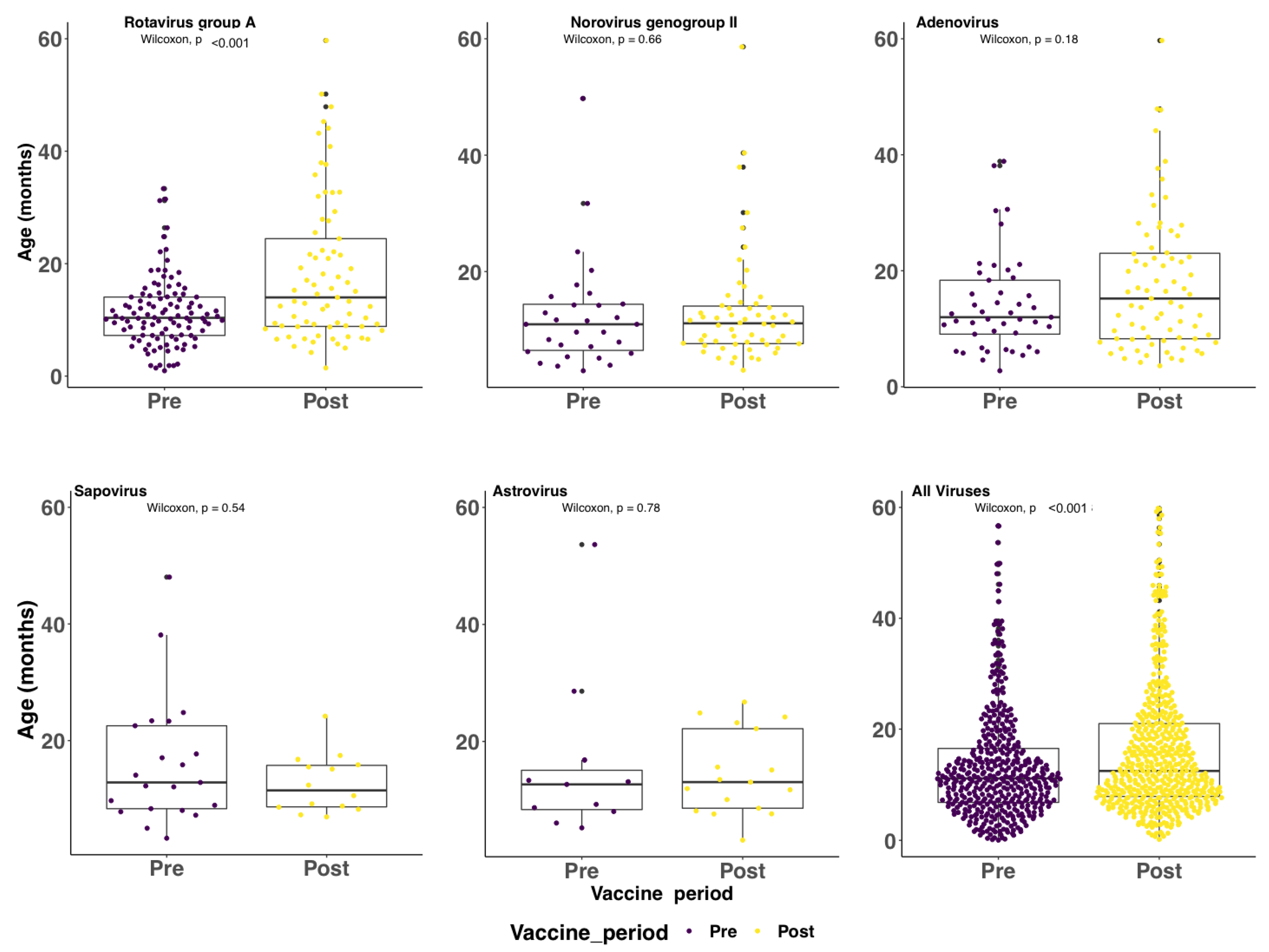
2.3. Patterns Pre-Post Vaccine Introduction
2.4. Virus Coinfections (i.e., Two or More Viruses in a Single Specimen)
2.5. Circulating RVA Genotypes Pre- and Post-Vaccine Introduction
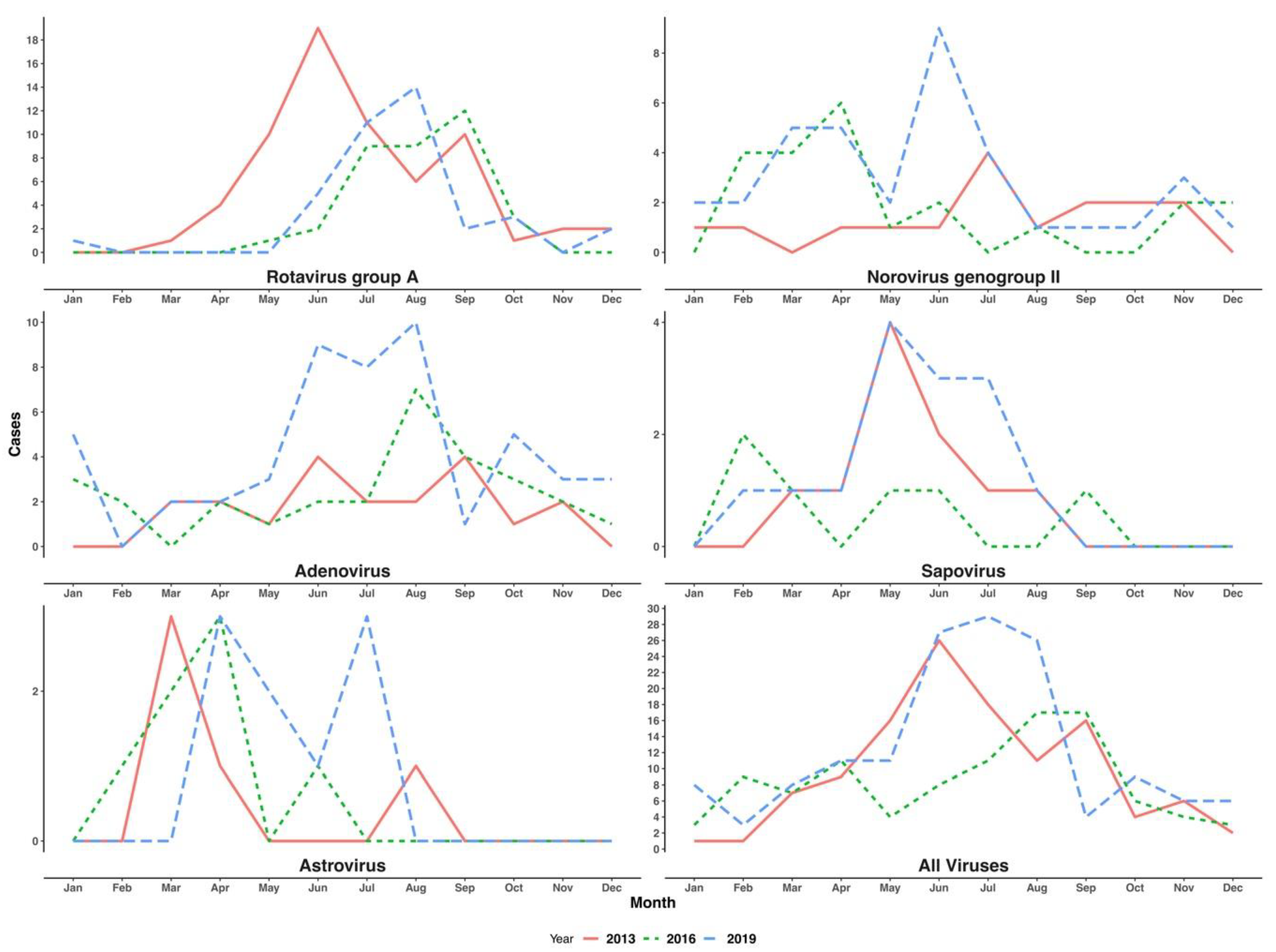
2.6. Seasonality of the Detected Viruses
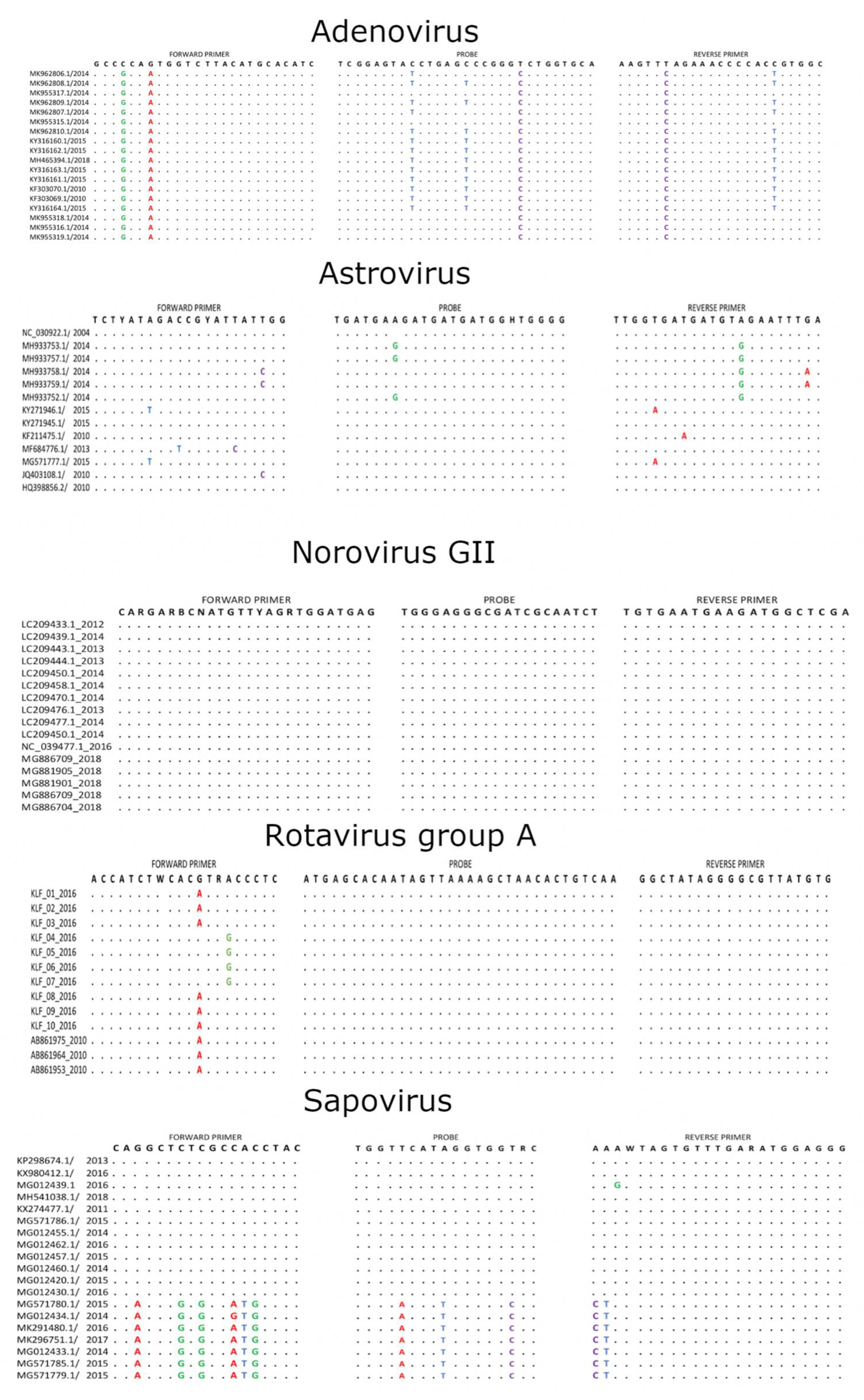
2.7. Primer/Probe Mismatches with Contemporary Sequences
3. Discussion
4. Materials and Methods
4.1. Study Site and Population
4.2. Laboratory Methods
4.3. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef] [Green Version]
- Platts-Mills, J.A.; Liu, J.; Rogawski, E.T.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R.; et al. Use of quantitative molecular diagnostic methods to assess the aetiology, burden, and clinical characteristics of diarrhoea in children in low-resource settings: A reanalysis of the MAL-ED cohort study. Lancet Glob. Health 2018, 6, e1309–e1318. