
Ophthalmic Manifestations of the Monkeypox Virus: A Systematic Review and Meta-Analysis
 , , , , ,
, , , , ,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question and Selection Criteria
2.2. Databases Included and Search Strategy
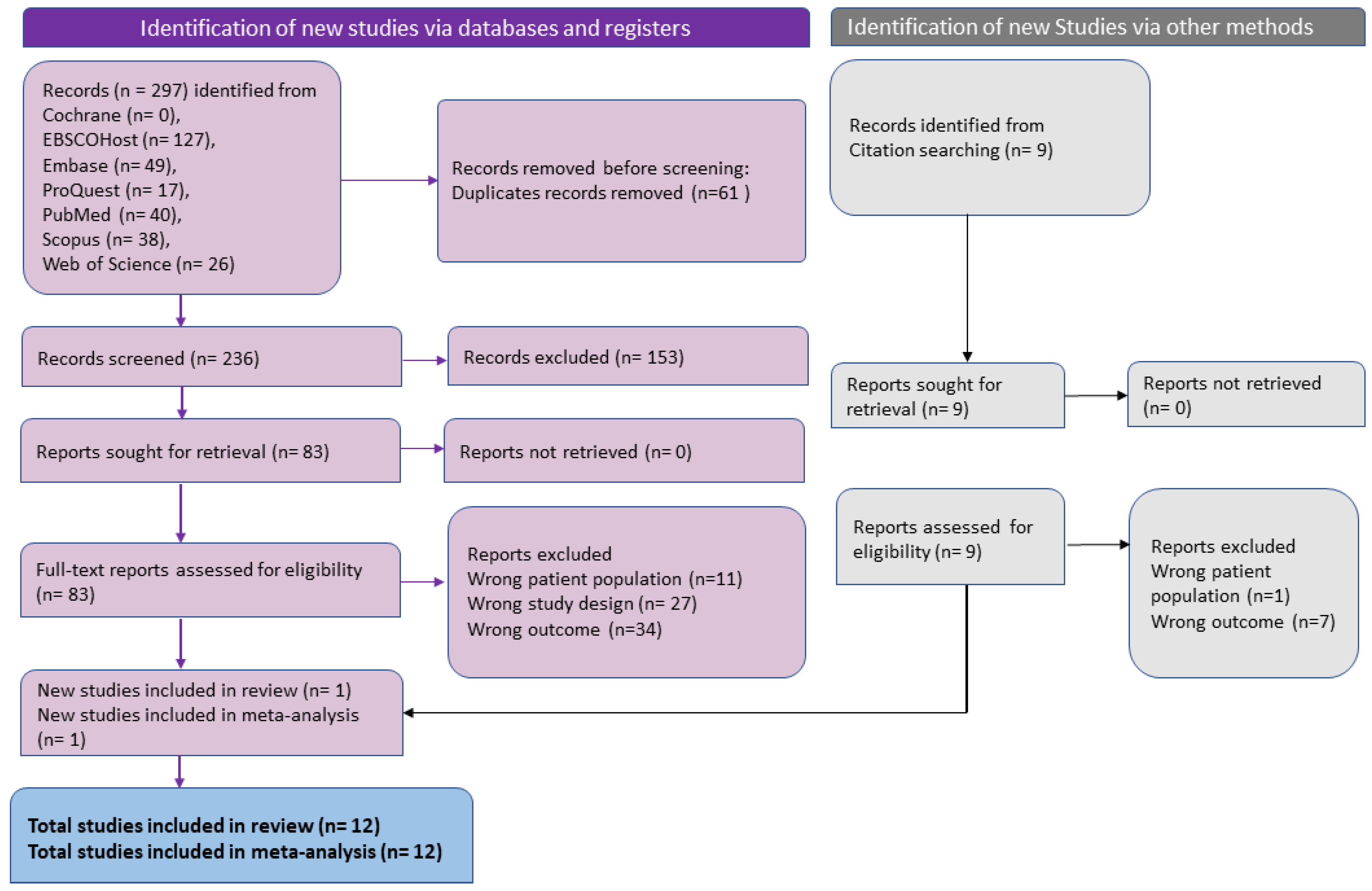
2.3. Selection of Studies
2.3.1. Title Abstract Screening
2.3.2. Full-Text Screening and Data Extraction
2.3.3. Quality Assessment
2.4. Data Analysis
3. Results
3.1. Eligible Studies
