Severe Clinical Outcomes of Tuberculosis in Kharkiv Region, Ukraine, Are Associated with Beijing Strains of Mycobacterium tuberculosis

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
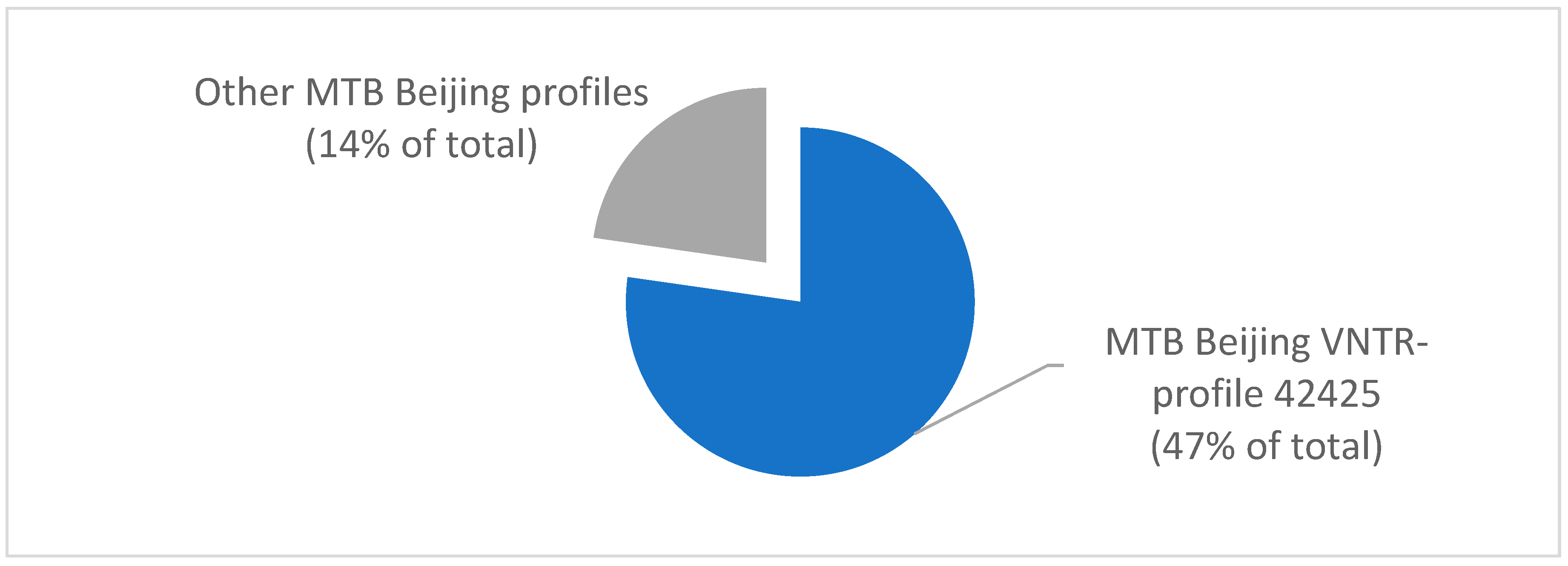
2.1. Dominant Genotypes of M. tuberculosis in TB Cases in Kharkiv Region, Ukraine
2.2. Analysis of Risk Factors for Severe TB Outcomes
2.3. Effectiveness of Treatment
2.4. Tuberculosis Co-Infection and Strain Replacement
3. Discussion
4. Materials and Methods
4.1. Tuberculosis Cases, Clinical Data and Exclusion Criteria
4.2. Drug Susceptibility Testing, ETR and MIRU-VNTR Genotyping
4.3. Biostatistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Organisation Mondiale de la Santé. Global Tuberculosis Report 2016; Organisation Mondiale de la Santé: Geneva, Switzerland, 2016; ISBN 978-92-4-156539-4. [Google Scholar]
- Dudnyk, A.; Rzhepishevska, O.; Rogach, K.; Kutsyna, G.; Lange, C. Multidrug-resistant tuberculosis in Ukraine at a time of military conflict. Int. J. Tuberc. Lung Dis. 2015, 19, 492–493. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of Ukraine. Order #620. Unified Clinical Protocol of the Primary, Secondary (Specialized) and Third (High—Specialized) Medical Help for Adults: Tuberculosis. 2014. Available online: https://apps.who.int/iris/bitstream/handle/10665/58717/WHO_TB_94.179.pdf;jsessionid=369B4976AC6B7AD8E7EC7E663FC5AD16?sequence=1 (accessed on 10 June 2019).