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Platts-Mills, J.A.; Juma, J.; Kabir, F.; Nkeze, J.; Okoi, C.; Operario, D.J.; Uddin, J.; Ahmed, S.; Alonso, P.L.; et al. Use of quantitative molecular diagnostic methods to identify causes of diarrhoea in children: A reanalysis of the GEMS case-control study. Lancet 2016. [Google Scholar] [CrossRef]
- Aliabadi, N.; Antoni, S.; Mwenda, J.M.; Weldegebriel, G.; Biey, J.N.M.; Cheikh, D.; Fahmy, K.; Teleb, N.; Ashmony, H.A.; Ahmed, H.; et al. Global impact of rotavirus vaccine introduction on rotavirus hospitalisations among children under 5 years of age, 2008–2016: Findings from the Global Rotavirus Surveillance Network. Lancet Glob. Health 2019, 7, e893–e903. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.J.; Chen, S.Y.; Tsai, C.N.; Chao, H.C.; Kong, M.S.; Chang, Y.J.; Chiu, C.H. Long-term impact of suboptimal rotavirus vaccines on acute gastroenteritis in hospitalized children in Northern Taiwan. J. Formos. Med. Assoc. 2018, 117, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Muhsen, K.; Kassem, E.; Rubenstein, U.; Goren, S.; Ephros, M.; Shulman, L.M.; Cohen, D. No evidence of an increase in the incidence of norovirus gastroenteritis hospitalizations in young children after the introduction of universal rotavirus immunization in Israel. Hum. Vaccines Immunother. 2019, 15, 1284–1293. [Google Scholar] [CrossRef] [Green Version]
- Halasa, N.; Piya, B.; Stewart, L.S.; Rahman, H.; Payne, D.C.; Woron, A.; Thomas, L.; Constantine-Renna, L.; Garman, K.; McHenry, R.; et al. The Changing Landscape of Pediatric Viral Enteropathogens in the Post-Rotavirus Vaccine Era. Clin. Infect. Dis. 2020, 53, 1689–1699. [Google Scholar] [CrossRef]
- Wandera, E.A.; Mohammad, S.; Ouko, J.O.; Yatitch, J.; Taniguchi, K.; Ichinose, Y. Variation in rotavirus vaccine coverage by sub-counties in Kenya. Trop. Med. Health 2017. [Google Scholar] [CrossRef]