3.2. Study Characteristics
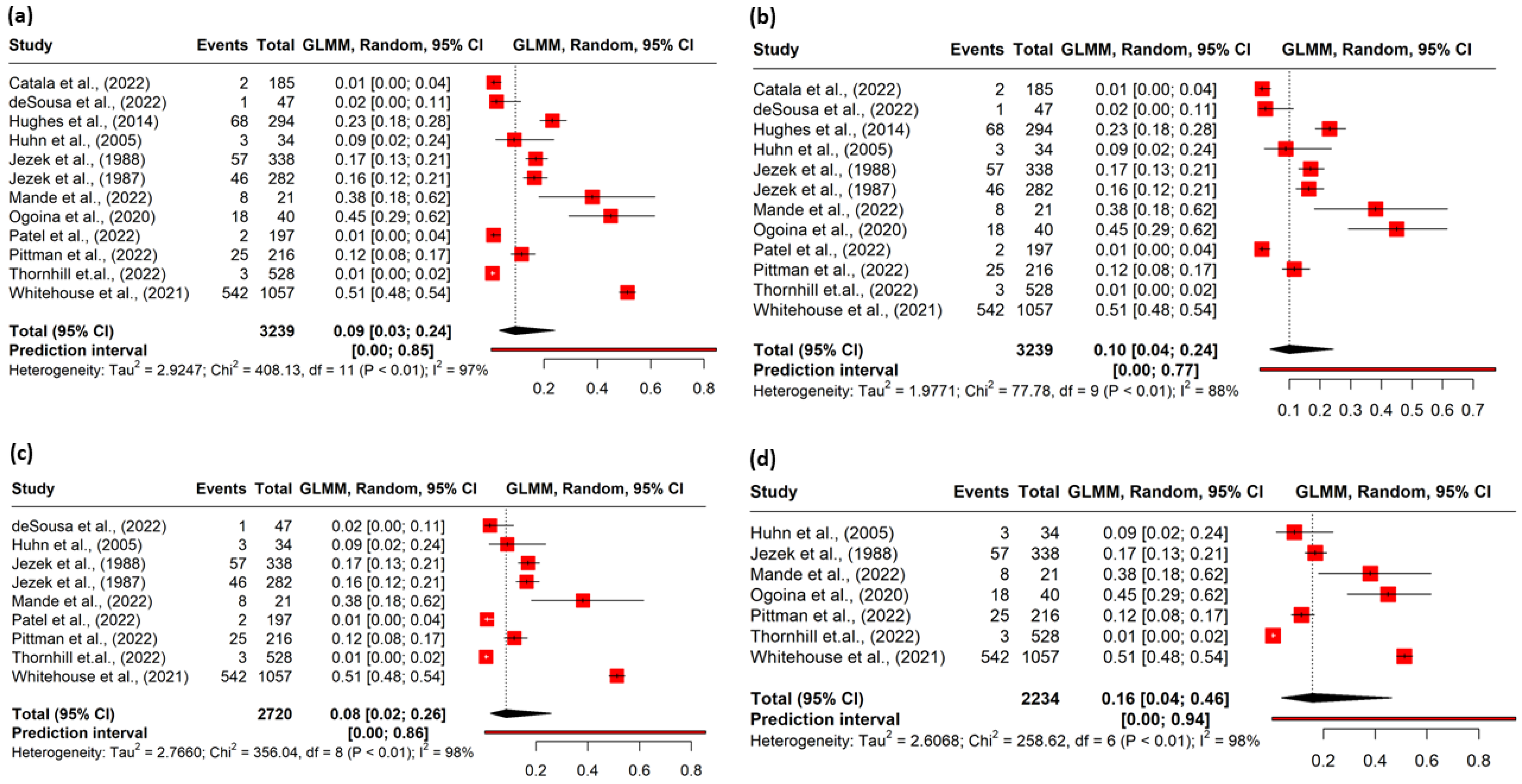
3.3. Pooled Prevalence
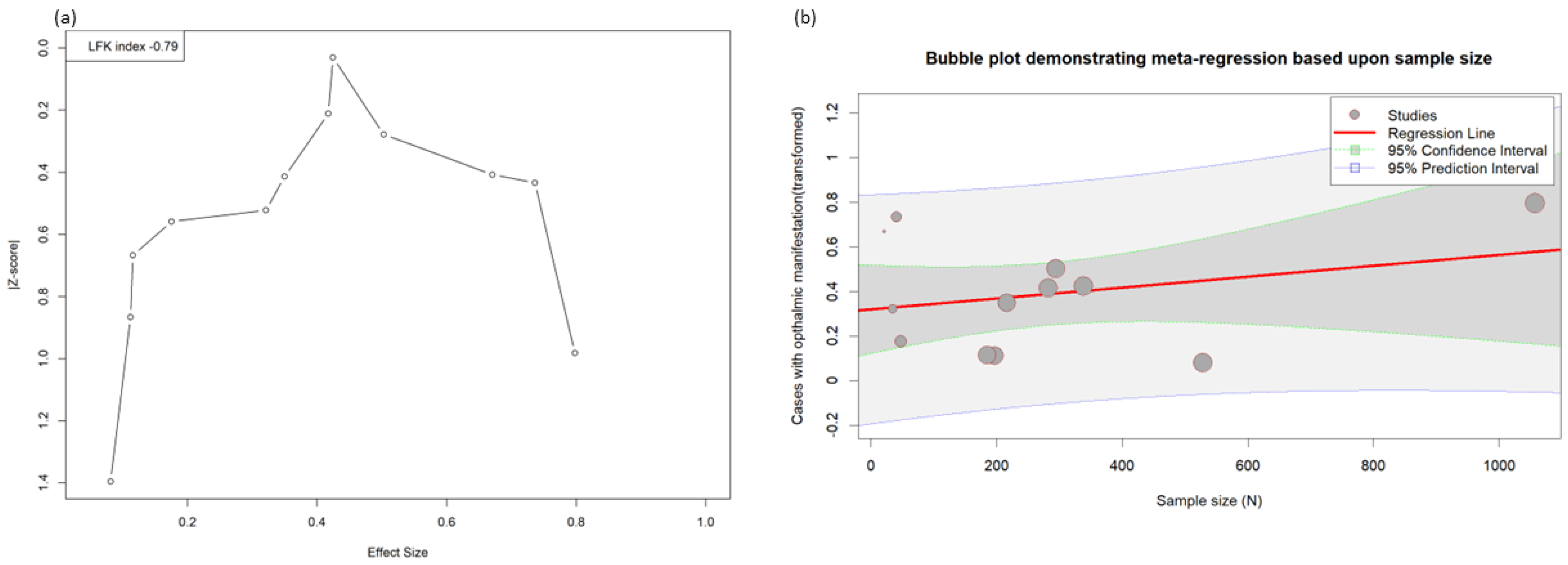
3.4. Risk of Bias
3.5. Subgroup Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data availability statement
Conflicts of Interest
References
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A Human Infection Caused by Monkeypox Virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593–597. [Google Scholar] [PubMed]
- Huang, Y.; Mu, L.; Wang, W. Monkeypox: Epidemiology, Pathogenesis, Treatment and Prevention. Signal Transduct. Target. Ther. 2022, 7, 373. [Google Scholar] [CrossRef] [PubMed]
- World Health Orginazation Multi-Country Outbreak of Monkeypox, External Situation Report #12—14 December 2022. Available online: https://www.who.int/publications/m/item/multi-country-outbreak-of-mpox--external-situation-report-12--14-december-2022 (accessed on 26 December 2022).
