
Histological Alterations in Placentas of Pregnant Women with SARS-CoV-2 Infection: A Single-Center Case Series
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Macroscopic Characteristics
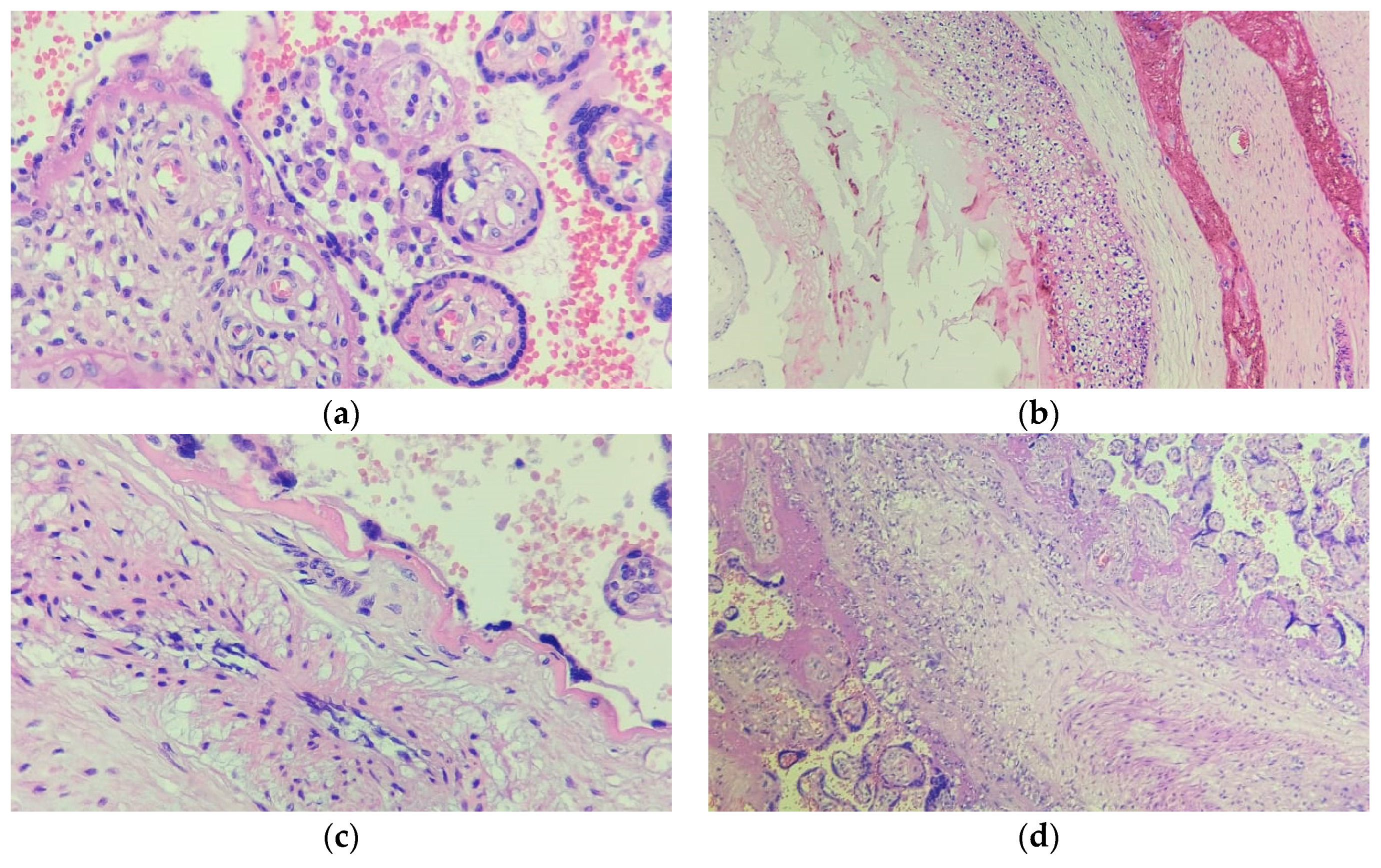
3.2. Microscopic Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The Species Severe Acute Respiratory Syndrome-Related Coronavirus: Classifying 2019-NCoV and Naming It SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 4 June 2023).
