
Challenges Facing Viral Hepatitis C Elimination in Lebanon



Abstract
:1. Introduction and Background
2. Methodology
3. HCV in Lebanon
3.1. Prevalence and Incidence
3.2. Routes of Transmission and High-Risk Groups
3.3. Genotype Distribution of HCV among High-Risk Groups
3.4. Therapy Prescription
3.5. Barriers to HCV Elimination
3.5.1. Absence of a National Screening Plan
3.5.2. Intravenous Drug Use and Associated Stigma
3.5.3. High-Risk Prison Environment
3.5.4. Refugees
3.5.5. Economic Collapse
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Lindenbach, B.D.; Rice, C.M. Unravelling hepatitis C virus replication from genome to function. Nature 2005, 436, 933–938. [Google Scholar] [CrossRef]
- World Health Organisation. Hepatitis C. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 11 December 2021).
- Kato, N. Genome of human hepatitis C virus (HCV): Gene organization, sequence diversity, and variation. Microb. Comp. Genom. 2000, 5, 129–151. [Google Scholar] [CrossRef]
- Bukh, J. The history of hepatitis C virus (HCV): Basic research reveals unique features in phylogeny, evolution and the viral life cycle with new perspectives for epidemic control. J. Hepatol. 2016, 65, S2–S21. [Google Scholar] [CrossRef] [Green Version]
- Smith, B.D.; Morgan, R.L.; A Beckett, G.; Falck-Ytter, Y.; Holtzman, D.; Teo, C.-G.; Jewett, A.; Baack, B.; Rein, D.B.; Patel, N.; et al. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945–1965. MMWR Recomm. Rep. 2012, 61, 1–32. [Google Scholar]
- Kermode, M. Unsafe injections in low-income country health settings: Need for injection safety promotion to prevent the spread of blood-borne viruses. Health Promot. Int. 2004, 19, 95–103. [Google Scholar] [CrossRef]
- Jafari, S.; Copes, R.; Baharlou, S.; Etminan, M.; Buxton, J. Tattooing and the risk of transmission of hepatitis C: A systematic review and meta-analysis. Int. J. Infect. Dis. 2010, 14, e928–e940. [Google Scholar] [CrossRef] [Green Version]
- Benova, L.; Mohamoud, Y.A.; Calvert, C.; Abu-Raddad, L. Vertical Transmission of Hepatitis C Virus: Systematic Review and Meta-analysis. Clin. Infect. Dis. 2014, 59, 765–773. [Google Scholar] [CrossRef] [Green Version]
- Hagan, H.; Jordan, A.E.; Neurer, J.; Cleland, C. Incidence of sexually transmitted hepatitis C virus infection in HIV-positive men who have sex with men. Aids 2015, 29, 2335–2345. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.L.; Seeff, L.B. Natural history of hepatitis C. Clin. Liver Dis. 2005, 9, 383–398. [Google Scholar] [CrossRef]
- Erman, A.; Krahn, M.; Hansen, T.; Wong, J.; Bielecki, J.; Feld, J.J.; Wong, W.W.; Grootendorst, P.; Thein, H.-H. Estimation of fibrosis progression rates for chronic hepatitis C: A systematic review and meta-analysis update. BMJ Open 2019, 9, e027491. [Google Scholar] [CrossRef] [Green Version]
- Westbrook, R.H.; Dusheiko, G. Natural history of hepatitis C. J. Hepatol. 2014, 61 (Suppl. S1), S58–S68. [Google Scholar] [CrossRef] [Green Version]
- Cacoub, P.; Comarmond, C.; Domont, F.; Savey, L.; Desbois, A.C.; Saadoun, D. Extrahepatic manifestations of chronic hepatitis C virus infection. Ther. Adv. Infect. Dis. 2015, 3, 3–14. [Google Scholar] [CrossRef]
- Leigh, J.P.; Bowlus, C.L.; Leistikow, B.N.; Schenker, M. Costs of hepatitis C. Arch. Intern. Med. 2001, 161, 2231–2237. [Google Scholar] [CrossRef] [Green Version]
- Shah, B.B.; Wong, J.B. The Economics of Hepatitis C Virus. Clin. Liver Dis. 2006, 10, 717–734. [Google Scholar] [CrossRef]
- Zeuzem, S. Treatment options in hepatitis C: The current state of the art. Dtsch. Ärzteblatt Int. 2017, 114, 11. [Google Scholar]
- Hafez, T.A. Public Health and Economic Burden of Hepatitis C Infection in Developing Countries; Academic Press: Cambridge, MA, USA, 2018; pp. 25–32. [Google Scholar] [CrossRef]
- Presidency of Council of Ministers Central Adminstration of Statistics. The Republic of Lebanon. Available online: http://www.cas.gov.lb/index.php/about-lebanon-en (accessed on 11 December 2021).