- Alakunle, E.; Moens, U.; Nchinda, G.; Okeke, M.I. Monkeypox Virus in Nigeria: Infection Biology, Epidemiology, and Evolution. Viruses 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Damon, I.K. Status of Human Monkeypox: Clinical Disease, Epidemiology and Research. Vaccine 2011, 29, D54–D59. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.S.; Lin, C.Y.; Urbina, A.N.; Wang, W.H.; Assavalapsakul, W.; Tseng, S.P.; Lu, P.L.; Chen, Y.H.; Yu, M.L.; Wang, S.F. The First Case of Monkeypox Virus Infection Detected in Taiwan: Awareness and Preparation. Int. J. Infect. Dis. 2022, 122, 991–995. [Google Scholar] [CrossRef]
- Benites-Zapata, V.A.; Ulloque-Badaracco, J.R.; Alarcon-Braga, E.A.; Hernandez-Bustamante, E.A.; Mosquera-Rojas, M.D.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Clinical Features, Hospitalisation and Deaths Associated with Monkeypox: A Systematic Review and Meta-Analysis. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 36. [Google Scholar] [CrossRef]
- Kumar, N.; Acharya, A.; Gendelman, H.E.; Byrareddy, S.N. The 2022 Outbreak and the Pathobiology of the Monkeypox Virus. J. Autoimmun. 2022, 131, 102855. [Google Scholar] [CrossRef]
- Pourriyahi, H.; Aryanian, Z.; Afshar, Z.M.; Goodarzi, A. A Systematic Review and Clinical Atlas on Mucocutaneous Presentations of Monkeypox: With a Comprehensive Approach to All Aspects of the New and Previous Monkeypox Outbreaks. J. Med. Virol. 2022, 95, e28230. [Google Scholar] [CrossRef]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The Changing Epidemiology of Human Monkeypox—A Potential Threat? A Systematic Review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- Gandhi, P.A.; Patro, S.K.; Sandeep, M.; Satapathy, S.; Shamim, M.A.; Kumar, V.; Aggarwal, A.K.; Padhi, B.K.; Sah, R. Oral Manifestation of the Monkeypox Virus: A Systematic Review and Meta-Analysis. eClinicalMedicine 2023, 56, 101817. [Google Scholar] [CrossRef]
- Abdelaal, A.; Serhan, H.A.; Mahmoud, M.A.; Rodriguez-Morales, A.J.; Sah, R. Ophthalmic Manifestations of Monkeypox Virus. Eye 2022, 37, 383–385. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.; McCollum, A.; Pukuta, E.; Karhemere, S.; Nguete, B.; Lushima, R.S.; Kabamba, J.; Balilo, M.; Tamfum, J.-J.M.; Wemakoy, O. Ocular Complications Associated with Acute Monkeypox Virus Infection, DRC. Int. J. Infect. Dis. 2014, 21, 276–277. [Google Scholar] [CrossRef] [Green Version]
- Ly-Yang, F.; Miranda-Sánchez, A.; Burgos-Blasco, B.; Fernández-Vigo, J.I.; Gegúndez-Fernández, J.A.; Díaz-Valle, D. Conjunctivitis in an Individual With Monkeypox. JAMA Ophthalmol. 2022, 140, 1022–1024. [Google Scholar] [CrossRef] [PubMed]
- Ogoina, D.; Iroezindu, M.; James, H.I.; Oladokun, R.; Yinka-Ogunleye, A.; Wakama, P.; Otike-Odibi, B.; Usman, L.M.; Obazee, E.; Aruna, O.; et al. Clinical Course and Outcome of Human Monkeypox in Nigeria. Clin. Infect. Dis. 2020, 71, e210–e214. [Google Scholar] [CrossRef] [PubMed]
- Jezek, Z.; Grab, B.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M. Clinico-Epidemiological Features of Monkeypox Patients with an Animal or Human Source of Infection. Bull. World Health Organ. 1988, 66, 459–464. [Google Scholar] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A Basic Introduction to Fixed-Effect and Random-Effects Models for Meta-Analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M. Research Note: In a Meta-Analysis, the I(2) Index Does Not Tell Us How Much the Effect Size Varies across Studies. J. Physiother. 2020, 66, 135–139. [Google Scholar] [CrossRef]
- Comprehensive Meta-Analysis Software (CMA). Available online: https://www.meta-analysis.com/ (accessed on 1 March 2023).
