
Leprosy in an Adopted Woman Diagnosed by Molecular Tools: A Case Report from a Non-Endemic Area

 , , , ,
, , , ,
Abstract
:1. Introduction
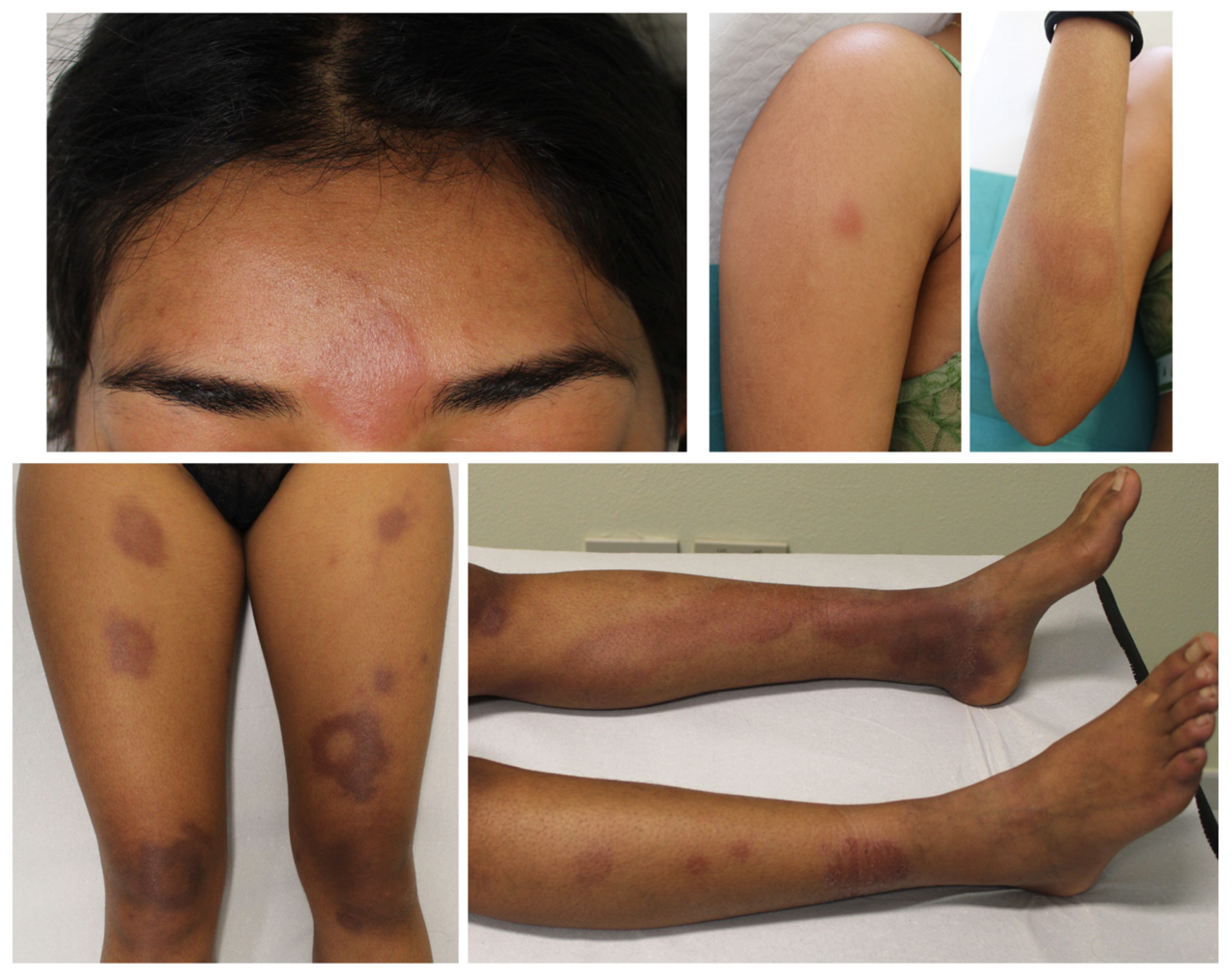
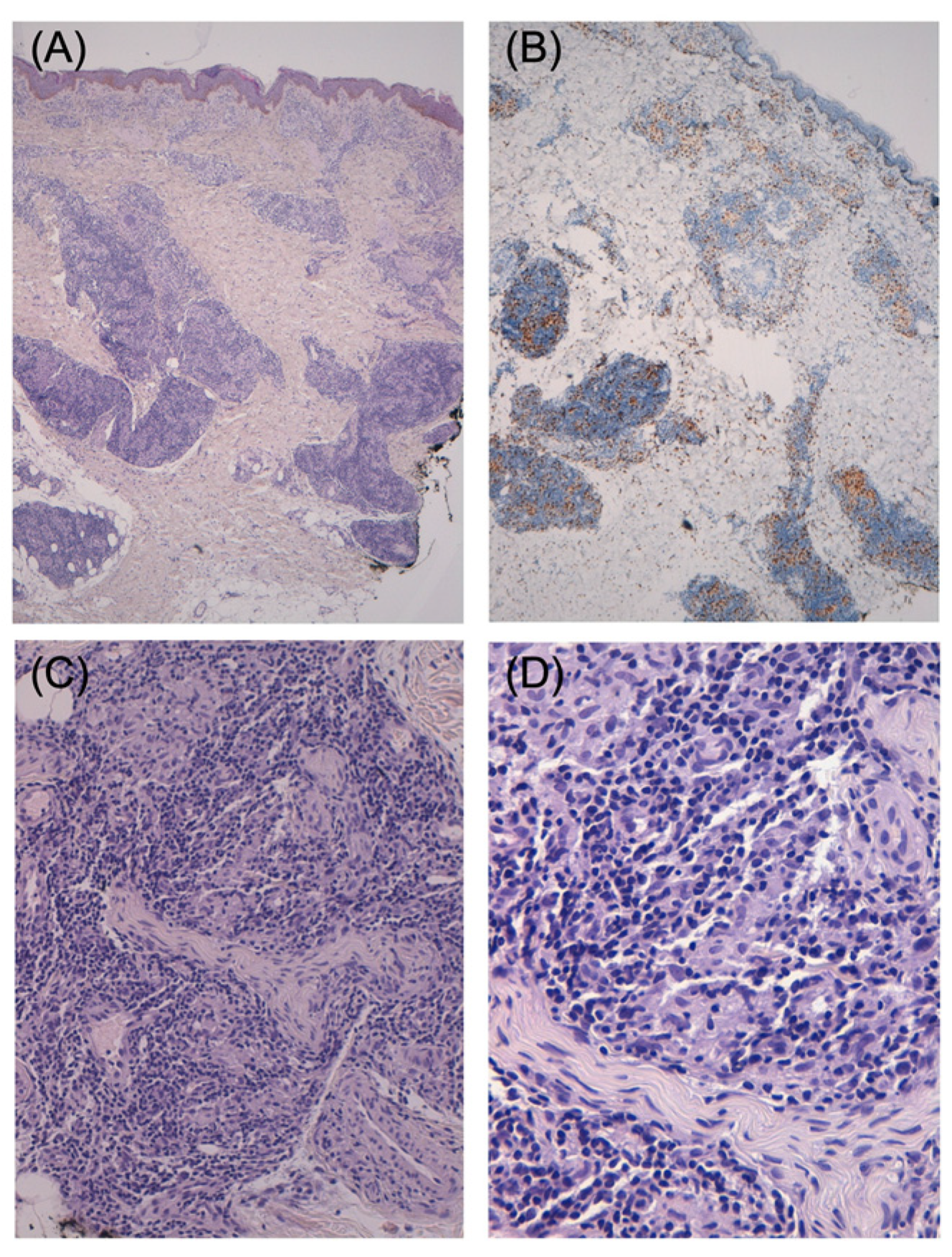
2. Case Report
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rodrigues, L.C.; Lockwood, D. Leprosy now: Epidemiology, progress, challenges, and research gaps. Lancet Infect Dis. 2011, 11, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Deps, P.; Collin, S.M. Mycobacterium lepromatosis as a Second Agent of Hansen’s Disease. Front. Microbiol. 2021, 12, 698588. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Towards Zero Leprosy. Global Leprosy (Hansen’s Disease) Strategy 2021–2030. 2021. Available online: https://www.who.int/publications/i/item/9789290228509 (accessed on 1 October 2022).
