No-Touch Automated Room Disinfection after Autopsies of Exhumed Corpses

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
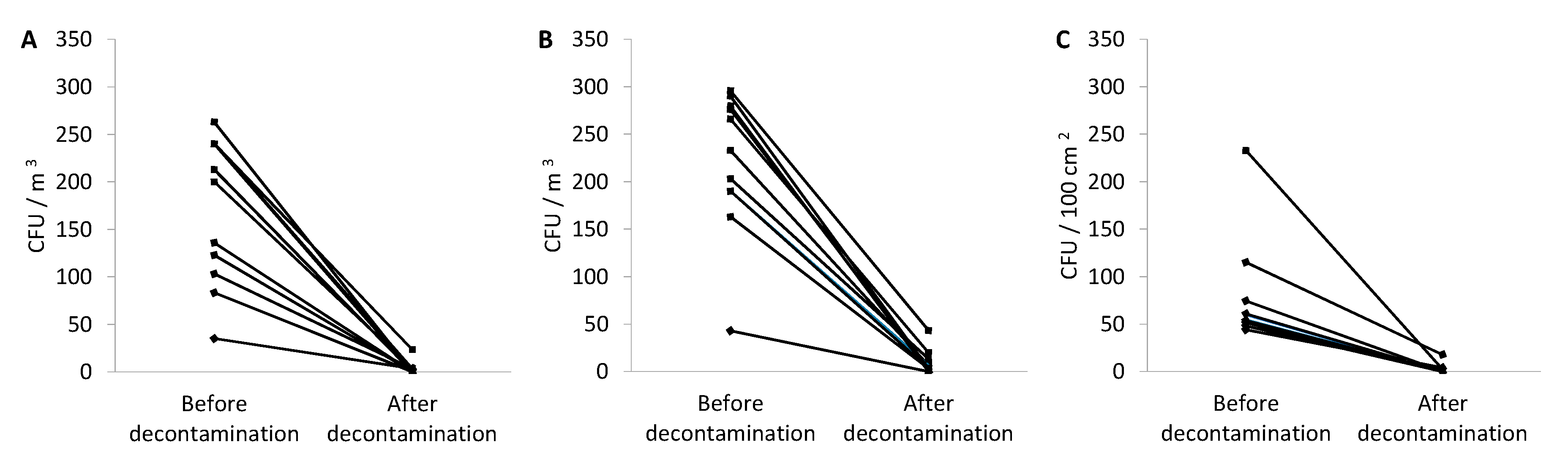
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Device
4.3. Microbiological Studies
Author Contributions
Funding
Conflicts of Interest
References
- Nolte, K.B.; Taylor, D.G.; Richmond, J.Y. Biosafety considerations for autopsy. Am. J. Forensic Med. Pathol. 2002, 23, 107–122. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, L.; Byard, R.W. Issues in the handling of cases of tuberculosis in the mortuary. J. Forensic Leg. Med. 2019, 64, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Gu, J.; Shi, X.; Gong, E.; Li, X.; Shao, H.; Shi, X.; Jiang, H.; Gao, X.; Cheng, D.; et al. Biosafety Level 3 Laboratory for Autopsies of Patients with Severe Acute Respiratory Syndrome: Principles, Practices, and Prospects. Clin. Infect. Dis. 2005, 41, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Brooks, E.G.; Utley-Bobak, S.R. Autopsy Biosafety. Acad. Forensic Pathol. 2018, 8, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, P.; Dannaoui, E.; Gehl, A.; Felske-Zech, H.; Birngruber, C.G.; Dettmeyer, R.B.; Verhoff, M.A. Molecular identification of fungi found on decomposed human bodies in forensic autopsy cases. Int. J. Leg. Med. 2015, 129, 785–791. [Google Scholar] [CrossRef]
- Łukaszuk, C.; Krajewska-Kułak, E.; Guzowski, A.; Kraszyńska, B.; Grassmann, M.; Dobrowolski, R. Analysis of the incidence fungi in a crypt cemetery. J. Air Waste Manag. Assoc. 2015, 65, 1141–1147. [Google Scholar] [CrossRef] [Green Version]
- Tarka, P.; Nitsch-Osuch, A.; Gorynski, P.; Tyszko, P.; Bogdan, M.; Kanecki, K. Epidemiology of Pulmonary Aspergillosis in Hospitalized Patients in Poland During 2009–2016. In Advances in Pulmonary Medicine: Research and Innovations; Pokorski, M., Ed.; Springer: Cham, Switzerland, 2019; Volume 1160, pp. 73–80. [Google Scholar] [CrossRef]
- Fu, X.; Guo, J.; Finkelbergs, D.; He, J.; Zha, L.; Guo, Y.; Cai, J. Fungal succession during mammalian cadaver decomposition and potential forensic implications. Sci. Rep. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Ishii, K.; Hitosugi, M.; Kido, M.; Yaguchi, T.; Nishimura, K.; Hosoya, T.; Tokudome, S. Analysis of fungi detected in human cadavers. Leg. Med. 2006, 8, 188–190. [Google Scholar] [CrossRef]
- Sri-indrasutdhi, V.; Ueapattanakit, J.; Sommatas, A. Investigation of airborne fungi and their ability to grow on formalin-fixed human cadavers. Mycosphere 2015, 6, 729–736. [Google Scholar] [CrossRef]
- Chimutsa, M.; Olakanye, A.O.; Thompson, T.J.U.; Ralebitso-Senior, T.K. Soil fungal community shift evaluation as a potential cadaver decomposition indicator. Forensic Sci. Int. 2015, 257, 155–159. [Google Scholar] [CrossRef] [Green Version]
