
Prevalence and Determinants of Schistosoma mansoni Infection among Pre-School Age Children in Southern Ethiopia
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
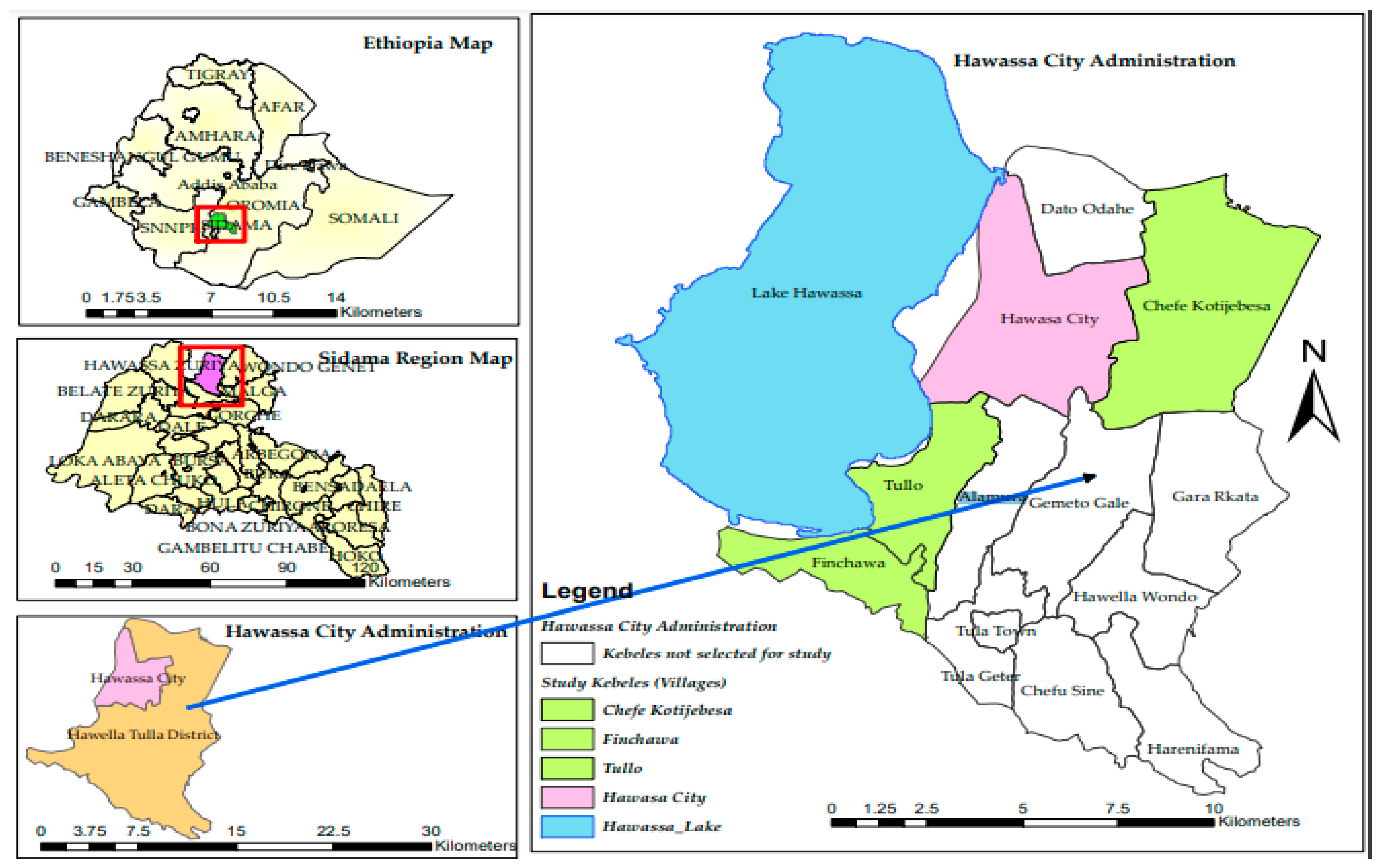
2.1. Study Area, Population, and Design
2.2. Eligibility Criteria
2.3. Sample Size Determination
2.4. Sampling Procedure
2.5. Study Variables
2.6. Data Collection Tools and Procedures
2.7. Data Analysis
3. Results
3.1. Study Participants’ Characteristics
3.2. Prevalence of S. mansoni Infection
3.3. Intensity of S. mansoni Infection in Pre-SAC
3.4. Determinants of S. mansoni Infection in Pre-SAC
3.4.1. Effect of Determinants on S. mansoni Infection
3.4.2. Between-Village Variability on the Risk of S. mansoni Infection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Schistosomiasis. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis (accessed on 4 April 2023).
