


The Course of COVID-19 and Long COVID: Identifying Risk Factors among Patients Suffering from the Disease before and during the Omicron-Dominant Period

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- Group 0 included people without clinical symptoms or with symptoms lasting up to 3 days;
- Group 1 consisted of patients treated at home with symptoms lasting up to 7 days;
- Group 2 comprised patients treated at home with symptoms lasting 7 to 14 days;
- Group 3 included patients treated at home with symptoms lasting at least 14 days and fever above 38 °C, shortness of breath, and oxygen saturation less than 94% for at least 3 days;
- Group 4 concerned hospitalized patients.
Statistical Analyses
3. Results
3.1. Characteristics of the Study Group
3.2. The Course of COVID-19
3.3. Long COVID
3.4. Risk Factors for Developing Long COVID
4. Discussion
Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 4 January 2024).
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Dobrowolska, K.; Brzdek, M.; Zarebska-Michaluk, D.; Rzymski, P.; Rogalska, M.; Moniuszko-Malinowska, A.; Szymanek-Pasternak, A.; Jaroszewicz, J.; Dutkiewicz, E.; Kowalska, J.; et al. Differences between the course of SARS-CoV-2 infections in the periods of the Delta and Omicron variant dominance in Poland. Pol. Arch. Intern. Med. 2023, 133. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Babicki, M.; Kapusta, J.; Pieniawska-Smiech, K.; Kaluzinska-Kolat, Z.; Kolat, D.; Mastalerz-Migas, A.; Jankowski, P.; Chudzik, M. Do COVID-19 Vaccinations Affect the Most Common Post-COVID Symptoms? Initial Data from the STOP-COVID Register-12-Month Follow-Up. Viruses 2023, 15, 1370. [Google Scholar] [CrossRef]
- Tulimilli, S.V.; Dallavalasa, S.; Basavaraju, C.G.; Kumar Rao, V.; Chikkahonnaiah, P.; Madhunapantula, S.V.; Veeranna, R.P. Variants of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Vaccine Effectiveness. Vaccines 2022, 10, 1751. [Google Scholar] [CrossRef]
- Nagy, A.; Pongor, S.; Gyorffy, B. Different mutations in SARS-CoV-2 associate with severe and mild outcome. Int. J. Antimicrob. Agents 2021, 57, 106272. [Google Scholar] [CrossRef] [PubMed]
- Rochman, N.D.; Wolf, Y.I.; Faure, G.; Mutz, P.; Zhang, F.; Koonin, E.V. Ongoing global and regional adaptive evolution of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2021, 118, 2104241118. [Google Scholar] [CrossRef]
- Tian, D.; Sun, Y.; Xu, H.; Ye, Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J. Med. Virol. 2022, 94, 2376–2383. [Google Scholar] [CrossRef]
- Hu, F.H.; Jia, Y.J.; Zhao, D.Y.; Fu, X.L.; Zhang, W.Q.; Tang, W.; Hu, S.Q.; Wu, H.; Ge, M.W.; Du, W.; et al. Clinical outcomes of the severe acute respiratory syndrome coronavirus 2 Omicron and Delta variant: Systematic review and meta-analysis of 33 studies covering 6 037 144 coronavirus disease 2019-positive patients. Clin. Microbiol. Infect. 2023, 29, 835–844. [Google Scholar] [CrossRef]
- Bouzid, D.; Visseaux, B.; Kassasseya, C.; Daoud, A.; Femy, F.; Hermand, C.; Truchot, J.; Beaune, S.; Javaud, N.; Peyrony, O.; et al. Comparison of Patients Infected With Delta Versus Omicron COVID-19 Variants Presenting to Paris Emergency Departments: A Retrospective Cohort Study. Ann. Intern. Med. 2022, 175, 831–837. [Google Scholar] [CrossRef]
- Chatterjee, S.; Bhattacharya, M.; Nag, S.; Dhama, K.; Chakraborty, C. A Detailed Overview of SARS-CoV-2 Omicron: Its Sub-Variants, Mutations and Pathophysiology, Clinical Characteristics, Immunological Landscape, Immune Escape, and Therapies. Viruses 2023, 15, 167. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhi, H.; Teng, Y. The outbreak of SARS-CoV-2 Omicron lineages, immune escape, and vaccine effectivity. J. Med. Virol. 2023, 95, e28138. [Google Scholar] [CrossRef]