- Whitehouse, E.R.; Bonwitt, J.; Hughes, C.M.; Lushima, R.S.; Likafi, T.; Nguete, B.; Kabamba, J.; Monroe, B.; Doty, J.B.; Nakazawa, Y.; et al. Clinical and Epidemiological Findings from Enhanced Monkeypox Surveillance in Tshuapa Province, Democratic Republic of the Congo During 2011–2015. J. Infect. Dis. 2021, 223, 1870–1878. [Google Scholar] [CrossRef]
- Jezek, Z.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M. Human Monkeypox: Clinical Features of 282 Patients. J. Infect. Dis. 1987, 156, 293–298. [Google Scholar] [CrossRef]
- Huhn, G.D.; Bauer, A.M.; Yorita, K.; Graham, M.B.; Sejvar, J.; Likos, A.; Damon, I.K.; Reynolds, M.G.; Kuehnert, M.J. Clinical Characteristics of Human Monkeypox, and Risk Factors for Severe Disease. Clin. Infect. Dis. 2005, 41, 1742–1751. [Google Scholar] [CrossRef]
- Mande, G.; Akonda, I.; De Weggheleire, A.; Brosius, I.; Liesenborghs, L.; Bottieau, E.; Ross, N.; Gembu, G.-C.; Colebunders, R.; Verheyen, E.; et al. Enhanced Surveillance of Monkeypox in Bas-Uélé, Democratic Republic of Congo: The Limitations of Symptom-Based Case Definitions. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2022, 122, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Bilinska, J.; Tam, J.C.H.; Da Silva Fontoura, D.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C.; et al. Clinical Features and Novel Presentations of Human Monkeypox in a Central London Centre during the 2022 Outbreak: Descriptive Case Series. BMJ 2022, 378, e072410. [Google Scholar] [CrossRef] [PubMed]
- de Sousa, D.; Patrocínio, J.; Frade, J.; Brazão, C.; Mancha, D.; Correia, C.; Borges-Costa, J.; Filipe, P. Monkeypox Diagnosis by Cutaneous and Mucosal Findings. Infect. Dis. Rep. 2022, 14, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Pittman, P.R.; Martin, J.W.; Kingebeni, P.M.; Tamfum, J.-J.M.; Wan, Q.; Reynolds, M.G.; Quinn, X.; Norris, S.; Townsend, M.B.; Satheshkumar, P.S.; et al. Clinical Characterization of Human Monkeypox Infections in the Democratic Republic of the Congo. medRxiv 2022. [Google Scholar] [CrossRef]
- Català, A.; Clavo-Escribano, P.; Riera-Monroig, J.; Martín-Ezquerra, G.; Fernandez-Gonzalez, P.; Revelles-Peñas, L.; Simon-Gozalbo, A.; Rodríguez-Cuadrado, F.J.; Castells, V.G.; de la Torre Gomar, F.J.; et al. Monkeypox Outbreak in Spain: Clinical and Epidemiological Findings in a Prospective Cross-Sectional Study of 185 Cases. Br. J. Dermatol. 2022, 187, 765–772. [Google Scholar] [CrossRef]
- Taha, M.J.J.; Abuawwad, M.T.; Alrubasy, W.A.; Sameer, S.K.; Alsafi, T.; Al-Bustanji, Y.; Abu-Ismail, L.; Nashwan, A.J. Ocular Manifestations of Recent Viral Pandemics: A Literature Review. Front. Med. 2022, 9, 1011335. [Google Scholar] [CrossRef]
- Shamim, M.A.; Padhi, B.K.; Satapathy, P.; Veeramachaneni, S.D.; Chatterjee, C.; Tripathy, S.; Akhtar, N.; Pradhan, A.; Dwivedi, P.; Mohanty, A. The Use of Antivirals in the Treatment of Human Monkeypox Outbreaks: A Systematic Review: Antivirals in Treatment of Monkeypox: Systematic Review. Int. J. Infect. Dis. 2022, 127, 150–161. [Google Scholar] [CrossRef]
- Vogel, L. Making Sense of Monkeypox Death Rates. C. Can. Med. Assoc. J. 2022, 194, E1097. [Google Scholar] [CrossRef]