- Osakunor, D.N.M.; Woolhouse, M.E.J.; Mutapi, F. Paediatric schistosomiasis: What we know and what we need to know. PLoS Negl. Trop. Dis. 2018, 12, e0006144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebreyesus, T.D.; Tadele, T.; Mekete, K.; Barry, A.; Gashaw, H.; Degefe, W.; Tadesse, B.T.; Gerba, H.; Gurumurthy, P.; Makonnen, E.; et al. Prevalence, Intensity, and Correlates of Schistosomiasis and Soil-Transmitted Helminth Infections after Five Rounds of Preventive Chemotherapy among School Children in Southern Ethiopia. Pathogens 2020, 9, 920. [Google Scholar] [CrossRef] [PubMed]
- Colley, D.G.; Bustinduy, A.L.; Secor, W.E.; King, C.H. Human schistosomiasis. Lancet 2014, 383, 2253–2264. [Google Scholar] [CrossRef]
- Abudho, B.O.; Ndombi, E.M.; Guya, B.; Carter, J.M.; Riner, D.K.; Kittur, N.; Karanja, D.M.S.; Secor, W.E.; Colley, D.G. Impact of Four Years of Annual Mass Drug Administration on Prevalence and Intensity of Schistosomiasis among Primary and High School Children in Western Kenya: A Repeated Cross-Sectional Study. Am. J. Trop. Med. Hyg. 2018, 98, 1397–1402. [Google Scholar] [CrossRef] [Green Version]
- Verani, J.R.; Butler, S.E.; Montgomery, S.P.; Karanja, D.M.S.; Mwinzi, P.N.M.; Shane, H.L.; Abudho, B.; Secor, W.E. Schistosomiasis among Young Children in Usoma, Kenya. Am. J. Trop. Med. Hyg. 2011, 84, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Faust, C.L.; Osakunor, D.N.; Downs, J.A.; Kayuni, S.; Stothard, J.R.; Lamberton, P.H.; Reinhard-Rupp, J.; Rollinson, D. Schistosomiasis Control: Leave No Age Group Behind. Trends Parasitol. 2020, 36, 582–591. [Google Scholar] [CrossRef]
- Ekpo, U.F.; Oluwole, A.S.; Abe, E.M.; Etta, H.E.; Olamiju, F.; Mafiana, C.F. Schistosomiasis in infants and pre-school-aged children in sub-Saharan Africa: Implication for control. Parasitology 2012, 139, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Munisi, D.Z.; Buza, J.; Mpolya, E.A.; Kinung’hi, S.M. Schistosoma mansoni Infections, Undernutrition and Anaemia among Primary Schoolchildren in Two Onshore Villages in Rorya District, North-Western Tanzania. PLoS ONE 2016, 11, e0167122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinung’hi, S.M.; Mazigo, H.D.; Dunne, D.W.; Kepha, S.; Kaatano, G.; Kishamawe, C.; Ndokeji, S.; Angelo, T.; Nuwaha, F. Coinfection of intestinal schistosomiasis and malaria and association with haemoglobin levels and nutritional status in school children in Mara region, Northwestern Tanzania: A cross-sectional exploratory study. BMC Res. Notes 2017, 10, 583. [Google Scholar] [CrossRef]
- Njiru, J.; Muhoho, N.; Simbauni, J.; Kabiru, E. Effects of Soil-Transmitted Helminths and Schistosoma Species on Nutritional Status of Children in Mwea Irrigation Scheme, Kenya. J. Appl. Life Sci. Int. 2016, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Abera, B.; Alem, G.; Yimer, M.; Herrador, Z. Epidemiology of soil-transmitted helminths, Schistosoma mansoni, and haematocrit values among schoolchildren in Ethiopia. J. Infect. Dev. Ctries. 2013, 7, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Mnkugwe, R.H.; Minzi, O.S.; Kinung’hi, S.M.; Kamuhabwa, A.A.; Aklillu, E. Prevalence and correlates of intestinal schistosomiasis infection among school-aged children in North-Western Tanzania. PLoS ONE 2020, 15, e0228770. [Google Scholar] [CrossRef] [Green Version]
