
COVID-19, Framing and Naming a Pandemic: How What Is Not in a Disease Name May Be More Important than What Is
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Disease Framing, When Similarities of Kind Get in the Way of Differences in Degree
1.1. The Basics
1.2. COVID-19 in the “Public Square”
2. Rethinking Uncertainty, Public Health Messaging between Risk and Vulnerability
“We are certainly right now in this country out of the pandemic phase…”Fauci, 4/27/22 NPR [33].
“It’s not over…” “We are in a different moment of the pandemic.”Fauci, 4/28/22 APNews [34].
3. Beyond Labeling, Disease Names as Important Frames for Public Health Messaging
ICTV announced “severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)” as the name of the new virus on 11 February 2020. This name was chosen because the virus is genetically related to the coronavirus responsible for the SARS outbreak of 2003. While related, the two viruses are different.[42]
4. How Acronyms Alienate Audiences, Overestimate Understanding, and Complicate Communication
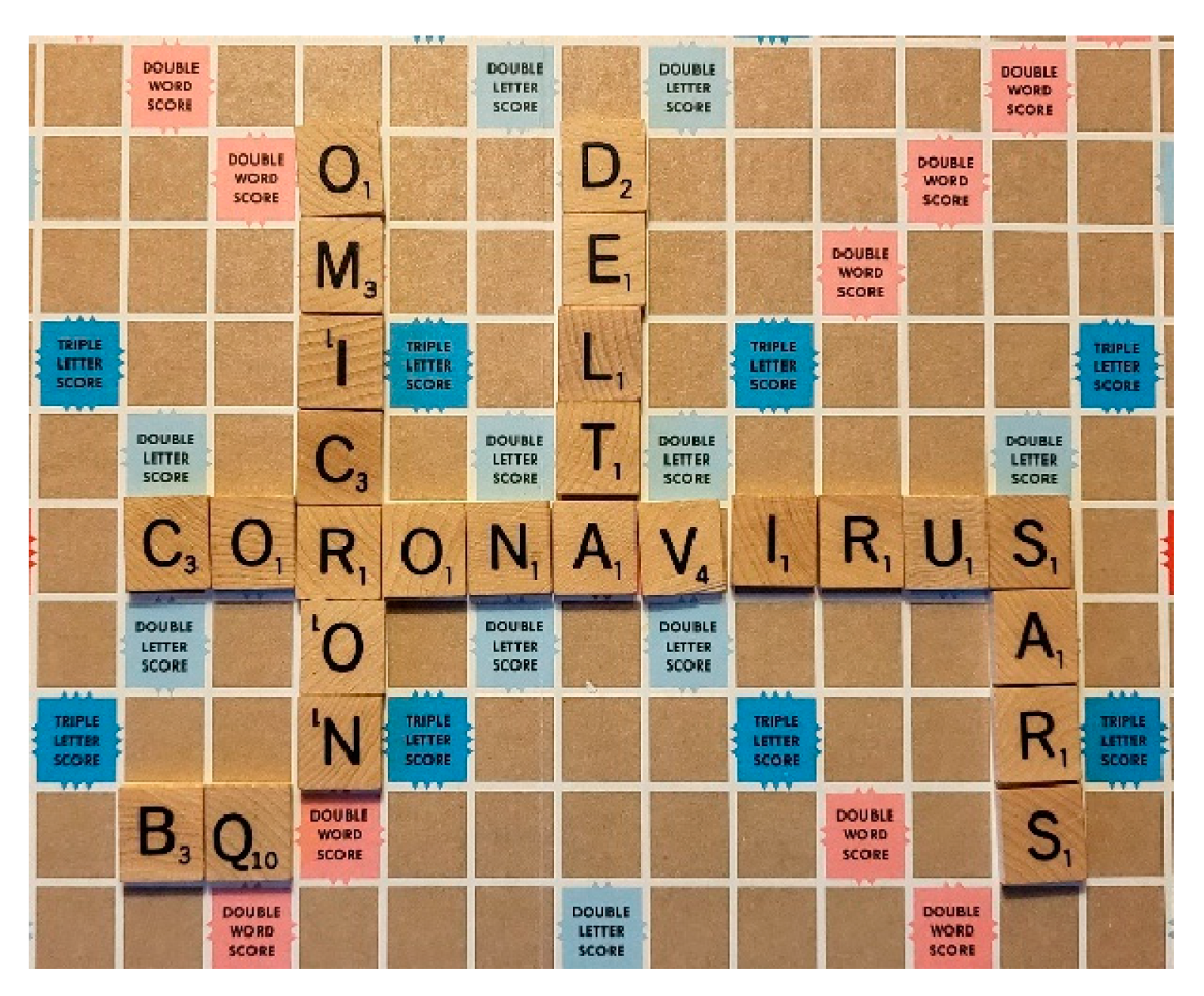
We’ve been repeating a pattern. Now with these new omicron subvariants—I call them the Scrabble variants, because they’re these high-valued Scrabble letters such as Q and X and B. We’re seeing cases go up again (excerpt from Andrew Dansby’s interview with Peter Hotez, published 17 October 2022 in RE/New Houston).
