
Major Depressive Disorder and Pulmonary Tuberculosis Comorbidity Exacerbates Proinflammatory Immune Response—A Preliminary Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Antibodies and Reagents
2.3. Blood Samples
2.4. Cell Culture and Flow Cytometry
2.5. Cytokine Measurement
2.6. Statistical Analysis
3. Results
3.1. Mayor Depressive Disorder Was Frequent in TB Patients

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy Controls (n = 11) | MDD Patients (n = 11) | TB Patients (n = 19) | MDD-TB Patients (n = 13) | |
|---|---|---|---|---|
| Age (years) | 28.9 ± 3.6 | 35.5 ± 9.0 | 44.2 ± 15.0 | 49.5 ± 18.8 |
| Gender | ||||
| Men | 5 (45.5%) | 0 (0.0%) | 8 (42.1%) | 8 (66.7%) |
| Women | 6 (54.5%) | 11 (100%) | 11 (57.9%) | 5 (33.3%) |
| BDI score | 1.9 ± 3.1 | 38.4 ± 11.5 | 4.5 ± 2.0 | 20.8 ± 3.3 |
| HDRS score | 1.0 ± 1.7 | 24.4 ± 4.8 | 3.4 ± 2.0 | 24.8 ± 3.0 |
| WHOQOL score | 98.8 ± 5.4 | 65.6 ± 16.4 | 92.7 ± 12.8 | 66.3 ± 14.5 |
3.2. High Intracellular IFN-γ-Producing Activated Cell Percentage in MDD-TB Patients
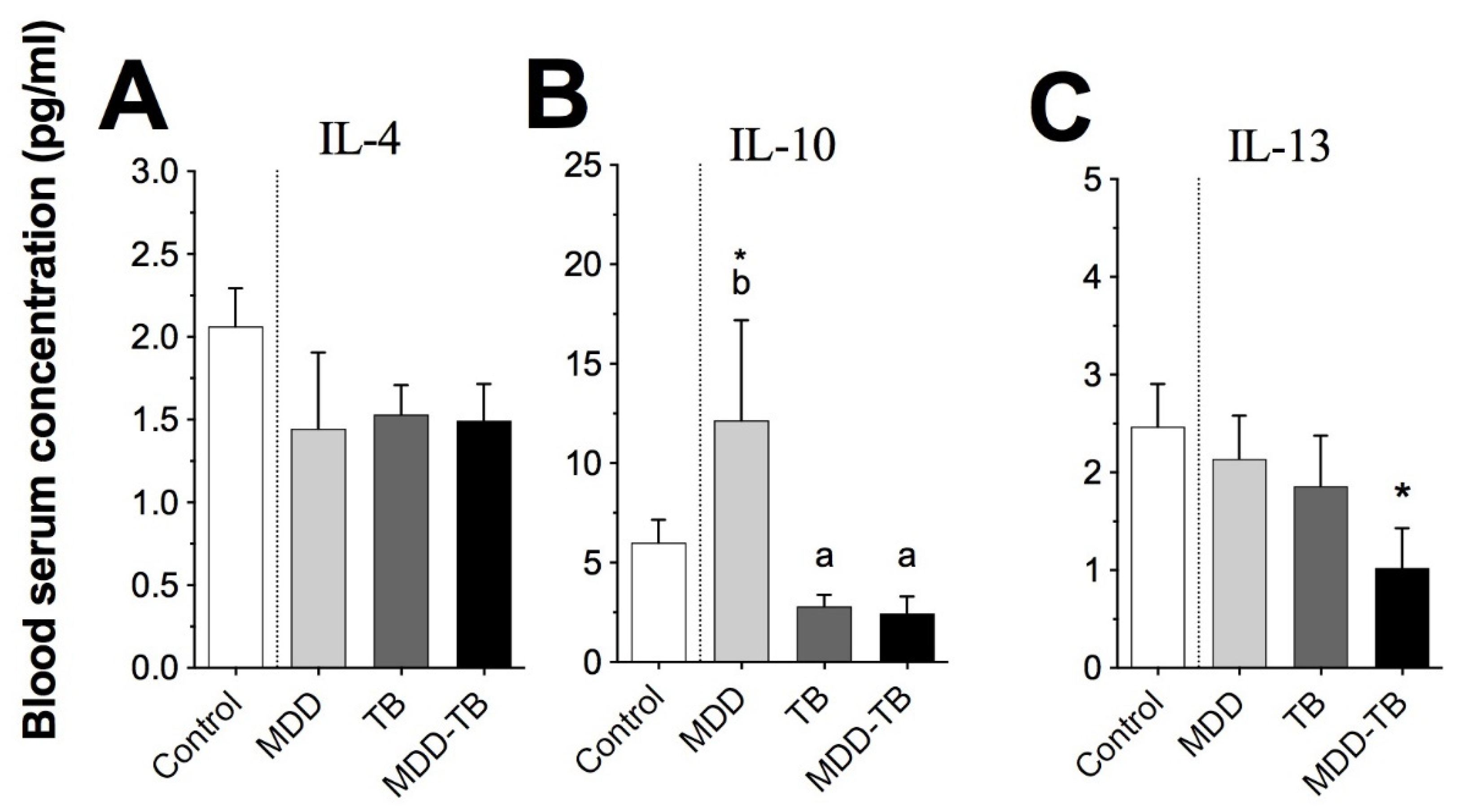
3.3. Low Levels of Serum Anti-Inflammatory Cytokines Were Strongly Associated to the MDD-TB Group
3.4. Serums MCP-1β and IL-8 Showed Similar Levels in Mtb-Infected Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Available online: https://apps.who.int/iris/handle/10665/254610 (accessed on 21 November 2019).