- Burton, J.L. Health and safety at necropsy. J. Clin. Pathol. 2003, 56, 254–260. [Google Scholar] [CrossRef]
- Xu, X.; Goddard, W.A. Peroxone chemistry: Formation of H2O3 and ring-(HO2)(HO3) from O3/H2O2. Proc. Natl. Acad. Sci. USA 2002, 99, 15308–15312. [Google Scholar] [CrossRef] [Green Version]
- United States Environmental Protection Agency. Alternative Disinfectants and Oxidants Guidance Manual. 1999. Available online: https://nepis.epa.gov/Exe/ZyPDF.cgi/2000229L.PDF?Dockey=2000229L.PDF (accessed on 22 May 2020).
- Litter, M. Introduction to Photochemical Advanced Oxidation Processes for Water Treatment. In Environmental Photochemistry Part II; Boule, P., Bahnemann, D., Robertson, P., Eds.; Springer: Berlin/Heidelberg, Germany, 2005; ISBN 978-3-540-00269-7. [Google Scholar]
- Garvey, M.I.; Bradley, C.W.; Jumaa, P. Environmental decontamination following occupancy of a burns patient with multiple carbapenemase-producing organisms. J. Hosp. Infect. 2016, 93, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Blazejewski, C.; Wallet, F.; Rouzé, A.; Le Guern, R.; Ponthieux, S.; Salleron, J.; Nseir, S. Efficiency of hydrogen peroxide in improving disinfection of ICU rooms. Crit. Care 2015, 19, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donskey, C.J. Decontamination devices in health care facilities: Practical issues and emerging applications. Am. J. Infect. Control 2019, 47, A23–A28. [Google Scholar] [CrossRef] [PubMed]
- Steindl, G.; Fiedler, A.; Huhulescu, S.; Wewalka, G.; Allerberger, F. Effect of airborne hydrogen peroxide on spores of Clostridium difficile. Wien. Klin. Wochenschr. 2015, 127, 421–426. [Google Scholar] [CrossRef]
- Fu, T.Y.; Gent, P.; Kumar, V. Efficacy, efficiency and safety aspects of hydrogen peroxide vapour and aerosolized hydrogen peroxide room disinfection systems. J. Hosp. Infect. 2012, 80, 199–205. [Google Scholar] [CrossRef]
- Lowe, J.J.; Gibbs, S.G.; Iwen, P.C.; Smith, P.W.; Hewlett, A.L. Decontamination of a Hospital Room Using Gaseous Chlorine Dioxide: Bacillus anthracis, Francisella tularensis, and Yersinia pestis. J. Occup. Env. Hyg. 2013, 10, 533–539. [Google Scholar] [CrossRef]
- Moat, J.; Cargill, J.; Shone, J.; Upton, M. Application of a novel decontamination process using gaseous ozone. Can. J. Microbiol. 2009, 55, 928–933. [Google Scholar] [CrossRef]
- Munter, R. Advanced oxidation processes-current status and prospects. Proc. Est. Acad. Sci. Chem. 2001, 50, 59–80. [Google Scholar]
- Koburger, T.; Below, H.; Dornquast, T.; Kramer, A. Decontamination of room air and adjoining wall surfaces by nebulizing hydrogen peroxide. GMS Krankenhhyg. Interdiszip. 2011, 6, Doc09. [Google Scholar] [CrossRef] [PubMed]