5. The Lingering and Malignant Place of Prejudice in Public Health Messaging
6. Considering Disease Names That Can Frame Public Health Messages
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers For Disease Control and Prevention. COVID-19 Vaccines & Boosters . 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/faq.html#Basics (accessed on 2 May 2021).
- Gibson, J.J. The theory of affordances. In Perceiving, Acting, and Knowing; Shaw, R.E., Bransford, J., Eds.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1977. [Google Scholar]
- James, J.G. The Ecological Approach to Visual Perception; Houghton Mifflin: Boston, MA, USA, 1979. [Google Scholar]
- Goffman, E. Frame Analysis: An Essay on the Organization of Experience/Erving Goffman; Harper & Row; Harvard University: Cambridge, MA, USA, 1974. [Google Scholar]
- Hallahan, K. Strategic Framing. In The International Encyclopedia of Communication; Donsbach, W., Ed.; 2008. [Google Scholar] [CrossRef]
- Lakoff, G. Metaphors We Live By; University of Chicago Press: Chicago, IL, USA, 1980. [Google Scholar]
- Kapur, R.L. Commentary on culture bound syndromes and international disease classification. Cult. Med. Psych. 1987, 11, 43–48. [Google Scholar] [CrossRef]
- Entman, R. Framing: Toward Clarification of a Fractured Paradigm. J. Commun. 1993, 43, 51–58. [Google Scholar] [CrossRef]
- Hymes, D. Introduction: Toward Ethnographies of Communication. Am. Anthropol. 1964, 66, 1–34. [Google Scholar] [CrossRef]
- Gentner, D.; Jeziorski, M. The shift from metaphor to analogy in Western science. In Metaphor and Thought; Cambridge University Press: Cambridge, UK, 1993; pp. 447–480. [Google Scholar]
- Lakoff, G. Metaphor and War: The Metaphor System Used to Justify War in the Gulf. Cogn. Semiot. 1992, 4, 5–19. [Google Scholar] [CrossRef]
- Thibodeau Hendricks, R.K.; Boroditsky, L. How Linguistic Metaphor Scaffolds Reasoning. Trends Cogn. Sci. 2017, 21, 852–863. [Google Scholar] [CrossRef]
- Patwa Sharma, S.; Pykl, S.; Guptha, V.; Kumari, G.; Akhtar, M.S.; Ekbal, A.; Das, A.; Chakraborty, T. Fighting an Infodemic: COVID-19 Fake News Dataset. In Combating Online Hostile Posts in Regional Languages during Emergency Situation; Springer International Publishing: Cham, Switzerland, 2021; pp. 21–29. [Google Scholar] [CrossRef]
- Briggs, C.; Hallin, D.C. Biocommunicability: The neoliberal subject and its contradictions in news coverage of health issues. Soc. Text 2007, 93, 43–66. [Google Scholar] [CrossRef]
- Kleinman, A. The Illness Narratives; Basic Books: New York, NY, USA, 1988. [Google Scholar]
- KUTV. 2020. Available online: https://kutv.com/news/coronavirus/gallery/photos-96-protest-signs-spotted-at-nationwide-rallies-against-stay-at-home-orders#photo-11 (accessed on 20 May 2020).