- Allotey, J.; Fernandez, S.; Bonet, M.; Stallings, E.; Yap, M.; Kew, T.; Zhou, D.; Coomar, D.; Sheikh, J.; Lawson, H.; et al. Clinical Manifestations, Risk Factors, and Maternal and Perinatal Outcomes of Coronavirus Disease 2019 in Pregnancy: Living Systematic Review and Meta-Analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- Siiteri, P.K.; Febres, F.; Clemens, L.E.; Chang, R.J.; Gondos, B.; Stites, D. Progesterone and Maintenance of Pregnancy: Is Progesterone Nature’s Immunosuppressant? Ann. N. Y. Acad. Sci. 1977, 286, 384–397. [Google Scholar] [CrossRef] [PubMed]
- Lomauro, A.; Aliverti, A.; Frykholm, P.; Alberico, D.; Persico, N.; Boschetti, G.; Debellis, M.; Briganti, F.; Nosotti, M.; Righi, I. Adaptation of Lung, Chest Wall, and Respiratory Muscles during Pregnancy: Preparing for Birth. J. Appl. Physiol. 2019, 127, 1640–1650. [Google Scholar] [CrossRef] [PubMed]
- Hirnle, L.; Lysenko, L.; Gerber, H.; Lesnik, P.; Baranowska, A.; Rachwalik, M.; Leszczyszyn, J.; Strozecki, L. Respiratory Function in Pregnant Women. In Advances in Experimental Medicine and Biology; Springer Science and Business Media, LLC: Dordrecht, The Netherlands, 2013; Volume 788, pp. 153–160. ISBN 9789400766266. [Google Scholar]
- Abu-Raya, B.; Michalski, C.; Sadarangani, M.; Lavoie, P.M. Maternal Immunological Adaptation During Normal Pregnancy. Front. Immunol. 2020, 11, 575197. [Google Scholar] [CrossRef]
- Kourtis, A.P.; Read, J.S.; Jamieson, D.J. Pregnancy and Infection. N. Engl. J. Med. 2014, 370, 2211–2218. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, Transmission, and Pathogenesis of SARS-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef]
- Mahyuddin, A.P.; Kanneganti, A.; Wong, J.J.L.; Dimri, P.S.; Su, L.L.; Biswas, A.; Illanes, S.E.; Mattar, C.N.Z.; Huang, R.Y.J.; Choolani, M. Mechanisms and Evidence of Vertical Transmission of Infections in Pregnancy Including SARS-CoV-2s. Prenat. Diagn. 2020, 40, 1655–1670. [Google Scholar] [CrossRef]
- Adhikari, E.H.; Moreno, W.; Zofkie, A.C.; MacDonald, L.; McIntire, D.D.; Collins, R.R.J.; Spong, C.Y. Pregnancy Outcomes Among Women with and without Severe Acute Respiratory Syndrome Coronavirus 2 Infection. JAMA Netw. Open 2020, 3, e2029256. [Google Scholar] [CrossRef]
- Valdés, G.; Neves, L.A.A.; Anton, L.; Corthorn, J.; Chacón, C.; Germain, A.M.; Merrill, D.C.; Ferrario, C.M.; Sarao, R.; Penninger, J.; et al. Distribution of Angiotensin-(1-7) and ACE2 in Human Placentas of Normal and Pathological Pregnancies. Placenta 2006, 27, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical Characteristics and Intrauterine Vertical Transmission Potential of COVID-19 Infection in Nine Pregnant Women: A Retrospective Review of Medical Records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The Impact of COVID-19 on Pregnancy Outcomes: A Systematic Review and Meta-Analysis. Can. Med. Assoc. J. 2021, 193, E540–E548. [Google Scholar] [CrossRef] [PubMed]
- Di Mascio, D.; Buca, D.; Berghella, V.; Khalil, A.; Rizzo, G.; Odibo, A.; Saccone, G.; Galindo, A.; Liberati, M.; D’Antonio, F. Counseling in Maternal–Fetal Medicine: SARS-CoV-2 Infection in Pregnancy. Ultrasound Obstet. Gynecol. 2021, 57, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Morotti, D. Placental Pathology of COVID-19 with and without Fetal and Neonatal Infection: Trophoblast Necrosis and Chronic Histiocytic Intervillositis as Risk Factors for Transplacental Transmission of SARS-CoV-2. Viruses 2020, 12, 1308. [Google Scholar] [CrossRef]