- World Health Organization. Global Leprosy (Hansen Disease) Update, 2020: Impact of COVID-19 on Global Leprosy Control. 2021. Available online: https://www.who.int/wer (accessed on 1 October 2022).
- Beltrame, A.; Barabino, G.; Wei, Y.; Clapasson, A.; Orza, P.; Perandin, F.; Piubelli, C.; Monteiro, G.B.; Longoni, S.S.; Rodari, P.; et al. Leprosy in Refugees and Migrants in Italy and a Literature Review of Cases Reported in Europe between 2009 and 2018. Microorganisms 2020, 8, 1113. [Google Scholar] [CrossRef] [PubMed]
- Beauvillain, Q.; Lok, C.; Joachim, C.; Hamdad, F.; Lafabregue, E.; Attencourt, C.; Sevestre, H.; Chaby, G. Autochthonous leprosy in Europe: A case report and literature review. Int. J. Infect. Dis. 2021, 110, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Greco, D.; Galanti, M.R. Leprosy in Italy. Int. J. Lepr. Other Mycobact. Dis. 1983, 51, 495–499. [Google Scholar]
- Massone, C.; Brunasso, A.M.; Noto, S.; Campbell, T.M.; Clapasson, A.; Nunzi, E. Imported leprosy in Italy. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 999–1006. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Balzarini, F.; Mezzoiuso, A.G.; Ranzieri, S.; Vaccaro, F.G.; Odone, A.; Signorelli, C. Epidemiology of leprosy in Italy (1920–2019): A comprehensive review on existing data. Acta Biomed. 2019, 90, 7–14. [Google Scholar]
- Araujo, S.; Freitas, L.O.; Goulart, L.R.; Goulart, I.M. Molecular Evidence for the Aerial Route of Infection of Mycobacterium leprae and the Role of Asymptomatic Carriers in the Persistence of Leprosy. Clin. Infect. Dis. 2016, 63, 1412–1420. [Google Scholar] [CrossRef] [Green Version]
- Ridley, D.S.; Jopling, W.H. Classification of leprosy according to immunity. A five-group system. Int J Lepr Other Mycobact Dis. 1966, 34, 255–273. [Google Scholar]
- Maymone, M.B.C.; Laughter, M.; Venkatesh, S.; Dacso, M.M.; Rao, P.N.; Stryjewska, B.M.; Hugh, J.; Dellavalle, R.P.; Dunnick, C.A. Leprosy: Clinical aspects and diagnostic techniques. J. Am. Acad. Dermatol. 2020, 83, 1–14. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for the Diagnosis, Treatment and Prevention of Leprosy; World Health Organization, Regional Office for South-East Asia: New Delhi, India, 2018. [Google Scholar]
- Sales, A.M.; Ponce de Leon, A.; Düppre, N.C.; Hacker, M.A.; Nery, J.A.; Sarno, E.N.; Penna, M.L.F. Leprosy among patient contacts: A multilevel study of risk factors. PLoS Negl. Trop. Dis. 2011, 5, e1013. [Google Scholar] [CrossRef]
- Bratschi, M.W.; Steinmann, P.; Wickenden, A.; Gillis, T.P. Current knowledge on Mycobacterium leprae transmission: A systematic literature review. Lepr. Rev. 2015, 86, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Longoni, S.S.; Beltrame, A.; Prato, M.; Spencer, J.S.; Bergamaschi, N.; Clapasson, A.; Parodi, A.; Piubelli, C.; Perandin, F. ELISA Test Based on the Phenolic Glycolipid-I (PGL-I) of Mycobacterium leprae: A Reality of a Laboratory from a Non-Endemic Country. Pathogens 2022, 11, 894. [Google Scholar] [CrossRef] [PubMed]