- Miller, A.H.; Maletic, V.; Raison, C.L. Inflammation and its discontents: The role of cytokines in the pathophysiology of major depression. Biol. Psychiatry 2009, 65, 732–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A meta-analysis of cytokines in major depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ho, R.C.; Mak, A. Interleukin (IL)-6, tumour necrosis factor alpha (TNF-alpha) and soluble interleukin-2 receptors (sIL-2R) are elevated in patients with major depressive disorder: A meta-analysis and meta-regression. J. Affect. Disord. 2012, 139, 230–239. [Google Scholar] [CrossRef]
- Thom, R.; Silbersweig, D.A.; Boland, R.J. Major depressive disorder in medical illness: A review of assessment, prevalence, and treatment options. Psychosom. Med. 2019, 81, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Husain, M.O.; Dearman, S.P.; Chaudhry, I.B.; Rizvi, N.; Waheed, W. The relationship between anxiety, depression and illness perception in tuberculosis patients in Pakistan. Clin. Pract. Epidemiol. Ment. Health 2008, 4, 4. [Google Scholar] [CrossRef] [Green Version]
- Moussas, G.; Tselebis, A.; Karkanias, A.; Stamouli, D.; Ilias, I.; Bratis, D.; Vassila-Demi, K. A comparative study of anxiety and depression in patients with bronchial asthma, chronic obstructive pulmonary disease and tuberculosis in a general hospital of chest diseases. Ann. Gen. Psychiatry 2008, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Ige, O.M.; Lasebikan, V.O. Prevalence of depression in tuberculosis patients in comparison with non-tuberculosis family contacts visiting the DOTS clinic in a Nigerian tertiary care hospital and its correlation with disease pattern. Ment. Health Fam. Med. 2011, 8, 235–241. [Google Scholar]
- Peltzer, K.; Naidoo, P.; Matseke, G.; Louw, J.; McHunu, G.; Tutshana, B. Prevalence of psychological distress and associated factors in tuberculosis patients in public primary care clinics in South Africa. BMC Psychiatry 2012, 12, 89. [Google Scholar] [CrossRef] [Green Version]
- Masumoto, S.; Yamamoto, T.; Ohkado, A.; Yoshimatsu, S.; Querri, A.G.; Kamiya, Y. Prevalence and associated factors of depressive state among pulmonary tuberculosis patients in Manila, The Philippines. Int. J. Tuberc. Lung Dis. 2014, 18, 174–179. [Google Scholar] [CrossRef] [Green Version]
- Duko, B.; Gebeyehu, A.; Ayano, G. Prevalence and correlates of depression and anxiety among patients with tuberculosis at Wolaita Sodo University Hospital and Sodo Health Center, Wolaita Sodo, South Ethiopia. BMC Psychiatry 2015, 15, 214. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Tuberculosis Report 2019. Available online: https://www.who.int/tb/publications/global_report/en/ (accessed on 7 May 2020).
- Cooper, A.M.; Roberts, A.D.; Rhoades, E.R.; Callahan, J.E.; Getzy, D.M.; Orme, I.M. The role of interleukin-12 in acquired immunity to Mycobacterium tuberculosis infection. Immunology 1995, 84, 423–432. [Google Scholar]
- Flynn, J.L.; Chan, J. Immunology of tuberculosis. Annu. Rev. Immunol. 2001, 19, 93–129. [Google Scholar] [CrossRef] [PubMed]
- Clay, H.; Volkman, H.E.; Ramakrishnan, L. Tumor necrosis factor signaling mediates resistance to mycobacteria by inhibiting bacterial growth and macrophage death. Immunity 2008, 29, 283–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonecini-Almeida, M.G.; Ho, J.L.; Boéchat, N.; Huard, R.C.; Chitale, S.; Doo, H.; Geng, J.; Rego, L.; Lazzarini, L.C.; Kritski, A.L.; et al. Down-modulation of lung immune responses by interleukin-10 and transforming growth factor beta (TGF-beta) and analysis of TGF-beta receptors I and II in active tuberculosis. Infect. Immun. 2004, 72, 2628–2634. [Google Scholar] [CrossRef] [Green Version]
- Ndishimye, P.; Seghrouchni, F.; Domokos, B.; Soritau, O.; Sadak, A.; Homorodean, D.; Aouada, R.E.; Pop, C.M. Evaluation of interleukin-10 levels in the plasma of patients with various stages of tuberculosis. Clujul Med. 2015, 88, 164–167. [Google Scholar] [CrossRef] [Green Version]