- Aghaamoo, S.; Ghods, K.; Rahmanian, M. Pregnant Women with COVID-19: The Placental Involvement and Consequences. J. Mol. Histol. 2021, 52, 427–435. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Morotti, D.; Beigi, B.; Moshfegh, F.; Zafaranloo, N.; Patanè, L. Confirming Vertical Fetal Infection with Coronavirus Disease 2019: Neonatal and Pathology Criteria for Early Onset and Transplacental Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 From Infected Pregnant Mothers. Arch. Pathol. Lab. Med. 2020, 144, 1451–1456. [Google Scholar] [CrossRef]
- Oltean, I.; Tran, J.; Lawrence, S.; Ruschkowski, B.A.; Zeng, N.; Bardwell, C.; Nasr, Y.; de Nanassy, J.; El Demellawy, D. Impact of SARS-CoV-2 on the Clinical Outcomes and Placental Pathology of Pregnant Women and Their Infants: A Systematic Review. Heliyon 2021, 7, e06393. [Google Scholar] [CrossRef]
- Narang, K.; Cheek, E.H.; Enninga, E.A.L.; Theiler, R.N. Placental Immune Responses to Viruses: Molecular and Histo-Pathologic Perspectives. Int. J. Mol. Sci. 2021, 22, 2921. [Google Scholar] [CrossRef]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental Transmission of SARS-CoV-2 Infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef]
- Algarroba, G.N.; Rekawek, P.; Vahanian, S.A.; Khullar, P.; Palaia, T.; Peltier, M.R.; Chavez, M.R.; Vintzileos, A.M. Visualization of Severe Acute Respiratory Syndrome Coronavirus 2 Invading the Human Placenta Using Electron Microscopy. Am. J. Obstet. Gynecol. 2020, 223, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Suhren, J.-T.; Meinardus, A.; Hussein, K.; Schaumann, N. Meta-Analysis on COVID-19-Pregnancy-Related Placental Pathologies Shows No Specific Pattern. Placenta 2022, 117, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, R.; Khalil, A.; Alameddine, S.; D’Angelo, E.; Galliani, C.; Matarrelli, B.; Buca, D.; Liberati, M.; Rizzo, G.; D’Antonio, F. Placental Histopathology after SARS-CoV-2 Infection in Pregnancy: A Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. MFM 2021, 3, 100468. [Google Scholar] [CrossRef] [PubMed]
- Radan, A.-P.; Baud, D.; Favre, G.; Papadia, A.; Surbek, D.; Baumann, M.; Raio, L. Low Placental Weight and Altered Metabolic Scaling after Severe Acute Respiratory Syndrome Coronavirus Type 2 Infection during Pregnancy: A Prospective Multicentric Study. Clin. Microbiol. Infect. 2022, 28, 718–722. [Google Scholar] [CrossRef]
- Brien, M.-E.; Bouron-Dal Soglio, D.; Dal Soglio, S.; Couture, C.; Boucoiran, I.; Nasr, Y.; Widdows, K.; Sharps, M.C.; El Demellawy, D.; EP Heazell, A.; et al. Pandemic Stress and SARS-CoV-2 Infection Are Associated with Pathological Changes at the Maternal-Fetal Interface. Placenta 2021, 115, 37–44. [Google Scholar] [CrossRef]
- Husen, M.F.; van der Meeren, L.E.; Verdijk, R.M.; Fraaij, P.L.A.; van der Eijk, A.A.; Koopmans, M.P.G.; Freeman, L.; Bogers, H.; Trietsch, M.D.; Reiss, I.K.M.; et al. Unique Severe COVID-19 Placental Signature Independent of Severity of Clinical Maternal Symptoms. Viruses 2021, 13, 1670. [Google Scholar] [CrossRef]