- Briggs, C.; Charles, L.; Mantini-Briggs, C. Tell Me Why My Children Died: Rabies, Indigenous Knowledge, and Communicative Justice. In Critical Global Health: Evidence, Efficacy, Ethnography; Duke University Press: Durham, UK, 2016. [Google Scholar]
- Bennett, P. Risk Communication and Public Health; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Frewer, W. Public Risk Perceptions and Risk Communication. In Risk Communication and Public Health; Bennet, P., Calman, K., Eds.; Oxford University Press: Oxford, UK, 1997; pp. 3–19. [Google Scholar]
- Harvey, T.S. Cyanobacteria Blooms: Maya Peoples between the Politics of Risk and the Threat of Disaster. Med. Anthropol. Cross Cult. Stud. Health Illn. 2012, 31, 477–496. [Google Scholar] [CrossRef]
- Williamson Herald. 2020. Available online: https://www.williamsonherald.com/news/mask-mandate-protesters-rally-on-franklin-square/article_de15b866-179d-11eb-8af2-6318ea3c51f3.html (accessed on 30 October 2022).
- Kasperson, R.; Renn, O.; Slovic, P.; Brown, H.; Emel, J.; Goble, R.; Kasperson, J.; Ratick, S. The Social Amplification of Risk: A Conceptual Framework. Risk Anal. 1988, 8, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Pidgeon, N.; Kasperson, R.E.; Slovic, P. The Social Amplification of Risk; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Wallace Davis, M. Big Farms Make Big Flu: Dispatches on Influenza, Agribusiness, and the Nature of Science; Monthly Review Press: New York, NY, USA, 2016. [Google Scholar]
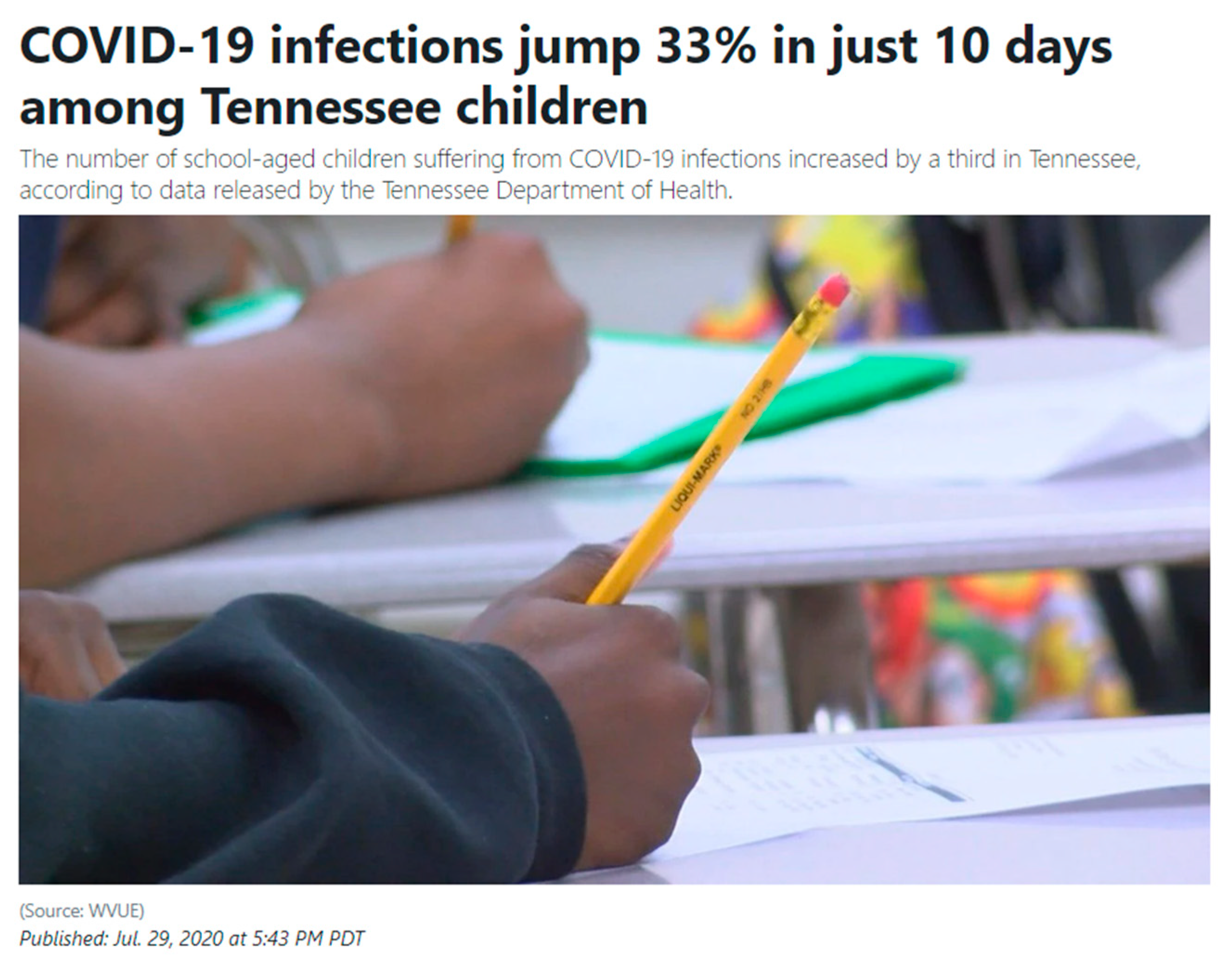
- WTVF/WVLT 2020. COVID-19 Infections Jump 33% in Just 10 Days among Tennessee Children (wvlt.tv). Available online: https://www.wvlt.tv/2020/07/30/covid-19-infections-jump-33-in-just-10-days-among-tennessee-children/ (accessed on 31 July 2020).