- Guarner, J.; Johnson, B.J.; Paddock, C.D.; Shieh, W.-J.; Goldsmith, C.S.; Reynolds, M.G.; Damon, I.K.; Regnery, R.L.; Zaki, S.R. Monkeypox Transmission and Pathogenesis in Prairie Dogs. Emerg. Infect. Dis. 2004, 10, 426–431. [Google Scholar] [CrossRef]
- Mazzotta, V.; Mondi, A.; Carletti, F.; Baldini, F.; Santoro, R.; Meschi, S.; Moccione, M.; Teklè, S.G.; Minosse, C.; Camici, M. Ocular Involvement in Monkeypox: Description of an Unusual Presentation during the Current Outbreak. J. Infect. 2022, 85, 573–607. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Study Design | Geography | Sample Size | Prevalence (Ophthalmic Lesion) | Cluster | Key Findings |
|---|---|---|---|---|---|---|
| Catala et al., (2022) | Cross-sectional | Spain | 185 | 1% | Patients from the national surveillance database system. | Pustules or pseudo pustules were noted on eyelids in two patients. Complications: pain, dysphagia, and conjunctivitis were reasons for hospitalization. |
| De Sousa et al., (2022) | Retrospective observational | Portugal | 47 | 2% | Individuals with confirmed mpox infection. | Only one patient had palpebral conjunctiva ulceration. |
| Hughes et al., (2014) | Cross-sectional | Democratic Republic of Congo | 294 | 23.1% | Real time PCR mpox positive patients. | A total of 23.1% of the mpox patients had conjunctivitis, and 47% of the conjunctivitis patients were bed-ridden. |
| Huhn et al., (2005) | Cross-sectional | United States | 34 | 9% | Patients with confirmed mpox in medical records. | Around 9% of cases had involvement of conjunctiva (eye), and only one case had involvement of cornea, i.e., presented with keratitis and corneal ulceration. |
| Jezek et al., (1987) | Cross-sectional | Democratic Republic of Congo | 282 | 13.4% | Mpox-diagnosed patients. | Forty-six were found to have opthalmic lesions (focal lesions). Keratitis, corneal ulceration was reported among 12 patients. |
| Jezek et al., (1988) | Cross-sectional | Democratic Republic of Congo | 338 | 25% | Mpox-diagnosed patients. | Fifty-seven patients were reported to have conjunctivitis; eleven had corneal ulcers. Deforming scars, weak vision, and unilateral and bilateral blindness were observed in primary cases (10%) and secondary cases (5%) (29 cases). |
| Mande et al., (2022) | Cross-sectional | Democratic Republic of Congo | 21 | 38% | Mpox-positive patients. | Of the 21 positive patients, 8 reported ocular lesions/corneal opacities. |
| Ogoina et al., (2020) | Retrospective study | Nigeria | 40 | 45% | Hospitalised mpox-infected patients. | Eyes rashes were seen in 25% of 35 of the patients who gave details of their first symptom (9 patients). Nine patients reported conjunctivitis and photophobia. |
| Patel et al., (2022) | Descriptive case series | United Kingdom | 197 | 1% | Patients confirmed with MPXV with a polymerase chain reaction. | Out of 197 patients, only 2 had conjunctivitis. |
| Pittman et al., (2022) | Prospective observational | Democratic Republic of Congo | 216 | 18% | MPXV-specific PCR-positive patients. | Twenty patients had eye manifestations, which included eye redness, eye pain, and eye discharge. Five patients (2.3%) had reported visual changes. Conjunctival and other lesions were experienced by 14 patients. |