- de Laat, M.; Franx, A.; van Alderen, E.; Nikkels, P.; Visser, G. The Umbilical Coiling Index, a Review of the Literature. J. Matern. Fetal Neonatal Med. 2005, 17, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Tasca, C.; Rossi, R.S.; Corti, S.; Anelli, G.M.; Savasi, V.; Brunetti, F.; Cardellicchio, M.; Caselli, E.; Tonello, C.; Vergani, P.; et al. Placental Pathology in COVID-19 Affected Pregnant Women: A Prospective Case-Control Study. Placenta 2021, 110, 9–15. [Google Scholar] [CrossRef]
- Blasco Santana, L.; Miraval Wong, E.; Álvarez-Troncoso, J.; Sánchez García, L.; Bartha, J.L.; Regojo-Zapata, R.M. Maternal and Perinatal Outcomes and Placental Pathologic Examination of 29 SARS-CoV-2 Infected Patients in the Third Trimester of Gestation. J. Obstet. Gynaecol. Res. 2021, 47, 2131–2139. [Google Scholar] [CrossRef]
- Hessami, K.; Aagaard, K.M.; Castro, E.C.; Arian, S.E.; Nassr, A.A.; Barrozo, E.R.; Seferovic, M.D.; Shamshirsaz, A.A. Placental Vascular and Inflammatory Findings from Pregnancies Diagnosed with Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Am. J. Perinatol. 2022, 39, 1643–1653. [Google Scholar] [CrossRef]
- Nizyaeva, N.; Lomova, N.; Dolgopolova, E.; Petrova, U.; Karapetyan, T.; Shmakov, R.; Frankevich, V. The Impact of the Novel Coronavirus Infection COVID-19 on the Mother-Placenta-Fetus System. Bull. Russ. State Med. Univ. 2021, 2, 25–31. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Avvad-Portari, E.; Babál, P.; Baldewijns, M.; Blomberg, M.; Bouachba, A.; Camacho, J.; Collardeau-Frachon, S.; Colson, A.; Dehaene, I.; et al. Placental Tissue Destruction and Insufficiency From COVID-19 Causes Stillbirth and Neonatal Death From Hypoxic-Ischemic Injury. Arch. Pathol. Lab. Med. 2022, 146, 660–676. [Google Scholar] [CrossRef] [PubMed]
- Musa, S.S.; Bello, U.M.; Zhao, S.; Abdullahi, Z.U.; Lawan, M.A.; He, D. Vertical Transmission of SARS-CoV-2: A Systematic Review of Systematic Reviews. Viruses 2021, 13, 1877. [Google Scholar] [CrossRef] [PubMed]
- Ayala-Ramírez, P.; González, M.; Escudero, C.; Quintero-Arciniegas, L.; Giachini, F.R.; Alves de Freitas, R.; Damiano, A.E.; García-Robles, R. Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Pregnancy. A Non-Systematic Review of Clinical Presentation, Potential Effects of Physiological Adaptations in Pregnancy, and Placental Vascular Alterations. Front. Physiol. 2022, 13, 785274. [Google Scholar] [CrossRef]
- Chi, J.; Gong, W.; Gao, Q. Clinical Characteristics and Outcomes of Pregnant Women with COVID-19 and the Risk of Vertical Transmission: A Systematic Review. Arch. Gynecol. Obstet. 2021, 303, 337–345. [Google Scholar] [CrossRef]
- Stenton, S.; McPartland, J.; Shukla, R.; Turner, K.; Marton, T.; Hargitai, B.; Bamber, A.; Pryce, J.; Peres, C.L.; Burguess, N.; et al. SARS-CoV-2 Placentitis and Pregnancy Outcome: A Multicentre Experience during the Alpha and Early Delta Waves of Coronavirus Pandemic in England. EClinicalMedicine 2022, 47, 101389. [Google Scholar] [CrossRef]
- Allotey, J.; Chatterjee, S.; Kew, T.; Gaetano, A.; Stallings, E.; Fernández-García, S.; Yap, M.; Sheikh, J.; Lawson, H.; Coomar, D.; et al. SARS-CoV-2 Positivity in Offspring and Timing of Mother-to-Child Transmission: Living Systematic Review and Meta-Analysis. BMJ 2022, 376, e067696. [Google Scholar] [CrossRef]
- Rodrigues, C.; Baía, I.; Domingues, R.; Barros, H. Pregnancy and Breastfeeding During COVID-19 Pandemic: A Systematic Review of Published Pregnancy Cases. Front. Public Health 2020, 8, 558144. [Google Scholar] [CrossRef]


{kind=link}
| Placental Characteristics | N = 29 | |
|---|---|---|