- Foucault, M. Discipline and Punish: The Birth of a Prison; Penguin: London, UK, 1991. [Google Scholar]
- Braveman, P.; Gottlieb, L. The Social Determinants of Health: It’s Time to Consider the Causes of the Causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Napier David, A.; Depledge, M.; Knipper, M.; Lovell, R.; Ponarin, E.; Sanabria, E.; Thomas, F. Culture Matters: Using a Cultural Contexts of Health Approach to Enhance Policy-Making; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2017. [Google Scholar]
- Paules Marston, H.D.; Fauci, A.S. Coronavirus Infections—More Than Just the Common Cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [Green Version]
- Coombs, T.W. The parameters for crisis communication. In The Handbook of Crisis Communication; Coombs, W.T., Holladay, S.J., Eds.; Wiley-Blackwell: Singapore, 2010; pp. 17–57. [Google Scholar]
- Button, G. Disaster Culture Knowledge and Uncertainty in the Wake of Human and Environmental Catastrophe; Left Coast Press: Walnut Creek, CA, USA, 2010. [Google Scholar]
- World Health Organization. Communicating Risk in Public Health Emergencies: A WHO Guideline for Emergency Risk Communication (ERC) Policy and Practice; License: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/259807 (accessed on 4 April 2020).
- NPR. 2022. Available online: https://www.npr.org/2022/04/27/1094997608/fauci-us-pandemic-phase-covid-19 (accessed on 4 April 2020).
- APNews. 2022. Available online: https://apnews.com/article/covid-health-pandemics-infectious-diseases-united-states-b7fbd92253900045321878d97b8e1b89 (accessed on 14 December 2022).