- Truman, R.W.; Andrews, P.K.; Robbins, N.Y.; Adams, L.B.; Krahenbuhl, J.L.; Gillis, T.P. Enumeration of Mycobacterium leprae using real-time PCR. PLoS Negl. Trop. Dis. 2008, 2, e328. [Google Scholar] [CrossRef] [Green Version]
- Avanzi, C.; Lécorché, E.; Rakotomalala, F.A.; Benjak, A.; Rapelanoro Rabenja, F.; Ramarozatovo, L.S.; Cauchoix, B.; Rakoto-Andrianarivelo, M.; Tió-Coma, M.; Leal-Calvo, T.; et al. Population Genomics of Mycobacterium leprae Reveals a New Genotype in Madagascar and the Comoros. Front Microbiol. 2020, 11, 711. [Google Scholar] [CrossRef]
- Lockwood, D.N.; Reid, A.J. The diagnosis of leprosy is delayed in the United Kingdom. QJM 2001, 94, 207–212. [Google Scholar] [CrossRef] [Green Version]
- King, K.; Browning, J.C.; Metry, D.W.; Prestigiacomo, J.; Scollard, D.; Schutze, G.E.; Stryjewska, B.; Schwarzwald, H. Leprosy and international adoption: A case report and review of diagnostic and treatment dilemmas. Pediatr. Infect. Dis. J. 2009, 28, 322–325. [Google Scholar] [CrossRef]
- Giacomet, V.; Vigano, A.; Fabiano, V.; Antinori, S.; Longhi, E.; Zuccotti, G. Leprosy: A disease not to be forgotten in the era of globalization. Pediatr. Int. 2010, 52, 849–850. [Google Scholar] [CrossRef]
- Avanzi, C.; Singh, P.; Truman, R.W.; Suffys, P.N. Molecular epidemiology of leprosy: An update. Infect. Genet. Evol. 2020, 86, 104581. [Google Scholar] [CrossRef]
- Scollard, D.M.; Joyce, M.P.; Gillis, T.P. Development of leprosy and type 1 leprosy reactions after treatment with infliximab: A report of 2 cases. Clin. Infect. Dis. 2006, 43, e19–e22. [Google Scholar] [CrossRef]
- Freitas, D.S.; Machado, N.; Andrigueti, F.V.; Reis Neto, E.T.; Pinheiro, M.M. Lepromatous leprosy associated with the use of anti-TNF α therapy: Case report. Rev. Bras. Reumatol. 2010, 50, 333–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barroso, D.H.; Brandão, J.G.; Andrade, E.S.N.; Correia, A.C.B.; Aquino, D.C.; Chen, A.C.R.; Vernal, S.; de Araújo, W.N.; da Mota, L.M.H.; Sampaio, R.N.R.; et al. Leprosy detection rate in patients under immunosuppression for the treatment of dermatological, rheumatological, and gastroenterological diseases: A systematic review of the literature and meta-analysis. BMC Infect Dis. 2021, 21, 347. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, R.R.; Wakhlu, A.; Agarwal, V. Neglected tropical rheumatic diseases. Clin. Rheumatol. 2022, 41, 1293–1304. [Google Scholar] [CrossRef] [PubMed]
- Wallis, R.S.; Broder, M.; Wong, J.; Lee, A.; Hoq, L. Reactivation of latent granulomatous infections by infliximab. Clin. Infect. Dis. 2005, 41 (Suppl. S3), S194–S198. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, D.N.; Nicholls, P.; Smith, W.C.; Das, L.; Barkataki, P.; van Brakel, W.; Suneetha, S. Comparing the clinical and histological diagnosis of leprosy and leprosy reactions in the INFIR cohort of Indian patients with multibacillary leprosy. PLoS Negl. Trop. Dis. 2012, 6, e1702. [Google Scholar] [CrossRef] [Green Version]