- Rodríguez-Castillo, J.G.; Pino, C.; Niño, L.F.; Rozo, J.C.; Llerena-Polo, C.; Parra-López, C.A.; Tauch, A.; Murcia-Aranguren, M.I. Comparative genomic analysis of Mycobacterium tuberculosis Beijing-like strains revealed specific genetic variations associated with virulence and drug resistance. Infect. Genet. Evol. 2017, 54, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wan, B.; Zhou, A.; Ni, J.; Xu, Z.; Li, S.; Tao, J.; Yao, Y. Whole genome analysis of an MDR Beijing/W strain of Mycobacterium tuberculosis with large genomic deletions associated with resistance to isoniazid. Gene 2016, 582, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Garzelli, C.; Lari, N.; Rindi, L. Genomic diversity of Mycobacterium tuberculosis Beijing strains isolated in Tuscany, Italy, based on large sequence deletions, SNPs in putative DNA repair genes and MIRU-VNTR polymorphisms. Tuberculosis 2016, 97, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Almeida, F.M.; Ventura, T.L.B.; Amaral, E.P.; Ribeiro, S.C.M.; Calixto, S.D.; Manhães, M.R.; Rezende, A.L.; Souzal, G.S.; de Carvalho, I.S.; Silva, E.C.; et al. Hypervirulent Mycobacterium tuberculosis strain triggers necrotic lung pathology associated with enhanced recruitment of neutrophils in resistant C57BL/6 mice. PLoS ONE 2017, 12, e0173715. [Google Scholar] [CrossRef]
- Merker, M.; Blin, C.; Mona, S.; Duforet-Frebourg, N.; Lecher, S.; Willery, E.; Blum, M.G.B.; Rüsch-Gerdes, S.; Mokrousov, I.; Aleksic, E.; et al. Evolutionary history and global spread of the Mycobacterium tuberculosis Beijing lineage. Nat. Genet. 2015, 47, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Glynn, J. National Institute for Public Health and the Environment (RIVM) European Concerted Action on New Generation Genetic Markers and Techniques for the Epidemiology and Control of Tuberculosis. Beijing/W Genotype Mycobacterium tuberculosis and Drug Resistance. Emerg. Infect. Dis. 2006, 12, 736–743. [Google Scholar] [CrossRef]
- Eldholm, V.; Pettersson, J.H.-O.; Brynildsrud, O.B.; Kitchen, A.; Rasmussen, E.M.; Lillebaek, T.; Rønning, J.O.; Crudu, V.; Mengshoel, A.T.; Debech, N.; et al. Armed conflict and population displacement as drivers of the evolution and dispersal of Mycobacterium tuberculosis. Proc. Natl. Acad. Sci. USA 2016, 113, 13881–13886. [Google Scholar] [CrossRef]
- Kontsevaya, I.; Nikolayevskyy, V.; Kovalyov, A.; Ignatyeva, O.; Sadykhova, A.; Simak, T.; Tikhonova, O.; Dubrovskaya, Y.; Vasiliauskiene, E.; Davidaviciene, E.; et al. Tuberculosis cases caused by heterogeneous infection in Eastern Europe and their influence on outcomes. Infect. Genet. Evol. 2017, 48, 76–82. [Google Scholar] [CrossRef]
- Krüüner, A.; Pehme, L.; Ghebremichael, S.; Koivula, T.; Hoffner, S.E.; Mikelsaar, M. Use of molecular techniques to distinguish between treatment failure and exogenous reinfection with Mycobacterium tuberculosis. Clin. Infect. Dis. 2002, 35, 146–155. [Google Scholar] [CrossRef]