- Chemaitelly, H.; Chaabna, K.; Abu-Raddad, L.J. The Epidemiology of Hepatitis C Virus in the Fertile Crescent: Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0135281. [Google Scholar] [CrossRef] [Green Version]
- United Nations Department of Economic and Social Affairs. World Population Prospects 2019. Available online: https://population.un.org/wpp/Download/Files/1_Indicators%20(Standard)/EXCEL_FILES/1_Population/WPP2019_POP_F01_1_TOTAL_POPULATION_BOTH_SEXES.xlsx (accessed on 11 December 2021).
- Lebanese Ministry of Public Health. National Strategy for Older Individuals. 2021. Available online: http://www.socialaffairs.gov.lb/admin/NewsImages/6432_3.pdf (accessed on 11 December 2021).
- United Nations Department of Economic and Social Affairs. World Populations Prospects: The 2008 Revisions, Highlights, and Advances; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2008. [Google Scholar]
- Rached, A.A.; Kheir, S.A.; Saba, J.; Ammar, W. Epidemiology of hepatitis B and hepatitis C in Lebanon. Arab. J. Gastroenterol. 2016, 17, 29–33. [Google Scholar] [CrossRef]
- Rached, A.A.; Kheir, S.A.; Saba, J.; Yaghi, C.; Ammar, W. Prevalence of Hepatitis C and Fibrosis Stage per Age Group in Lebanese Population. Gastroenterol. Insights 2017, 8, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Abou Rached, A.; Abou Kheir, S.; Saba, J.; Assaf, S.; Kassis, G.; Gonzalez, Y.S.; Ethgen, O. Hepatitis C in Lebanon: The burden of the disease and the value of comprehensive screening and treatment. Hepatic Med. Evid. Res. 2018, 10, 73. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global health sector strategy on viral hepatitis 2016-2021. Towards Ending Viral Hepatitis. World Health Organization. 2016. Available online: https://apps.who.int/iris/handle/10665/246177 (accessed on 11 December 2021).
- Rached, A.A.; Yaghi, C.; Khalil, L.; Saba, J.; Ammar, W. Prevalence of hepatitis C virus genotypes and subtypes in Lebanese population and major high risk groups. Arab. J. Gastroenterol. 2017, 18, 114–117. [Google Scholar] [CrossRef]
- Rached, A.A.; Nakhoul, M.; Richa, C.; Jreij, A.; Hanna, P.A.; Ammar, W. Prevalence of hepatitis B and anti-hepatitis C virus antibody among people who inject drugs in the Lebanese population. East. Mediterr. Health J. 2020, 26, 461–467. [Google Scholar] [CrossRef]
- Mahfoud, Z.; Kassak, K.; Kreidieh, K.; Shamra, S.; Ramia, S. Prevalence of antibodies to human immunodeficiency virus (HIV), hepatitis B and hepatitis C and risk factors in prisoners in Lebanon. J. Infect. Dev. Ctries. 2010, 4, 144–149. [Google Scholar] [CrossRef]
- Heijnen, M.; Mumtaz, G.R.; Abu-Raddad, L.J. Status of HIV and hepatitis C virus infections among prisoners in the Middle East and North Africa: Review and synthesis. J. Int. AIDS Soc. 2016, 19, 20873. [Google Scholar] [CrossRef] [Green Version]
- Makhoul, N.; Choueiri, M.; Kattar, M.; Soweid, A.; Shamseddeen, W.; Estephan, H.; Khalife, J.; Haddad, A.; Rached, A.A.; Zalloua, P. Distribution of hepatitis C virus (HCV) genotypes among HCV infection risk groups in Lebanon. J. Clin. Virol. 2008, 41, 166–167. [Google Scholar] [CrossRef]
- Sharara, A.I.; Ramia, S.; Ramlawi, F.; Fares, J.E.; Klayme, S.; Naman, R. Genotypes of hepatitis C virus (HCV) among positive Lebanese patients: Comparison of data with that from other Middle Eastern countries. Epidemiol. Infect. 2006, 135, 427–432. [Google Scholar] [CrossRef]