| Thornhill et.al., (2022) | Case series | America, Europe, Israel, Australia | 528 | 1% | Confirmed human mpox infection cases from 16 countries. | Three patients had conjunctival mucosa lesions. |
| Whitehouse et al., (2021) | Cross-sectional | Democratic Republic of Congo | 1057 | 51% | PCR-confirmed mpox patients. | A total of 210 (20.7%) had conjunctivitis, and 332 (33.2%) had photophobia. |
| Analysis | Pooled Estimate | 95% CI | p Value | 95% PI | I2 |
|---|---|---|---|---|---|
| Main analysis | 0.09 | 0.03–0.24 | <0.01 | 0–0.85 | 97% |
| Outliers removed * | 0.10 | 0.04–0.24 | <0.01 | 0–0.77 | 88% |
| Poor-quality studies removed ** | 0.08 | 0.02–0.26 | <0.01 | 0–0.88 | 98% |
| Potential overlapping studies removed # | 0.16 | 0.04–0.46 | <0.01 | 0–0.94 | 98% |
| Factors | Estimate (95% CI) | p | I2 | P Subgroup |
|---|---|---|---|---|
| Endemicity | <0.001 | |||
| Non-endemic | 1.05 [0.09–2.68] | 0.07 | 53.93% | |
| Endemic | 27.22 [13.69–43.26] | <0.001 | 98.09% | |
| Waves of outbreak | <0.001 | |||
| 2022 multi-country outbreak | 0.61 [0.13–1.31] | 0.55 | 0% | |
| Pre-2022 outbreak | 24.78 [12.41–39.62] | <0.001 | 97.84% | |
| Continent | <0.001 | |||
| Europe | 0.98 [0.14–2.31] | - | - | |
| Africa | 27.22 [12.69–43.26] | <0.001 | 98.09 | |
| North America | 8.82 [3.05–22.96] | - | - | |
| Multi-continent | 0.57 [0.19–1.66] | - | - |
| Number of Studies | Pooled Prevalence ES | 95% CI | |
|---|---|---|---|
| Manifestations | |||
| Conjunctivitis | 6 * | 13.89% | 6.92–22.67 |
| Conjunctival ulceration | 1 | 2.13% | 0.38–11.11 |
| Conjunctival lesion (unspecified) | 2 | 1.62% | 0.80–2.69 |
| Eye rash (location unspecified) | 2 | 14.37% | 6.91–23.71 |
| Pustules or pseudo-pustules in eyelid | 1 | 1.08% | 0.30–3.86 |
| Redness, pain, and discharge | 1 | 9.26% | 6.07–13.87 |
| Complications | |||
| Photophobia | 2 | 30.87% | 28.13–33.67 |
| Keratitis/Corneal ulceration | 3 | 3.33% | 1.99–4.95 |
| Corneal opacity | 1 | 38.1% | 20.75–59.12 |
| blindness (Unilateral/Bilateral) | 1 | 7.69% | 5.30–11.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gandhi, A.P.; Gupta, P.C.; Padhi, B.K.; Sandeep, M.; Suvvari, T.K.; Shamim, M.A.; Satapathy, P.; Sah, R.; León-Figueroa, D.A.; Rodriguez-Morales, A.J.; et al. Ophthalmic Manifestations of the Monkeypox Virus: A Systematic Review and Meta-Analysis. Pathogens 2023, 12, 452. https://doi.org/10.3390/pathogens12030452
Gandhi AP, Gupta PC, Padhi BK, Sandeep M, Suvvari TK, Shamim MA, Satapathy P, Sah R, León-Figueroa DA, Rodriguez-Morales AJ, et al. Ophthalmic Manifestations of the Monkeypox Virus: A Systematic Review and Meta-Analysis. Pathogens. 2023; 12(3):452. https://doi.org/10.3390/pathogens12030452
Chicago/Turabian StyleGandhi, Aravind P., Parul Chawla Gupta, Bijaya K. Padhi, Mokanpally Sandeep, Tarun Kumar Suvvari, Muhammad Aaqib Shamim, Prakasini Satapathy, Ranjit Sah, Darwin A. León-Figueroa, Alfonso J. Rodriguez-Morales, and et al. 2023. "Ophthalmic Manifestations of the Monkeypox Virus: A Systematic Review and Meta-Analysis" Pathogens 12, no. 3: 452. https://doi.org/10.3390/pathogens12030452