

Dermatological Manifestations in COVID-19: A Case Study of SARS-CoV-2 Infection in a Genetic Thrombophilic Patient with Mthfr Mutation
 , , , , , and
, , , , , and 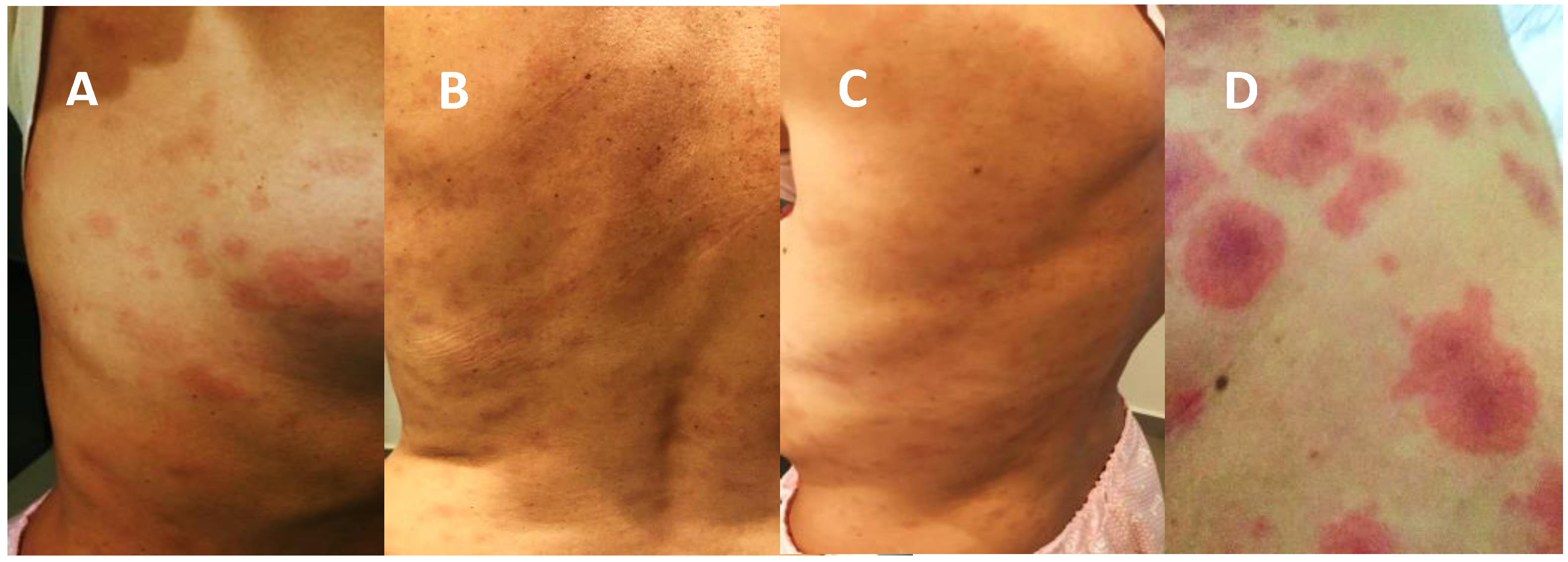{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
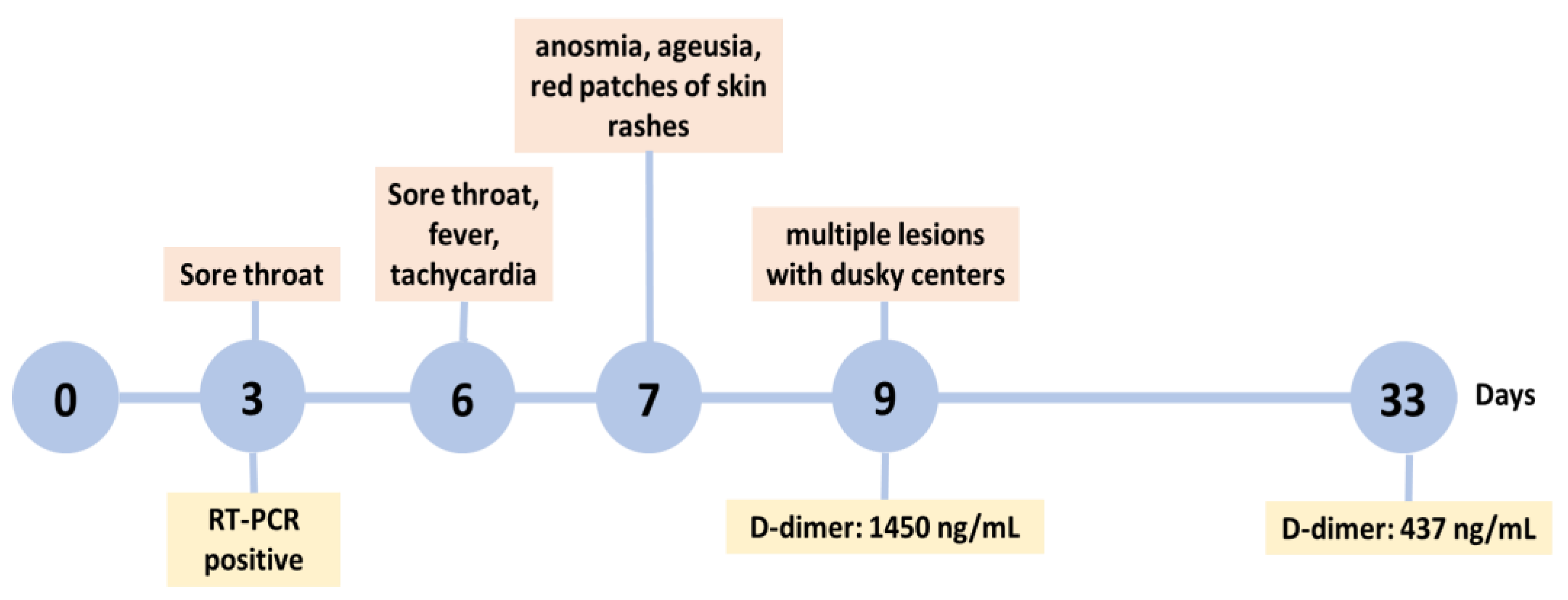
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thakur, V.; Ratho, R.K.; Kumar, P.; Bhatia, S.K.; Bora, I.; Mohi, G.K.; Saxena, S.K.; Devi, M.; Yadav, D.; Mehariya, S. Multi-Organ Involvement in COVID-19: Beyond Pulmonary Manifestations. J. Clin. Med. 2021, 10, 446. [Google Scholar] [CrossRef]
- Kreutmair, S.; Kauffmann, M.; Unger, S.; Ingelfinger, F.; Núñez, N.G.; Alberti, C.; De Feo, D.; Krishnarajah, S.; Friebel, E.; Ulutekin, C.; et al. Preexisting comorbidities shape the immune response associated with severe COVID-19. J. Allergy Clin. Immunol. 2022, 150, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Seque, C.A.; Enokihara, M.M.S.e.S.; Porro, A.M.; Tomimori, J. Skin Manifestations Associated with COVID-19. An. Bras. Dermatol. 2022, 97, 75–88. [Google Scholar] [CrossRef]
- Suchonwanit, P.; Leerunyakul, K.; Kositkuljorn, C. Cutaneous Manifestations In COVID-19: Lessons Learned From Current Evidence. J. Am. Acad. Dermatol. 2020, 83, e57–e60. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.W.; Tam, Y.C.; Oh, C.C. Skin Manifestations of COVID-19: A Worldwide Review. JAAD Int. 2021, 2, 119–133. [Google Scholar] [CrossRef]
- Genovese, G.; Moltrasio, C.; Berti, E.; Marzano, A.V. Skin Manifestations Associated with COVID-19: Current Knowledge and Future Perspectives. Dermatology 2021, 237, 1–12. [Google Scholar] [CrossRef]
- Bilaloglu, S.; Aphinyanaphongs, Y.; Jones, S.; Iturrate, E.; Hochman, J.; Berger, J.S. Thrombosis in Hospitalized Patients with COVID-19 in a New York City Health System. JAMA J. Am. Med. Assoc. 2020, 324, 799–801. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 Novel Coronavirus (2019-NCoV) by Real-Time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greninger, A.L.; Naccache, S.N.; Federman, S.; Yu, G.; Mbala, P.; Bres, V.; Stryke, D.; Bouquet, J.; Somasekar, S.; Linnen, J.M.; et al. Rapid Metagenomic Identification of Viral Pathogens in Clinical Samples by Real-Time Nanopore Sequencing Analysis. Genome Med. 2015, 7, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendel, S.; Kutner, J.M.; Machado, R.; Fontão-Wendel, R.; Bub, C.; Fachini, R.; Yokoyama, A.; Candelaria, G.; Sakashita, A.; Achkar, R.; et al. Screening for SARS-CoV-2 Antibodies in Convalescent Plasma in Brazil: Preliminary Lessons from a Voluntary Convalescent Donor Program. Transfusion 2020, 60, 2938–2951. [Google Scholar] [CrossRef]