- European Parliament. Directive 2000/54/EC of the European Parliament and of the Council of 18 September 2000 on the protection of workers from risks related to exposure to biological agents at work. Off. J. Eur. Commun. 2000, L262, 21–45. [Google Scholar]
- Hardin, N.J. Infection control at autopsy: A guide for pathologists and autopsy personnel. Curr. Diagn. Pathol. 2000, 6, 75–83. [Google Scholar] [CrossRef]
- Polish Committee for Standardization. Chemical Disinfectants and Antiseptics. Methods of Airborne Room Disinfection by Automated Process. Determination of Bactericidal, Mycobactericidal, Sporicidal, Fungicidal, Yeasticidal, Virucidal and Phagocidal Activities; EN 17272:2020. 2020. Available online: https://shop.bsigroup.com/ProductDetail?pid=000000000030374486 (accessed on 22 May 2020).
- Totaro, M.; Costa, A.; Casini, B.; Profeti, S.; Gallo, A.; Frendo, L.; Porretta, A.; Valentini, P.; Privitera, G.; Baggiani, A. Microbiological Air Quality in Heating, Ventilation and Air Conditioning Systems of Surgical and Intensive Care Areas: The Application of a Disinfection Procedure for Dehumidification Devices. Pathogens 2019, 8, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukutomi, Y.; Taniguchi, M. Sensitization to fungal allergens: Resolved and unresolved issues. Allergol. Int. 2015, 64, 321–331. [Google Scholar] [CrossRef] [Green Version]
- Kwon-Chung, K.J.; Sugui, J.A. Aspergillus fumigatus—What Makes the Species a Ubiquitous Human Fungal Pathogen? PLoS Pathog. 2013, 9, e1003743. [Google Scholar] [CrossRef]
- Hedayati, M.T.; Pasqualotto, A.C.; Warn, P.A.; Bowyer, P.; Denning, D.W. Aspergillus flavus: Human pathogen, allergen and mycotoxin producer. Microbiology 2007, 153, 1677–1692. [Google Scholar] [CrossRef] [Green Version]
- Baranyi, N.; Kocsubé, S.; Jakšić Despot, D.; Šegvić Klarić, M.; Szekeres, A.; Bencsik, O.; Kecskeméti, A.; Manikandan, P.; Tóth, B.; Kredics, L.; et al. Combined genotyping strategy reveals structural differences between Aspergillus flavus lineages from different habitats impacting human health. J. Basic Microbiol. 2017, 57, 899–909. [Google Scholar] [CrossRef]
- Desai, M.R.; Ghosh, S. Occupational exposure to airborne fungi among rice mill workers with special reference to aflatoxin producing A. flavus strains. Ann. Agric. Environ. Med. 2003, 10, 159–162. [Google Scholar]
- Kowalska, A.; Walkiewicz, K.; Kozieł, P.; Muc-Wierzgoń, M. Aflatoxins: Characteristics and impact on human health. Postepy Hig. Med. Dosw. 2017, 71, 315–327. [Google Scholar] [CrossRef]
- Kespohl, S.; Raulf, M. Mold Sensitization in Asthmatic and Non-asthmatic Subjects Diagnosed with Extract-Based Versus Component-Based Allergens. In Medical Science and Research; Pokorski, M., Ed.; Springer: Cham, Switzerland, 2019; Volume 1153. [Google Scholar]