- Desikan, K.V.; Rao, K.V.; Bharambe, M.S.; Rao, P.V. Appraisal of skin smear reports of field laboratories. Lepr. Rev. 2006, 77, 311–316. [Google Scholar] [CrossRef]
- Moschella, S.L. An update on the diagnosis and treatment of leprosy. J. Am. Acad. Dermatol. 2004, 51, 417–426. [Google Scholar] [CrossRef]
- Mahajan, V.K. Slit-skin smear in leprosy: Lest we forget it! Indian J. Lepr. 2013, 85, 177–183. [Google Scholar]
- Rao, P.N.; Suneetha, S. Pure neuritic leprosy: Current status and relevance. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 252–261. [Google Scholar] [CrossRef]
- Banerjee, S.; Biswas, N.; Kanti Das, N.; Sil, A.; Ghosh, P.; Hasanoor Raja, A.H.; Dasgupta, S.; Datta, P.K.; Bhattacharya, B. Diagnosing leprosy: Revisiting the role of the slit-skin smear with critical analysis of the applicability of polymerase chain reaction in diagnosis. Int. J. Dermatol. 2011, 50, 1522–1527. [Google Scholar] [CrossRef]
- Barbieri, R.R.; Manta, F.S.N.; Moreira, S.J.M.; Sales, A.M.; Nery, J.A.C.; Nascimento, L.P.R.; Hacker, M.A.; Pacheco, A.G.; Machado, A.M.; Sarno, E.M.; et al. Quantitative polymerase chain reaction in paucibacillary leprosy diagnosis: A follow-up study. PLoS Negl. Trop. Dis. 2019, 13, e0007147. [Google Scholar] [CrossRef] [PubMed]
- van Hooij, A.; Tjon Kon Fat, E.M.; de Jong, D.; Khatun, M.; Soren, S.; Chowdhury, A.S.; Roy, J.C.; Alam, K.; Kim, J.-P.; Richardus, J.H.; et al. Prototype multi-biomarker test for point-of-care leprosy diagnostics. iScience 2021, 24, 102006. [Google Scholar] [CrossRef] [PubMed]
- Bang, P.D.; Suzuki, K.; Phuong, L.T.; Chu, T.M.; Ishii, N.; Khang, T.H. Evaluation of polymerase chain reaction-based detection of Mycobacterium leprae for the diagnosis of leprosy. J. Dermatol. 2009, 36, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, M.C.; Ramuno, N.M.; Fachin, L.R.; Tassa, M.; Rosa, P.S.; Belone, A.F.; Diório, S.M.; Soares, C.T.; Garlet, G.P.; Trombone, A.P.F. qPCR detection of Mycobacterium leprae in biopsies and slit skin smear of different leprosy clinical forms. Braz. J. Infect. Dis. 2017, 21, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Marques LÉ, C.; Frota, C.C.; Quetz, J.D.S.; Bindá, A.H.; Mota, R.M.S.; Pontes, M.A.A.; Goncalves, H.D.S.; Kendall, C.; Kerr, L.R.F.S. Evaluation of 16S rRNA qPCR for detection of Mycobacterium leprae DNA in nasal secretion and skin biopsy samples from multibacillary and paucibacillary leprosy cases. Pathog. Glob. Health 2018, 112, 72–78. [Google Scholar] [CrossRef]
- Martinez, A.N.; Talhari, C.; Moraes, M.O.; Talhari, S. PCR-based techniques for leprosy diagnosis: From the laboratory to the clinic. PLoS Negl. Trop. Dis. 2014, 8, e2655. [Google Scholar] [CrossRef] [Green Version]