- Agnihothri, R.; Fox, L.P. Clinical Patterns and Morphology of COVID-19 Dermatology. Dermatol. Clin. 2021, 39, 487–503. [Google Scholar] [CrossRef]
- Burlando, M.; Russo, R.; Cozzani, E.; Parodi, A. COVID-19 “Second Wave” and Vaccines: The Dermatologists’ Perspective. Int. J. Dermatol. 2021, 60, 889–890. [Google Scholar] [CrossRef]
- Galván Casas, C.; Català, A.; Carretero Hernández, G.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa Lario, A.; Navarro Fernández, I.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Llamas Velasco, M.; et al. Classification of the Cutaneous Manifestations of COVID-19: A Rapid Prospective Nationwide Consensus Study in Spain with 375 Cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Català, A.; Galván-Casas, C.; Carretero-Hernández, G.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa, A.; Navarro-Fernández, Í.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Llamas-Velasco, M.; et al. Maculopapular Eruptions Associated to COVID-19: A Subanalysis of the COVID-Piel Study. Dermatol. Ther. 2020, 33, e14170. [Google Scholar] [CrossRef]
- Sławińska, M.; Nowicki, R.J. Dermatological Manifestations of COVID-19: A Practical Summary of the Current State of Knowledge. Przegl. Dermatol. 2020, 107, 228–233. [Google Scholar] [CrossRef]
- Nonaka, C.K.V.; Franco, M.M.; Gräf, T.; de Lorenzo Barcia, C.A.; de Ávila Mendonça, R.N.; de Sousa, K.A.F.; Costa Neiva, L.M.; Fosenca, V.; Mendes, A.V.A.; de Aguiar, R.S.; et al. Genomic Evidence of SARS-CoV-2 Reinfection Involving E484K Spike Mutation, Brazil. Emerg. Infect. Dis. 2021, 27, 1522–1524. [Google Scholar] [CrossRef]
- Yadav, P.; Mohandas, S.; Sarkale, P.; Nyayanit, D.; Shete, A.; Sahay, R.; Potdar, V.; Baradkar, S.; Gupta, N.; Sapkal, G.; et al. Isolation of SARS-CoV-2 B.1.1.28.2 (P2) Variant and Pathogenicity Comparison with D614G Variant in Hamster Model. J. Infect. Public Health 2022, 15, 164–171. [Google Scholar] [CrossRef]
- Garcia-Beltran, W.F.; Lam, E.C.; St. Denis, K.; Nitido, A.D.; Garcia, Z.H.; Hauser, B.M.; Feldman, J.; Pavlovic, M.N.; Gregory, D.J.; Poznansky, M.C.; et al. Multiple SARS-CoV-2 Variants Escape Neutralization by Vaccine-Induced Humoral Immunity. Cell 2021, 184, 2372–2383.e9. [Google Scholar] [CrossRef] [PubMed]
- Souza, W.M.; Amorim, M.R.; Sesti-Costa, R.; Coimbra, L.D.; Brunetti, N.S.; Toledo-Teixeira, D.A.; de Souza, G.F.; Muraro, S.P.; Parise, P.L.; Barbosa, P.P.; et al. Neutralisation of SARS-CoV-2 Lineage P.1 by Antibodies Elicited through Natural SARS-CoV-2 Infection or Vaccination with an Inactivated SARS-CoV-2 Vaccine: An Immunological Study. Lancet Microbe 2021, 2, e527–e535. [Google Scholar] [CrossRef] [PubMed]