| Weight (g) | 423.0 (385.0–521.0) | |
| Placental weight in relation to newborn weight | Less than adequate | 14 (58.3%) |
| Higher than adequate | 9 (37.5%) | |
| Adequate | 1 (4.2%) | |
| Width (cm) | 18.0 (16.5–20.5) | |
| Length (cm) | 16.0 (15.0–18.0) | |
| Thickness (cm) | 2.7 (2.5–3.0) | |
| Fetal surface staining | Violet | 26 (89.7%) |
| Brown | 2 (6.9%) | |
| Greenish-brown | 1 (3.4%) | |
| Trabeculation | Well-trabeculated | 4 (13.8%) |
| Moderate | 24 (82.8%) | |
| Discreet | 1 (3.4%) | |
| Placental lobes | Poorly delimited | 25 (86.2%) |
| Well-delimited | 4 (13.8%) | |
| Maternal surface staining | Normal | 27 (93.1%) |
| Dark red | 2 (6.9%) | |
| Insertion of the umbilical cord | Central | 2 (6.9%) |
| Paracentral | 26 (89.7%) | |
| Paramarginal | 1 (3.4%) | |
| Umbilical cord length (cm) | 44.0 (37.0–47.0) | |
| Greenish-brown umbilical cord staining | 2 (6.9%) | |
| Maximum diameter of the umbilical cord (cm) | 1.5 (1.3–1.8) | |
| Cord with more than 15 turns | 15 (51.7%) | |
| Placental Characteristics | N = 29 | |
|---|---|---|
| Microscopic examination of the umbilical cord | Neutrophilic exudate | 4 (13.8%) |
| Amnion with squamous metaplasia | 4 (13.8%) | |
| Neutrophilic infiltrate | 3 (10.3%) | |
| Cuboidal without atypia, foci of squamous metaplasia | 1 (3.6%) | |
| Amnion with neutrophilic infiltrate | 1 (3.4%) | |
| Extraplacental membranes | Fibrin deposition | 27 (93.1%) |
| Presence of necrosis | 18 (62.0%) | |
| Calcifications | 15 (51.7%) | |
| Cysts | 11 (37.9%) | |
| Presence of leukocytes | 9 (31.0%) | |
| Presence of neutrophilic exudate | 5 (17.2%) | |
| Thrombosis | 4 (13.8%) | |
| Delayed placental maturation | 2 (6.9%) | |
| Presence of neutrophilic infiltrate | 1 (3.4%) | |
| Microscopic examination of the placenta | Placental histology compatible with gestational age | 27 (93.1%) |
| Chorionic villi compatible with gestational age | 28 (96.6%) | |
| Placental infarction | 6 (20.6%) | |
| Intervillous thrombosis | 6 (20.6%) | |
| Chorioamnionitis | 6 (20.6%) | |
| Villitis | 4 (13.8%) | |
| Perivillositis | 4 (13.8%) | |
| Intervillositis | 3 (10.3%) | |
| Tissue laminar necrosis | 2 (6.9%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patiño Escarcina, J.E.; da Silva, A.K.C.V.; Medeiros, M.O.d.A.; Fernandes, S.S.S.; Agareno, L.A.; Garboggini, L.A.; Gouveia, M.d.S.; Duarte, V.C.; Morbeck, D.L.; Moreira, L.M.O. Histological Alterations in Placentas of Pregnant Women with SARS-CoV-2 Infection: A Single-Center Case Series. Pathogens 2023, 12, 1197. https://doi.org/10.3390/pathogens12101197
Patiño Escarcina JE, da Silva AKCV, Medeiros MOdA, Fernandes SSS, Agareno LA, Garboggini LA, Gouveia MdS, Duarte VC, Morbeck DL, Moreira LMO. Histological Alterations in Placentas of Pregnant Women with SARS-CoV-2 Infection: A Single-Center Case Series. Pathogens. 2023; 12(10):1197. https://doi.org/10.3390/pathogens12101197
Chicago/Turabian StylePatiño Escarcina, Jesus Enrique, Ana Keila Carvalho Vieira da Silva, Malú Oliveira de Araújo Medeiros, Stephanie Santos Santana Fernandes, Luiza Andrade Agareno, Louise Andrade Garboggini, Marcela de Sá Gouveia, Vanessa Campos Duarte, Diogo Lago Morbeck, and Lícia Maria Oliveira Moreira. 2023. "Histological Alterations in Placentas of Pregnant Women with SARS-CoV-2 Infection: A Single-Center Case Series" Pathogens 12, no. 10: 1197. https://doi.org/10.3390/pathogens12101197