- Pather, S.; Madhi, S.A.; Cowling, B.J.; Moss, P.; Kamil, J.P.; Ciesek, S.; Muik, A.; Tureci, O. SARS-CoV-2 Omicron variants: Burden of disease, impact on vaccine effectiveness and need for variant-adapted vaccines. Front. Immunol. 2023, 14, 1130539. [Google Scholar] [CrossRef]
- Flisiak, R.; Zarebska-Michaluk, D.; Dobrowolska, K.; Rorat, M.; Rogalska, M.; Krynska, J.A.; Moniuszko-Malinowska, A.; Czupryna, P.; Kozielewicz, D.; Jaroszewicz, J.; et al. Change in the Clinical Picture of Hospitalized Patients with COVID-19 between the Early and Late Period of Dominance of the Omicron SARS-CoV-2 Variant. J. Clin. Med. 2023, 12, 5572. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Seyler, L.; Van Nedervelde, E.; De Cock, D.; Mann, C.; Pien, K.; Allard, S.D.; Demuyser, T. Surfing the Waves: Differences in Hospitalised COVID-19 Patients across 4 Variant Waves in a Belgian University Hospital. Viruses 2023, 15, 618. [Google Scholar] [CrossRef]
- Khanna, D.; Peltzer, C.; Kahar, P.; Parmar, M.S. Body Mass Index (BMI): A Screening Tool Analysis. Cureus 2022, 14, e22119. [Google Scholar] [CrossRef]
- Babicki, M.; Kolat, D.; Kapusta, J.; Kaluzinska-Kolat, Z.; Jankowski, P.; Mastalerz-Migas, A.; Banach, M.; Mordaka, R.; Chudzik, M. Prevalence and assessment of risk factors among Polish adults with post-COVID-19 syndrome: A 12-month follow-up study. Pol. Arch. Intern. Med. 2023, 133. [Google Scholar] [CrossRef]
- Rzymski, P.; Pokorska-Spiewak, M.; Jackowska, T.; Kuchar, E.; Nitsch-Osuch, A.; Pawlowska, M.; Babicki, M.; Jaroszewicz, J.; Szenborn, L.; Wysocki, J.; et al. Key Considerations during the Transition from the Acute Phase of the COVID-19 Pandemic: A Narrative Review. Vaccines 2023, 11, 1502. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Hong, V.X.; Patel, M.M.; Kahn, R.; Lipsitch, M.; Tartof, S.Y. Clinical outcomes associated with SARS-CoV-2 Omicron (B.1.1.529) variant and BA.1/BA.1.1 or BA.2 subvariant infection in Southern California. Nat. Med. 2022, 28, 1933–1943. [Google Scholar] [CrossRef]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286–1288. [Google Scholar] [CrossRef]
- Severity of Disease Associated with Omicron Variant as Compared with Delta Variant in Hospitalized Patients with Suspected or Confirmed SARS-CoV-2 Infection. Available online: https://www.who.int/publications/i/item/9789240051829 (accessed on 4 January 2024).
- Brandal, L.T.; MacDonald, E.; Veneti, L.; Ravlo, T.; Lange, H.; Naseer, U.; Feruglio, S.; Bragstad, K.; Hungnes, O.; Odeskaug, L.E.; et al. Outbreak caused by the SARS-CoV-2 Omicron variant in Norway, November to December 2021. Euro Surveill. 2021, 26, 2101147. [Google Scholar] [CrossRef]
- Patil, B. Omicron: The tsunami? Indian J. Health Sci. Biomed. Res. (KLEU) 2022, 15, 1. [Google Scholar] [CrossRef]
- Das, S.; Samanta, S.; Banerjee, J.; Pal, A.; Giri, B.; Kar, S.S.; Dash, S.K. Is Omicron the end of pandemic or start of a new innings? Travel. Med. Infect. Dis. 2022, 48, 102332. [Google Scholar] [CrossRef]
- Monge, S.; Rojas-Benedicto, A.; Olmedo, C.; Mazagatos, C.; Jose Sierra, M.; Limia, A.; Martin-Merino, E.; Larrauri, A.; Hernan, M.A.; on behalf of IBERCovid. Effectiveness of mRNA vaccine boosters against infection with the SARS-CoV-2 omicron (B.1.1.529) variant in Spain: A nationwide cohort study. Lancet Infect. Dis. 2022, 22, 1313–1320. [Google Scholar] [CrossRef]
- COVID-19 Advice for the Public: Getting Vaccinated. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice (accessed on 4 January 2024).