- Chia, W.N.; Zhu, F.; Ong, S.W.X.; Young, B.E.; Fong, S.W.; le Bert, N.; Tan, C.W.; Tiu, C.; Zhang, J.; Tan, S.Y.; et al. Dynamics of SARS-CoV-2 Neutralising Antibody Responses and Duration of Immunity: A Longitudinal Study. Lancet Microbe 2021, 2, e240–e249. [Google Scholar] [CrossRef]
- Pang, N.Y.L.; Pang, A.S.R.; Chow, V.T.; Wang, D.Y. Understanding Neutralising Antibodies against SARS-CoV-2 and Their Implications in Clinical Practice. Mil. Med. Res. 2021, 8, 47. [Google Scholar] [CrossRef]
- Röltgen, K.; Powell, A.E.; Wirz, O.F.; Stevens, B.A.; Hogan, C.A.; Najeeb, J.; Hunter, M.; Wang, H.; Sahoo, M.K.; Huang, C.H.; et al. Defining the Features and Duration of Antibody Responses to SARS-CoV-2 Infection Associated with Disease Severity and Outcome. Sci. Immunol. 2020, 5, eabe0240. [Google Scholar] [CrossRef]
- Voloch, C.M.; da Silva Francisco, R.; de Almeida, L.G.P.; Cardoso, C.C.; Brustolini, O.J.; Gerber, A.L.; Guimarães, A.P.d.C.; Mariani, D.; da Costa, R.M.; Ferreira, O.C.; et al. Genomic Characterization of a Novel SARS-CoV-2 Lineage from Rio de Janeiro, Brazil. J. Virol. 2021, 95. [Google Scholar] [CrossRef]
- Demoliner, M.; da Silva, M.S.; Gularte, J.S.; Hansen, A.W.; de Almeida, P.R.; Weber, M.N.; Heldt, F.H.; Silveira, F.; Filippi, M.; de Abreu Góes Pereira, V.M.; et al. Predominance of SARS-CoV-2 P.1 (Gamma) Lineage Inducing the Recent COVID-19 Wave in Southern Brazil and the Finding of an Additional S: D614A Mutation. Infect. Genet. Evol. 2021, 96, 105134. [Google Scholar] [CrossRef] [PubMed]
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B.; et al. Tracking Changes in SARS-CoV-2 Spike: Evidence That D614G Increases Infectivity of the COVID-19 Virus. Cell 2020, 182, 812–827.e19. [Google Scholar] [CrossRef]
- von Bartheld, C.S.; Hagen, M.M.; Butowt, R. The D614G Virus Mutation Enhances Anosmia in COVID-19 Patients: Evidence from a Systematic Review and Meta-Analysis of Studies from South Asia. ACS Chem. Neurosci. 2021, 12, 3535–3549. [Google Scholar] [CrossRef]
- Majumdar, P.; Niyogi, S. SARS-CoV-2 Mutations: The Biological Trackway towards Viral Fitness. Epidemiol. Infect. 2021, 149, e110. [Google Scholar] [CrossRef] [PubMed]
- Luo, R.; Delaunay-Moisan, A.; Timmis, K.; Danchin, A. SARS-CoV-2 Biology and Variants: Anticipation of Viral Evolution and What Needs to Be Done. Environ. Microbiol. 2021, 23, 2339–2363. [Google Scholar] [CrossRef] [PubMed]
- Visconti, A.; Murray, B.; Rossi, N.; Wolf, J.; Ourselin, S.; Spector, T.D.; Freeman, E.E.; Bataille, V.; Falchi, M. Cutaneous Manifestations of SARS-CoV-2 Infection during the Delta and Omicron Waves in 348,691 UK Users of the UK ZOE COVID Study App. Br. J. Dermatol. 2022, 187, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Ko, W.C.; Lee, P.I.; Jean, S.S.; Hsueh, P.R. Extra-Respiratory Manifestations of COVID-19. Int. J. Antimicrob. Agents 2020, 56, 106024. [Google Scholar] [CrossRef]