- Mahfoud, Z.; Kassak, K.; Kreidieh, K.; Shamra, S.; Ramia, S. Distribution of hepatitis C virus genotypes among injecting drug users in Lebanon. Virol. J. 2010, 7, 96. [Google Scholar] [CrossRef] [Green Version]
- Ramia, S.; Koussa, S.; Taher, A.; Haraki, S.; Klayme, S.; Sarkis, D.; Naman, R. Hepatitis-C-virus genotypes and hepatitis-G-virus infection in Lebanese thalassaemics. Ann. Trop. Med. Parasitol. 2002, 96, 197–202. [Google Scholar] [CrossRef]
- Inati, A.; Taher, A.; Ghorra, S.; Koussa, S.; Sheikh-Taha, M.; Aoun, E.; Sharara, A.I. Efficacy and tolerability of peginterferon alpha-2a with or without ribavirin in thalassaemia major patients with chronic hepatitis C virus infection. Br. J. Haematol. 2005, 130, 644–646. [Google Scholar] [CrossRef]
- Irani-Hakime, N.; Samaha, H.; Almawi, W.; Nasr, E.; Mokhbat, J.; Jaoude, M.A.; Daccache, J.; Rahal, E. Prevalence of hepatitis C virus isolate genotypes from chronically infected Lebanese patients: A hospital-based study. Leban. Med. J. 2005, 51, 121–126. [Google Scholar]
- Ashkani-Esfahani, S.; Alavian, S.M.; Salehi-Marzijarani, M. Prevalence of hepatitis C virus infection among hemodialysis patients in the Middle-East: A systematic review and meta-analysis. World J. Gastroenterol. 2017, 23, 151–166. [Google Scholar] [CrossRef]
- Denniston, M.M.; Klevens, R.M.; McQuillan, G.M.; Jiles, R.B. Awareness of infection, knowledge of hepatitis C, and medical follow-up among individuals testing positive for hepatitis C: National Health and Nutrition Examination Survey 2001–2008. Hepatology 2011, 55, 1652–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghaddar, A.; Nassar, K.; Elsoury, G. Barriers to Access to Sterile Syringes as Perceived by Pharmacists and Injecting Drug Users: Implications for Harm Reduction in Lebanon. Subst. Use Misuse 2017, 52, 1420–1428. [Google Scholar] [CrossRef] [PubMed]
- Haidar, A.; Adib, S.M. Les structures de santé et d’hygiène dans les prisons libanaises Health structures and hygiene in Lebanese prisons. J. Med. Liban. 2001, 49, 197–203. [Google Scholar] [PubMed]
- UNHCR. Lebanon at a Glance. Available online: https://www.unhcr.org/lb/at-a-glance (accessed on 11 December 2021).
- Fullman, N.; Yearwood, J.; Abay, S.M.; Abbafati, C.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; Abebe, Z.; Abebo, T.A.; Aboyans, V.; et al. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. Lancet 2018, 391, 2236–2271. [Google Scholar] [CrossRef]
- Bizri, A.R.; Khalil, P.B. A Lebanese physician’s dilemma: Not how, but with what? Lancet 2021, 398, 841. [Google Scholar] [CrossRef]
- Chao, D.T.; Abe, K.; Nguyen, M.H. Systematic review: Epidemiology of hepatitis C genotype 6 and its management. Aliment. Pharmacol. Ther. 2011, 34, 286–296. [Google Scholar] [CrossRef]
- Slim, J.; Afridi, M.S. Managing Adverse Effects of Interferon-Alfa and Ribavirin in Combination Therapy for HCV. Infect. Dis. Clin. N. Am. 2012, 26, 917–929. [Google Scholar] [CrossRef]
- Li, G.; De Clercq, E. Current therapy for chronic hepatitis C: The role of direct-acting antivirals. Antivir. Res. 2017, 142, 83–122. [Google Scholar] [CrossRef]
- Messina, J.P.; Humphreys, I.; Flaxman, A.; Brown, A.; Cooke, G.S.; Pybus, O.G.; Barnes, E. Global distribution and prevalence of hepatitis C virus genotypes. Hepatology 2014, 61, 77–87. [Google Scholar] [CrossRef] [Green Version]
- Shannon, C.E.; Weaver, W. The mathematical theory of communication. 1963. MD Comput. 1997, 14, 306–317. [Google Scholar]
- CDC. What is Hepatitis C. 2020. Available online: https://www.cdc.gov/hepatitis/hcv/cfaq.htm#E1 (accessed on 11 December 2021).