- Zhang, Z.; Reponen, T.; Hershey, G.K. Fungal Exposure and Asthma: IgE and Non-IgE-Mediated Mechanisms. Curr. Allergy Asthma Rep. 2016, 16, 86. [Google Scholar] [CrossRef] [PubMed]
- Batra, N.; Kaur, H.; Mohindra, S.; Singh, S.; Shamanth, A.S.; Rudramurthy, S.M. Cladosporium Sphaerospermum Causing Brain Abscess, a Saprophyte Turning Pathogen: Case and Review of Published Reports. J. Mycol. Med. 2019, 29, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Perrone, G.; Susca, A. Penicillium Species and Their Associated Mycotoxins. In Mycotoxigenic Fungi. Methods in Molecular Biology; Moretti, A., Susca, A., Eds.; Humana Press: New York, NY, USA, 2017; Volume 1542, pp. 107–119. [Google Scholar]
- Ahmad, M.; Jacobs, D.; Wu, H.H.; Wolk, D.M.; Kazmi, S.A.J.; Jaramillo, C.; Toms, S.A. Cladophialophora Bantiana: A Rare Intracerebral Fungal Abscess—Case Series and Review of Literature. Surg. J. N. Y. 2017, 3, e62–e68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, C.; Xi, L.; Chaturvedi, V. Talaromycosis (Penicilliosis) Due to Talaromyces (Penicillium) marneffei: Insights into the Clinical Trends of a Major Fungal Disease 60 Years After the Discovery of the Pathogen. Mycopathologia 2019, 184, 709–720. [Google Scholar] [CrossRef] [PubMed]
- van de Voorde, H.; Van Dijck, P.J. Determination of the time of death by fungal growth. Z. Für Rechtsmed. 1982, 89, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Čavka, M.; Glasnović, A.; Janković, I.; Šikanjić, P.R.; Perić, B.; Brkljačić, B.; Mlinarić-Missoni, E.; Škrlin, J. Microbiological analysis of a mummy from the archeological museum in Zagreb. Coll. Antropol. 2010, 34, 803–805. [Google Scholar]
- Hitosugi, M.; Ishii, K.; Yaguchi, T.; Chigusa, Y.; Kurosu, A.; Kido, M.; Nagai, T.; Tokudome, S. Fungi can be a useful forensic tool. Leg. Med. 2006, 8, 240–242. [Google Scholar] [CrossRef]
- Sidrim, J.J.C.; Moreira Filho, R.E.; Cordeiro, R.A.; Rocha, M.F.G.; Caetano, E.P.; Monteiro, A.J.; Brilhante, R.S.N. Fungal microbiota dynamics as a postmortem investigation tool: Focus on Aspergillus, Penicillium and Candida species. J. Appl. Microbiol. 2010, 108, 1751–1756. [Google Scholar] [CrossRef]
- Polish Committee for Standardization. Workplace Atmosphere—Guidelines for Measurement of Airborne Microorganisms and Endotoxins; PN-EN 13098:2007. Available online: http://normy.ekoinfonet.pl/ics.php?ic=07&kat=Powietrze%20na%20stanowiskach%20pracy (accessed on 22 May 2020).
- European Committee for Standardization. CEN/TC 243—Cleanroom Technology. 1993. Available online: https://standards.iteh.ai/catalog/tc/cen/9f58539c-5394-4f44-afe3-8528a2e35e33/cen-tc-243 (accessed on 22 May 2020).