- Singh, H.; Kaur, H.; Singh, K.; Sen, C.K. Cutaneous Manifestations of COVID-19: A Systematic Review. Adv. Wound Care 2021, 10, 51–80. [Google Scholar] [CrossRef] [PubMed]
- Jindal, R.; Chauhan, P. Cutaneous Manifestations of Coronavirus Disease 2019 in 458 Confirmed Cases: A Systematic Review. J. Fam. Med. Prim. Care 2020, 9, 4563. [Google Scholar] [CrossRef]
- Martinez-Lopez, A.; Cuenca-Barrales, C.; Montero-Vilchez, T.; Molina-Leyva, A.; Arias-Santiago, S. Review of Adverse Cutaneous Reactions of Pharmacologic Interventions for COVID-19: A Guide for the Dermatologist. J. Am. Acad. Dermatol. 2020, 83, 1738–1748. [Google Scholar] [CrossRef] [PubMed]
- Florêncio, F.K.Z.; de Oliveira Tenório, M.; Andrade, A.R.M.; de Lima, S.G. Angioedema, Endothelium, ACE2, and Bradykinin—Interrelationships in COVID-19: A Case Report. Medicina 2020, 53, 309–312. [Google Scholar] [CrossRef]
- Kroumpouzos, G. Cutaneous Manifestations of COVID-19: An Unusual Presentation with Edematous Plaques and Pruritic, Erythematous Papules, and Comment on the Role of Bradykinin Storm and Its Therapeutic Implications. Dermatol. Ther. 2021, 34, e14753. [Google Scholar] [CrossRef] [PubMed]
- Ehrenfeld, P.; Millan, C.; Matus, C.E.; Figueroa, J.E.; Burgos, R.A.; Nualart, F.; Bhoola, K.D.; Figueroa, C.D. Activation of Kinin B1 Receptors Induces Chemotaxis of Human Neutrophils. J. Leukoc. Biol. 2006, 80, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Kenne, E.; Rasmuson, J.; Renné, T.; Vieira, M.L.; Müller-Esterl, W.; Herwald, H.; Lindbom, L. Neutrophils Engage the Kallikrein-Kinin System to Open up the Endothelial Barrier in Acute Inflammation. FASEB J. 2019, 33, 2599–2609. [Google Scholar] [CrossRef] [Green Version]
- Kaya, G.; Kaya, A.; Saurat, J.-H. Clinical and Histopathological Features and Potential Pathological Mechanisms of Skin Lesions in COVID-19: Review of the Literature. Dermatopathology 2020, 7, 2. [Google Scholar] [CrossRef]
- Salimi-Jeda, A.; Abbassi, S.; Mousavizadeh, A.; Esghaie, M.; Bokharaei-Salim, F.; Jeddi, F.; Shafaati, M.; Abdoli, A. SARS-CoV-2: Current Trends in Emerging Variants, Pathogenesis, Immune Responses, Potential Therapeutic, and Vaccine Development Strategies. Int. Immunopharmacol. 2021, 101, 108232. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620938149. [Google Scholar] [CrossRef] [PubMed]
- Ali, N. Elevated Level of C-Reactive Protein May Be an Early Marker to Predict Risk for Severity of COVID-19. J. Med. Virol. 2020, 92, 2409–2411. [Google Scholar] [CrossRef]