- Otieno, G.P.; Bottomley, C.; Khagayi, S.; Adetifa, I.; Ngama, M.; Omore, R.; Ogwel, B.; Owor, B.E.; Bigogo, G.; Ochieng, J.B.; et al. Impact of the Introduction of Rotavirus Vaccine on Hospital Admissions for Diarrhea Among Children in Kenya: A Controlled Interrupted Time-Series Analysis. Clin. Infect. Dis. 2019, 1–8. [Google Scholar] [CrossRef]
- Lewis, K. Vesikari Clinical Severity Scoring System Manual. Path. 2011, pp. 1–50. Available online: https://www.path.org/publications/files/VAD_vesikari_scoring_manual.pdf (accessed on 22 July 2020).
- Khagayi, S.; Omore, R.; Otieno, G.P.; Ogwel, B.; Ochieng, J.B.; Juma, J.; Apondi, E.; Bigogo, G.; Onyango, C.; Ngama, M.; et al. Effectiveness of monovalent rotavirus vaccine against hospitalization with acute rotavirus gastroenteritis in Kenyan children. Clin. Infect. Dis. 2020, 70, 2298–2305. [Google Scholar] [CrossRef] [Green Version]
- VIEW-hub, International Vaccine Access Center (IVAC), Johns Hopkins Bloomberg School of Public Health. Available online: https://view-hub.org/map/?set=wuenic-coverage&group=vaccine-coverage&category=rv (accessed on 31 July 2020).