- Faust, J.S.; Du, C.; Liang, C.; Mayes, K.D.; Renton, B.; Panthagani, K.; Krumholz, H.M. Excess Mortality in Massachusetts During the Delta and Omicron Waves of COVID-19. JAMA 2022, 328, 74–76. [Google Scholar] [CrossRef]
- Kim, A.R.; Lee, J.; Park, S.; Kang, S.W.; Lee, Y.W.; Lim, S.Y.; Chang, E.; Bae, S.; Jung, J.; Kim, M.J.; et al. Comparison of the causes of death associated with delta and Omicron SARS-CoV-2 variants infection. J. Infect. Public Health 2023, 16, 133–135. [Google Scholar] [CrossRef]
- Relan, P.; Motaze, N.V.; Kothari, K.; Askie, L.; Le Polain, O.; Van Kerkhove, M.D.; Diaz, J.; Tirupakuzhi Vijayaraghavan, B.K. Severity and outcomes of Omicron variant of SARS-CoV-2 compared to Delta variant and severity of Omicron sublineages: A systematic review and metanalysis. BMJ Glob. Health 2023, 8, e012328. [Google Scholar] [CrossRef]
- Niu, J.; Kim, M.; Jalal, A.T.; Goldberg, J.E.; Acevedo Martinez, E.M.; Suarez Moscoso, N.P.; Rubio-Gomez, H.; Mayer, D.; Visbal, A.; Sareli, C.; et al. Distinct Clinical Presentations and Outcomes of Hospitalized Adults with the SARS-CoV-2 Infection Occurring during the Omicron Variant Surge. Healthcare 2023, 11, 1703. [Google Scholar] [CrossRef]
- Arabi, M.; Al-Najjar, Y.; Mhaimeed, N.; Salameh, M.A.; Paul, P.; AlAnni, J.; Abdelati, A.A.; Laswi, I.; Khanjar, B.; Al-Ali, D.; et al. Severity of the Omicron SARS-CoV-2 variant compared with the previous lineages: A systematic review. J. Cell Mol. Med. 2023, 27, 1443–1464. [Google Scholar] [CrossRef]
- Poniedzialek, B.; Rzymski, P.; Zarebska-Michaluk, D.; Rogalska, M.; Rorat, M.; Czupryna, P.; Kozielewicz, D.; Hawro, M.; Kowalska, J.; Jaroszewicz, J.; et al. Short-term exposure to ambient air pollution and COVID-19 severity during SARS-CoV-2 Delta and Omicron waves: A multicenter study. J. Med. Virol. 2023, 95, e28962. [Google Scholar] [CrossRef]
- Uemura, K.; Kanata, T.; Ono, S.; Michihata, N.; Yasunaga, H. The disease severity of COVID-19 caused by Omicron variants: A brief review. Ann. Clin. Epidemiol. 2023, 5, 31–36. [Google Scholar] [CrossRef]
- Fall, A.; Eldesouki, R.E.; Sachithanandham, J.; Morris, C.P.; Norton, J.M.; Gaston, D.C.; Forman, M.; Abdullah, O.; Gallagher, N.; Li, M.; et al. The displacement of the SARS-CoV-2 variant Delta with Omicron: An investigation of hospital admissions and upper respiratory viral loads. EBioMedicine 2022, 79, 104008. [Google Scholar] [CrossRef]