- Capoferri, G.; Daikeler, T.; Mühleisen, B.; Trendelenburg, M.; Müller, S. Cutaneous Leukocytoclastic Vasculitis Secondary to COVID-19 Infection Leading to Extensive Skin Necrosis. Clin. Dermatol. 2022, 40, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Karst, M.; Hollenhorst, J.; Achenbach, J. Life-Threatening Course in Coronavirus Disease 2019 (COVID-19): Is There a Link to Methylenetetrahydrofolic Acid Reductase (MTHFR) Polymorphism and Hyperhomocysteinemia? Med. Hypotheses 2020, 144, 110234. [Google Scholar] [CrossRef]
- Annunziata, A.; Coppola, A.; di Spirito, V.; Cauteruccio, R.; Marotta, A.; di Micco, P.; Fiorentino, G. The Angiotensin Converting Enzyme Deletion/Deletion Genotype Is a Risk Factor for Severe COVID-19: Implication and Utility for Patients Admitted to Emergency Department. Medicina 2021, 57, 844. [Google Scholar] [CrossRef] [PubMed]
- Cantanhede, M.H.D.; Sarges, K.M.d.L.; Leite, M.d.M.; Miyajima, F.; dos Santos, E.J.M. Suscetibilidade de polimorfismos genéticos a trombofilia e seu papel na COVID-19. Braz. J. Infect. Dis. 2022, 26, 47. [Google Scholar] [CrossRef]
- Yafei, W.; Lijun, P.; Jinfeng, W.; Xiaoying, Z. Is the Prevalence of MTHFR C677T Polymorphism Associated with Ultraviolet Radiation in Eurasia? J. Hum. Genet. 2012, 57, 780–786. [Google Scholar] [CrossRef]
- Yadav, U.; Kumar, P.; Gupta, S.; Rai, V. Distribution of MTHFR C677T Gene Polymorphism in Healthy North Indian Population and an Updated Meta-Analysis. Indian J. Clin. Biochem. 2017, 32, 399–410. [Google Scholar] [CrossRef]
- Wilcken, B.; Bamforth, F.; Li, Z.; Zhu, H.; Ritvanen, A.; Redlund, M.; Stoll, C.; Alembik, Y.; Dott, B.; Czeizel, A.E.; et al. Geographical and Ethnic Variation of the 677C>T Alleleof 5,10 Methylenetetrahydrofolate Reductase (MTHFR): Findings from over 7000 Newborns from 16 Areas Worldwide. J. Med. Genet. 2003, 40, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Russo, G.T.; Friso, S.; Jacques, P.F.; Rogers, G.; Cucinotta, D.; Wilson, P.W.F.; Ordovas, J.M.; Rosenberg, I.H.; Selhub, J. Age and Gender Affect the Relation between Methylenetetrahydrofolate Reductase C677T Genotype and Fasting Plasma Homocysteine Concentrations in the Framingham Offspring Study Cohort. J. Nutr. 2003, 133, 3416–3421. [Google Scholar] [CrossRef] [Green Version]
- Smits, S.L.; de Lang, A.; van den Brand, J.M.A.; Leijten, L.M.; van Ijcken, W.F.; Eijkemans, M.J.C.; van Amerongen, G.; Kuiken, T.; Andeweg, A.C.; Osterhaus, A.D.M.E.; et al. Exacerbated Innate Host Response to SARS-CoV in Aged Non-Human Primates. PLoS Pathog. 2010, 6, e1000756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berbert, A. Further comment on articles pertaining to: “Homocysteine as a potential predictor of cardiovascular risk in patients with COVID-19”. Med. Hypotheses 2021, 155, 110676. [Google Scholar] [CrossRef] [PubMed]