- Tatipally, S.; Srikantam, A.; Kasetty, S. Polymerase Chain Reaction (PCR) as a Potential Point of Care Laboratory Test for Leprosy Diagnosis-A Systematic Review. Trop. Med. Infect. Dis. 2018, 3, 107. [Google Scholar] [CrossRef] [Green Version]
- Manta, F.S.N.; Leal-Calvo, T.; Moreira, S.J.M.; Marques, B.L.C.; Ribeiro-Alves, M.; Rosa, P.S.; Nery, J.A.C.; Rampazzo, R.C.P.; Costa, A.D.T.; Krieger, M.A.; et al. Ultra-sensitive detection of Mycobacterium leprae: DNA extraction and PCR assays. PLoS Negl. Trop. Dis. 2020, 14, e0008325. [Google Scholar] [CrossRef]
- Sharma, R.; Singh, P.; McCoy, R.C.; Lenz, S.M.; Donovan, K.; Ochoa, M.T.; Estrada-Garcia, I.; Silva-Miranda, M.; Cruz, F.J.-F.; Balagon, M.F.; et al. Isolation of Mycobacterium lepromatosis and Development of Molecular Diagnostic Assays to Distinguish Mycobacterium leprae and M. lepromatosis. Clin. Infect. Dis. 2020, 71, e262–e269. [Google Scholar] [CrossRef] [Green Version]
- Cambau, E.; Saunderson, P.; Matsuoka, M.; Cole, S.T.; Kai, M.; Suffys, P.; Rosa, P.S.; Williams, D.; Gupta, U.D.; Lavania, M.; et al. Antimicrobial resistance in leprosy: Results of the first prospective open survey conducted by a WHO surveillance network for the period 2009-15. Clin. Microbiol. Infect. 2018, 24, 1305–1310. [Google Scholar] [CrossRef] [Green Version]
- Aubry, A.; Sammarco Rosa, P.; Chauffour, A.; Fletcher, M.L.; Cambau, E.; Avanzi, C. Drug resistance in leprosy: An update following 70years of chemotherapy. Infect. Dis. Now. 2022, 52, 243–251. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sample Name | Type of Sample | Sampling Date (DD.MM.YY) | qPCR Ct () |
|---|---|---|---|
| 3654-2136/21 | Skin biopsy (right forearm) | 19.04.21 | 24.67 |
| 3654-5546/21 | Skin biopsy (right arm) | 15.07.21 | 28.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beltrame, A.; Fargnoli, M.C.; Avanzi, C.; Sollima, L.; Pomari, E.; Mori, A.; Longoni, S.S.; Moro, L.; Orza, P.; Jackson, M.; et al. Leprosy in an Adopted Woman Diagnosed by Molecular Tools: A Case Report from a Non-Endemic Area. Pathogens 2023, 12, 165. https://doi.org/10.3390/pathogens12020165
Beltrame A, Fargnoli MC, Avanzi C, Sollima L, Pomari E, Mori A, Longoni SS, Moro L, Orza P, Jackson M, et al. Leprosy in an Adopted Woman Diagnosed by Molecular Tools: A Case Report from a Non-Endemic Area. Pathogens. 2023; 12(2):165. https://doi.org/10.3390/pathogens12020165
Chicago/Turabian StyleBeltrame, Anna, Maria Concetta Fargnoli, Charlotte Avanzi, Laura Sollima, Elena Pomari, Antonio Mori, Silvia Stefania Longoni, Lucia Moro, Pierantonio Orza, Mary Jackson, and et al. 2023. "Leprosy in an Adopted Woman Diagnosed by Molecular Tools: A Case Report from a Non-Endemic Area" Pathogens 12, no. 2: 165. https://doi.org/10.3390/pathogens12020165