- Ungar, S. Moral panic versus the risk society. In Understanding Deviance: Connecting Classical and Contemporary Perspectives; Routledge: Oxfordshire, UK, 2014; p. 371. [Google Scholar]
- Pidgeon, N.; Henwood, K.; Maguire, B. Public health communication and the social amplification of risks: Present knowledge and future prospects. In Handbook of Environmental Risk and Management; Blackwell Science: Oxford, UK, 1999; pp. 289–318. [Google Scholar]
- Green, J.; Fischer, E.F.; Fitzgerald, D.; Harvey, T.S.; Thomas, F. The publics of public health: Learning from COVID-19. Crit. Public Health 2022, 32, 592–599. [Google Scholar] [CrossRef]
- Andreu, S.; Martin-Pascual, M.-A. Fake images of the SARS-CoV-2 coronavirus in the communication of information at the beginning of the first Covid-19 pandemic. El Prof. De La Inf. 2020, 29, e290309. [Google Scholar] [CrossRef]
- Basch Hillyer, G.C.; Jaime, C. COVID-19 on TikTok: Harnessing an emerging social media platform to convey important public health messages. Int. J. Adolesc. Med. Health 2020, 34, 367–369. [Google Scholar] [CrossRef]
- Orso Federici, N.; Copetti, R.; Vetrugno, L.; Bove, T. Infodemic and the spread of fake news in the COVID-19-era. Eur. J. Emerg. Med. 2020, 27, 327–328. [Google Scholar] [CrossRef]
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- World Health Organization. Naming the Coronavirus Disease (COVID-19) and the Virus that Causes It. 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 20 February 2021).
- Trostle, J.A. Chapter 7: Perceiving and Representing Risk. In Epidemiology and Culture; Cambridge University Press: Cambridge, UK, 2005; pp. 150–167. [Google Scholar]
- Islam, M.S.; Sujan MS, H.; Tasnim, R.; Sikder, M.T.; Potenza, M.N.; Van Os, J. Psychological Responses During the COVID-19 Outbreak Among University Students in Bangladesh. PLoS ONE 2020, 15, e0245083. [Google Scholar] [CrossRef]
- Toppenberg-Pejcic, D.; Noyes, J.; Allen, T.; Alexander, N.; Vanderford, M.; Gamhewage, G. Emergency Risk Communication: Lessons Learned from a Rapid Review of Recent Gray Literature on Ebola, Zika, and Yellow Fever. Health Commun. 2019, 34, 437–455. [Google Scholar] [CrossRef]
- Brown, P. Naming and Framing: The Social Construction of Diagnosis and Illness. J. Health Soc. Behav. 1995, 35, 34–52. [Google Scholar] [CrossRef] [Green Version]
- Simons, R.C. A feasible and timely enterprise: Commentary on “culture-bound syndromes and international disease classifications” by Raymond Prince and Françoise Tcheng-Laroche. Cult. Med. Psych. 1987, 11, 21–28. [Google Scholar] [CrossRef]
- Gaines, A.D. From DSM-I to III-R; Voices of Self, Mastery and the Other: A Cultural Constructivist Reading of U.S. Psychiatric Classification. Soc. Sci. Med. (1982) 1992, 35, 3–24. [Google Scholar] [CrossRef]
- Smith, L.; Nelson, C. International intelligibility of English: Directions and resources. World Engl. 1985, 4, 333–342. [Google Scholar] [CrossRef]
- Briggs, C.L. Beyond the Linguistic/Medical Anthropology Divide: Retooling Anthropology to Face COVID-19. Med. Anthropol. 2020, 39, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Harvey, T.S. Wellness Beyond Words; University of New Mexico Press: Albuquerque, NM, USA, 2013. [Google Scholar]