- DeWitt, M.E.; Tjaden, A.H.; Herrington, D.; Schieffelin, J.; Gibbs, M.; Weintraub, W.S.; Sanders, J.W.; Edelstein, S.L.; Partnership, C.-C.R. COVID-19 Symptoms by Variant Period in the North Carolina COVID-19 Community Research Partnership, North Carolina, USA. Emerg. Infect. Dis. 2023, 29, 207–211. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef] [PubMed]
- Vihta, K.D.; Pouwels, K.B.; Peto, T.E.; Pritchard, E.; House, T.; Studley, R.; Rourke, E.; Cook, D.; Diamond, I.; Crook, D.; et al. Omicron-associated changes in SARS-CoV-2 symptoms in the United Kingdom. Clin. Infect. Dis. 2022, 76, e133–e141. [Google Scholar] [CrossRef]
- Nakakubo, S.; Kishida, N.; Okuda, K.; Kamada, K.; Iwama, M.; Suzuki, M.; Yokota, I.; Ito, Y.M.; Nasuhara, Y.; Boucher, R.C.; et al. Associations of COVID-19 symptoms with omicron subvariants BA.2 and BA.5, host status, and clinical outcomes in Japan: A registry-based observational study. Lancet Infect. Dis. 2023, 23, 1244–1256. [Google Scholar] [CrossRef]
- Kang, Y.R.; Huh, J.Y.; Oh, J.Y.; Lee, J.H.; Lee, D.; Kwon, H.S.; Kim, T.B.; Choi, J.C.; Cho, Y.S.; Chung, K.F.; et al. Clinical Characteristics of Post-COVID-19 Persistent Cough in the Omicron Era. Allergy Asthma Immunol. Res. 2023, 15, 395–405. [Google Scholar] [CrossRef]
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef]
- Diexer, S.; Klee, B.; Gottschick, C.; Xu, C.; Broda, A.; Purschke, O.; Binder, M.; Frese, T.; Girndt, M.; Hoell, J.I.; et al. Association between virus variants, vaccination, previous infections, and post-COVID-19 risk. Int. J. Infect. Dis. 2023, 136, 14–21. [Google Scholar] [CrossRef]
- Gottlieb, M.; Wang, R.C.; Yu, H.; Spatz, E.S.; Montoy, J.C.C.; Rodriguez, R.M.; Chang, A.M.; Elmore, J.G.; Hannikainen, P.A.; Hill, M.; et al. Severe Fatigue and Persistent Symptoms at 3 Months Following Severe Acute Respiratory Syndrome Coronavirus 2 Infections During the Pre-Delta, Delta, and Omicron Time Periods: A Multicenter Prospective Cohort Study. Clin. Infect. Dis. 2023, 76, 1930–1941. [Google Scholar] [CrossRef]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mule, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Martin-Guerrero, J.D.; Pellicer-Valero, O.J.; Navarro-Pardo, E.; Gomez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalon, J.A.; Cigaran-Mendez, M.; Hernandez-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef]