- Lord, N.; Ruwart, M.J. Homocysteine and the SARS-CoV-2 Coronavirus—The X factor of severe disease and death. SSRN 2020, 1–6. [Google Scholar] [CrossRef]
- Ponti, G.; Roli, L.; Oliva, G.; Manfredini, M.; Trenti, T.; Kaleci, S.; Iannella, R.; Balzano, B.; Coppola, A.; Fiorentino, G.; et al. Homocysteine (Hcy) assessment to predict outcomes of hospitalized COVID-19 patients: A multicenter study on 313 COVID-19 patients. Clin. Chem. Lab. Med. 2021, 59, e354–e357. [Google Scholar] [CrossRef]
- Tavares, L.S.; Ortiz, J.V. Development of thrombosis in patients with and without SARS-Cov-2 infection—Literature review. Res. Soc. Dev. 2021, 10, e410101522959. [Google Scholar] [CrossRef]
- de la Morena-Barrio, M.E.; Bravo-Pérez, C.; de la Morena-Barrio, B.; Orlando, C.; Cifuentes, R.; Padilla, J.; Miñano, A.; Herrero, S.; Marcellini, S.; Revilla, N.; et al. A pilot study on the impact of congenital thrombophilia in COVID-19. Eur. J. Clin. Investig. 2021, 51, e13546. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, Y. Potential Interventions for Novel Coronavirus in China: A Systematic Review. J. Med Virol. 2020, 92, 479–490. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Lázaro, D.; Garrosa, M. Identification, Mechanism, and Treatment of Skin Lesions in COVID-19: A Review. Viruses 2021, 13, 1916. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Levi, M.; Thachil, J. Coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 2103–2109. [Google Scholar] [CrossRef]
- Chan, N.C.; Weitz, J.I. COVID-19 coagulopathy, thrombosis, and bleeding. Blood 2020, 136, 381–833. [Google Scholar] [CrossRef]
- Ponti, G.; Pastorino, L.; Manfredini, M.; Ozben, T.; Oliva, G.; Kaleci, S.; Lannella, R.; Tomasi, A. COVID-19 spreading across world correlates with C677T allele of the methylenetetrahydrofolate reductase (MTHFR) gene prevalence. J. Clin. Lab. Anal. 2021, 35, e23798. [Google Scholar] [CrossRef] [PubMed]
- Dusse, L.M.; Carvalho, M.; Braganca, W.F.; Paiva, S.G.; Godoi, L.C.; Guimaraes, D.A.; Godoi, L.C.; Guimarães, D.A.M.; Fernandes, A.P. Inherited thrombophilias and pre-eclampsia in Brazilian women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 134, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Filho, I.L.; Leite, A.C.; Moura, P.G.; Ribeiro, G.S.; Cavalcante, A.C.; Azevedo, F.C.; Andrada-Serpa, M.J. Genetic polymorphisms and cerebrovascular disease in children with sickle cell anemia from Rio de Janeiro, Brazil. Arq. Neuropsiquiatr. 2011, 69, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabino, A.P.; Guimarães, D.A.M.; Ribeiro, D.D.; Paiva, S.G.; Dusse, L.M.; Carvalho, M.G.; Fernandes, A.P. Increased Factor V Leiden frequency is associated with venous thrombotic events among young Brazilian patients. J. Thromb. Thrombolysis 2007, 24, 261–266. [Google Scholar] [CrossRef]