- Nigo, M.M.; Odermatt, P.; Nigo, D.W.; Salieb-Beugelaar, G.B.; Battegay, M.; Hunziker, P.R. Morbidity associated with Schistosoma mansoni infection in north-eastern Democratic Republic of the Congo. PLoS Negl. Trop. Dis. 2021, 15, e0009375. [Google Scholar] [CrossRef]
- Sakari, S.S.W.; Mbugua, A.K.; Mkoji, G.M. Prevalence of Soil-Transmitted Helminthiases and Schistosomiasis in Preschool Age Children in Mwea Division, Kirinyaga South District, Kirinyaga County, and Their Potential Effect on Physical Growth. J. Trop. Med. 2017, 2017, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Alemu, A.; Tegegne, Y.; Damte, D.; Melku, M. Schistosoma mansoni and soil-transmitted helminths among preschool-aged children in Chuahit, Dembia district, Northwest Ethiopia: Prevalence, intensity of infection and associated risk factors. BMC Public Health 2016, 16, 422. [Google Scholar] [CrossRef] [Green Version]
- Mazigo, H.D.; Uisso, C.; Kazyoba, P.; Nshala, A.; Mwingira, U.J. Prevalence, infection intensity and geographical distribution of schistosomiasis among pre-school and school aged children in villages surrounding Lake Nyasa, Tanzania. Sci. Rep. 2021, 11, 295. [Google Scholar] [CrossRef] [PubMed]
- Mugono, M.; Konje, E.; Kuhn, S.; Mpogoro, F.J.; Morona, D.; Mazigo, H.D. Intestinal schistosomiasis and geohelminths of Ukara Island, North-Western Tanzania: Prevalence, intensity of infection and associated risk factors among school children. Parasites Vectors 2014, 7, 612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemal, M.; Tadesse, G.; Esmael, A.; Abay, S.M.; Kebede, T. Schistosoma mansoni infection among preschool age children attending Erer Health Center, Ethiopia and the response rate to praziquantel. BMC Res. Notes 2019, 12, 211. [Google Scholar] [CrossRef] [PubMed]
- Cisse, M.; Sangare, I.; Djibougou, A.D.; Tahita, M.C.; Gnissi, S.; Bassinga, J.K.W.; Konda, S.; Diallo, A.H. Prevalence and risk factors of Schistosoma mansoni infection among preschool-aged children from Panamasso village, Burkina Faso. Parasites Vectors 2021, 14, 185. [Google Scholar] [CrossRef]
- Sheehy, C.; Lawson, H.; Andriamasy, E.H.; Russell, H.J.; Reid, A.; Raderalazasoa, G.U.; Dodge, G.; Kornitschky, R.; Penney, J.M.S.; Ranaivoson, T.N.; et al. Prevalence of intestinal schistosomiasis in pre-school aged children: A pilot survey in Marolambo District, Madagascar. Infect. Dis. Poverty 2021, 10, 87. [Google Scholar] [CrossRef]
- Sacolo-Gwebu, H.; Chimbari, M.; Kalinda, C. Prevalence and risk factors of schistosomiasis and soil-transmitted helminthiases among preschool aged children (1–5 years) in rural KwaZulu-Natal, South Africa: A cross-sectional study. Infect. Dis. Poverty 2019, 8, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayele, A.; Tegegne, Y.; Derso, A.; Eshetu, T.; Zeleke, A.J. Prevalence and Associated Factors of Intestinal Helminths Among Kindergarten Children in Gondar Town, Northwest Ethiopia. Pediatr. Health Med. Ther. 2021, 12, 35–41. [Google Scholar] [CrossRef]