- Cohen, T.; Van Helden, P.D.; Wilson, D.; Colijn, C.; McLaughlin, M.M.; Abubakar, I.; Warren, R.M. Mixedstrain Mycobacterium tuberculosis infections and the implications for tuberculosis treatment and control. Clin. Microbiol. Rev. 2012, 24, 708–719. [Google Scholar] [CrossRef] [PubMed]
- Kajunguri, D. Modelling the Impact of TB Superinfection on the Dynamics of HIV-TB Coinfection. Master’s Thesis, University of Stellenbosch, Stellenbosch, South Africa, 2009. [Google Scholar]
- Hofmann-Thiel, S.; van Ingen, J.; Feldmann, K.; Turaev, L.; Uzakova, G.T.; Murmusaeva, G.; van Soolingen, D.; Hoffmann, H. Mechanisms of heteroresistance to isoniazid and rifampin of Mycobacterium tuberculosis in Tashkent, Uzbekistan. Eur. Respir. J. 2009, 33, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Allix-Beguec, C.; Harmsen, D.; Weniger, T.; Supply, P.; Niemann, S. Evaluation and Strategy for use of MIRU-VNTRplus, a multifunctional database for online analysis of genotyping data and phylogenetic identification of Mycobacterium tuberculosis complex isolates. J. Clin. Microbiol. 2008, 46, 2692–2699. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Definitions and Reporting Framework for Tuberculosis; 2013 Revision; (WHO/HTM/TB/2013.2); World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Mansoori, N.; Yaseri, M.; Vaziri, F.; Douraghi, M. Genetic diversity of Mycobacterium tuberculosis complex isolates circulating in an area with high tuberculosis incidence: Using 24-locus MIRU-VNTR method. Tuberculosis 2018, 112, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Erie, H.; Kaboosi, H.; Javid, N.; Shirzad-Aski, H.; Taziki, M.; Kuchaksaraee, M.B.; Ghaemi, E.A. The high prevalence of Mycobacterium tuberculosis Beijing strain at an early age and extra-pulmonary tuberculosis cases. Iran. J. Microbiol. 2017, 9, 312–317. [Google Scholar]
- Cha, S.B.; Kim, W.S.; Kim, J.-S.; Kim, H.; Kwon, K.W.; Han, S.J.; Cho, S.-N.; Coler, R.N.; Reed, S.G.; Shin, S.J. Pulmonary immunity and durable protection induced by the ID93/GLA-SE vaccine candidate against the hyper-virulent Korean Beijing Mycobacterium tuberculosis strain K. Vaccine 2016, 34, 2179–2187. [Google Scholar] [CrossRef] [PubMed]
- Bainomugisa, A.; Duarte, T.; Lavu, E.; Pandey, S.; Coulter, C.; Marais, B.J.; Coin, L.M. A complete high-quality MinION nanopore assembly of an extensively drug-resistant Mycobacterium tuberculosis Beijing lineage strain identifies novel variation in repetitive PE/PPE gene regions. Microb. Genom. 2018, 4, e000188. [Google Scholar] [CrossRef]
- Amaral, E.P.; Machado de Salles, É.; Barbosa Bomfim, C.C.; Salgado, R.M.; Almeida, F.M.; de Souza, P.C.; Alvarez, J.M.; Hirata, M.H.; Lasunskaia, E.B.; D’Império-Lima, M.R. Inhibiting adenosine receptor signaling promotes accumulation of effector CD4+ T cells in the lung parenchyma during severe tuberculosis. J. Infect. Dis. 2018, 219, 964–974. [Google Scholar] [CrossRef]