- Mantini-Briggs, C.; Briggs, C.L. Stories in the Time of Cholera: Racial Profiling During a Medical Nightmare, 1st ed.; University of California Press: Berkeley, CA, USA, 2003. [Google Scholar] [CrossRef]
- Briggs, C.L. Communicability, Racial Discourse, and Disease. Annu. Rev. Anthropol. 2005, 34, 269–291. [Google Scholar] [CrossRef]
- Briggs, C.L. Why Nation-States and Journalists Can’t Teach People to Be Healthy: Power and Pragmatic Miscalculation in Public Discourses on Health. Med. Anthropol. Q. 2003, 17, 287–321. Available online: http://www.jstor.org/stable/3655387 (accessed on 23 June 2021). [CrossRef] [PubMed]
- Hayes Michael, V. On the epistemology of risk: Language, logic and social science. Soc. Sci. Med. 1992, 35, 401–407. [Google Scholar] [CrossRef]
- Jakobson, R. Linguistics and Poetics. In Style in Language; Sebeok, T., Ed.; M.I.T. Press: Cambridge, MA, USA, 1960; pp. 350–377. [Google Scholar]
- Ochs, E. Indexing gender. Rethinking Context: Language as an Interactive Phenomenon; Duranti, A., Goodwin, C., Eds.; Cambridge University Press: Cambridge, UK, 1992; pp. 335–358. [Google Scholar]
- Trouillot, M.R. Anthropology and the Savage Slot: The Poetics and Politics of Otherness. In Global Transformations; Palgrave Macmillan: New York, NY, USA, 2003. [Google Scholar] [CrossRef]
- Austin, J.L. How to Do Things with Words, 2nd ed.; Urmson, J.O., Marina, S., Eds.; Harvard University Press: Cambridge, MA, USA, 1975. [Google Scholar]
- Tan, H.-T.; Wang, E.Y.; Yoo, G.-S. Who likes jargon? The joint effect of jargon type and industry knowledge on investors’ judgments. J. Account. Econ. 2019, 67, 416–437. [Google Scholar] [CrossRef]
- Agha, A. Registers of Language. In A Companion to Linguistic Anthropology; Alessandro, D., Ed.; Blackwell: New York, NY, USA; Oxford, UK, 2004; pp. 23–45. [Google Scholar]
- Plavén-Sigray, P.; Matheson, G.J.; Schiffler, B.C.; Thompson, W.H. The readability of scientific texts is decreasing over time. eLife 2017, 6, e27725. [Google Scholar] [CrossRef]
- Barnett, A.; Doubleday, Z. Meta-Research: The growth of acronyms in the scientific literature. eLife 2020, 9, e60080. [Google Scholar] [CrossRef]
- Barnett, A.; Zoe, D. Science Is Becoming Less Readable as the Number of New Acronyms Boom; OSF: Minato, Tokyo, 2020. [Google Scholar]
- Hales, A.H.; Williams, K.D.; Rector, J. Alienating the audience: How abbreviations hamper scientific communication. Assoc. Psychol. Sci. Obs. 2017, 30, 22–24. [Google Scholar]
- Rakedzon, T.; Segev, E.; Chapnik, N. Automatic jargon identifier for scientists engaging with the public and science communication educators. PLoS ONE 2017, 12, e0181742. [Google Scholar] [CrossRef] [Green Version]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Risk communication: An integral element in public health emergencies. Int. J. Prev. Med. 2016, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Harvey, T.S. Muddying the Waters: Protection, Public Participation, and Ambiguity in the Language of Pollution in the Great Lakes. Cult. Agric. Food Environ. 2015, 37, 107–115. [Google Scholar] [CrossRef]
- Cultural Issues and Linguistic Complications in Health Communication. In International Encyclopedia of Public Health, 2nd ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2017; pp. 202–207.