- Sousa-Figueiredo, J.C.; Pleasant, J.; Day, M.; Betson, M.; Rollinson, D.; Montresor, A.; Kazibwe, F.; Kabatereine, N.B.; Stothard, J.R. Treatment of intestinal schistosomiasis in Ugandan preschool children: Best diagnosis, treatment efficacy and side-effects, and an extended praziquantel dosing pole. Int. Health 2010, 2, 103–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poole, H.; Terlouw, D.J.; Naunje, A.; Mzembe, K.; Stanton, M.; Betson, M.; Lalloo, D.G.; Stothard, J.R. Schistosomiasis in pre-school-age children and their mothers in Chikhwawa district, Malawi with notes on characterization of schistosomes and snails. Parasit Vectors 2014, 7, 153. [Google Scholar] [CrossRef] [Green Version]
- Rujeni, N.; Bayingana, J.B.; Nyandwi, E.; Ntakarutimana, A.; Kagabo, J.; Rutayisire, R.; Shema, E.; Kanimba, P.; Mbonigaba, J.B.; Ruberanziza, E. Prevalence Mapping of Schistosoma mansoni Among Pre-school Age Children in Rwanda. Front. Pediatr. 2022, 10, 906177. [Google Scholar] [CrossRef]
- Bekana, T.; Berhe, N.; Eguale, T.; Aemero, M.; Medhin, G.; Tulu, B.; G/Hiwot, Y.; Liang, S.; Hu, W.; Erko, B. Prevalence and factors associated with intestinal schistosomiasis and human fascioliasis among school children in Amhara Regional State, Ethiopia. Trop. Med. Health 2021, 49, 35. [Google Scholar] [CrossRef]
- Ansha, M.G.; Kuti, K.A.; Girma, E. Prevalence of Intestinal Schistosomiasis and Associated Factors among School Children in Wondo District, Ethiopia. J. Trop. Med. 2020, 2020, 1–8. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Ending the Neglect to attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2020; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- World Health Organization. Preventive Chemotherapy in Human Helminthiasis; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Aula, O.P.; McManus, D.P.; Jones, M.K.; Gordon, C.A. Schistosomiasis with a Focus on Africa. Trop. Med. Infect. Dis. 2021, 6, 109. [Google Scholar] [CrossRef] [PubMed]
- Woldeyohannes, D.; Sahiledengle, B.; Tekalegn, Y.; Hailemariam, Z. Prevalence of Schistosomiasis (S. mansoni and S. haematobium) and its association with gender of school age children in Ethiopia: A systematic review and meta-analysis. Parasite Epidemiol. Control 2021, 13, e00210. [Google Scholar] [CrossRef]
- Ethiopia|ESPEN. Available online: https://espen.afro.who.int/countries/ethiopia (accessed on 4 April 2023).
- World Health Organization. WHO Recommendation Expansion of Preventive Chemotherapy to All in Need. Available online: https://www.who.int/activities/expanding-preventive-chemotherapy-to-all-in-need (accessed on 12 April 2023).
- Ministry of Health of Ethiopia. Neglected Tropical Diseases (NTDs) Program. Available online: https://www.moh.gov.et/site/initiatives-4-col/Neglected_Tropical_Diseases_Program (accessed on 3 April 2023).
- Federal Democratic Republic of Ethiopia Ministry of Health. National Master Plan for Neglected Tropical Diseases (NTDs). Addis Ababa; 2013–2015. Available online: http://ec2-18-210-136-214.compute-1.amazonaws.com/sites/default/files/docs/national_ntd_master_plan_ethiopia_2013-2015 (accessed on 4 April 2023).