- Dunlap, M.D.; Howard, N.; Das, S.; Scott, N.; Ahmed, M.; Prince, O.; Rangel-Moreno, J.; Rosa, B.A.; Martin, J.; Kaushal, D.; et al. A novel role for C-C motif chemokine receptor 2 during infection with hypervirulent Mycobacterium tuberculosis. Mucosal Immunol. 2018, 11, 1727. [Google Scholar] [CrossRef]
- Wang, F.; Shao, L.; Fan, X.; Shen, Y.; Diao, N.; Jin, J.; Sun, F.; Wu, J.; Chen, J.; Weng, X.; et al. Evolution and transmission patterns of extensively drug-resistant tuberculosis in China. Antimicrob. Agents Chemother. 2015, 59, 818–825. [Google Scholar] [CrossRef]
- Mai, T.Q.; Martinez, E.; Menon, R.; Van Anh, N.T.; Hien, N.T.; Marais, B.J.; Sintchenko, V. Mycobacterium tuberculosis drug resistance and transmission among Human Immunodeficiency Virus-infected patients in Ho Chi Minh City, Vietnam. Am. J. Trop. Med. Hyg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhao, Q.; Werngren, J.; Hoffner, S.; Diwan, V.K.; Xu, B. Drug resistance characteristics and cluster analysis of M. tuberculosis in Chinese patients with multiple episodes of anti-tuberculosis treatment. BMC Infect. Dis. 2016, 16, 4. [Google Scholar] [CrossRef] [PubMed]
- Vasylyeva, T.I.; Liulchuk, M.; Friedman, S.R.; Sazonova, I.; Faria, N.R.; Katzourakis, A.; Babii, N.; Scherbinska, A.; Thézé, J.; Pybus, O.G.; et al. Molecular epidemiology reveals the role of war in the spread of HIV in Ukraine. Proc. Natl. Acad. Sci. USA 2018, 115, 1051–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mai, T.Q.; Van Anh, N.T.; Hien, N.T.; Lan, N.H.; Giang, D.C.; Hang, P.T.T.; Lan, N.T.N.; Marais, B.J.; Sintchenko, V. Drug resistance and Mycobacterium tuberculosis strain diversity in TB/HIV co-infected patients in Ho Chi Minh city, Vietnam. J. Glob. Antimicrob. Resist. 2017, 10, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Eurosurveillance Editorial Team. WHO revised definitions and reporting framework for tuberculosis. Euro Surveill. 2013, 18, 20455. [Google Scholar]
- Frothingham, R.; Meeker-O’Connell, W.A. Genetic diversity in the Mycobacterium tuberculosis complex based on variable numbers of tandem DNA repeats. Microbiology 1998, 144, 1189–1196. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Strain 42425, n = 102 | Other Strains, n = 113 | F | p | |||
|---|---|---|---|---|---|---|
| Associated Factors | n | % | n | % | ||
| Treatment Adherence | 46 | 45% | 69 | 61% | 5.53 | 0.0198 |
| Alcoholism | 58 | 57% | 46 | 41% | 5.65 | 0.0200 |
| Drug Addiction | 19 | 19% | 7 | 6% | 8.13 | 0.0040 |
| HIV Positive Status | 17 | 17% | 5 | 4% | 9.33 | 0.0019 |
| Strain 42425, n = 102 | Other Strains, n = 113 | F | p | |||
|---|---|---|---|---|---|---|
| Outcome | n | % | n | % | ||
| Cured | 11 | 11% | 25 | 22% | 5.16 | 0.0323 |
| Treatment Completed | 13 | 13% | 38 | 34% | 13.79 | 0.0151 |
| Treatment Failed | 31 | 30% | 18 | 16% | 6.44 | 0.0098 |
| Lost to Follow-up | 13 | 13% | 11 | 10% | 0.49 | 0.4900 |
| Death | 34 | 33% | 21 | 19% | 6.18 | 0.0198 |
| Overall Treatment Effectiveness | 24 | 21% | 63 | 56% | 29.69 | 0.0001 |
| Before Treatment | After 1 Month of Treatment | After 3 Months of Treatment | After 8 Months of Treatment | |