- Randall, J.H.; Graf, L.R. Linguistics meets “legalese”: Syntax, semantics, and jury instruction reform. LSA Annu. Meet. Ext. Abstr. 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Adams, D.C.; Bitetti, M.S.D.; Janson, C.H.; Slobodkin, L.B.; Valenzuela, N. An “Audience Effect” for Ecological Terminology: Use and Misuse of Jargon. Oikos 1997, 80, 632. [Google Scholar] [CrossRef] [Green Version]
- Hirst, R. Scientific jargon, good and bad. J. Tech. Writ. Commun. 2003, 33, 201–229. [Google Scholar] [CrossRef] [Green Version]
- Giachino, P.M.; Vailati, D. Considerations on biological and terminological aspects of the subterranean and endogean environments. Diversity, correlations and faunistic interchange. Atti. Accad. Naz. Ital. Di Entomol. 2017, 65, 57–166. [Google Scholar]
- Martínez, A.; Mammola, S. Specialized Terminology Limits the Reach of New Scientific Knowledge. BioRxiv 2020. [Google Scholar] [CrossRef]
- Montgomery, S.L. The cult of jargon: Reflections on language in science. Sci. Cult. 1989, 1, 42–77. [Google Scholar] [CrossRef]
- Orwell, S.; Angos, I.; Orwell, G. Politics and English Language. In The Collected Essays, Journalism and Letters of George Orwell; Harcourt, Brace: New York, NY, USA, 1968; Volume 4, pp. 127–140. [Google Scholar]
- Sharon, A.J.; Baram-Tsabari, A. Measuring mumbo jumbo: A preliminary quantification of the use of jargon in science communication. Public Underst. Sci. 2014, 23, 528–546. [Google Scholar] [CrossRef] [Green Version]
- Kay, M. Lexemic change and semantic shift in disease names. Cult. Med. Psychiatry 1979, 3, 73–94. [Google Scholar] [CrossRef]
- Norman Geoffrey, R.; Arfai, B.; Gupta, A.; Brooks Lee, R.; Eva Kevin, W. The Privileged Status of Prestigious Terminology: Impact of “Medicalese” on Clinical Judgments. Acad. Med. 2003, 78, S82–S84. [Google Scholar] [PubMed]
- Young, M.E.; Norman, G.R.; Humphreys, K.R. The role of medical language in changing public perceptions of illness. PLoS ONE 2008, 3, e3875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, T.S. Where there is no patient: An anthropological treatment of a biomedical category. Cult. Med. Psychiatry 2008, 32, 577–606. [Google Scholar] [CrossRef] [PubMed]
- Wynne, B. Misunderstood Misunderstanding: Social Identities and Public Uptake of Science; Public Understanding of Science: Bristol, UK, 1992; pp. 281–304. [Google Scholar]
- Fleischman, S. Language and Medicine. In The Handbook of Discourse Analysis; Schiffrin, D., Tannen, D., Hamilton, H.E., Eds.; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2005. [Google Scholar] [CrossRef]
- Heath, C. The Delivery and Reception of Diagnosis in General-Practice Consultation. In Talk at Work: Interaction in Institutional Settings; Drew, P., Heritage, J., Eds.; Cambridge UP: New York, NY, USA, 1992; pp. 235–267. [Google Scholar]
- West, C. Routine Complications: Troubles with Talk Between Doctors and Patients; Indiana UP: Bloomington, Indiana, 1984. [Google Scholar]
- LeBlanc, T.W.; Hesson, A.; Williams, A.; Feudtner, C.; Holmes-Rovner, M.; Williamson, L.D.; Ubel, P.A. Patient understanding of medical jargon: A survey study of U.S. medical students. Patient Educ. Couns. 2014, 95, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, T. Spanish Flu: When Infectious Disease Names Blur Origins and Stigmatize Those Infected. Am. J. Public Health 2018, 108, 1462–1464. [Google Scholar] [CrossRef]
- Eichelberger, L. SARS and New York’s Chinatown: The politics of risk and blame during an epidemic of fear. Soc. Sci. Med. 2007, 65, 1284–1295. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization Best Practices for the Naming of New Human Infectious Diseases. Available online: https://www.who.int/publications/i/item/WHO-HSE-FOS-15.1 (accessed on 4 April 2020).