- World Health Organization. Bench Aids for the Diagnosis of Intestinal Parasites. WHO, 1994. Available online: http://apps.who.int/iris/bitstream/10665/37323/1/9789241544764 (accessed on 4 April 2023).
- World Health Organization. WHO Guideline on Control and Elimination of Human Schistosomiasis; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications-detail-redirect/9789240041608 (accessed on 4 April 2023).
- WHO. Schistosomiasis: Progress Report 2001–2011, Strategic Plan 2012–2020; World Health Organization: Geneva, Switzerland, 2013; ISBN 978-92-4-150317-4. [Google Scholar]
- Federal Ministry of Health, Ethiopia. Guideline for the Transition of the Enhanced Outreach Strategy (EOS) to the Community Health Days/Health Extension Programme (CHD/HEP); Federal Ministry of Health: Addis Ababa, Ethiopia, 2012.


{kind=link}
| Variable | Category | Frequency N (%) |
|---|---|---|
| Age (in years) | Four | 393 (23.4) |
| Five | 465 (27.6) | |
| Six | 424 (25.2) | |
| Seven | 401 (23.8) | |
| Sex | Female | 803 (47.7) |
| Male | 880 (52.3) | |
| Educational level of mothers/primary caregivers of pre-SAC | No formal education | 701 (41.6) |
| Primary education | 486 (28.9) | |
| Secondary education | 232 (13.8) | |
| College and above | 264 (15.7) | |
| Current major occupation of mothers/primary caregivers of pre-SAC | Farmer | 397 (23.6) |
| Full-time housewife | 1139 (67.7) | |
| Merchant/employed | 147 (8.7) | |
| Wealth Index | Poorest | 413 (24.5) |
| Poorer | 357 (21.2) | |
| Middle | 271 (16.1) | |
| Richer | 313 (18.6) | |
| Richest | 329 (19.6) | |
| District | Tullo | 763 (45.3) |
| Finchawa | 447 (26.6) | |
| Chefe Kotijebesa | 473 (28.1) | |
| Distance from the water sources | Less than 1 km | 304 (18.1) |
| 1 km to 2 km | 977 (58.0) | |
| More than 2 km | 402 (23.9) |
| Age | S. mansoni Infection Prevalence | S. mansoni Infection Intensity in Pre-SAC | ||
|---|---|---|---|---|
| Light | Moderate | Heavy | ||
| Overall | 14.3% | 8.1% | 4.1% | 2.1% |
| 4 years | 6.9% | 4.1% | 2.3% | 0.5% |
| 5 years | 9.9% | 5.5% | 3.0% | 1.3% |
| 6 years | 16.3% | 9.9% | 3.6% | 2.8% |
| 7 years | 24.7% | 13.2% | 7.7% | 3.8% |
| Variable | Category | S. mansoni Infection | Univariable Multilevel LR | Multivariable Multilevel LR | |||
|---|---|---|---|---|---|---|---|
| Non-Infected | Infected | COR (95%Cl) | p Value | AOR (95%Cl) | p Value | ||
| Age (in years) | Four | 366 (93.1%) | 27 (6.9%) | 1 a | 1 a | ||
| Five | 419 (90.1%) | 46 (9.9%) | 1.62 (0.98, 2.68) | 0.06 | 1.57 (0.93, 2.66) | 0.09 | |
| Six | 355 (83.7% | 69 (16.3%) | 3.00 (1.86, 4.83) | <0.001 | 2.58 (1.55, 4.27) | <0.001 | |
| Seven | 302 (75.3%) | 99 (24.7%) | 5.72 (3.59, 9.12) | <0.001 | 4.63 (2.82, 7.62) | <0.001 | |
| Marital status of parents | Married | 1412 (86.1) | 228 (13.9) | 1 a | 1 a | ||