- Wolff, D.; Drewitz, K.P.; Ulrich, A.; Siegels, D.; Deckert, S.; Sprenger, A.A.; Kuper, P.R.; Schmitt, J.; Munblit, D.; Apfelbacher, C. Allergic diseases as risk factors for Long-COVID symptoms: Systematic review of prospective cohort studies. Clin. Exp. Allergy 2023, 53, 1162–1176. [Google Scholar] [CrossRef]
- Jassat, W.; Karim, S.S.A.; Mudara, C.; Welch, R.; Ozougwu, L.; Groome, M.J.; Govender, N.; von Gottberg, A.; Wolter, N.; Wolmarans, M.; et al. Clinical severity of COVID-19 in patients admitted to hospital during the omicron wave in South Africa: A retrospective observational study. Lancet Glob. Health 2022, 10, e961–e969. [Google Scholar] [CrossRef]
- Meng, B.; Abdullahi, A.; Ferreira, I.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 usage by SARS-CoV-2 Omicron impacts infectivity and fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef]
- Kozlov, M. Omicron’s feeble attack on the lungs could make it less dangerous. Nature 2022, 601, 177. [Google Scholar] [CrossRef]
- Suzuki, R.; Yamasoba, D.; Kimura, I.; Wang, L.; Kishimoto, M.; Ito, J.; Morioka, Y.; Nao, N.; Nasser, H.; Uriu, K.; et al. Attenuated fusogenicity and pathogenicity of SARS-CoV-2 Omicron variant. Nature 2022, 603, 700–705. [Google Scholar] [CrossRef]
- Paul, P.; El-Naas, A.; Hamad, O.; Salameh, M.A.; Mhaimeed, N.; Laswi, I.; Abdelati, A.A.; AlAnni, J.; Khanjar, B.; Al-Ali, D.; et al. Effectiveness of the pre-Omicron COVID-19 vaccines against Omicron in reducing infection, hospitalization, severity, and mortality compared to Delta and other variants: A systematic review. Hum. Vaccin. Immunother. 2023, 19, 2167410. [Google Scholar] [CrossRef] [PubMed]
- Arabi, M.; Al-Najjar, Y.; Sharma, O.; Kamal, I.; Javed, A.; Gohil, H.S.; Paul, P.; Al-Khalifa, A.M.; Laws, S.; Zakaria, D. Role of previous infection with SARS-CoV-2 in protecting against omicron reinfections and severe complications of COVID-19 compared to pre-omicron variants: A systematic review. BMC Infect. Dis. 2023, 23, 432. [Google Scholar] [CrossRef]
- Notarte, K.I.; Catahay, J.A.; Velasco, J.V.; Pastrana, A.; Ver, A.T.; Pangilinan, F.C.; Peligro, P.J.; Casimiro, M.; Guerrero, J.J.; Gellaco, M.M.L.; et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: A systematic review. EClinicalMedicine 2022, 53, 101624. [Google Scholar] [CrossRef]