- Saffi, M.; Howard, N. Exploring the Effectiveness of Mandatory Premarital Screening and Genetic Counselling Programmes for β-Thalassaemia in the Middle East: A Scoping Review. Public Health Genom. 2015, 18, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Lebanese Ministry of Public Health. Quality and Safety: Blood Transfusions. Available online: https://www.moph.gov.lb/en/Pages/4/3262/blood-transfusion- (accessed on 11 December 2021).
- Haddad, A.; Assi, T.B.; Garraud, O. Can a decentralized blood system ensure self-sufficiency and blood safety? The Lebanese experience. J. Public Health Policy 2017, 38, 359–365. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Hepatitis Report. 2017. Available online: http://apps.who.int/iris/bitstream/10665/255016/1/9789241565455-eng.pdf (accessed on 11 December 2021).
- Hojati, S.A.; Maserat, E.; Ghorbani, M.; Safarpour, A.; Fattehi, M.R. Hepatitis C Treatment in Patients with Drug Addiction Is Effective or Not Effective? Med Arch. 2018, 72, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Paterson, B.L.; Backmund, M.; Hirsch, G.; Yim, C. The depiction of stigmatization in research about hepatitis C. Int. J. Drug Policy 2007, 18, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Marinho, R.T.; Barreira, D.P. Hepatitis C, stigma and cure. World J. Gastroenterol. 2013, 19, 6703–6709. [Google Scholar] [CrossRef]
- Larney, S.; Kopinski, H.; Beckwith, C.G.; Zaller, N.D.; Jarlais, D.D.; Hagan, H.; Rich, J.D.; Bergh, B.J.V.D.; Degenhardt, L. Incidence and prevalence of hepatitis C in prisons and other closed settings: Results of a systematic review and meta-analysis. Hepatology 2013, 58, 1215–1224. [Google Scholar] [CrossRef] [Green Version]
- Schulte, B.; Stover, H.; Thane, K.; Schreiter, C.; Gansefort, D.; Reimer, J. Substitution treatment and HCV/HIV-infection in a sample of 31 German prisons for sentenced inmates. Int. J. Prison. Health 2009, 5, 39–44. [Google Scholar] [CrossRef] [PubMed]
- James, B. Clean needles save lives. HIV and injecting drug use. AIDS Action 1993, 21, 4–5. [Google Scholar]
- Gassowski, M.; Nielsen, S.; Bannert, N.; Bock, C.-T.; Bremer, V.; Ross, R.S.; Wenz, B.; Marcus, U.; Zimmermann, R. History of detention and the risk of hepatitis C among people who inject drugs in Germany. Int. J. Infect. Dis. 2019, 81, 100–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaac, I.; Malaeb, M.; Khalil, A.B.; Musharrafieh, U.; Bizri, A. Infectious Diseases in Times of Conflict and War: The Loyal Companions. J. Infect. Dis. Epidemiol. 2020, 6, 172. [Google Scholar] [CrossRef]
- Lebanese Ministry of Public Health. Epidemiological Surveillance. 2021. Available online: https://www.moph.gov.lb/en/Pages/2/193/esu (accessed on 11 December 2021).
- U.S. Department of Labor. In Occupational Safety and Health Administration—Worker Protections against Occupational Exposure to Infectious Diseases; U.S. Department of Labor: Washington, DC, USA.
- American Association for the Study of Liver Diseases. Management of Acute HCV Infection Journal of Hepatology. Available online: https://www.hcvguidelines.org/unique-populations/acute-infection (accessed on 11 December 2021).