- Bucardo, F.; Reyes, Y.; Svensson, L.; Nordgren, J. Predominance of norovirus and sapovirus in nicaragua after implementation of universal rotavirus vaccination. PLoS ONE 2014, 9, e98201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAtee, C.L.; Webman, R.; Gilman, R.H.; Mejia, C.; Bern, C.; Apaza, S.; Espetia, S.; Pajuelo, M.; Saito, M.; Challappa, R.; et al. Burden of norovirus and rotavirus in children after rotavirus vaccine introduction, Cochabamba, Bolivia. Am. Trop. Med. Hyg. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payne, D.C.; Vinjé, J.; Szilagyi, P.G.; Edwards, K.M.; Staat, M.A.; Weinberg, G.A.; Hall, C.B.; Chappell, J.; Bernstein, D.I.; Curns, A.T.; et al. Norovirus and medically attended gastroenteritis in US children. N. Engl. J. Med. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelaw, A.; Pietsch, C.; Liebert, U.G. Molecular epidemiology of rotaviruses in Northwest Ethiopia after national vaccine introduction. Infect. Genet. Evol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Rahajamanana, V.L.; Raboba, J.L.; Rakotozanany, A.; Razafindraibe, N.J.; Andriatahirintsoa, E.J.P.R.; Razafindrakoto, A.C.; Mioramalala, S.A.; Razaiarimanga, C.; Weldegebriel, G.G.; Burnett, E.; et al. Impact of rotavirus vaccine on all-cause diarrhea and rotavirus hospitalizations in Madagascar. Vaccine 2018. [Google Scholar] [CrossRef] [PubMed]
- Zeller, M.; Rahman, M.; Heylen, E.; De Coster, S.; De Vos, S.; Arijs, I.; Novo, L.; Verstappen, N.; Van Ranst, M.; Matthijnssens, J. Rotavirus incidence and genotype distribution before and after national rotavirus vaccine introduction in Belgium. Vaccine 2010. [Google Scholar] [CrossRef]
- Mwanga, M.J.; Owor, B.E.; Ochieng, J.B.; Ngama, M.H.; Ogwel, B.; Onyango, C.; Juma, J.; Njeru, R.; Gicheru, E.; Otieno, G.P.; et al. Rotavirus group A genotype circulation patterns across Kenya before and after nationwide vaccine introduction, 2010–2018. BMC Infect. Dis. 2020, 20, 504. [Google Scholar] [CrossRef]
- Pitzer, V.E.; Bilcke, J.; Heylen, E.; Crawford, F.W.; Callens, M.; De Smet, F.; Van Ranst, M.; Zeller, M.; Matthijnssens, J. Did Large-Scale Vaccination Drive Changes in the Circulating Rotavirus Population in Belgium? Sci. Rep. 2015, 5, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Talbert, A.; Ngari, M.; Bauni, E.; Mwangome, M.; Mturi, N.; Otiende, M.; Maitland, K.; Walson, J.; Berkley, J.A. Mortality after inpatient treatment for diarrhea in children: A cohort study. BMC Med. 2019. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Lopman, B.A.; Levy, K. A Systematic Review and Meta-Analysis of the Global Seasonality of Norovirus. PLoS ONE 2013, 8, e75922. [Google Scholar] [CrossRef]
- Dey, S.K.; Phathammavong, O.; Nguyen, T.D.; Thongprachum, A.; Chan-It, W.; Okitsu, S.; Mizuguchi, M.; Ushijima, H. Seasonal pattern and genotype distribution of sapovirus infection in Japan, 2003–2009. Epidemiol. Infect. 2012, 140, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Omore, R.; Tate, J.E.; O’Reilly, C.E.; Ayers, T.; Williamson, J.; Moke, F.; Schilling, K.A.; Awuor, A.O.; Jaron, P.; Ochieng, J.B.; et al. Epidemiology, seasonality and factors associated with rotavirus infection among children with moderate-to-severe diarrhea in rural western Kenya, 2008–2012: The Global Enteric Multicenter Study (GEMS). PLoS ONE 2016, 11, e0160060. [Google Scholar] [CrossRef] [PubMed]