|---|---|---|---|---|
| 1 | URAL (52423) | LAM (42522) | LAM (42522) | LAM (42522) |
| 2 | LAM (32221) | LAM (32221) | LAM (42522) | LAM (42522) |
| 3 | Haarlem (22525) | LAM (42522) | LAM (42522) | LAM (42522) |
| 4 | Haarlem (31423) | Beijing (42425) | Beijing (42425) | Beijing (42425) |
| 5 | LAM (22423) | LAM (22423) | LAM (22222) | LAM (22222) |
| 6 | URAL (52423) | Beijing (42425) | Beijing (42425) | Beijing (42425) |
| 7 | Beijing (42425) | LAM (22222) | Beijing (42425) | Beijing (42425) |
| 8 | Beijing (42425) | Beijing (42425) | LAM (22222) | LAM (22222) |
| 9 | URAL (52423) | LAM (22222) | LAM (22222) | LAM (22222) |
| 10 | Haarlem (31423) | Beijing (42425) | Beijing (42425) | Beijing (42425) |
| Locus | Type | Primer Sequence | t | Formula |
|---|---|---|---|---|
| MIRU26 | F | TAGGTCTACCGTCGAAATCTGTGAC | 60 °C | (n-234)/51 |
| R | CATAGGCGACCAGGCGAATAG | |||
| MIRU40 | F | GGGTTGCTGGATGACAACGTGT | 60°C | (n-354)/54 |
| R | GGGTGATCTCGGCGAAATCAGATA | |||
| MIRU10 | F | GTTCTTGACCAACTGCAGTCGTCC | 62 °C | (n-484)/53 |
| R | GCCACCTTGGTGATCAGCTACCT | |||
| MIRU16 | F | TCGGTGATCGGGTCCAGTCCAAGTA | 62 °C | (n-565)/53 |
| R | CCCGTCGTGCAGCCCTGGTAC | |||
| Mtub04 | F | CTTGGCCGGCATCAAGCGCATTATT | 62 °C | (n-537)/51 |
| R | GGCAGCAGAGCCCGGGATTCTTC | |||
| Mtub30 | F | CTTGAAGCCCCGGTCTCATCTGT | 62 °C | (n-247)/58 |
| R | ACTTGAACCCCCACGCCCATTAGTA | |||
| Mtub39 | F | CGGTGGAGGCGATGAACGTCTTC | 62 °C | (n-272)/58 |
| R | TAGAGCGGCACGGGGGAAAGCTTAG | |||
| QUB4156 | F | TGACCACGGATTGCTCTAGT | 52 °C | (n-563)/59 |
| R | GCCGGCGTCCATGTT | |||
| Mtub39 | F | CGGTGGAGGCGATGAACGTCTTC | 62 °C | (n-272)/58 |
| R | TAGAGCGGCACGGGGGAAAGCTTAG | |||
| QUB11b | F | CGTAAGGGGGATGCGGGAAATAGG | 52 °C | (n-67)/69 |
| R | CGAAGTGAATGGTGGCAT | |||
| Mtub21 | F | AGATCCCAGTTGTCGTCGTC | 52 °C | (n-92)/57 |
| R | CAACATCGCCTGGTTCTGTA | |||
| QUB26 | F | AACGCTCAGCTGTCGGAT | 62 °C | (n-153)/111 |
| R | CGGCCGTGCCGGCCAGGTCCTTCCCGAT |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konstantynovska, O.; Rekrotchuk, M.; Hrek, I.; Rohozhyn, A.; Rudova, N.; Poteiko, P.; Gerilovych, A.; Bortz, E.; Solodiankin, O. Severe Clinical Outcomes of Tuberculosis in Kharkiv Region, Ukraine, Are Associated with Beijing Strains of Mycobacterium tuberculosis. Pathogens 2019, 8, 75. https://doi.org/10.3390/pathogens8020075
Konstantynovska O, Rekrotchuk M, Hrek I, Rohozhyn A, Rudova N, Poteiko P, Gerilovych A, Bortz E, Solodiankin O. Severe Clinical Outcomes of Tuberculosis in Kharkiv Region, Ukraine, Are Associated with Beijing Strains of Mycobacterium tuberculosis. Pathogens. 2019; 8(2):75. https://doi.org/10.3390/pathogens8020075
Chicago/Turabian StyleKonstantynovska, Olha, Mariia Rekrotchuk, Ivan Hrek, Anton Rohozhyn, Nataliia Rudova, Petro Poteiko, Anton Gerilovych, Eric Bortz, and Oleksii Solodiankin. 2019. "Severe Clinical Outcomes of Tuberculosis in Kharkiv Region, Ukraine, Are Associated with Beijing Strains of Mycobacterium tuberculosis" Pathogens 8, no. 2: 75. https://doi.org/10.3390/pathogens8020075