- de Hoog, G.; Guarro, J.; Gené, J.; Figueras, M. Atlas of Clinical Fungi, 3rd ed.; CBS-KNAW Fungal Biodiversity Centre: Utrecht, The Netherlands, 2009. [Google Scholar]


{kind=link}
| Oxidative Agent | Redox Potential (V) |
|---|---|
| Hydroxyl radical •HO | 2.80 |
| Molecular oxygen O2 | 2.42 |
| Ozone in the acidic environment | 2.07 |
| Hydrogen peroxide in the acidic environment (H2O2/H) | 1.78 |
| Manganese ion (VII) in the acidic environment | 1.69 |
| Chloride dioxide | 1.57 |
| Chloride | 1.36 |
| Bacteria | Fungi † |
|---|---|
| Bacillus simplex Bacillus vallismortis Enhydrobacter aerosaccus Gordonia sputi Kocuria rhizophila Kocuria rosea Kytococcus scedentarius Micrococcus luteus Moraxella osloensis Paenibacillus lantus Paenibacillus pabuli Paracoccus yeei Psychrobacter phenylpruvicus Staphylococcus auricularis Staphylococcus cohnii spp. Staphylococcus epidermidis Staphylococcus equorum Staphylococcus haemolyticus Staphylococcus hominis Staphylococcus pettekoferii Staphylococcus warneri Truicella otitidis | Alternaria spp. (1) Aspergillus flavus (2) Aspergillus fumigatus (2) Aspergillus niger (1) Chaetomium spp. (1) Cladosporium spp. (≤3) Fusarium spp. (1) Oidiodendron spp. (1) Penicillium citrinum (1) Penicillium spp. (≤3) Rhizopus spp. (1) Scopulariopsis spp. (1) Trichoderma spp. (1) |
| Dissecting Table | The Working Surface of the Dissecting Table | Floor | The Working Surface of Tools Trolley | Sitting Surface of the Chair | ||
|---|---|---|---|---|---|---|
| Autopsy 1 | Before | 32 (2) | 48 (2) | 92 (2) | 40 (2) | 28 (2) |
| After | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Autopsy 2 | Before | 76 (2) | 20 (2) | 128 (3) | 20 (2) | 12 (2) |
| After | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Autopsy 3 | Before | 200 (3) | 20 (2) | 24 (2) | 4 (1) | 24 (2) |
| After | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Autopsy 4 | Before | 120 (3) | 44 (2) | 32 (2) | 60 (2) | 44 (2) |
| After | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Autopsy 5 | Before | 108 (3) | 12 (2) | 32 (2) | 52 (2) | 16 (2) |
| After | 8 (1) | 4 (1) | 0 (0) | 0 (0) | 8 (1) | |
| Autopsy 6 | Before | 128 (3) | 24 (2) | 88 (2) | 60 (2) | 4 (1) |
| After | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Autopsy 7 | Before | 400 (3) | 60 (2) | 48 (2) | 40 (2) | 28 (2) |
| After | 0 (0) | 24 (2) | 25 (2) | 24 (2) | 16 (2) | |
| Autopsy 8 | Before | 140 (3) | 16 (2) | 108 (3) | 88 (2) | 20 (2) |
| After | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Autopsy 9 | Before | 800 (3) | 68 (2) | 108 (3) | 136 (3) | 52 (2) |
| After | 4 (1) | 4 (1) | 4 (1) | 0 (0) | 0 (0) | |
| Autopsy 10 | Before | 120 (3) | 36 (2) | 116 (3) | 40 (2) | 60 |
| After | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Autopsy 11 | Before | 144 (3) | 20 (2) | 64 (2) | 32 (2) | 8 (1) |
| After | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarka, P.; Borowska-Solonynko, A.; Brzozowska, M.; Nitsch-Osuch, A.; Kanecki, K.; Kuthan, R.; Garczewska, B. No-Touch Automated Room Disinfection after Autopsies of Exhumed Corpses. Pathogens 2020, 9, 648. https://doi.org/10.3390/pathogens9080648
Tarka P, Borowska-Solonynko A, Brzozowska M, Nitsch-Osuch A, Kanecki K, Kuthan R, Garczewska B. No-Touch Automated Room Disinfection after Autopsies of Exhumed Corpses. Pathogens. 2020; 9(8):648. https://doi.org/10.3390/pathogens9080648
Chicago/Turabian StyleTarka, Patryk, Aleksandra Borowska-Solonynko, Małgorzata Brzozowska, Aneta Nitsch-Osuch, Krzysztof Kanecki, Robert Kuthan, and Barbara Garczewska. 2020. "No-Touch Automated Room Disinfection after Autopsies of Exhumed Corpses" Pathogens 9, no. 8: 648. https://doi.org/10.3390/pathogens9080648