- Vetter, M.R.; Staggemeier, R.; Vecchia, A.D.; Henzel, A.; Rigotto, C.; Spilki, F.R. Seasonal variation on the presence of adenoviruses in stools from non-diarrheic patients. Braz. J. Microbiol. 2015, 46, 749–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadhouders, R.; Pas, S.D.; Anber, J.; Voermans, J.; Mes, T.H.; Schutten, M. The effect of primer-template mismatches on the detection and quantification of nucleic acids using the 5′ nuclease assay. Mol. Diagn. 2010, 12, 109–117. [Google Scholar] [CrossRef]
- Lefever, S.; Pattyn, F.; Hellemans, J.; Vandesompele, J. Single-nucleotide polymorphisms and other mismatches reduce performance of quantitative PCR assays. Clin. Chem. 2013, 59, 1470–1480. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Gratz, J.; Amour, C.; Nshama, R.; Walongo, T.; Maro, A.; Mduma, E.; Platts-Mills, J.; Boisen, N.; Nataro, J.; et al. Optimization of quantitative PCR methods for enteropathogen detection. PLoS ONE 2016, 11, e0158199. [Google Scholar] [CrossRef] [Green Version]
- Bennett, S.; Gunson, R.N. The development of a multiplex real-time RT-PCR for the detection of adenovirus, astrovirus, rotavirus and sapovirus from stool samples. Virol. Methods 2017, 242, 30–34. [Google Scholar] [CrossRef]
- Van Maarseveen, N.M.; Wessels, E.; de Brouwer, C.S.; Vossen, A.C.; Claas, E.C. Diagnosis of viral gastroenteritis by simultaneous detection of Adenovirus group F, Astrovirus, Rotavirus group A, Norovirus genogroups I and II, and Sapovirus in two internally controlled multiplex real-time PCR assays. Clin. Virol. 2010. [Google Scholar] [CrossRef]
- Katoh, K.; Standley, D.M. MAFFT multiple sequence alignment software version 7: Improvements in performance and usability. Mol. Biol. Evol. 2013. [Google Scholar] [CrossRef] [Green Version]
- Magagula, N.B.; Esona, M.D.; Nyaga, M.M.; Stucker, K.M.; Halpin, R.A.; Stockwell, T.B.; Seheri, M.L.; Steele, A.D.; Wentworth, D.E.; Mphahlele, M.J. Whole genome analyses of G1P[8] rotavirus strains from vaccinated and non-vaccinated South African children presenting with diarrhea. Med. Virol. 2015, 87, 79–101. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 22 October 2019).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Subjects | Sampled (%) | Not Sampled (%) | p-Value |
|---|---|---|---|---|
| Total Admissions | 2156 | 1397 (64.8) | 759 (35.2) | |
| Admissions Per Year | ||||
| 2003 | 1007 (46.7) | 587 (42.0) | 420 (55.3) | |
| 2013 | 332 (15.4) | 254 (18.2) | 78 (10.3) | |
| 2016 | 334 (15.5) | 257 (18.4) | 77 (10.1) | |
| 2019 | 483 (22.4) | 299 (21.4) | 184 (24.2) | |
| Gender | 0.838 | |||
| Male | 1262 (58.5) | 815 (58.3) | 447 (58.9) | |
| Female | 894 (41.5) | 582 (41.7) | 312 (41.1) | |
| Age | ||||
| Median (IQR) | 12.4 (7.7–20.5) | 11.7 (7.4–19.7) | 13.8 (8.5–22.1) | <0.001 |
| Mean (SD) | 15.7 (11.4) | 15.0 (11.1) | 16.9 (12.0) | <0.001 |
| Age Group | 0.001 | |||
| 0–11 Months | 1045 (48.4) | 718 (51.4) | 326 (43.0) | |
| 12–23 Months | 716 (33.2) | 444 (31.8) | 272 (35.8) | |
| 24–59 Months | 396 (18.4) | 235 (16.8) | 161 (21.2) | |
| Discharge Outcome (n = 2153) # | <0.001 | |||
| Alive | 1918 (88.9) | 1306 (93.5) | 612 (80.5) | |
| Dead | 235 (10.9) | 89 (6.4) | 146 (19.3) |
| Characteristics | Total | Pre-Vaccine Introduction (%) | Post-Vaccine Introduction (%) | p-Value |