- European Association for the Study of the Liver. Recommendations on Treatment of Hepatitis C: Final Updater of the Series. J. Hepatol. 2020, 73, 1170–1218. Available online: https://www.journal-of-hepatology.eu/article/S0168-8278(20)30548-1/fulltext#secsectitle0360 (accessed on 11 December 2021).
- Sakr, C.J.; Alameddine, R.; Hoteit, R.; Daou, C.; Doudakian, R.; Kreidieh, K.; Musharrafieh, U.; Rahme, D.V. Occupational Exposure to Blood-Borne Pathogens among Healthcare Workers in a Tertiary Care Center in Lebanon. Ann. Work. Expo. Health 2021, 65, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Zigmund, S.; Ho, E.Y.; Masuda, M.; Ippolito, L.; LaBrecque, D.R. They treated me like a leper”: Stigmatization and the quality of life of patients with hepatitis C. J. Gen. Intern. Med. 2003, 18, 835–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, J.R.; Servidone, M.; Easterbrook, P.; Linas, B.P. Economic evaluation of HCV testing approaches in low and middle income countries. BMC Infect. Dis. 2017, 17, 697. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
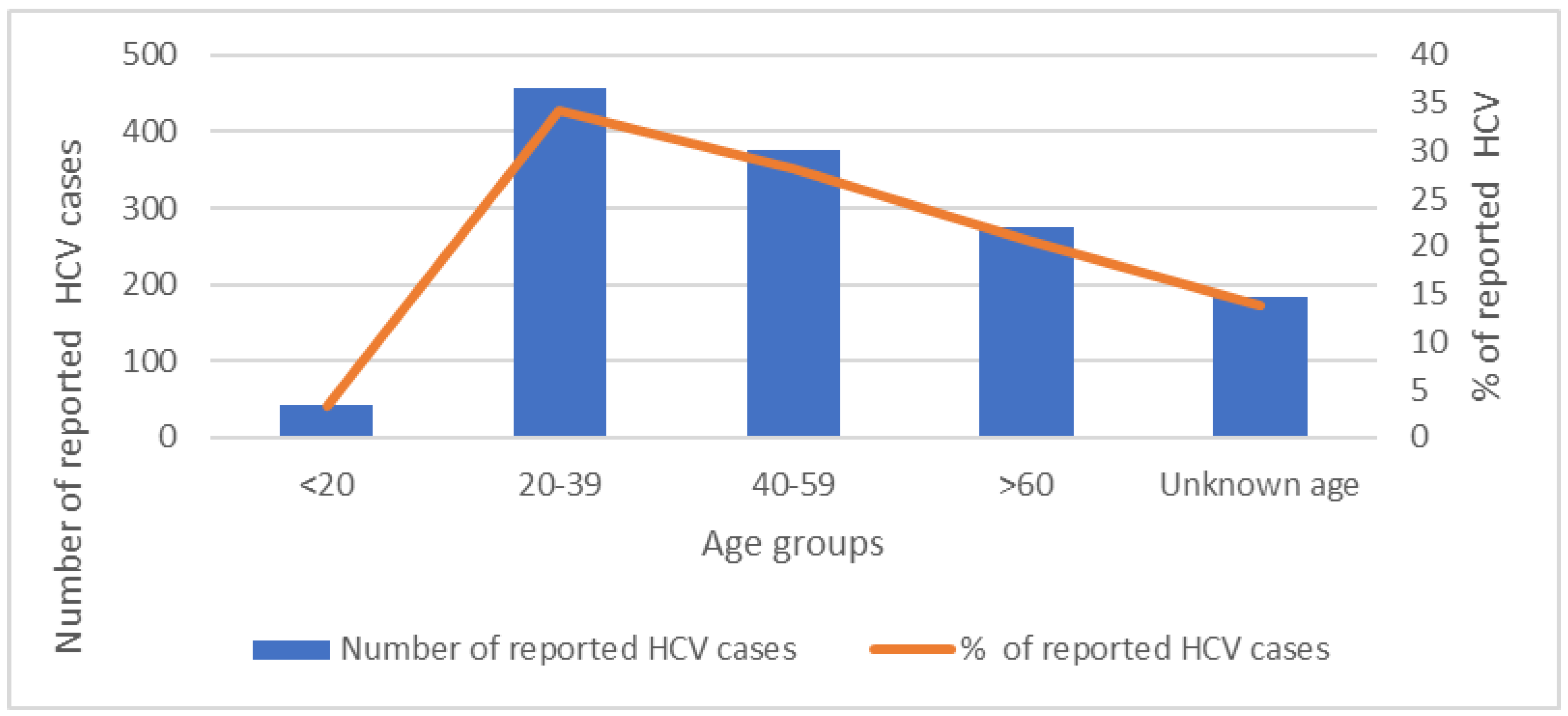
| <20 Years | 20–39 Years | 40–59 Years | >60 Years | Unknown Age | Total | |
|---|---|---|---|---|---|---|
| HCV Number | 43 | 456 | 376 | 275 | 183 | 1333 |
| HCV % | 3.2% | 34.2% | 28.2% | 20.6% | 13.7% |
| Genotype | PWID | Hemodialysis | Transfusion | Sexual | Vertical | Unknown | Total |
|---|---|---|---|---|---|---|---|
| 1 | 34.5% | 61.7% | 56.3% | 0 | 100% | 23.1% | 47% |
| 2 | 6.9% | 2.2% | 1.4% | 0% | 0% | 2.1% | 3.7% |
| 3 | 37.9% | 0% | 3.5% | 0% | 0% | 5.2% | 14.1% |
| 4 | 17.2% | 36.1% | 38.7% | 100% | 0% | 24.7% | 33.9% |
| 5 | 3.4% | 0.0% | 0% | 0% | 0% | 0.8% | 1.4% |
| Total | 28.1% | 17.7% | 27.5% | 0.3% | 0.2% | 26.1% | 1031 |
| Targeted Population | Current Strategies | Recommendations | References |
|---|---|---|---|
| Community at large | - Premarital screening. - No current universal screening. | - At least once, screen people ≥ 18 years old. - Educate about the nature of the disease, modes of transmission, and the availability of curative treatment. | [49,50,51,52] Table 1 Figure 1 and Figure 4 |