- Dick-Guareschi, J.; Fontana, J.C.; Sanseverino, M.T.V.; Kubaski, F.; Sekine, L.; Mesquita, N.F.; Onsten, T.G.H.; Leistner-Segala, S. Prevalence of thrombophilia-associated genetic risk factors in blood donors of a regional hospital in southern Brazil. Hematol. Transfus. Cell Ther. 2022, 44, 379–385. [Google Scholar] [CrossRef]
- Soligo, A.G.; Barini, R.; Annichino-Bizzacchi, J.M. Prevalence of the MTHFR C677T mutation in fertile and infertile women. Rev. Bras. Ginecol. Obstet. 2017, 39, 659–662. [Google Scholar] [CrossRef] [Green Version]
- Dupont, L.; Duquia, R.P.; Pizutti, G.W.; Nunes, F.B.; Branchini, G.; Mosquera, E.S.B.; Bonamigo, R.R. Cutaneous manifestations in patients with COVID-19 treated at an university hospital in southern Brazil. Cureus 2022, 14, e31566. [Google Scholar] [CrossRef]
- Passarelli-Araujo, H.; Pott-Junior, H.; Susuki, A.M.; Olak, A.S.; Pescim, R.R.; Tomimatsu, M.F.A.I.; Volce, C.J.; Neves, M.A.Z.; Silva, F.F.; Narciso, S.G.; et al. The impact of COVID-19 vaccination on case fatality rates in a city in Southern Brazil. Am. J. Infect. Control. 2022, 50, 491–496. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Celestino, G.G.; Amarante, M.K.; Vespero, E.C.; Tavares, E.R.; Yamauchi, L.M.; Candido, É.D.; de Oliveira, D.B.L.; Durigon, E.L.; Yamada-Ogatta, S.F.; Faccin-Galhardi, L.C. Dermatological Manifestations in COVID-19: A Case Study of SARS-CoV-2 Infection in a Genetic Thrombophilic Patient with Mthfr Mutation. Pathogens 2023, 12, 438. https://doi.org/10.3390/pathogens12030438
Celestino GG, Amarante MK, Vespero EC, Tavares ER, Yamauchi LM, Candido ÉD, de Oliveira DBL, Durigon EL, Yamada-Ogatta SF, Faccin-Galhardi LC. Dermatological Manifestations in COVID-19: A Case Study of SARS-CoV-2 Infection in a Genetic Thrombophilic Patient with Mthfr Mutation. Pathogens. 2023; 12(3):438. https://doi.org/10.3390/pathogens12030438
Chicago/Turabian StyleCelestino, Gabriela Gomes, Marla Karine Amarante, Eliana Carolina Vespero, Eliandro Reis Tavares, Lucy Megumi Yamauchi, Érika Donizetti Candido, Danielle Bruna Leal de Oliveira, Edison Luiz Durigon, Sueli Fumie Yamada-Ogatta, and Ligia Carla Faccin-Galhardi. 2023. "Dermatological Manifestations in COVID-19: A Case Study of SARS-CoV-2 Infection in a Genetic Thrombophilic Patient with Mthfr Mutation" Pathogens 12, no. 3: 438. https://doi.org/10.3390/pathogens12030438