- Tsuchida, T.; Hirose, M.; Inoue, Y.; Kunishima, H.; Otsubo, T.; Matsuda, T. Relationship between changes in symptoms and antibody titers after a single vaccination in patients with Long COVID. J. Med. Virol. 2022, 94, 3416–3420. [Google Scholar] [CrossRef] [PubMed]
- Peghin, M.; De Martino, M.; Palese, A.; Gerussi, V.; Bontempo, G.; Graziano, E.; Visintini, E.; D’Elia, D.; Dellai, F.; Marrella, F.; et al. Post-COVID-19 syndrome and humoral response association after 1 year in vaccinated and unvaccinated patients. Clin. Microbiol. Infect. 2022, 28, 1140–1148. [Google Scholar] [CrossRef] [PubMed]
- Wisnivesky, J.P.; Govindarajulu, U.; Bagiella, E.; Goswami, R.; Kale, M.; Campbell, K.N.; Meliambro, K.; Chen, Z.; Aberg, J.A.; Lin, J.J. Association of Vaccination with the Persistence of Post-COVID Symptoms. J. Gen. Intern. Med. 2022, 37, 1748–1753. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Pre-Omicron (N = 1308) | Omicron (N = 659) | p-Value | The Whole Group (N = 1967) | |
|---|---|---|---|---|---|
| Age | 54.8 ± 13.2 | 55.7 ± 14.0 | 0.272 * | 55.1 ± 13.5 | |
| BMI | 27.9 ± 5.4 | 27.8 ± 5.9 | 0.153 * | 27.8 ± 5.5 | |
| Gender: | Female | 834 (63.8) | 458 (69.5) | 0.011 # | 1292 (65.7) |
| Male | 474 (36.2) | 201 (30.5) | 675 (34.3) | ||
| Diabetes | 136 (10.4) | 72 (10.9) | 0.719 # | 208 (10.6) | |
| Hypertension | 509 (38.9) | 263 (39.9) | 0.669 # | 772 (39.2) | |
| Asthma | 122 (9.3) | 80 (12.1) | 0.053 # | 202 (10.3) | |
| Thyroid diseases | 236 (18.0) | 112 (17.0) | 0.566 # | 348 (17.7) | |
| Hyperlipidemia | 277 (21.2) | 133 (20.2) | 0.608 # | 410 (20.8) | |
| Previous heart attack(s) | 33 (2.5) | 16 (2.4) | 0.895 # | 49 (2.5) | |
| Coronary artery disease | 78 (6.0) | 37 (5.6) | 0.755 # | 115 (5.8) | |
| Any chronic diseases | 805 (61.5) | 413 (62.7) | 0.627 # | 1218 (61.9) | |
| COVID-19 vaccination | 1114 (85.2) | 477 (72.4) | <0.001 # | 1591 (80.9) | |
| Variable | Pre-Omicron (N = 1308) | Omicron (N = 659) | p-Value | The Whole Group (N = 1967) | |
|---|---|---|---|---|---|
| Temperature < 36.6 °C | 209 (16.0) | 72 (10.9) | 0.002 # | 281 (14.3) | |
| Temperature > 37.5 °C | 705 (53.9) | 338 (51.3) | 0.273 # | 1043 (53.0) | |
| Cough | 851 (65.1) | 504 (76.6) | <0.001 # | 1355 (68.9) | |
| Dyspnea | 663 (50.7) | 329 (49.9) | 0.749 # | 992 (50.4) | |
| Chest pain | 604 (46.2) | 284 (43.2) | 0.204 # | 888 (45.1) | |