- American Thoracic Society; The Centers for Disease Control and Prevention. Diagnostic Standards and classification of tuberculosis in adults and children. Am. J. Respir. Crit. Care Med. 2000, 161, 1376–1395. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Section II: Depressive disorders. In DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Kupfer, D.J., Regier, D.A., Arango-López, C., Ayuso-Mateos, J.L., Vieta-Pascual, E., Bagney-Lifante, A., Eds.; American Psychiatric Association Publisher: Washington, DC, USA, 2013; pp. 104–108. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- WHOQOL Group. Study protocol for the World Health Organization project to develop a quality of life assessment instrument (WHOQOL). Qual. Life Res. 1993, 2, 153–159. [Google Scholar] [CrossRef]
- Boyum, A. Isolation of lymphocytes, granulocytes and macrophages. Scand. J. Immunol. 1976, 5, 9–15. [Google Scholar] [CrossRef]
- D’Agostino, R.B. Tests for the normal distribution. In Goodness-of-Fit Techniques; D’Agostino, R.B., Stephens, M.A., Eds.; Marcel Dekker: New York, NY, USA, 1986; pp. 367–420. [Google Scholar]
- Snedecor, G.W.; Cochran, W.G. Analysis of variance. In Statistical Methods, 8th ed.; Snedecor, G.W., Cochran, W.G., Eds.; Iowa State University Press: Ames, IA, USA, 1989; pp. 251–252. [Google Scholar]
- Dunnett, C.W. A multiple comparison procedure for comparing several treatments with a control. J. Am. Stat. Assoc. 1955, 50, 1096–1121. [Google Scholar] [CrossRef]
- Dunnett, C.W. New tables for multiple comparisons with a control. Biometrics 1964, 20, 482–491. [Google Scholar] [CrossRef] [Green Version]
- Tukey, J.W. Comparing individual means in the analysis of variance. Biometrics 1949, 5, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.S.; Santos, N.C.; Cunha, P.; Cotter, J.; Sousa, N. The use of multiple correspondence analysis to explore associations between categories of qualitative variables in healthy ageing. J. Aging Res. 2013, 2013, 302163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbas, A.K.; Lichtman, A.H.; Pillai, S. Cellular and Molecular Immunology, 9th ed.; Elsevier Inc.: Philadelphia, PA, USA, 2018; pp. 52–53. [Google Scholar]
- Jiménez-Fernandez, S.; Gurpegui, M.; Díaz-Atienza, F.; Pérez-Costillas, L.; Gerstenberg, M.; Correll, C.U. Oxidative stress and antioxidant parameters in patients with major depressive disorder compared to healthy controls before and after antidepressant treatment: Results from a meta-analysis. J. Clin. Psychiatry 2015, 76, 1658–1667. [Google Scholar] [CrossRef]
- Seo, Y.B.; Im, S.J.; Namkoong, H.; Kim, S.W.; Choi, Y.W.; Kang, M.C.; Lim, H.S.; Jin, H.T.; Yang, S.H.; Cho, M.L.; et al. Crucial roles of interleukin-7 in the development of T follicular helper cells and in the induction of humoral immunity. J. Virol. 2014, 88, 8998–9009. [Google Scholar] [CrossRef] [Green Version]
- Lehto, S.M.; Huotari, A.; Niskanen, L.; Herzig, K.H.; Tolmunen, T.; Viinamäki, H.; Koivumaa-Honkanen, H.; Honkalampi, K.; Sinikallio, S.; Ruotsalainen, H.; et al. Serum IL-7 and G-CSF in major depressive disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2010, 34, 846–851. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarez-Sekely, M.; Lopez-Bago, A.; Báez-Saldaña, R.; Pezoa-Jares, R.E.; Gorocica, P.; Zenteno, E.; Lascurain, R.; Saldívar-González, A. Major Depressive Disorder and Pulmonary Tuberculosis Comorbidity Exacerbates Proinflammatory Immune Response—A Preliminary Study. Pathogens 2023, 12, 361. https://doi.org/10.3390/pathogens12030361
Alvarez-Sekely M, Lopez-Bago A, Báez-Saldaña R, Pezoa-Jares RE, Gorocica P, Zenteno E, Lascurain R, Saldívar-González A. Major Depressive Disorder and Pulmonary Tuberculosis Comorbidity Exacerbates Proinflammatory Immune Response—A Preliminary Study. Pathogens. 2023; 12(3):361. https://doi.org/10.3390/pathogens12030361
Chicago/Turabian StyleAlvarez-Sekely, Magaly, Ana Lopez-Bago, Renata Báez-Saldaña, Rodolfo E. Pezoa-Jares, Patricia Gorocica, Edgar Zenteno, Ricardo Lascurain, and Alfredo Saldívar-González. 2023. "Major Depressive Disorder and Pulmonary Tuberculosis Comorbidity Exacerbates Proinflammatory Immune Response—A Preliminary Study" Pathogens 12, no. 3: 361. https://doi.org/10.3390/pathogens12030361