| Incarcerated individuals | - No current HCV screening policy. | - Screen regularly. - Link those who test positive to care. - Improve prison conditions (hygiene). - Educate about modes of transmission and safe needle use and safer sexual practices. - Establish needle-exchange programs. - Provide post-release support. - Screen guards and employees working at prisons. | [49,57,58,59,60] |
| PWID | - NGO-based counseling centers. - NGO-based needle distribution. | - Implement strategies to reach PWIDs. - Screen regularly. - Link those who test positive to care. - Educate about modes of transmission and safe drug (needles) use, social behaviors, and sexual practices. - Establish needle-exchange programs. - Eliminate stigma by raising awareness among the general population and medical staff. | [49,53,54,55,56] |
| Foreign working force | - Screen prior to work permit. | - Link positive individuals to care in collaboration with ILO. | |
| Refugees | - No available data. | - Apply same screening and preventive strategies as those of the Lebanese population. - Work closely with UNRWA, UNHCR, and other NGOs to screen and treat positive individuals. | [61,62] |
| Hemodialysis | - Screen patients twice annually. | Keep same. | [49] |
| Blood bank | - Screen blood products and blood. | Keep same. Encourage self-deferral. | [49] |
| Healthcare workers | - Provide appropriate PPE. - Abide by universal precautions. - Train on safe injection practices and sharps disposal.- Provide PEP. | Keep same. | [49,63,64,65] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayoub, N.; Hatab, T.; Bizri, A.R. Challenges Facing Viral Hepatitis C Elimination in Lebanon. Pathogens 2023, 12, 432. https://doi.org/10.3390/pathogens12030432
Ayoub N, Hatab T, Bizri AR. Challenges Facing Viral Hepatitis C Elimination in Lebanon. Pathogens. 2023; 12(3):432. https://doi.org/10.3390/pathogens12030432
Chicago/Turabian StyleAyoub, Nour, Taha Hatab, and Abdul Rahman Bizri. 2023. "Challenges Facing Viral Hepatitis C Elimination in Lebanon" Pathogens 12, no. 3: 432. https://doi.org/10.3390/pathogens12030432