- Davis, T.; LaCour, M.; Goldwater, M.; Hughes, B.; Ireland, M.E.; Darrell, A.; Worthy, D.A.; Gaylord, N.; Van Allen, J. Communicating about diseases that originate in animals: Lessons from the psychology of inductive reasoning. Behav. Sci. Policy J. 2020, 6, 1–11. [Google Scholar] [CrossRef]
- Dhanani, L.Y.; Franz, B. Unexpected public health consequences of the COVID-19 pandemic: A national survey examining anti-Asian attitudes in the USA. Int. J. Public Health 2020, 65, 747–754. [Google Scholar] [CrossRef]
- Dick, H.; Kristina, W. Racializing discourses. J. Linguist. Anthropol. 2011, 21, E2–E10. [Google Scholar] [CrossRef]
- Foucault, M. The Order of Things: An Archaeology of the Human Sciences/Michel Foucault; Vintage Books: New York, NY, USA, 1973. [Google Scholar]
- Gamble Vanessa, N. Under the Shadow of Tuskegee: African American Health Care. Am. J. Public Health 1997, 87, 418–426. [Google Scholar]
- Prather Fuller, T.R.; Jeffries, W.L.; Marshall, K.J.; Howell, A.V.; Belyue-Umole, A.; King, W. Racism, African American Women, and Their Sexual and Reproductive Health: A Review of Historical and Contemporary Evidence and Implications for Health Equity. Health Equity 2018, 2, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Reverby, S.M. “Normal Exposure’ and Inoculation Syphilis: A PHS ‘Tuskegee’ Doctor in Guatemala, 1946–1948. J. Policy Hist. 2011, 23, 6–28. [Google Scholar] [CrossRef] [Green Version]
- Sebeok, T. Style in Language; Thomas, A.S., Ed.; The MIT Press: Cambridge, MA, USA, 1958. [Google Scholar]
- Fanon, F. Black Skin, White Masks; Pluto Press: London, UK, 1967. [Google Scholar]
- Weedon, C. Feminist Practice and Post-Structuralist Theory; Basil Blackwell: Oxford, UK, 1987. [Google Scholar]
- Gershon, I. Media Ideologies: An Introduction. J. Linguist. Anthropol. 2010, 20, 283–293. [Google Scholar] [CrossRef] [Green Version]
- New York Times. 2021. Available online: https://www.nytimes.com/2021/03/02/opinion/letters/hate-crimes-asian-americans.html (accessed on 14 December 2022).
- Fong, V. SARS, a shipwreck, a NATO attack, and September 11, 2001: Global information flows and Chinese responses to tragic news events. Am. Ethnol. 2007, 34, 521–539. [Google Scholar] [CrossRef] [PubMed]
- Briggs, C.; Nichter, M. Biocommunicability and the biopolitics of pandemic threats. Med. Anthropol. 2009, 28, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Dionne, K.; Turkmen, F. The Politics of Pandemic Othering: Putting COVID-19 in Global and Historical Context. Int. Organ. 2020, 74, E213–E230. [Google Scholar] [CrossRef]
- Karalis Noel, T. Conflating culture with COVID-19: Xenophobic repercussions of a global pandemic. Soc. Sci. Humanit. Open 2020, 2, 100044. [Google Scholar] [CrossRef]
- Team, V.; Manderson, L. How COVID-19 Reveals Structures of Vulnerability. Med. Anthropol. 2020, 39, 671–674. [Google Scholar] [CrossRef]
- Beeman, W. Discourse of Demonization. In The “Great Satan” Vs. the “Mad Mullahs”: How the United States and Iran Demonize Each Other; University of Chicago Press: Chicago, IL, USA, 2005; pp. 1–11. [Google Scholar]
- Moran, M.H. Barbarism, Old and New: Denaturalizing the Rhetoric of Warfare. In Complexities: Beyond Nature and Nurture; Susan, M., Sydel, S., Eds.; University of Chicago Press: Chicago, IL, USA, 2005; pp. 251–267. [Google Scholar]
- Getty Images. Credit Bettmann. 1968. Available online: https://www.gettyimages.com/detail/news-photo/sign-of-the-times-catches-the-eyes-of-anne-and-mike-joslin-news-photo/515019802?adppopup=true (accessed on 4 April 2020).






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harvey, T.S. COVID-19, Framing and Naming a Pandemic: How What Is Not in a Disease Name May Be More Important than What Is. Pathogens 2023, 12, 346. https://doi.org/10.3390/pathogens12020346
Harvey TS. COVID-19, Framing and Naming a Pandemic: How What Is Not in a Disease Name May Be More Important than What Is. Pathogens. 2023; 12(2):346. https://doi.org/10.3390/pathogens12020346
Chicago/Turabian StyleHarvey, T. S. 2023. "COVID-19, Framing and Naming a Pandemic: How What Is Not in a Disease Name May Be More Important than What Is" Pathogens 12, no. 2: 346. https://doi.org/10.3390/pathogens12020346