|---|---|---|---|---|
| Number of Samples Tested | 984 | 454 (46.1) | 530 (53.9) | |
| Samples Tested (Year) | ||||
| 2003 | 223 | 223 | - | |
| 2013 | 231 | 231 | - | |
| 2016 | 239 | - | 239 | |
| 2019 | 291 | - | 291 | |
| Gender | 0.847 | |||
| Male | 570 (57.9) | 261 (57.5) | 309 (58.3) | |
| Female | 414 (42.1) | 193 (42.5) | 221 (41.7) | |
| Age | ||||
| Mean (SD) | 15 (11.2) | 13.4 (9.9) | 16.3 (12) | <0.001 |
| Median (IQR) | 11.7 (7.3–19.3) | 11.2 (6.8–16.5) | 12.5 (7.9–21) | <0.001 |
| Age group | 0.003 | |||
| 0–11 Months | 505 (51.3) | 252 (55.5) | 253 (47.7) | |
| 12–23 Months | 323 (32.8) | 148 (32.6) | 175 (33.0) | |
| 24–59 Months | 156 (15.9) | 54 (11.9) | 102 (19.3) | |
| Disease Severity in RVA Cases = n (139) | ||||
| Mild | 12 (8.6) | 7 (10.6) | 5 (6.8) | 0.441 |
| Moderate | 50 (36.0) | 26 (39.4) | 24 (32.9) | |
| Severe | 77 (55.4) | 33 (50) | 44 (60.3) | |
| Discharge Outcome = n (982) # | 0.556 | |||
| Alive | 925 (94.2) | 425 (93.6) | 500 (94.7) | |
| Dead | 57 (5.8) | 29 (6.4) | 28 (5.3) |
| Viruses Detected | Total | Pre-Vaccine Introduction (%) | Post-Vaccine Introduction (%) | p-Value |
|---|---|---|---|---|
| Samples Tested | 984 | 454 (46.1) | 530 (53.9) | |
| Rotavirus Group A | 179 (18.2) | 106 (23.3) | 73 (13.8) | <0.001 |
| Adenovirus | 120 (12.2) | 45 (9.9) | 75 (14.2) | 0.053 |
| Norovirus GII | 88 (8.9) | 30 (6.6) | 58 (10.9) | 0.023 |
| Astrovirus | 28 (2.8) | 11 (2.4) | 17 (3.2) | 0.585 |
| Sapovirus | 35 (3.6) | 21 (4.6) | 14 (2.6) | 0.133 |
| PATHOGEN COINFECTION | PRE-VACCINE INTRODUCTION | POST-VACCINE INTRODUCTION |
|---|---|---|
| RVA & NOR GII | 1 | 2 |
| RVA & ADV | 2 | 15 |
| RVA & ASV | 3 | 0 |
| RVA & SAP | 6 | 1 |
| NOR GII& ADV | 3 | 4 |
| NOR GII & ASV | 0 | 1 |
| NOVGII & SAP | 2 | 1 |
| ADV & ASV | 1 | 3 |
| ADV & SAP | 1 | 1 |
| ASV & SAP | 1 | 2 |
| Year | 2003 | 2013 | 2016 | 2019 | ||||
|---|---|---|---|---|---|---|---|---|
| No. of Cases | % | No. of Cases | % | No. of Cases | % | No. of Cases | % | |
| RVA Positive | 40 | 66 | 36 | 37 | ||||
| Genotyped | 2 | 5.0 | 48 | 72.7 | 34 | 94.4 | 36 | 97.3 |
| Genotypes | ||||||||
| G1P[8] | 1 | 50.0 | 43 | 89.6 | 5 | 14.7 | 1 | 2.8 |
| G2P[4] | - | - | 2 | 4.2 | 29 | 85.3 | - | - |
| G3P[8] | - | - | 1 | 2.1 | - | - | 34 | 94.4 |
| G9P[8] | 1 | 50.0 | 1 | 2.1 | - | - | - | - |
| G10P[8] | - | - | 1 | 2.1 | - | - | - | - |
| G8P[8] | - | - | - | - | - | - | 1 | 2.8 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambisia, A.W.; Onchaga, S.; Murunga, N.; Lewa, C.S.; Nyanjom, S.G.; Agoti, C.N. Epidemiological Trends of Five Common Diarrhea-Associated Enteric Viruses Pre- and Post-Rotavirus Vaccine Introduction in Coastal Kenya. Pathogens 2020, 9, 660. https://doi.org/10.3390/pathogens9080660
Lambisia AW, Onchaga S, Murunga N, Lewa CS, Nyanjom SG, Agoti CN. Epidemiological Trends of Five Common Diarrhea-Associated Enteric Viruses Pre- and Post-Rotavirus Vaccine Introduction in Coastal Kenya. Pathogens. 2020; 9(8):660. https://doi.org/10.3390/pathogens9080660
Chicago/Turabian StyleLambisia, Arnold W., Sylvia Onchaga, Nickson Murunga, Clement S. Lewa, Steven Ger Nyanjom, and Charles N. Agoti. 2020. "Epidemiological Trends of Five Common Diarrhea-Associated Enteric Viruses Pre- and Post-Rotavirus Vaccine Introduction in Coastal Kenya" Pathogens 9, no. 8: 660. https://doi.org/10.3390/pathogens9080660