| Fatigue | 992 (75.8) | 446 (67.9) | <0.001 # | 1438 (73.1) | |
| Musculoskeletal pain | 921 (70.4) | 465 (70.6) | 0.945 # | 1386 (70.5) | |
| Smell and/or taste disorders | 680 (52.0) | 141 (21.3) | <0.001 # | 711 (36.1) | |
| Headaches | 790 (60.4) | 364 (55.1) | 0.031 # | 1154 (58.7) | |
| Diarrhea | 277 (21.2) | 113 (17.2) | 0.034 # | 390 (19.8) | |
| Vomiting | 101 (7.7) | 43 (6.5) | 0.336 # | 144 (7.3) | |
| Hearing impairment | 130 (9.9) | 77 (11.7) | 0.233 # | 207 (10.5) | |
| Duration of symptoms | 12.4 ± 6.9 | 11.1 ± 7.5 | <0.001 * | 11.98 ± 7.1 | |
| COVID-19 course severity: | 0 | 80 (6.2) | 8 (1.2) | <0.001 # | 88 (4.5) |
| 1 | 360 (27.5) | 215 (32.6) | 575 (29.2) | ||
| 2 | 364 (27.8) | 228 (34.6) | 592 (30.1) | ||
| 3 | 296 (22.6) | 121 (18.4) | 417 (21.2) | ||
| 4 | 208 (15.9) | 87 (13.2) | 295 (15.0) | ||
| Variable | Pre-Omicron (N = 1308) | Omicron (N = 659) | p-Value | The Whole Group (N = 1967) |
|---|---|---|---|---|
| Long COVID | 875 (66.9) | 314 (47.7) | <0.001 | 1189 (60.4) |
| Fatigue | 498 (38.1) | 170 (25.8) | <0.001 | 668 (33.9) |
| Cough | 38 (2.9) | 10 (1.5) | 0.060 | 48 (2.4) |
| Dyspnea | 92 (7.0) | 15 (2.3) | <0.001 | 107 (5.4) |
| Smell and/or taste disorders | 63 (4.8) | 15 (2.3) | 0.006 | 78 (4.0) |
| Musculoskeletal pain | 55 (4.2) | 17 (2.6) | 0.062 | 72 (3.7) |
| Chest pain | 79 (6.0) | 16 (2.4) | <0.001 | 95 (4.8) |
| Hair loss | 64 (4.9) | 22 (3.3) | 0.112 | 86 (4.4) |
| Concentration and memory problems | 171 (13.1) | 46 (7.0) | <0.001 | 217 (11.0) |
| Headaches | 25 (1.9) | 8 (1.2) | 0.257 | 33 (1.7) |
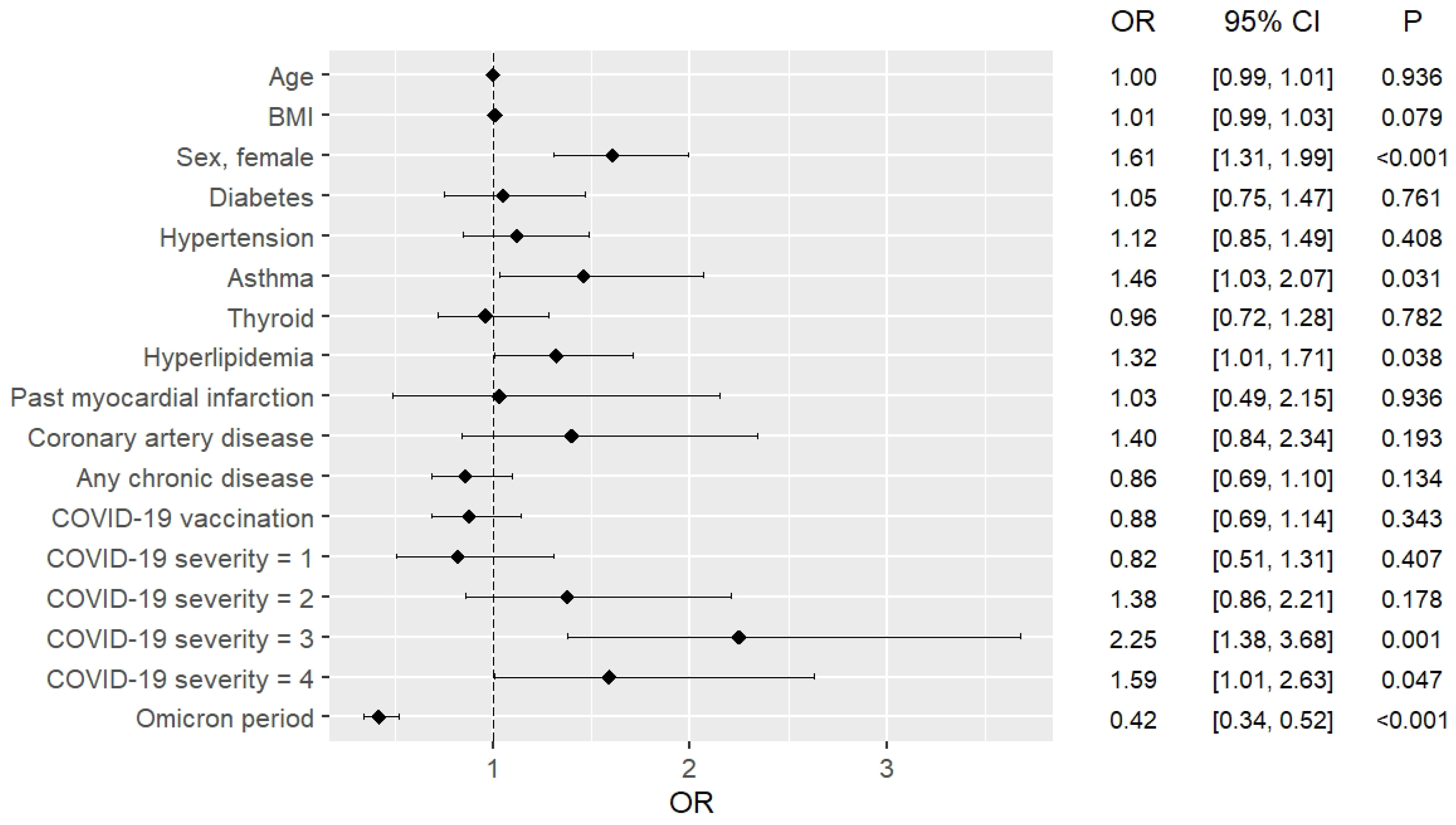
| Variable | The Whole Group (N = 1967) | Pre-Omicron (N = 1308) | Omicron (N = 659) | ||||
|---|---|---|---|---|---|---|---|
| OR [95% CI] | p-Value | OR [95% CI] | p-Value | OR [95% CI] | p-Value | ||
| Age | 1.00 [0.99, 1.01] | 0.936 | 0.99 [0.98, 1.07] | 0.642 | 1,00 [0.99, 1.02] | 0.561 | |
| BMI | 1.01 [0.99, 1.03] | 0.079 | 1.02 [1.00, 1.05] | 0.045 | 1.01 [0.98, 1.03] | 0.613 | |
| Gender, female | 1.61 [1.31, 1.99] | <0.001 | 1.62 [1.25, 2.11] | <0.001 | 1.74 [1.23, 2.53] | 0.003 | |
| Diabetes | 1.05 [0.75, 1.47] | 0.761 | 0.85 [0.56, 1.30] | 0.461 | 1.53 [0.89, 2.67] | 0.127 | |
| Hypertension | 1.12 [0.85, 1.49] | 0.408 | 0.95 [0.67, 1.35] | 0.796 | 1.08 [0.98, 1.75] | 0.098 | |