| Not married | 30 (69.8) | 13 (30.2) | 2.28 (1.16,4.51) | 0.02 | 1.40 (0.65, 3.01) | 0.39 | |
| Sex | Female | 706 (87.9) | 97 (12.1)) | 1 a | 1 a | ||
| Male | 736 (83.6) | 144 (16.4) | 1.49 (1.12, 1.97) | 0.006 | 1.25 (0.92, 1.70) | 0.16 | |
| The educational level of mothers/primary caregivers of pre-SAC | College and above | 235 (89.1) | 29 (10.9) | 1 a | 1 a | ||
| No formal education | 594 (84.7) | 107 (15.3) | 1.68 (1.08, 2.62) | 0.02 | 1.18 (0.68, 2.02) | 0.56 | |
| Primary education | 410 (84.4) | 76 (15.6) | 1.81 (1.13, 2.88) | 0.01 | 1.46 (0.86, 2.49) | 0.17 | |
| Secondary education | 203 (87.5) | 29 (12.5) | 1.24 (0.71, 2.17) | 0.44 | 1.03 (0.56, 1.89) | 0.92 | |
| Contact to infested water | No | 676 (90.5) | 71 (9.5) | 1 a | 1 a | ||
| Yes | 766 (81.8) | 170 (18.2) | 2.16 (1.60, 2.92) | <0.001 | 0.71 (0.31, 1.60) | 0.40 | |
| Frequency of accompany to the water source | Never | 675 (91.5) | 63 (8.5) | 1 a | 1 a | ||
| Sometime | 631 (84.5) | 116 (15.5) | 1.96 (1.41, 2.72) | <0.001 | 2.60 (1.12, 6.01) | 0.03 | |
| All the time | 136 (68.7) | 62 (31.3) | 5.05 (3.35, 7.63) | <0.001 | 5.91 (2.51, 13.90) | <0.001 | |
| Wealth index | Richest | 283 (86.0) | 46 (14.0) | 1.0 | 1 a | ||
| Poorest | 361 (87.4) | 52 (12.6) | 1.08 (0.70, 1.68) | 0.72 | 1.06 (0.62, 1.80) | 0.84 | |
| Poorer | 304 (85.2) | 53 (14.9) | 1.35 (0.87,2.09) | 0.18 | 1.10 (0.65, 1.85) | 0.72 | |
| Middle | 227 (83.8) | 44 (16.2) | 1.64 (1.03, 2.60) | 0.04 | 1.54 (0.90, 2.63) | 0.11 | |
| Richer | 267 (85.3) | 46 (14.7) | 1.23 (0.78,1.93) | 0.37 | 1.05 (0.63, 1.76) | 0.85 | |
| Distance to the water sources | More than 2 km | 356 (88.6) | 46 (11.4) | 1 a | 1 a | ||
| Less than 1 km | 215 (70.7) | 89 (29.3) | 3.50 (2.34, 5.24) | <0.001 | 3.17 (1.47, 6.83) | 0.003 | |
| 1 km to 2 km | 871 (89.2) | 106 (10.9) | 1.04 (0.72, 1.52) | 0.81 | 1.04 (0.63, 1.72) | 0.89 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tadele, T.; Astatkie, A.; Abay, S.M.; Tadesse, B.T.; Makonnen, E.; Aklillu, E. Prevalence and Determinants of Schistosoma mansoni Infection among Pre-School Age Children in Southern Ethiopia. Pathogens 2023, 12, 858. https://doi.org/10.3390/pathogens12070858
Tadele T, Astatkie A, Abay SM, Tadesse BT, Makonnen E, Aklillu E. Prevalence and Determinants of Schistosoma mansoni Infection among Pre-School Age Children in Southern Ethiopia. Pathogens. 2023; 12(7):858. https://doi.org/10.3390/pathogens12070858
Chicago/Turabian StyleTadele, Tafese, Ayalew Astatkie, Solomon Mequanente Abay, Birkneh Tilahun Tadesse, Eyasu Makonnen, and Eleni Aklillu. 2023. "Prevalence and Determinants of Schistosoma mansoni Infection among Pre-School Age Children in Southern Ethiopia" Pathogens 12, no. 7: 858. https://doi.org/10.3390/pathogens12070858