| Asthma | 1.46 [1.03, 2.07] | 0.031 | 1.81 [1.11, 2.95] | 0.016 | 1.21 [0.71, 2.07] | 0.489 | |
| Thyroid diseases | 0.96 [0.72, 1.28] | 0.782 | 0.80 [0.55, 1.14] | 0.215 | 1.40 [0.87, 2.29] | 0.168 | |
| Hyperlipidemia | 1.32 [1.01, 1.71] | 0.038 | 1.31 [0.93, 1.83] | 0.113 | 1.26 [0.81, 1.96] | 0.305 | |
| Previous heart attack(s) | 1.03 [0.49, 2.15] | 0.936 | 1.36 [0.48, 3.87] | 0.554 | 0.71 [0.21, 2.45] | 0.583 | |
| Coronary artery disease | 1.40 [0.84, 2.34] | 0.193 | 1.86 [0.93, 3.75] | 0.081 | 0.80 [0.35, 1.83] | 0.601 | |
| Any chronic diseases | 0.86 [0.69, 1.10] | 0.134 | 0.75 [0.50, 1.14] | 0.181 | 0.69 [0.40, 1.10] | 0.098 | |
| COVID-19 vaccination | 0.88 [0.69, 1.14] | 0.343 | 0.89 [0.64, 1.27] | 0.542 | 0.83 [0.57, 1.19] | 0.302 | |
| COVID-19 course severity: | 0 | Reference | Reference | Reference | Reference | Reference | Reference |
| 1 | 0.82 [0.51, 1.31] | 0.407 | 0.81 [0.49, 1.33] | 0.406 | 0.54 [0.13, 2.31] | 0.409 | |
| 2 | 1.38 [0.86, 2.21] | 0.178 | 1.46 [0.87, 2.43] | 0.143 | 0.82 [0.19, 3.51] | 0.794 | |
| 3 | 2.25 [1.38, 3.68] | 0.001 | 2.22 [1.31, 3.78] | 0.003 | 1.54 [0.36, 6.79] | 0.559 | |
| 4 | 1.59 [1.01, 2.63] | 0.047 | 1.88 [1.08, 3.29] | 0.025 | 0.74 [0.17, 3.31] | 0.693 | |
| Omicron period | 0.42 [0.34, 0.52] | <0.001 | --- | --- | --- | --- | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babicki, M.; Kołat, D.; Kałuzińska-Kołat, Ż.; Kapusta, J.; Mastalerz-Migas, A.; Jankowski, P.; Chudzik, M. The Course of COVID-19 and Long COVID: Identifying Risk Factors among Patients Suffering from the Disease before and during the Omicron-Dominant Period. Pathogens 2024, 13, 267. https://doi.org/10.3390/pathogens13030267
Babicki M, Kołat D, Kałuzińska-Kołat Ż, Kapusta J, Mastalerz-Migas A, Jankowski P, Chudzik M. The Course of COVID-19 and Long COVID: Identifying Risk Factors among Patients Suffering from the Disease before and during the Omicron-Dominant Period. Pathogens. 2024; 13(3):267. https://doi.org/10.3390/pathogens13030267
Chicago/Turabian StyleBabicki, Mateusz, Damian Kołat, Żaneta Kałuzińska-Kołat, Joanna Kapusta, Agnieszka Mastalerz-Migas, Piotr Jankowski, and Michał Chudzik. 2024. "The Course of COVID-19 and Long COVID: Identifying Risk Factors among Patients Suffering from the Disease before and during the Omicron-Dominant Period" Pathogens 13, no. 3: 267. https://doi.org/10.3390/pathogens13030267